
Healthcare Workers’ Attitudes toward Influenza Vaccination: A Behaviour and Social Drivers Survey
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Public Involvement
2.2. Participants and Data Collection
2.3. Measurement and Variables
3. Statistical Analysis
4. Results
5. Attitudes and Behaviour of HCWs towards Influenza Vaccine
6. Main Drivers of Influenza Vaccine Hesitancy by the BeSD Survey
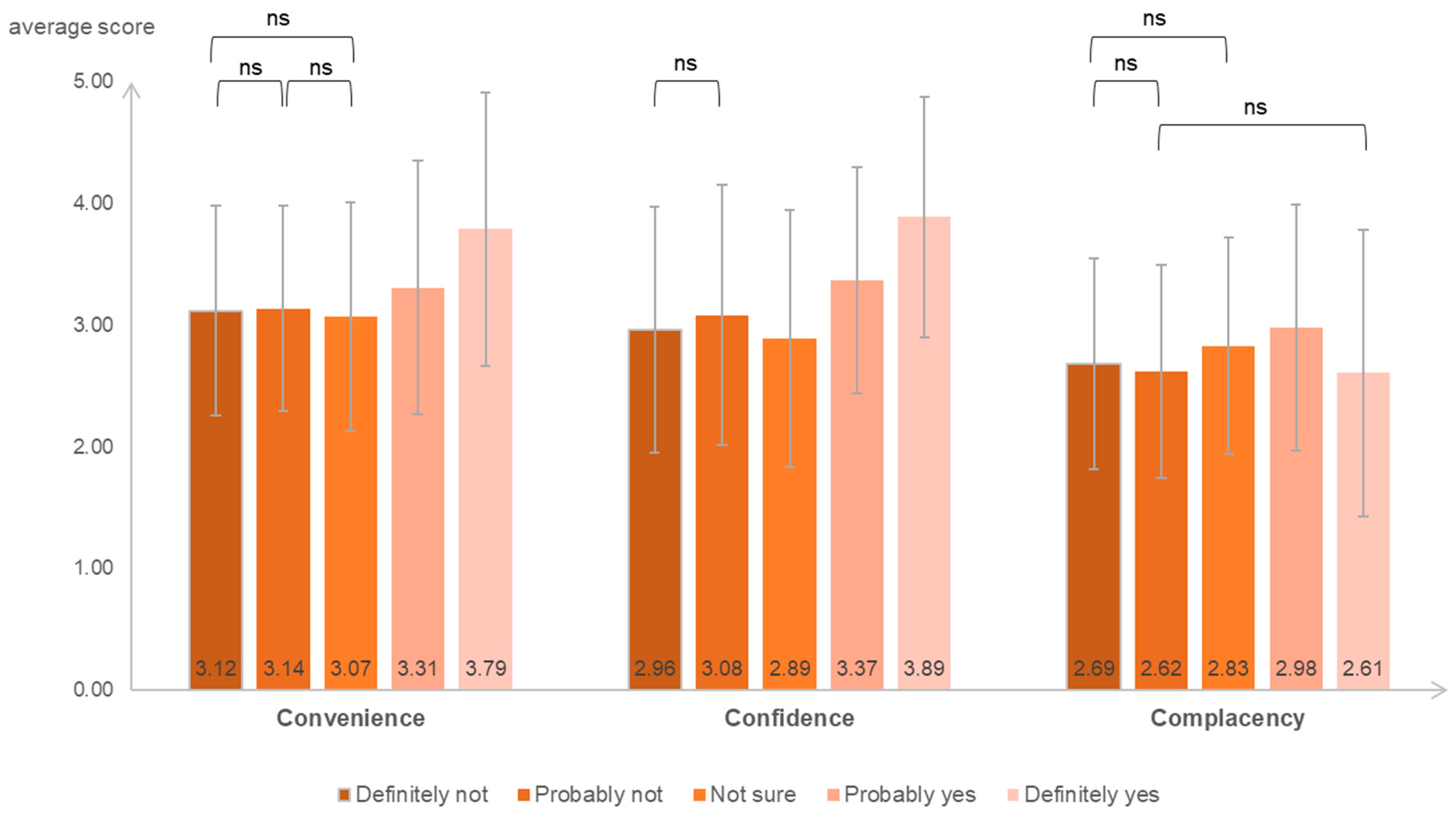
7. Main Drivers of Influenza Vaccine Hesitancy in 3Cs’ Model
8. Discussion
9. Conclusions
Author Contributions
Funding
Institution Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kuster, S.P.; Shah, P.S.; Coleman, B.L.; Lam, P.P.; Tong, A.; Wormsbecker, A.; McGeer, A. Incidence of influenza in healthy adults and healthcare workers: A systematic review and meta-analysis. PLoS ONE 2011, 6, e26239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Commission, C.N.H. National Influenza Prevention and Control Program (Pilotversion). Available online: http://www.nhc.gov.cn/jkj/s7923/201810/b30b71408e5641c7a166d4e389318103.shtml (accessed on 1 October 2022).
- Amodio, E.; Restivo, V.; Firenze, A.; Mammina, C.; Tramuto, F.; Vitale, F. Can influenza vaccination coverage among healthcare workers influence the risk of nosocomial influenza-like illness in hospitalized patients? J. Hosp. Infect. 2014, 86, 182–187. [Google Scholar] [CrossRef]
- Imai, C.; Toizumi, M.; Hall, L.; Lambert, S.; Halton, K.; Merollini, K. A systematic review and meta-analysis of the direct epidemiological and economic effects of seasonal influenza vaccination on healthcare workers. PLoS ONE 2018, 13, e0198685. [Google Scholar] [CrossRef] [PubMed]
- FluNet. Global Influenza Surveillance and Response System (GISRS) Data Generated on 15 September 2022. Available online: www.who.int/toolkits/flunet (accessed on 27 September 2022).
- Ma, L.; Han, X.; Ma, Y.; Yang, Y.; Xu, Y.; Liu, D.; Yang, W.; Feng, L. Decreased influenza vaccination coverage among Chinese healthcare workers during the COVID-19 pandemic. Infect. Dis. Poverty 2022, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Uyeki, T.M.; Hui, D.S.; Zambon, M.; Wentworth, D.E.; Monto, A.S. Influenza. Lancet 2022, 400, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Ghazy, R.M.; Al-Salahat, K.; Al-Mahzoum, K.; AlHadidi, N.M.; Eid, H.; Kareem, N.; Al-Ajlouni, E.; Batarseh, R.; Ababneh, N.A.; et al. The Role of Psychological Factors and Vaccine Conspiracy Beliefs in Influenza Vaccine Hesitancy and Uptake among Jordanian Healthcare Workers during the COVID-19 Pandemic. Vaccines 2022, 10, 1355. [Google Scholar] [CrossRef]
- World Health Organization. Understanding the behavioural and social drivers of vaccine uptake WHO position paper—May 2022. Wkly. Epidemiol. Rec. 2022, 97, 209–224. [Google Scholar]
- MacDonald, N.E.; Hesitancy, S.W.G.o.V. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Brewer, N.T. What Works to Increase Vaccination Uptake. Acad. Pediatr. 2021, 21, S9–S16. [Google Scholar] [CrossRef]
- National Immunization Advisory Committee Technical Working Group, I.V.T.W.G. Technical guidelines for seasonal influenza vaccination in China (2022–2023). Chin J. Prev. Med. 2022, 56, 4–34. [Google Scholar] [CrossRef]
- Verger, P.; Collange, F.; Fressard, L.; Bocquier, A.; Gautier, A.; Pulcini, C.; Raude, J.; Peretti-Watel, P. Prevalence and correlates of vaccine hesitancy among general practitioners: A cross-sectional telephone survey in France, April to July 2014. Euro. Surveill. 2016, 21, 30406. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Lindley, M.C.; Allred, N.; Weinbaum, C.M.; Grohskopf, L. Effect of influenza vaccination of healthcare personnel on morbidity and mortality among patients: Systematic review and grading of evidence. Clin. Infect. Dis. 2014, 58, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillari, A.; Polito, F.; Pucciarelli, G.; Serra, N.; Gargiulo, G.; Esposito, M.R.; Botti, S.; Rea, T.; Simeone, S. Influenza vaccination and healthcare workers: Barriers and predisposing factors. Acta Biomed. 2021, 92, e2021004. [Google Scholar] [CrossRef] [PubMed]
- Yi, H.; Yang, Y.; Zhang, L.; Zhang, M.; Wang, Q.; Zhang, T.; Zhang, Y.; Qin, Y.; Peng, Z.; Leng, Z.; et al. Improved influenza vaccination coverage among health-care workers: Evidence from a web-based survey in China, 2019/2020 season. Hum. Vaccin. Immunother 2021, 17, 2185–2189. [Google Scholar] [CrossRef]
- Shapiro, G.K.; Kaufman, J.; Brewer, N.T.; Wiley, K.; Menning, L.; Leask, J.; Be, S.D.W.G. A critical review of measures of childhood vaccine confidence. Curr. Opin. Immunol. 2021, 71, 34–45. [Google Scholar] [CrossRef]
- Gonzalez-Block, M.A.; Pelcastre-Villafuerte, B.E.; Riva Knauth, D.; Fachel-Leal, A.; Comes, Y.; Crocco, P.; Noboa, L.; Rodriguez Zea, B.; Ruoti, M.; Diaz Portillo, S.P.; et al. Influenza vaccination hesitancy in large urban centers in South America. Qualitative analysis of confidence, complacency and convenience across risk groups. PLoS ONE 2021, 16, e0256040. [Google Scholar] [CrossRef]
- Willems, L.D.; Dyzel, V.; Sterkenburg, P.S. COVID-19 Vaccination Intentions amongst Healthcare Workers: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 10192. [Google Scholar] [CrossRef]
- Hornsey, M.J.; Fielding, K.S. Attitude roots and Jiu Jitsu persuasion: Understanding and overcoming the motivated rejection of science. Am. Psychol. 2017, 72, 459–473. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science Into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- Hall, C.M.; Northam, H.; Webster, A.; Strickland, K. Determinants of seasonal influenza vaccination hesitancy among healthcare personnel: An integrative review. J. Clin. Nurs. 2022, 31, 2112–2124. [Google Scholar] [CrossRef]
- Scardina, G.; Ceccarelli, L.; Casigliani, V.; Mazzilli, S.; Napoletano, M.; Padovan, M.; Petillo, A.; Sironi, D.; Brilli, C.; Gattini, V.; et al. Evaluation of Flu Vaccination Coverage among Healthcare Workers during a 3 Years’ Study Period and Attitude towards Influenza and Potential COVID-19 Vaccination in the Context of the Pandemic. Vaccines (Basel) 2021, 9, 769. [Google Scholar] [CrossRef] [PubMed]
- Marcu, A.; Rubinstein, H.; Michie, S.; Yardley, L. Accounting for personal and professional choices for pandemic influenza vaccination amongst English healthcare workers. Vaccine 2015, 33, 2267–2272. [Google Scholar] [CrossRef] [PubMed]
- Jiang, V.; Wang, Z.; Jia, M.; Yan, H.; Su, Z.; Liu, S.; Yang, W.; Qian, Y.; Feng, L. Awareness, knowledge and attitude toward influenza vaccination in several population groups in China: A cross-sectional study. Front. Public Health 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Mayer, B.; Helm, S.; Heinz, E.; Barnett, M.; Arora, M. Doubt in store: Vaccine hesitancy among grocery workers during the COVID-19 pandemic. J. Behav. Med. 2022. [Google Scholar] [CrossRef]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- Durando, P.; Alicino, C.; Dini, G.; Barberis, I.; Bagnasco, A.M.; Iudici, R.; Zanini, M.; Martini, M.; Toletone, A.; Paganino, C.; et al. Determinants of adherence to seasonal influenza vaccination among healthcare workers from an Italian region: Results from a cross-sectional study. BMJ Open 2016, 6, e010779. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Levels | N | % | High Acceptance (n = 7516) | Moderate Acceptance (n = 5839) | ||
|---|---|---|---|---|---|---|---|
| n | % (95% CI) | n | % (95% CI) | ||||
| Gender | |||||||
| Male | 10,042 | 56.31 | 3753 | 37.37 (36.43–38.32) | 3338 | 33.24 (32.32–34.17) | |
| Per capita disposable income a | |||||||
| Low | 1762 | 9.88 | 864 | 49.04 (46.70–51.37) | 593 | 33.65 (31.48–35.89) | |
| Moderate | 4283 | 24.02 | 1940 | 45.30 (43.81–46.79) | 1468 | 34.28 (32.86–35.71) | |
| High | 11,787 | 66.10 | 4712 | 39.98 (39.09–40.86) | 3778 | 32.05 (31.21–32.90) | |
| Type of workplace | |||||||
| Primary hospitals/Community health centers | 2977 | 16.69 | 1419 | 47.67 (45.87–49.46) | 951 | 31.94 (30.29–33.64) | |
| Secondary hospitals | 4577 | 25.67 | 1923 | 42.01 (40.59–43.45) | 1491 | 32.58 (31.23–33.94) | |
| Tertiary hospitals | 5979 | 33.53 | 2720 | 45.49 (44.23–46.76) | 1930 | 32.28 (31.10–33.47) | |
| Medical education or academic institutions | 1255 | 7.04 | 315 | 25.10 (22.76–27.55) | 471 | 37.53 (34.88–40.23) | |
| Centers for disease control and prevention | 1614 | 9.05 | 634 | 39.28 (36.92–41.68) | 502 | 31.10 (28.88–33.39) | |
| Health-related public organizations | 1334 | 7.48 | 469 | 35.16 (32.63–37.75) | 451 | 33.81 (31.31–36.38) | |
| Others | 96 | 0.54 | 36 | 37.50 (28.30–47.44) | 43 | 44.79 (35.12–54.77) | |
| Professional title b | |||||||
| Senior | 5297 | 29.71 | 2440 | 46.06 (44.72–47.41) | 1929 | 36.42 (35.13–37.72) | |
| Intermediate | 5740 | 32.19 | 2610 | 45.47 (44.18–46.76) | 1870 | 32.58 (31.37–33.80) | |
| Junior | 4707 | 26.40 | 1565 | 33.25 (31.91–34.60) | 1454 | 30.89 (29.58–32.22) | |
| None | 2088 | 11.71 | 901 | 43.15 (41.04–45.28) | 586 | 28.07 (26.17–30.02) | |
| Chronic diseases | |||||||
| Yes | 4778 | 26.79 | 1574 | 32.94 (31.62–34.29) | 1450 | 30.35 (29.06–31.66) | |
| Perceived risk of influenza this season | |||||||
| Not at all concerned | 6672 | 37.42 | 4216 | 63.19 (62.03–64.34) | 1618 | 24.25 (23.23–25.29) | |
| A little concerned | 7170 | 40.21 | 2322 | 32.38 (31.31–33.48) | 3003 | 41.88 (40.74–43.03) | |
| Moderately concerned | 3171 | 17.78 | 659 | 20.78 (19.40–22.22) | 1071 | 33.77 (32.14–35.44) | |
| Very concerned | 819 | 4.59 | 319 | 38.95 (35.65–42.32) | 147 | 17.95 (15.44–20.69) | |
| Confidence in influenza vaccine benefits | |||||||
| Not at all important | 1713 | 9.61 | 802 | 46.82 (44.46–49.19) | 449 | 26.21 (24.17–28.33) | |
| A little important | 5610 | 31.46 | 1033 | 18.41 (17.42–19.44) | 2736 | 48.77 (47.46–50.08) | |
| Moderately important | 5113 | 28.67 | 1429 | 27.95 (26.73–29.19) | 2010 | 39.31 (37.98–40.66) | |
| Very important | 5396 | 30.26 | 4252 | 78.80 (77.69–79.87) | 644 | 11.93 (11.09–12.82) | |
| Ability to answer influenza vaccine questions | |||||||
| Not at all confident | 2676 | 15.01 | 927 | 34.64 (32.86–36.46) | 888 | 33.18 (31.42–34.99) | |
| A little confident | 5280 | 29.61 | 1085 | 20.55 (19.48–21.66) | 2267 | 42.94 (41.60–44.27) | |
| Moderately confident | 4442 | 24.91 | 1696 | 38.18 (36.76–39.62) | 1677 | 37.75 (36.34–39.19) | |
| Very confident | 5434 | 30.47 | 3808 | 70.08 (68.85–71.28) | 1007 | 18.53 (17.52–19.58) | |
| Colleague norms c | |||||||
| Yes | 10,930 | 61.29 | 5335 | 48.81 (47.87–49.75) | 3380 | 30.92 (30.06–31.80) | |
| No | 3739 | 20.97 | 1160 | 31.02 (29.56–32.52) | 1235 | 33.03 (31.54–34.55) | |
| Unclear | 3163 | 17.74 | 1021 | 32.28 (30.67–33.92) | 1224 | 38.70 (37.01–40.40) | |
| Attitude toward influenza vaccine by workplace this season | |||||||
| Required | 2788 | 15.63 | 1538 | 55.16 (53.31–57.00) | 758 | 27.19 (25.56–28.86) | |
| Encouraged | 10,918 | 61.23 | 4730 | 43.32 (42.40–44.25) | 3622 | 33.17 (32.30–34.06) | |
| Neutrality | 2945 | 16.52 | 826 | 28.05 (26.45–29.69) | 1053 | 35.76 (34.04–37.50) | |
| Unclear | 1181 | 6.62 | 422 | 35.73 (33.04–38.50) | 406 | 34.38 (31.71–37.12) | |
| Influenza vaccine valent | |||||||
| Trivalent | 7722 | 43.30 | 3443 | 44.59 (43.48–45.70) | 2453 | 31.77 (30.73–32.81) | |
| Quadrivalent | 6502 | 36.46 | 2281 | 35.08 (33.93–36.25) | 2298 | 35.34 (34.19–36.51) | |
| Unaffected | 3608 | 20.23 | 1792 | 49.67 (48.04–51.30) | 1088 | 30.16 (28.67–31.67) | |
| Influenza vaccine type | |||||||
| Inactive vaccine | 9036 | 50.67 | 4318 | 47.79 (46.76–48.82) | 2980 | 32.98 (32.02–33.95) | |
| live attenuated vaccine | 5380 | 30.17 | 1472 | 27.36 (26.18–28.56) | 1872 | 34.80 (33.53–36.08) | |
| Unaffected | 3416 | 19.16 | 1726 | 50.53 (48.85–52.20) | 987 | 28.89 (27.39–30.43) | |
| Recommendation willingness | |||||||
| High | 8562 | 48.01 | 5519 | 64.46 (63.44–65.47) | 1965 | 22.95 (22.07–23.85) | |
| Moderate | 6164 | 34.57 | 1469 | 23.83 (22.78–24.91) | 2878 | 46.69 (45.45–47.94) | |
| Hesitancy | 3106 | 17.42 | 528 | 17.00 (15.71–18.35) | 996 | 32.07 (30.44–33.72) | |
| 2021/2022 influenza vaccination site | |||||||
| Hospital | 4766 | 26.73 | 2765 | 58.02 (56.61–59.41) | 1306 | 27.40 (26.15–28.68) | |
| Centers for disease control and prevention | 4719 | 26.46 | 1740 | 36.87 (35.50–38.26) | 1553 | 32.91 (31.58–34.26) | |
| Community health centers | 2600 | 14.58 | 1112 | 42.77 (40.88–44.68) | 742 | 28.54 (26.83–30.30) | |
| Others | 12 | 0.07 | 8 | 66.67 (38.76–87.55) | 1 | 8.33 (0.91–32.85) | |
| No | 5735 | 32.16 | 1891 | 32.97 (31.77–34.20) | 2237 | 39.01 (37.75–40.27) | |
| On-site vaccination | |||||||
| Yes | 12,871 | 72.18 | 6408 | 49.79 (48.92–50.65) | 4122 | 32.03 (31.22–32.84) | |
| No | 4166 | 23.36 | 922 | 22.13 (20.89–23.41) | 1411 | 33.87 (32.44–35.32) | |
| Not sure | 795 | 4.46 | 186 | 23.40 (20.55–26.43) | 306 | 38.49 (35.16–41.91) | |
| Ways of influenza vaccine payment | |||||||
| Self-paid | 4557 | 25.56 | 2059 | 45.18 (43.74–46.63) | 1450 | 31.82 (30.48–33.18) | |
| Free | 7229 | 40.54 | 3026 | 41.86 (40.73–43.00) | 2278 | 31.51 (30.45–32.59) | |
| Employer paid | 3385 | 18.98 | 1242 | 36.69 (35.08–38.33) | 1134 | 33.50 (31.93–35.10) | |
| Medical insurance | 2587 | 14.51 | 1156 | 44.68 (42.78–46.61) | 962 | 37.19 (35.34–39.06) | |
| Others | 74 | 0.41 | 33 | 44.59 (33.66–55.95) | 15 | 20.27 (12.35–30.46) | |
| Affordability d | |||||||
| Not at all easy | 1875 | 10.51 | 660 | 35.20 (33.06–37.38) | 591 | 31.52 (29.45–33.65) | |
| A little easy | 4824 | 27.05 | 1058 | 21.93 (20.78–23.12) | 1891 | 39.20 (37.83–40.58) | |
| Moderately easy | 6080 | 34.10 | 2166 | 35.63 (34.43–36.84) | 2477 | 40.74 (39.51–41.98) | |
| Very easy | 5053 | 28.34 | 3632 | 71.88 (70.63–73.10) | 880 | 17.42 (16.39–18.48) | |
| Free vaccination provided by employers | |||||||
| Yes | 11,195 | 62.78 | 5777 | 51.60 (50.68–52.53) | 3435 | 30.68 (29.83–31.54) | |
| No | 4558 | 25.56 | 1106 | 24.27 (23.04–25.53) | 1604 | 35.19 (33.81–36.59) | |
| Unclear | 2079 | 11.66 | 633 | 30.45 (28.50–32.45) | 800 | 38.48 (36.41–40.59) | |
| Hesitancy | Moderate Acceptance | ||||
|---|---|---|---|---|---|
| Characteristics | Levels | aOR 95%CI | p.Value | aOR 95%CI | p.Value |
| Gender | |||||
| Female | ref | ref | |||
| Male | 1.41 (1.28–1.56) | <0.01 | 1.24 (1.14–1.36) | <0.01 | |
| Per capita disposable income | |||||
| High | ref | ref | |||
| Moderate | 0.83 (0.74–0.94) | <0.01 | 1.00 (0.90–1.10) | 0.93 | |
| Low | 0.70 (0.59–0.83) | <0.01 | 0.92 (0.80–1.06) | 0.24 | |
| Hospital level | |||||
| Tertiary | ref | ref | |||
| Secondary | 1.02 (0.90–1.15) | 0.78 | 0.95 (0.85–1.06) | 0.34 | |
| Primary/Community health centers | 0.98 (0.84–1.14) | 0.78 | 0.96 (0.85–1.09) | 0.55 | |
| non-nosocomial | 1.20 (1.05–1.36) | 0.01 | 1.01 (0.90–1.13) | 0.85 | |
| Professional title | |||||
| Senior | ref | ref | |||
| Intermediate | 1.27 (1.11–1.44) | <0.01 | 1.00 (0.90–1.11) | 0.98 | |
| Junior | 1.82 (1.57–2.10) | <0.01 | 1.08 (0.95–1.22) | 0.24 | |
| None | 1.40 (1.18–1.67) | <0.01 | 0.90 (0.77–1.05) | 0.18 | |
| Chronic diseases | |||||
| No | ref | ref | |||
| Yes/Unclear | 1.58 (1.41–1.77) | <0.01 | 1.02 (0.92–1.13) | 0.76 | |
| Thinking and feeling | |||||
| Confidence in influenza vaccine benefits | |||||
| Very important | ref | ref | |||
| Moderately important | 3.93 (3.41–4.53) | <0.01 | 4.55 (4.04–5.12) | <0.01 | |
| A little important | 4.69 (4.04–5.43) | <0.01 | 7.26 (6.42–8.22) | <0.01 | |
| Not at all important | 1.97 (1.63–2.37) | <0.01 | 2.27 (1.93–2.69) | <0.01 | |
| Perceived risk of influenza | |||||
| Very concerned | ref | ref | |||
| Moderately concerned | 0.84 (0.66–1.06) | 0.13 | 1.37 (1.07–1.76) | 0.01 | |
| A little concerned | 0.36 (0.29–0.45) | <0.01 | 1.10 (0.86–1.39) | 0.45 | |
| Not at all concerned | 0.24 (0.19–0.30) | <0.01 | 0.71 (0.56–0.90) | <0.01 | |
| Ability to answer questions | |||||
| Very confident | ref | ref | |||
| Moderately confident | 1.44 (1.25–1.67) | <0.01 | 1.49 (1.33–1.68) | <0.01 | |
| A little confident | 2.13 (1.85–2.46) | <0.01 | 1.99 (1.76–2.25) | <0.01 | |
| Not at all confident | 1.63 (1.39–1.91) | <0.01 | 1.46 (1.27–1.67) | <0.01 | |
| Social processes | |||||
| Colleague norms | |||||
| Yes | ref | ref | |||
| No | 1.57 (1.39–1.78) | <0.01 | 1.13 (1.00–1.26) | 0.04 | |
| Unclear | 1.39 (1.19–1.62) | <0.01 | 1.27 (1.11–1.45) | <0.01 | |
| Attitude toward influenza vaccine by workplace this season | |||||
| Required | ref | ref | |||
| Encouraged | 1.15 (1.00–1.33) | 0.06 | 1.20 (1.07–1.35) | <0.01 | |
| Others (Neutrality/Unclear) | 1.19 (1.00–1.42) | 0.04 | 0.99 (0.85–1.15) | 0.89 | |
| Motivation | |||||
| Influenza vaccine valent | |||||
| Trivalent | 0.79 (0.67–0.94) | 0.01 | 0.89 (0.77–1.04) | 0.14 | |
| quadrivalent | 0.88 (0.75–1.05) | 0.15 | 0.98 (0.85–1.13) | 0.78 | |
| Unaffected | ref | ref | |||
| Influenza vaccine type | |||||
| Inactive vaccine | 1.11 (0.94–1.31) | 0.23 | 1.34 (1.16–1.55) | <0.01 | |
| live attenuated vaccine | 2.05 (1.72–2.44) | <0.01 | 1.60 (1.37–1.87) | <0.01 | |
| Unaffected | ref | ref | |||
| Willingness to recommend | |||||
| High | ref | ref | |||
| Moderate | 2.64 (2.36–2.96) | <0.01 | 2.54 (2.31–2.80) | <0.01 | |
| Hesitancy | 5.31 (4.60–6.13) | <0.01 | 2.55 (2.22–2.94) | <0.01 | |
| Practical issues | |||||
| 2021/2022 influenza vaccination | |||||
| Yes | ref | ref | |||
| No | 1.28 (1.15–1.44) | <0.01 | 1.28 (1.16–1.41) | <0.01 | |
| On-site vaccination | |||||
| Yes | ref | ref | |||
| No | 1.86 (1.66–2.10) | <0.01 | 1.18 (1.06–1.32) | <0.01 | |
| Not sure | 1.83 (1.45–2.31) | <0.01 | 1.23 (0.99–1.54) | 0.06 | |
| Affordability | |||||
| Very easy | ref | ref | |||
| Moderately easy | 1.42 (1.23–1.63) | <0.01 | 1.69 (1.51–1.89) | <0.01 | |
| A little easy | 1.99 (1.71–2.32) | <0.01 | 1.71 (1.50–1.95) | <0.01 | |
| Not at all easy | 1.71 (1.42–2.05) | <0.01 | 1.48 (1.25–1.74) | <0.01 | |
| Free vaccination provided by employers | |||||
| Yes | ref | ref | |||
| No | 1.60 (1.42–1.81) | <0.01 | 1.11 (0.99–1.23) | 0.08 | |
| Unclear | 1.40 (1.17–1.67) | <0.01 | 1.11 (0.95–1.30) | 0.18 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, B.; Cao, Y.; Qian, J.; Jiang, M.; Huang, Q.; Sun, Y.; Dai, P.; Yi, H.; Zhang, R.; Xu, L.; et al. Healthcare Workers’ Attitudes toward Influenza Vaccination: A Behaviour and Social Drivers Survey. Vaccines 2023, 11, 143. https://doi.org/10.3390/vaccines11010143
Jiang B, Cao Y, Qian J, Jiang M, Huang Q, Sun Y, Dai P, Yi H, Zhang R, Xu L, et al. Healthcare Workers’ Attitudes toward Influenza Vaccination: A Behaviour and Social Drivers Survey. Vaccines. 2023; 11(1):143. https://doi.org/10.3390/vaccines11010143
Chicago/Turabian StyleJiang, Binshan, Yanlin Cao, Jie Qian, Mingyue Jiang, Qiangru Huang, Yanxia Sun, Peixi Dai, Heya Yi, Run Zhang, Lili Xu, and et al. 2023. "Healthcare Workers’ Attitudes toward Influenza Vaccination: A Behaviour and Social Drivers Survey" Vaccines 11, no. 1: 143. https://doi.org/10.3390/vaccines11010143