Abstract
Background: The public’s attitude towards Mpox vaccination is a critical factor in the success of immunisation programmes. Understanding the factors contributing to vaccine acceptance or hesitancy is critical for developing effective health communication strategies. This systematic review and meta-analysis aims to bring together evidence from observational studies on attitudes towards Mpox vaccination, including willingness and rejection. Methods: From this review’s inception until June 2023, a comprehensive search was conducted across four major electronic databases: PubMed, Web of Science, Scopus, and EBSCO. The inclusion criteria included studies investigating public attitudes towards Mpox vaccination, as defined by acceptance and willingness to be vaccinated versus rejection and unwillingness. Results: Thirty studies met the inclusion criteria among the screened literature. An analysis of 27 studies involving 81,792 participants revealed that 45,926 (56.14%) were willing to receive the Mpox vaccination. In contrast, ten studies involving 7448 participants revealed that 2156 people (28.94%) were unwilling to receive the Mpox vaccination. Females were less willing to receive the vaccine than males, with an odds ratio (OR) of 0.61 (95% CI, 0.43–0.86). Furthermore, homosexuals were found to be more willing than heterosexuals, with an OR of 1.44 (95% CI, 1.14–1.80). Conclusion: Vaccination is emerging as a critical strategy for preventing Mpox infection and fostering herd immunity against potential outbreaks. Improving public awareness and acceptance of vaccination is critical to avoiding a situation similar to the COVID-19 pandemic. Targeted educational and outreach programmes could explain the benefits of vaccination, bridging the information gap and encouraging a proactive public health approach to emerging infectious diseases.
1. Introduction
Mpox (monkeypox) is a re-emerging zoonotic disease caused by the human Mpox virus (MPXV), which is a complex DNA virus of the genus Orthopoxvirus [1]. It was identified for the first time in 1958 among monkeys in Denmark [2]. The human infection began in 1971 with a case in the Democratic Republic of the Congo, after which the disease spread to Central and West Africa. Notably, the disease spread beyond the African continent for the first time in 2003 [3,4].
Humans, although accidental hosts, are exposed to the infection directly or indirectly. Contact with infectious animal fluids, bites, or the consumption of uncooked animal flesh are all examples of direct transmission [5]. On the other hand, human-to-human transmission occurs through close or intimate contact with infectious skin lesions, fluids, respiratory droplets, or sexual contact, the latter of which is recognised as a significant risk factor. According to CDC data, many Mpox cases are linked to homosexual and bisexual men. Nonetheless, infection susceptibility extends to any individual who comes into contact with infected entities, regardless of sexual orientation [6].
A critical transmission route is maternal-to-foetal, in which the Mpox virus crosses the placental barrier and causes congenital infections. Contact with contaminated clothing, linens, or household items can also result in indirect transmission [2]. Manifestations of Mpox include a maculopapular rash, fever, headache, fatigue, and muscular discomfort [2]. Despite a symptomatic resemblance to smallpox, Mpox is distinguished by lymphadenitis, most commonly in the submandibular, submental, and inguinal regions [7].
Mpox infection cases increased across 30 countries in May 2022 [7]. The World Health Organisation (WHO) declared a multinational outbreak by the end of July, raising global alarm. As of August 10, 2023, the global case count had surpassed 89,308, with 152 fatalities recorded [8,9]. Recent increases in Mpox infection cases in various countries have highlighted the need for effective public health interventions to reduce the disease’s spread and impact.
Vaccination remains a critical strategy for preventing the spread of infectious diseases, effectively establishing herd immunity and preventing outbreaks. There is currently no Mpox vaccine available in the prophylactic landscape. However, according to the WHO and CDC recommendations, two existing smallpox vaccines, JYNNEOS and ACAM2000, have an 85% efficacy against Mpox [9]. Knowledge, cultural beliefs, previous vaccination experiences, and perceived hazards and benefits could all influence people’s attitudes and intentions towards receiving Mpox vaccination. Furthermore, given the recorded gaps in health-seeking behaviours and vaccine acceptance among different demographic groups, sexual and gender identities could have a role in influencing these attitudes.
Understanding public attitudes towards Mpox vaccination is critical for developing targeted educational and vaccination campaigns in the context of a strained global healthcare system following the COVID-19 pandemic. This will help increase vaccine uptake, slow disease spread, and decrease the risk of further strain on medical resources.
The main objective of this systematic review and meta-analysis is to compile existing literature studies to provide a comprehensive understanding of public attitudes towards Mpox vaccination. It will also investigate the possible impact of sexual and gender identities on these attitudes, providing information that could be useful in adapting initiatives to improve vaccine acceptance and coverage against this resurgent infectious threat.
2. Methods
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [10]. We registered the study protocol in PROSPERO (CRD42023451945).
2.1. Search Strategy
We searched four electronic databases (PubMed, Web of Science, Scopus, and EBSCO) from inception until June 2023. The following search strategy was used for all the databases: “(monkeypox OR Mpox OR mpxv) AND (vaccination) OR (vaccinated) OR (vaccine)”. Our search strategy was comprehensive, with no age, setting, or publication date restrictions.
2.2. Inclusion and Exclusion Criteria
We included studies investigating the attitudes of the people towards the Mpox vaccination, whether there is acceptance and willingness or a rejection and unwillingness to be vaccinated. We included all types of observational studies (cohort, case–control, and cross-sectional), while we excluded narrative and systematic reviews, meta-analyses, case reports, and case series.
2.3. Study Selection and Data Extraction
Four authors independently conducted the screening process in two steps: title and abstract screening and full-text screening to determine the final included studies. Any disagreements between the authors during the screening process were resolved by discussion with a senior author. Data were extracted in a preformed Microsoft Excel spreadsheet, which included study information (study design, year, country, sample size, and summary of findings), participant characteristics (gender, age, sexual orientation, population, preexisting diseases, and taking COVID-19 vaccination), and lastly, patients’ acceptance or refusal to receive Mpox vaccine.
2.4. Quality Assessment
We used the Newcastle–Ottawa scale to assess the included studies’ quality [11]. Four researchers conducted this assessment, and any disagreement was resolved with a senior reviewer. Scores of 0–3 were considered low quality, 4–6 as moderate quality, and 7–9 as high quality.
2.5. Statistical Analysis
We conducted the statistical analysis using Open Meta Analyst software to calculate the willingness and non-willingness rates to receive Mpox vaccines among all the participants in each study. We also used Review Manager version 5.4 to examine the factors affecting willingness to take vaccines. We used the pooled odds ratio analysis to determine the factors with higher odds of willingness to receive the vaccine. This analysis was conducted at a confidence level of 95% and a p-value of 0.05. Heterogeneity was assessed using I2 and a p-value of 0.05. We conducted subgroup analysis between different included populations using Open Meta Analyst software version 5.26.14.
3. Results
3.1. Literature Search Results
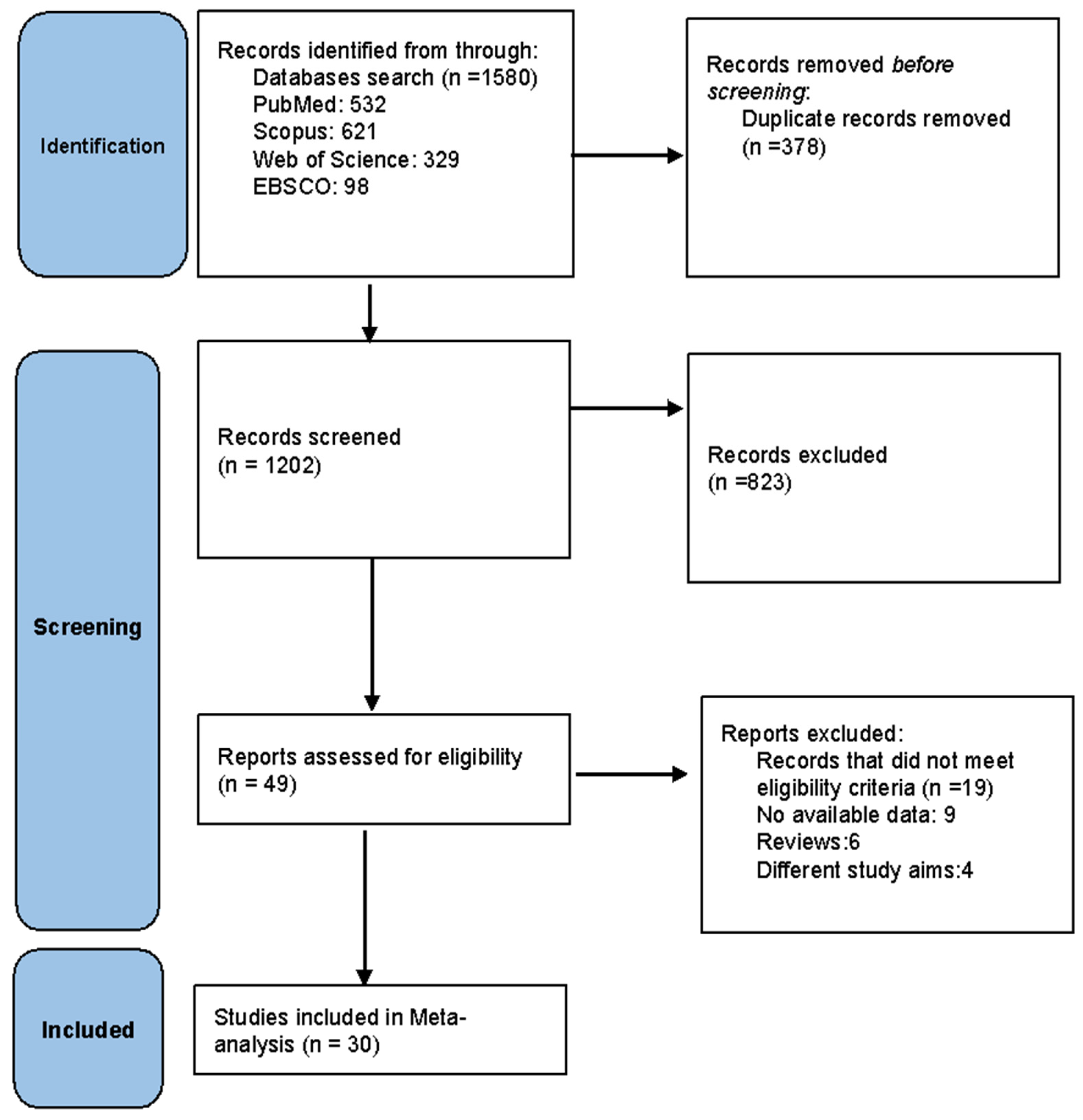
Our literature database search yielded 1580 records. After removing duplicates, 1202 studies remained for the title and abstract screening. Forty-nine articles were eligible for full-text screening. From these, 30 studies [1,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] were included in the meta-analysis. The PRISMA flow diagram of the study is shown in Figure 1.
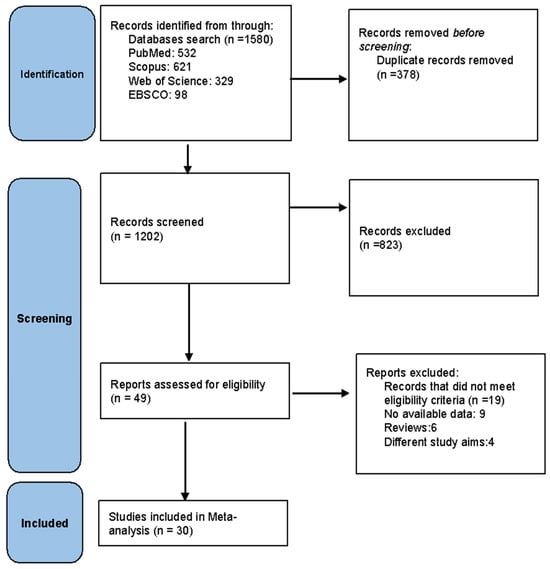
Figure 1.
PRISMA flow diagram of the included studies.
3.2. Baseline Characteristics
All the included studies were of cross-sectional design and were conducted in different regions such as Asia, Europe, Middle East, Africa, and North America. The population differed across the studies where some were conducted on the general population, other studies on HCWs, university students, and LGBTQ (lesbian, gay, bisexual, transgender, queer and questioning) community (Table 1).

Table 1.
Baseline characteristics and summary of the included studies.
3.3. Quality Assessment
According to NOS, six [13,18,24,25,27,37] of the included studies were of high quality, twenty-one [1,12,14,15,16,17,19,20,21,22,26,28,29,30,31,32,34,36,38,39,40] of moderate quality, and three [23,33,35] of low quality (Table 2).
Table 2.
Quality assessment of included studies using Newcastle–Ottawa scale.
3.4. Meta-Analysis
Willingness to Receive Mpox Vaccines
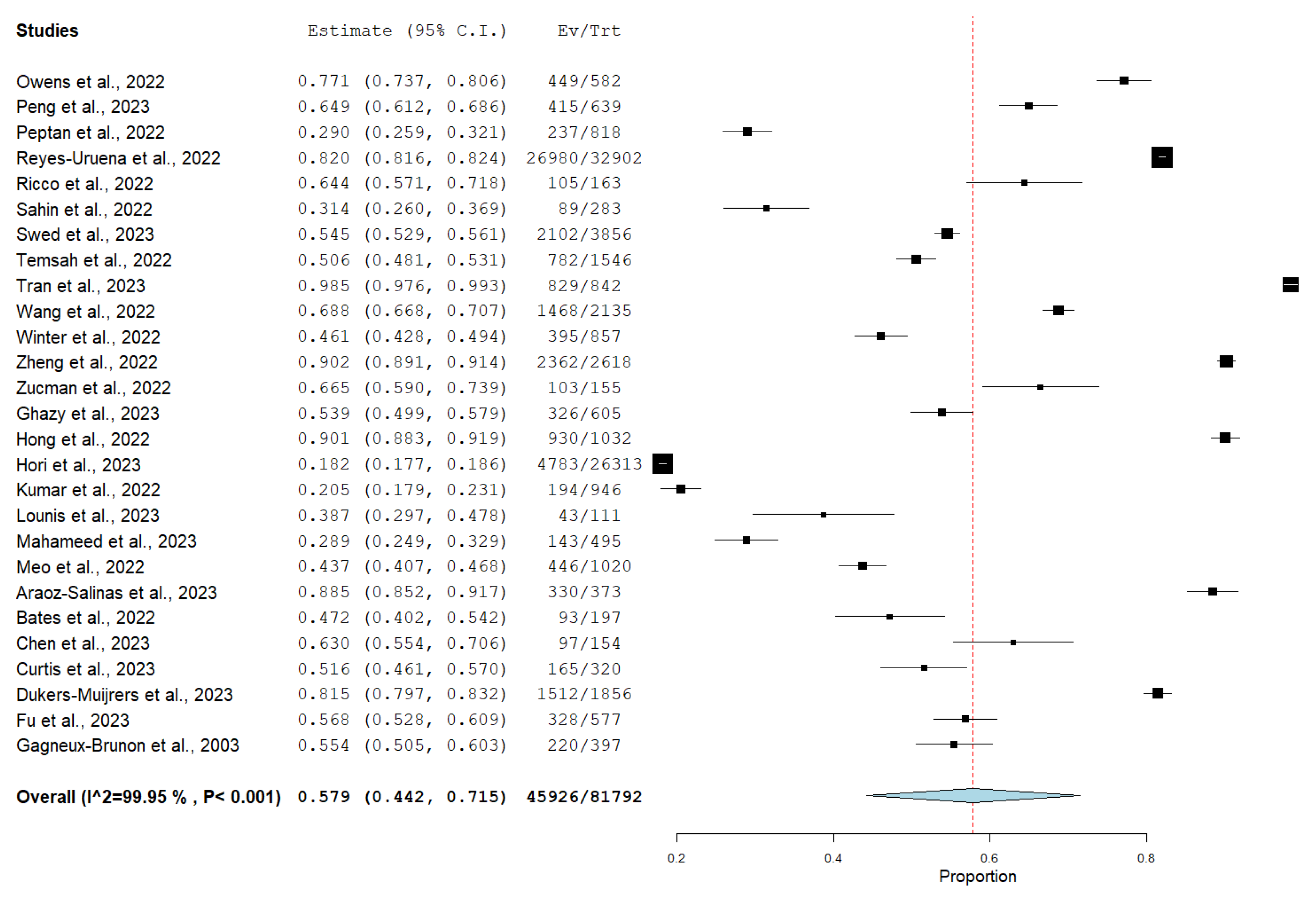
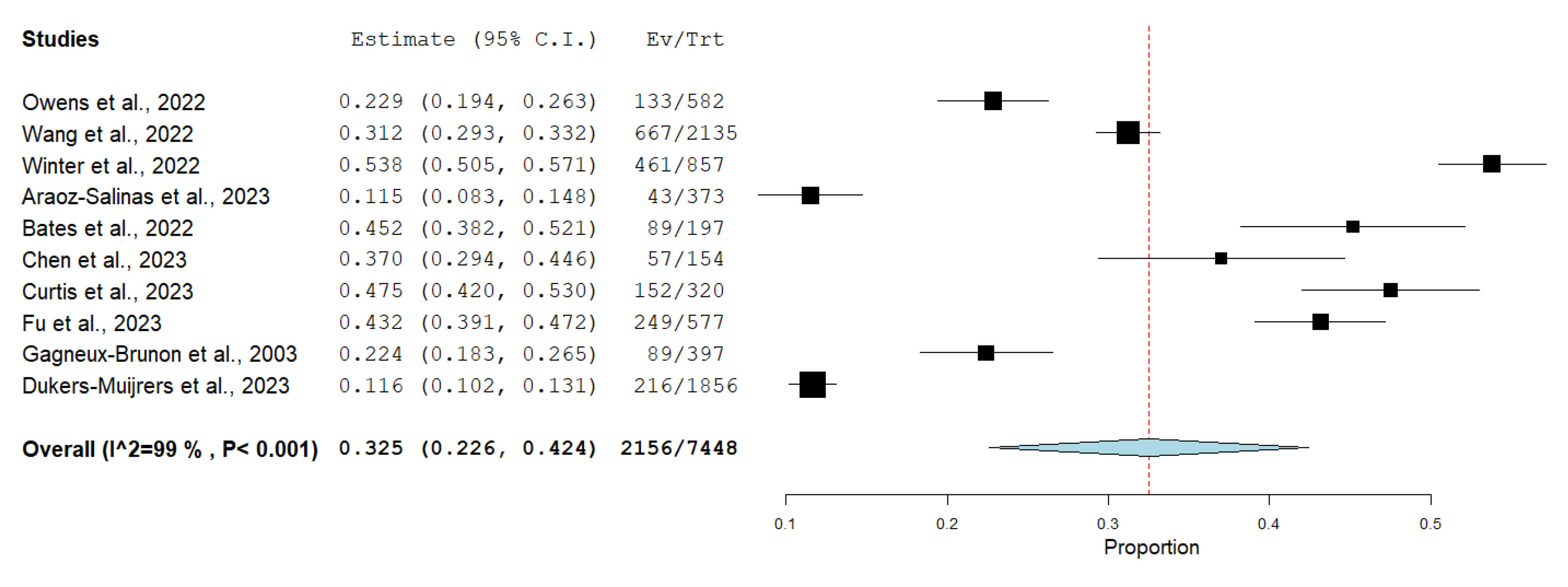
Among 30 of the included studies, 27 studies investigated the willingness to receive Mpox vaccine with a total of 81,792, of which, 45,926 (56.14%) of them were willing to receive Mpox vaccination, as shown in Figure 2, while only 10 of the included studies reported vaccine refusal with a total of 7448 participants, and 2156 (28.94%) were not willing to receive Mpox vaccination, as shown in Figure 3.
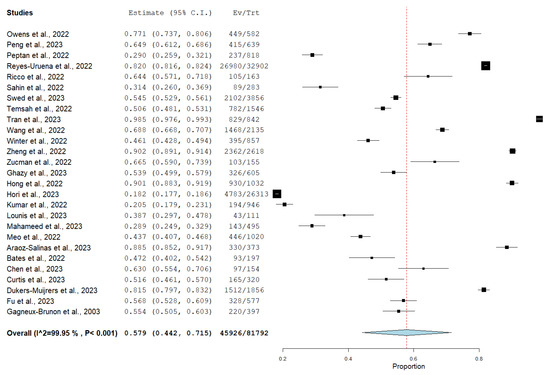
Figure 2.
Forest plot of overall willingness among study participants to receive Mpox vaccine. (Black: each study proportion; Blue: pooled result 95%CI; Red dashed: pooled result, central value).
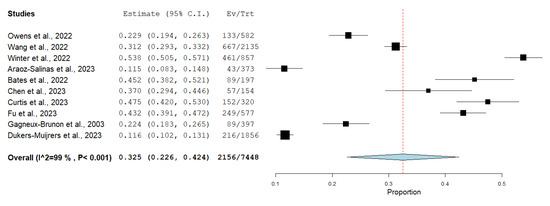
Figure 3.
Forest plot illustrating unwillingness among study participants to receive the Mpox vaccine.(Red: central value. Blue: pooled result 95%CI; Black: central value for each study).
3.5. Gender Difference in Willingness to Be Vaccinated against Mpox
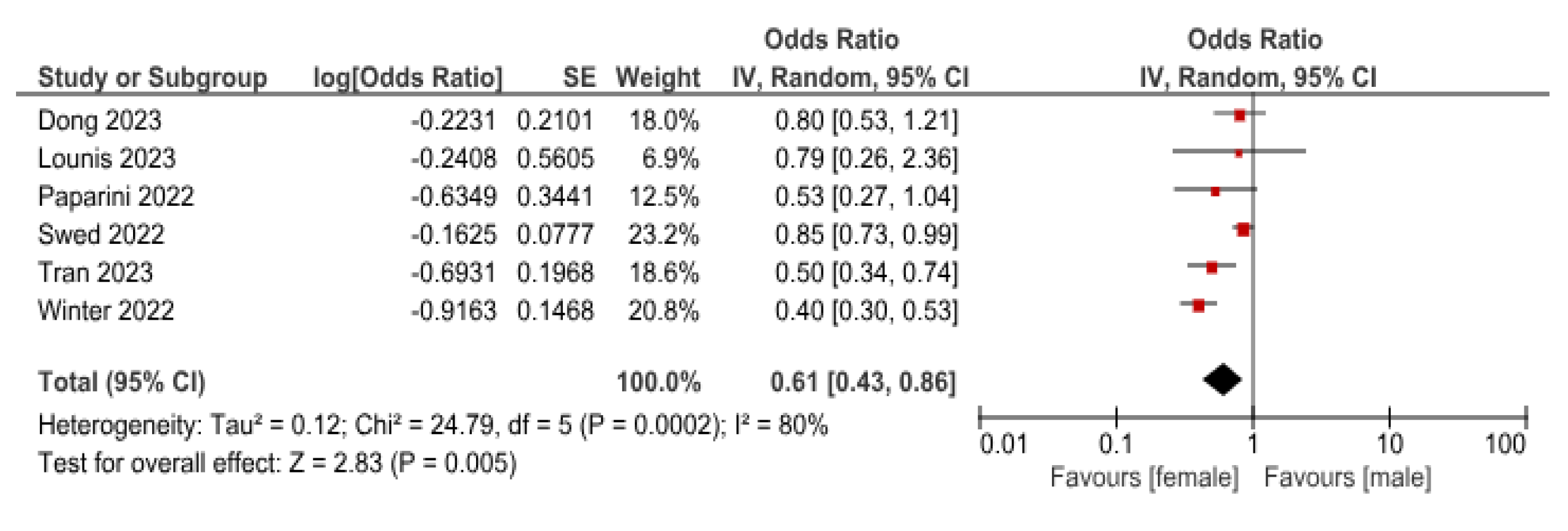
Six studies reported the different genders’ willingness to Mpox vaccine. The pooled OR indicated that females are less willing to receive the vaccine than males, with an OR (0.61 (95%CI, 0.43–0.86)), p = 0.005 (Figure 4).
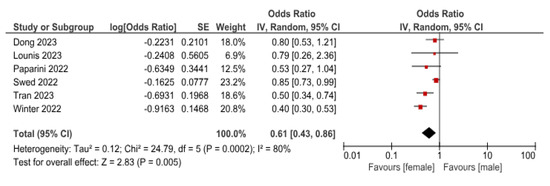
Figure 4.
Comparative analysis of willingness to receive Mpox vaccine between female and male participants. (Red: central value; Black: pooled result 95%CI).
3.6. Homosexual vs. Heterosexual
Two studies reported the frequency of homosexual or heterosexual willingness to receive the vaccine. The pooled OR indicated that homosexuals are more willing to receive the vaccine than heterosexuals with OR (1.44 (95%CI, 1.14–1.80)), p = 0.002 (Figure 5).

Figure 5.
Comparison of willingness to receive Mpox vaccine between homosexual and heterosexual participants. (Red: central value; Black: pooled result 95%CI).
3.7. COVID-19 Vaccinated vs. Unvaccinated
Three studies (n = 898) reported the COVID-19 vaccination status of patients and their willingness to receive the vaccine. The pooled OR indicated that COVID-19-vaccinated patients are more willing to be vaccinated for Mpox than unvaccinated with OR (3.57 (95% CI, 1.89–6.74)), p = 0.0001 (Figure 6).
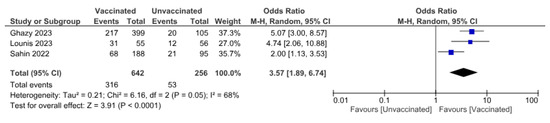
Figure 6.
Association between COVID-19 vaccination status and willingness to receive Mpox vaccine.
3.8. Patients with Chronic Diseases vs. Healthy Patients
Four studies reported patients’ health status and willingness to receive the vaccine. The pooled OR indicated that patients with chronic disease are more willing to receive the vaccine than healthy ones, with an OR (1.07 (95%CI, 1.03–1.11)), p = 0.0009 (Figure 7).
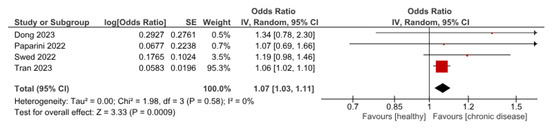
Figure 7.
Influence of chronic diseases on participants’ willingness to receive Mpox vaccine.
3.9. Subgroup Meta-Analysis According to the Population Willingness to Receive Monkeypox Vaccine
Through a subgroup analysis according to the population of the study, we had three different populations: LGBTQ, comprising a total of 38,806 participants, with an 82.2% willingness to take the Mpox vaccine; healthcare workers, comprising a total of 7173, with a 57.5% willingness to receive the Mpox vaccine; and the general population, who comprised a total of 80,224 with a 56.67% willingness to be vaccinated against Mpox (Figure 8).
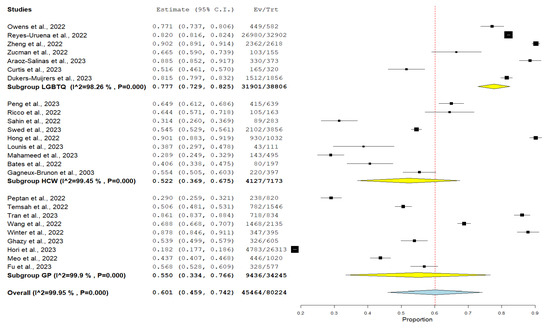
Figure 8.
Subgroup analysis of the participants’ willingness to receive monkeypox vaccine according to their population. (Yellow: subgroup pooled análisis; Blue: general pooled result 95%CI; Red dashed line: pooled central value).
4. Discussion
Vaccination remains integral to public health in infectious disease prevention and control. While vaccine development and distribution present their own scientific and logistical challenges, the success of these efforts is mainly dependent on public acceptance. As seen during the COVID-19 pandemic, vaccine hesitancy, which includes delays in accepting or refusing vaccines despite their availability, poses significant threats to achieving optimal vaccination coverage [41]. In this context, the Mpox vaccine emerges as a contemporary challenge, with low intention to receive vaccines by the general public and HCWs [13,15,42], demanding urgent attention and understanding of public perceptions and acceptance levels to ensure timely prevention and educational intervention.
As reported by the WHO, it is evident that the dynamics of Mpox transmission are undergoing significant shifts. Historically endemic to West or Central Africa [43], the re-emergence of the virus in Nigeria in 2017 underscored the potential for resurgence and inter-human transmission within familiar territories. However, the sudden rise in Mpox cases in Europe by May 2022, an area previously unaffected, led to swift governmental actions, encompassing an extensive educational paradigm and an expedited vaccine dissemination strategy [44]. A previous systematic review [45] reveals differences in Mpox vaccination acceptance across various geographical regions. Over half of the 8045 participants (56.0%) indicated acceptance of the vaccine, with European countries exhibiting higher acceptance rates at 70.0% compared to Asian countries at 50.0%. In our study, the observed 56.14% Mpox vaccine acceptance rate underlines notable geographical variations, with Asia—despite its delayed Mpox incidence—dominating the research landscape at 46.67% (14/30 studies) compared to Europe (7/30, 23.33%), Africa (2/30, 6.67%), North America (4/30, 13.33%), the Middle East (2/30, 6.67%), and South America (1/30, 3.33%). Remarkably, countries like Vietnam [21] and China [17,25] showcased high acceptance rates (>90%), likely influenced by the aftermath of the COVID-19 pandemic. Conversely, persistent low acceptance rates (<30%) in nations such as Romania [23], Japan [18], Pakistan [24], and Jordan [14] highlight the urgent need for tailored public health interventions. Given these disparities, it is evident that both historical experiences with pandemics and regional contexts play pivotal roles in shaping public health attitudes [46,47], necessitating targeted vaccination strategies for each unique setting.
The analysis shows marked disparities among distinct sub-populations. Individuals identifying as homosexuals are 37% [18] and 91% [20] more willing to receive the Mpox vaccine, aligning with previous systematic review outcomes [45]. The trend is arguably anchored in the enduring societal challenges this group confronts, predominantly discrimination and diminished self-worth [48,49]. Grounded in the looking-glass self-theory [50], such experiences contribute to their more empathetic response to communal practices that benefit their community [51]. Additionally, the heightened vulnerability of LGBTQ individuals to both infectious and non-communicable diseases likely augments their adherence to vaccination guidelines [52]. This is in line with our findings that showed that the highest subgroup to be willing to be vaccinated was the LGBTQ subgroup, with an 82.2% willingness rate, compared to healthcare workers (57.5%) and the general population (56.67%). In contrast, females exhibit a reduced acceptance rate of the Mpox vaccine compared to males, lower by a margin of 15% to 60% [12,16,19,21,22,33]. Our research reveals the intricate landscape of vaccine hesitancy in women, particularly among older age groups and pregnant women [53,54,55]. Notably, pregnant women exhibit significantly higher vaccine hesitancy rates [55], influenced by potential side effects and unverified information on social media [55]. These findings suggest a greater vaccine hesitancy among women than men, which could be attributed to their intricate family roles [56,57].
Our findings also indicate a significant correlation between Mpox vaccine acceptance and prior COVID-19 vaccination, with individuals having received COVID-19 vaccines exhibiting a 2- to 5-fold increased likelihood in willingness to accept the Mpox vaccine relative to their non-vaccinated counterparts [13,15,19]. This correlation may be attributable to the pervasive influence of misinformation and conspiracy theories, which have substantially polarised vaccine decision-making from cautious endorsement to outright refusal [58,59,60]. The proliferation of unfounded information and spurious claims regarding SARS-CoV-2 vaccines on digital platforms has undermined public trust even before the authorisation of efficacious vaccines [60]. This erosion in trust has engendered a marked polarisation in vaccination perspectives, with 4% to 7% of respondents in COVID-19 surveys expressing opposition to vaccination, aligning closely with our observed Mpox vaccine rejection rate of 4.5% [61].
Other socioeconomic factors such as marital status, social income, and educational level may have some influence on the willingness to be vaccinated [62]. However, this was not clearly described in the included studies, with a huge difference in age groups, marital status subdivisions, different educational levels, and social income levels.
Furthermore, results suggest a higher willingness to receive the Mpox vaccine among individuals with underlying conditions [12,16,21,33]. People with chronic illnesses often experience heightened health-related fear and anxiety, which could lead to adverse mental effects [63,64]. This proactive seeking of disease prevention methods, driven by such concerns, could account for the higher acceptance of Mpox vaccines among individuals with chronic conditions, as they view vaccination as a constructive approach [65,66]. Additionally, recommendations for regular vaccination to mitigate complications in individuals with chronic illnesses could further promote vaccine acceptance in this group [67].
The FDA has approved two paramount vaccines for Mpox prevention: JYNNEOS (Imvamune/Imvanex) and ACAM2000 (Dryvax). The safety profiles of these vaccines are commendable, predominantly presenting minor side effects such as localised pain, redness, and swelling. Notably, in light of the persistent Mpox outbreak, the FDA, in August 2022, expanded the emergency use authorisation for JYNNEOS to include individuals aged 18 years and below [68].
Our findings underscore the imperative for national and regional bodies to intensify educational campaigns, particularly leveraging social and news media platforms pivotal in disseminating credible vaccine information [69]. The results of this systematic review and meta-analysis contribute significantly to the global measures adopted for Mpox vaccination and public health policy formulation, specifically targeting sub-populations with documented lower acceptance rates for the Mpox vaccine. Furthermore, in the face of future outbreaks, these insights could facilitate identifying and stratifying demographics resistant to vaccination, enabling tailored interventions for these particular cohorts [69,70].
We can emphasise the significance of this meta-analysis by shedding light on vaccine hesitancy, highlighting its prevalence and disparities across demographic groups. Its novelty originates from its investigation of Mpox vaccination attitudes in relation to gender, sexual orientation, and COVID-19 vaccination status, which provides new insights into these domains. However, several limitations remain. All included studies are cross-sectional studies with differences in the methodologies and tools for measurement, which might introduce heterogeneity and affect the findings’ potential to be generalised. Moreover, several confounding variables, such as population differences, exist in every study that produces heterogeneous results. Most of the included studies are single-centred ones. There are definitely many people who are vaccine ambivalent; however, this was not clearly described in the included studies as they only mentioned the willingness or refusal to receive Mpox vaccine. Therefore, this may produce some sort of bias. We recommend further multi-centre studies to assess the willingness of Mpox vaccination. Future awareness campaigns are needed to illustrate the importance of vaccination against Mpox to overcome the occurrence of another pandemic. Media coverage, political situation, or previous experiences with vaccination campaigns can have a significant impact on vaccination decisions and change the minds of those thinking that the vaccination would cause harm [70,71]. This was previously proven by Cascini et al. [72] who noted that social media and other media platforms can be used as a forum for public health interventions and as a source of data to guide policy decisions aimed at addressing vaccine hesitancy and advancing vaccination rates across the globe. It is crucial to raise vaccination rates in order to establish herd immunity among community members [73]. As studies are evolving, similar to our results (56.14%, were willing to vaccinate against mpox), a previous meta-analysis found that the figure was 56.0% [45]. Improving acceptance for monkeypox vaccination involves addressing various factors, including education, communication, community engagement, and building trust.
5. Conclusions
This meta-analysis has advanced our understanding of public attitudes towards Mpox vaccination by highlighting disparities and key factors influencing it. While providing useful insights, it also serves as a starting point for future research aimed at developing more effective communication strategies and ensuring equitable vaccine coverage in the light of changing socio-cultural and health contexts.
Author Contributions
Conceptualisation, methodology, project administration: A.M.T.; Formal analysis and investigation: M.H.-E.M.; Data curation: W.A.E.-T.M., M.A., Y.A.M. and E.H. Writing—original draft preparation: D.N., M.A., Y.A.M., D.K.B.-A. and A.J.R.-M.; Writing—review and editing: A.M.T., D.K.B.-A. and A.J.R.-M. All authors participated in the interpretation of data for the work; and final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have read and agreed to the published version of the manuscript.
Funding
Universidad Continental covered the APCs of this publication.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors have no conflict of interest to declare. Dr. Wesam Abd El-Tawab Moawad is affiliated with Al-Azhar University and MARS Global, but the data in the paper has not been disputed or altered as consequence of this affiliation.
References
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef]
- Patel, M.; Adnan, M.; Aldarhami, A.; Bazaid, A.S.; Saeedi, N.H.; Alkayyal, A.A.; Saleh, F.M.; Awadh, I.B.; Saeed, A.; Alshaghdali, K. Current Insights into Diagnosis, Prevention Strategies, Treatment, Therapeutic Targets, and Challenges of Monkeypox (Mpox) Infections in Human Populations. Life 2023, 13, 249. [Google Scholar] [CrossRef]
- Farasani, A. Monkeypox virus: Future role in Human population. J. Infect. Public Health 2022, 15, 1270–1275. [Google Scholar] [CrossRef]
- Kabuga, A.I.; El Zowalaty, M.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med. Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef]
- Reynolds, M.G.; Yorita, K.L.; Kuehnert, M.J.; Davidson, W.B.; Huhn, G.D.; Holman, R.C.; Damon, I.K. Clinical Manifestations of Human Monkeypox Influenced by Route of Infection. J. Infect. Dis. 2006, 194, 773–780. [Google Scholar] [CrossRef]
- Yang, J.Z. Comparative risk perception of the monkeypox outbreak and the monkeypox vaccine. Risk Anal. 2023. ahead of print. [Google Scholar] [CrossRef]
- Girometti, N.; Byrne, R.; Bracchi, M.; Heskin, J.; McOwan, A.; Tittle, V.; Gedela, K.; Scott, C.; Patel, S.; Gohil, J.; et al. Demographic and clinical characteristics of confirmed human monkeypox virus cases in individuals attending a sexual health centre in London, UK: An observational analysis. Lancet Infect. Dis. 2022, 22, 1321–1328. [Google Scholar] [CrossRef]
- Guarner, J.; del Rio, C.; Malani, P.N. Monkeypox in 2022—What Clinicians Need to Know. JAMA 2022, 328, 139–140. [Google Scholar] [CrossRef]
- Nuzzo, J.B.; Borio, L.L.; Gostin, L.O. The WHO Declaration of Monkeypox as a Global Public Health Emergency. JAMA 2022, 328, 615–616. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Wells, G.; Wells, G.; Shea, B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch; Losos, M.; Tugwell, P.; Ga, S.W.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2014. Available online: https://www.semanticscholar.org/paper/The-Newcastle-Ottawa-Scale-(NOS)-for-Assessing-the-Wells-Wells/c293fb316b6176154c3fdbb8340a107d9c8c82bf#citing-papers (accessed on 20 September 2023).
- Dong, C.; Yu, Z.; Zhao, Y.; Ma, X. Knowledge and vaccination intention of monkeypox in China’s general population: A cross-sectional online survey. Travel. Med. Infect. Dis. 2023, 52, 102533. [Google Scholar] [CrossRef]
- Ghazy, R.M.; Yazbek, S.; Gebreal, A.; Hussein, M.; Addai, S.A.; Mensah, E.; Sarfo, M.; Kofi, A.; Al-Ahdal, T.; Eshun, G. Monkeypox Vaccine Acceptance among Ghanaians: A Call for Action. Vaccines 2023, 11, 240. [Google Scholar] [CrossRef]
- Mahameed, H.; Al-Mahzoum, K.; AlRaie, L.A.; Aburumman, R.; Al-Naimat, H.; Alhiary, S.; Barakat, M.; Al-Tammemi, A.B.; Salim, N.A.; Sallam, M. Previous Vaccination History and Psychological Factors as Significant Predictors of Willingness to Receive Mpox Vaccination and a Favorable Attitude towards Compulsory Vaccination. Vaccines 2023, 11, 897. [Google Scholar] [CrossRef]
- Sahin, T.K.; Erul, E.; Aksun, M.S.; Sonmezer, M.C.; Unal, S.; Akova, M. Knowledge and Attitudes of Turkish Physicians towards Human Monkeypox Disease and Related Vaccination: A Cross-Sectional Study. Vaccines 2022, 11, 19. [Google Scholar] [CrossRef]
- Swed, S.; Bohsas, H.; Alibrahim, H.; Rakab, A.; Hafez, W.; Sawaf, B.; Amir, R.M.; Motawei, A.S.; Aljabali, A.; Shoib, S.; et al. Monkeypox Post-COVID-19: Knowledge, Worrying, and Vaccine Adoption in the Arabic General Population. Vaccines 2023, 11, 759. [Google Scholar] [CrossRef]
- Zheng, M.; Qin, C.; Qian, X.; Yao, Y.; Liu, J.; Yuan, Z.; Ma, L.; Fan, J.; Tao, R.; Zhou, F.; et al. Knowledge and vaccination acceptance toward the human monkeypox among men who have sex with men in China. Front. Public Health 2022, 10, 997637. [Google Scholar] [CrossRef]
- Hori, D.; Kaneda, Y.; Ozaki, A.; Tabuchi, T. Sexual orientation was associated with intention to be vaccinated with a smallpox vaccine against mpox: A cross-sectional preliminary survey in Japan. Vaccine 2023, 41, 3954–3959. [Google Scholar] [CrossRef]
- Lounis, M.; Bencherit, D.; Abdelhadi, S. Knowledge and awareness of Algerian healthcare workers about human monkeypox and their attitude toward its vaccination: An online cross-sectional survey. Vacunas 2023, 24, 122–127. [Google Scholar] [CrossRef]
- Owens, C.; Hubach, R.D. Rural-urban differences in monkeypox behaviors and attitudes among men who have sex with men in the United States. J. Rural Health 2023, 39, 508–515. [Google Scholar] [CrossRef]
- Tran, B.X.; Do, L.A.; Hoang, T.P.; Boyer, L.; Auquier, P.; Fond, G.; Le, H.T.; Le Vu, M.N.; Dang, T.H.T.; Nguyen, A.H.T.; et al. Crucial choices in a global health crisis: Revealing the demand and willingness to pay for a hypothetical monkeypox vaccine—The PREVENT study. J. Glob. Health 2023, 13, 04033. [Google Scholar] [CrossRef]
- Winters, M.; Malik, A.A.; Omer, S.B. Attitudes towards Monkeypox vaccination and predictors of vaccination intentions among the US general public. PLoS ONE 2022, 17, e0278622. [Google Scholar] [CrossRef] [PubMed]
- Peptan, C.; Băleanu, V.D.; Mărcău, F.C. Study on the Vaccination of the Population of Romania against Monkeypox in Terms of Medical Security. Vaccines 2022, 10, 1834. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Ahmed, F.; Raza, M.S.; Rajpoot, P.L.; Rehman, W.; Alam Khatri, S.; Mohammed, M.; Muhammad, S.; Ahmad, R. Monkeypox Cross-Sectional Survey of Knowledge, Attitudes, Practices, and Willingness to Vaccinate among University Students in Pakistan. Vaccines 2022, 11, 97. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Pan, B.; Jiang, H.; Zhang, Q.; Xu, X.; Jiang, H.; Ye, J.; Cui, Y.; Yan, X.; Zhai, X.; et al. The willingness of Chinese healthcare workers to receive monkeypox vaccine and its independent predictors: A cross-sectional survey. J. Med. Virol. 2023, 95, e28294. [Google Scholar] [CrossRef] [PubMed]
- Araoz-Salinas, J.M.; Ortiz-Saavedra, B.; Ponce-Rosas, L.; Soriano-Moreno, D.R.; Soriano-Moreno, A.N.; Alave, J.; Gonzales-Zamora, J.A. Perceptions and Intention to Get Vaccinated against Mpox among the LGBTIQ+ Community during the 2022 Outbreak: A Cross-Sectional Study in Peru. Vaccines 2023, 11, 1008. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Grijalva, M.J. Knowledge, attitudes, and practices towards monkeypox during the 2022 outbreak: An online cross-sectional survey among clinicians in Ohio, USA. J. Infect. Public Health 2022, 15, 1459–1465. [Google Scholar] [CrossRef]
- Chen, Y.; Li, Y.; Fu, L.; Zhou, X.; Wu, X.; Wang, B.; Peng, X.; Sun, Y.; Liu, Q.; Lin, Y.-F.; et al. Knowledge of Human Mpox (Monkeypox) and Attitude towards Mpox Vaccination among Male Sex Workers in China: A Cross-Sectional Study. Vaccines 2023, 11, 285. [Google Scholar] [CrossRef]
- Curtis, M.G.; Davoudpour, S.; Rodriguez-Ortiz, A.E.; Felt, D.; French, A.L.; Hosek, S.G.; Phillips, G.; Serrano, P.A. Predictors of Mpox vaccine uptake among sexual and gender minority young adults living in Illinois: Unvaccinated vs. double vs. single dose vaccine recipients. Vaccine 2023, 41, 4002–4008. [Google Scholar] [CrossRef]
- Dukers-Muijrers, N.H.T.M.; Evers, Y.; Widdershoven, V.; Davidovich, U.; Adam, P.C.G.; de Coul, E.L.M.O.; Zantkuijl, P.; Matser, A.; Prins, M.; de Vries, H.J.C.; et al. Mpox vaccination willingness, determinants, and communication needs in gay, bisexual, and other men who have sex with men, in the context of limited vaccine availability in the Netherlands (Dutch Mpox-survey). Front. Public Health 2022, 10, 1058807. [Google Scholar] [CrossRef]
- Fu, L.; Sun, Y.; Li, Y.; Wang, B.; Yang, L.; Tian, T.; Wu, X.; Peng, X.; Liu, Q.; Chen, Y.; et al. Perception of and Vaccine Readiness towards Mpox among Men Who Have Sex with Men Living with HIV in China: A Cross-Sectional Study. Vaccines 2023, 11, 528. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Dauby, N.; Launay, O.; Botelho-Nevers, E. Attitudes towards monkeypox vaccination among healthcare workers in France and Belgium: An element of complacency? J. Hosp. Infect. 2022, 130, 144–145. [Google Scholar] [CrossRef] [PubMed]
- Paparini, S.; Whitacre, R.; Smuk, M.; Thornhill, J.; Mwendera, C.; Strachan, S.; Nutland, W.; Orkin, C. Public understanding and awareness of and response to monkeypox virus outbreak: A cross-sectional survey of the most affected communities in the United Kingdom during the 2022 public health emergency. HIV Med. 2023, 24, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Al-Khlaiwi, T.; Aljofan, Z.F.; Alanazi, A.I.; Meo, A.S. Public Perceptions of the Emerging Human Monkeypox Disease and Vaccination in Riyadh, Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 1534. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Wang, B.; Li, Y.; Chen, Y.; Wu, X.; Fu, L.; Sun, Y.; Liu, Q.; Lin, Y.-F.; Liang, B.; et al. Perceptions and worries about monkeypox, and attitudes towards monkeypox vaccination among medical workers in China: A cross-sectional survey. J. Infect. Public Health 2023, 16, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Urueña, J.; D’Ambrosio, A.; Croci, R.; Bluemel, B.; Cenciarelli, O.; Pharris, A.; Dukers-Muijrers, N.; Nutland, W.; Niaupari, S.; Badran, J.; et al. High monkeypox vaccine acceptance among male users of smartphone-based online gay-dating apps in Europe, 30 July to 12 August 2022. Eurosurveillance 2022, 27, 2200757. [Google Scholar] [CrossRef] [PubMed]
- Swed, S.; Alibrahim, H.; Bohsas, H.; Jawish, N.; Rais, M.A.; Nasif, M.N.; Hafez, W.; Sawaf, B.; Abdelrahman, A.; Fathey, S.; et al. A multinational cross-sectional study on the awareness and concerns of healthcare providers toward monkeypox and the promotion of the monkeypox vaccination. Front. Public Health 2023, 11, 1153136. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Aljamaan, F.; Alenezi, S.; Alhasan, K.; Saddik, B.; Al-Barag, A.; Alhaboob, A.; Bahabri, N.; Alshahrani, F.; Alrabiaah, A.; et al. Monkeypox caused less worry than COVID-19 among the general population during the first month of the WHO Monkeypox alert: Experience from Saudi Arabia. Travel. Med. Infect. Dis. 2022, 49, 102426. [Google Scholar] [CrossRef]
- Wang, B.; Peng, X.; Li, Y.; Fu, L.; Tian, T.; Liang, B.; Sun, Y.; Chen, Y.; Wu, X.; Liu, Q.; et al. Perceptions, precautions, and vaccine acceptance related to monkeypox in the public in China: A cross-sectional survey. J. Infect. Public Health 2023, 16, 163–170. [Google Scholar] [CrossRef]
- Zucman, D.; Fourn, E.; Touche, P.; Majerholc, C.; Vallée, A. Monkeypox Vaccine Hesitancy in French Men Having Sex with Men with PrEP or Living with HIV in France. Vaccines 2022, 10, 1629. [Google Scholar] [CrossRef]
- Rajkhowa, P.; Dsouza, V.S.; Kharel, R.; Cauvery, K.; Mallya, B.R.; Raksha, D.S.; Mrinalini, V.; Sharma, P.; Pattanshetty, S.; Narayanan, P.; et al. Factors Influencing Monkeypox Vaccination: A Cue to Policy Implementation. J. Epidemiol. Glob. Health 2023, 13, 226–238. [Google Scholar] [CrossRef]
- Rana, J.; Patel, S.K.; Agrawal, A.; Channabasappa, N.K.; Niranjan, A.K.; Das, B.C.; Pandey, M.K.; Tiwari, S.P.; Gaihre, M. Mpox vaccination in global perspective: Priorities and challenges. Ann. Med. Surg. 2023, 85, 2243–2246. [Google Scholar]
- Banuet-Martinez, M.; Yang, Y.; Jafari, B.; Kaur, A.; Butt, Z.A.; Chen, H.H.; Yanushkevich, S.; Moyles, I.R.; Heffernan, J.M.; Korosec, C.S. Monkeypox: A review of epidemiological modelling studies and how modelling has led to mechanistic insight. Epidemiol. Infect. 2023, 151, 1–44. [Google Scholar] [CrossRef] [PubMed]
- Aden, D.; Zaheer, S.; Kumar, R.; Ranga, S. Monkeypox (Mpox) outbreak during COVID-19 pandemic-Past and the future. J. Med. Virol. 2023, 95, e28701. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Alarcón-Braga, E.A.; Hernandez-Bustamante, E.A.; Al-kassab-Córdova, A.; Benites-Zapata, V.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Acceptance towards Monkeypox Vaccination: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 1248. [Google Scholar] [CrossRef] [PubMed]
- Filip, R.; Puscaselu, R.G.; Anchidin-Norocel, L.; Dimian, M.; Savage, W.K. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J. Pers. Med. 2022, 12, 1295. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Leigh, J.P.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 13, 3801. [Google Scholar] [CrossRef]
- Everett, B.G.; Onge, J.S.; Mollborn, S. Effects of Minority Status and Perceived Discrimination on Mental Health. Popul. Res. Policy Rev. 2016, 35, 445–469. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority Stress and Mental Health in Gay Men. J. Health Soc. Behav. 1995, 36, 38–56. [Google Scholar] [CrossRef]
- Crocker, J. Social Stigma and Self-Esteem: Situational Construction of Self-Worth. J. Exp. Soc. Psychol. 1999, 35, 89–107. [Google Scholar] [CrossRef]
- Saarinen, A.; Keltikangas-Järvinen, L.; Ravaja, N. Ethnicity, minority status, and inter-group bias: A systematic meta-analysis on fMRI studies. Front. Hum. Neurosci. 2022, 16, 1072345. [Google Scholar] [CrossRef]
- Phillips, G., II; Felt, D.; Ruprecht, M.M.; Wang, X.; Xu, J.; Pérez-Bill, E.; Bagnarol, R.M.; Roth, J.; Curry, C.W.; Beach, L.B. Addressing the Disproportionate Impacts of the COVID-19 Pandemic on Sexual and Gender Minority Populations in the United States: Actions Toward Equity. LGBT Health 2020, 7, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Terry, E.; Cartledge, S.; Damery, S.; Greenfield, S. Factors associated with COVID-19 vaccine intentions during the COVID-19 pandemic; a systematic review and meta-analysis of cross-sectional studies. BMC Public Health 2022, 22, 1667. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. Widespread Misinformation About Infertility Continues to Create COVID-19 Vaccine Hesitancy. JAMA 2022, 327, 1013–1015. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, O.; Siddiquea, B.N.; Shetty, A.; Afroz, A.; Billah, B. COVID-19 vaccine hesitancy among pregnant women: A systematic review and meta-analysis. BMJ Open 2022, 12, e061477. [Google Scholar] [CrossRef]
- Morales, D.X.; Beltran, T.F.; Morales, S.A. Gender, socioeconomic status, and COVID-19 vaccine hesitancy in the US: An intersectionality approach. Sociol. Health Illn. 2022, 44, 953–971. [Google Scholar] [CrossRef]
- Oliver, J.; Kaufman, J.; Bagot, K.; Bradfield, Z.; Homer, C.; Gibney, K.; Danchin, M. Drivers of COVID-19 vaccine hesitancy among women of childbearing age in Victoria, Australia: A descriptive qualitative study. Vaccine X 2022, 12, 100240. [Google Scholar] [CrossRef]
- Dunn, A.G.; Surian, D.; Leask, J.; Dey, A.; Mandl, K.D.; Coiera, E. Mapping information exposure on social media to explain differences in HPV vaccine coverage in the United States. Vaccine 2017, 35, 3033–3040. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Wilson, K.; Atkinson, K.; Deeks, S. Opportunities for utilizing new technologies to increase vaccine confidence. Expert. Rev. Vaccines 2014, 13, 969–977. [Google Scholar] [CrossRef]
- Donovan, J. Social-media companies must flatten the curve of misinformation. Nature 2020. ahead of print. [Google Scholar] [CrossRef]
- Islam, M.R.; Haque, M.A.; Ahamed, B.; Tanbir, M.; Khan, M.R.; Eqbal, S.; Rahman, A.; Shariar, M.; Bhuiyan, M.A. Assessment of vaccine perception and vaccination intention of Mpox infection among the adult males in Bangladesh: A cross-sectional study findings. PLoS ONE 2023, 18, e0286322. [Google Scholar] [CrossRef] [PubMed]
- Lebel, S.; Mutsaers, B.; Tomei, C.; Leclair, C.S.; Jones, G.; Petricone-Westwood, D.; Rutkowski, N.; Ta, V.; Trudel, G.; Laflamme, S.Z.; et al. Health anxiety and illness-related fears across diverse chronic illnesses: A systematic review on conceptualization, measurement, prevalence, course, and correlates. PLoS ONE 2020, 15, e0234124. [Google Scholar] [CrossRef] [PubMed]
- Zvolensky, M.J.; Eifert, G.H.; Feldner, M.T.; Leen-Feldner, E. Heart-focused anxiety and chest pain in postangiography medical patients. J. Behav. Med. 2003, 26, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Tegegne, M.D.; Girma, S.; Mengistu, S.; Mesfin, T.; Adugna, T.; Kokeb, M.; Melese, E.B.; Worku, Y.B.; Wubante, S.M. Willingness to receive COVID-19 vaccine and associated factors among adult chronic patients. A cross-sectional study in Northwest Ethiopia. PLoS ONE 2022, 17, e0269942. [Google Scholar] [CrossRef]
- Angelo, A.T.; Alemayehu, D.S.; Dachew, A.M. Health care workers intention to accept COVID-19 vaccine and associated factors in southwestern Ethiopia, 2021. PLoS ONE 2021, 16, e0257109. [Google Scholar] [CrossRef]
- Smith, K. Vaccines and Chronic Disease. Del. J. Public Health 2017, 3, 46–52. [Google Scholar] [CrossRef]
- Sah, R.; Humayun, M.; Baig, E.; Farooq, M.; Hussain, H.G.; Shahid, M.U.; Cheema, H.A.; Chandran, D.; Yatoo, M.I.; Sharma, A.K.; et al. FDA’s authorized “JYNNEOS” vaccine for counteracting monkeypox global public health emergency; an update—Correspondence. Int. J. Surg. 2022, 107, 106971. [Google Scholar] [CrossRef]
- Limaye, R.J.; Holroyd, T.A.; Blunt, M.; Jamison, A.F.; Sauer, M.; Weeks, R.; Wahl, B.; Christenson, K.; Smith, C.; Minchin, J.; et al. Social media strategies to affect vaccine acceptance: A systematic literature review. Expert. Rev. Vaccines 2021, 20, 959–973. [Google Scholar] [CrossRef]
- Albrecht, D. Vaccination, politics and COVID-19 impacts. BMC Public Health 2022, 22, 96. [Google Scholar] [CrossRef]
- Kevin, B.; de Figueiredo, A.; Rachel, G.-A.; Euzebiusz, J.; James, D.; Trudo, L.; Keshavjee, S.; Graham, J.E.; Baral, S. The unintended consequences of COVID-19 vaccine policy: Why mandates, passports and restrictions may cause more harm than good. BMJ Global Health 2022, 7, e008684. [Google Scholar]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.A.; Failla, G.; Puleo, V.; Melnyk, A.; Lontano, A.; Ricciardi, W. Social media and attitudes towards a COVID-19 vaccination: A systematic review of the literature. EClinicalMedicine 2022, 48, 101454. [Google Scholar] [CrossRef] [PubMed]
- Plans-Rubió, P. Percentages of Vaccination Coverage Required to Establish Herd Immunity against SARS-CoV-2. Vaccines 2022, 10, 736. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).