

COVID-19 Vaccination Hesitancy among Youths in Soweto, South Africa
 , , ,
, , ,
Abstract
1. Introduction
2. Methodology
2.1. Study Design and Setting
2.2. Description of Variables
2.2.1. Dependent Variables
2.2.2. Independent Variables
2.3. Sample Size Determination
2.4. Ethics Clearance
2.5. Inclusion and Exclusion Criteria
2.6. Targeting Participants
2.7. Consenting
2.8. Data Management
2.9. Statistical Methods
3. Results
3.1. Demographic Social Characteristics of the Study Sample
Social Demographics and Vaccine Hesitancy
3.2. Attitudes towards COVID-19 Disease and Vaccines
3.2.1. If a Teacher Is COVID-19 Positive, They Should Be Allowed to Continue Teaching
3.2.2. I Prefer to Break Physical Contact with People Living with COVID-19
3.2.3. It Is Better to Develop Immunity by Getting Sick Rather than by Getting a Vaccine
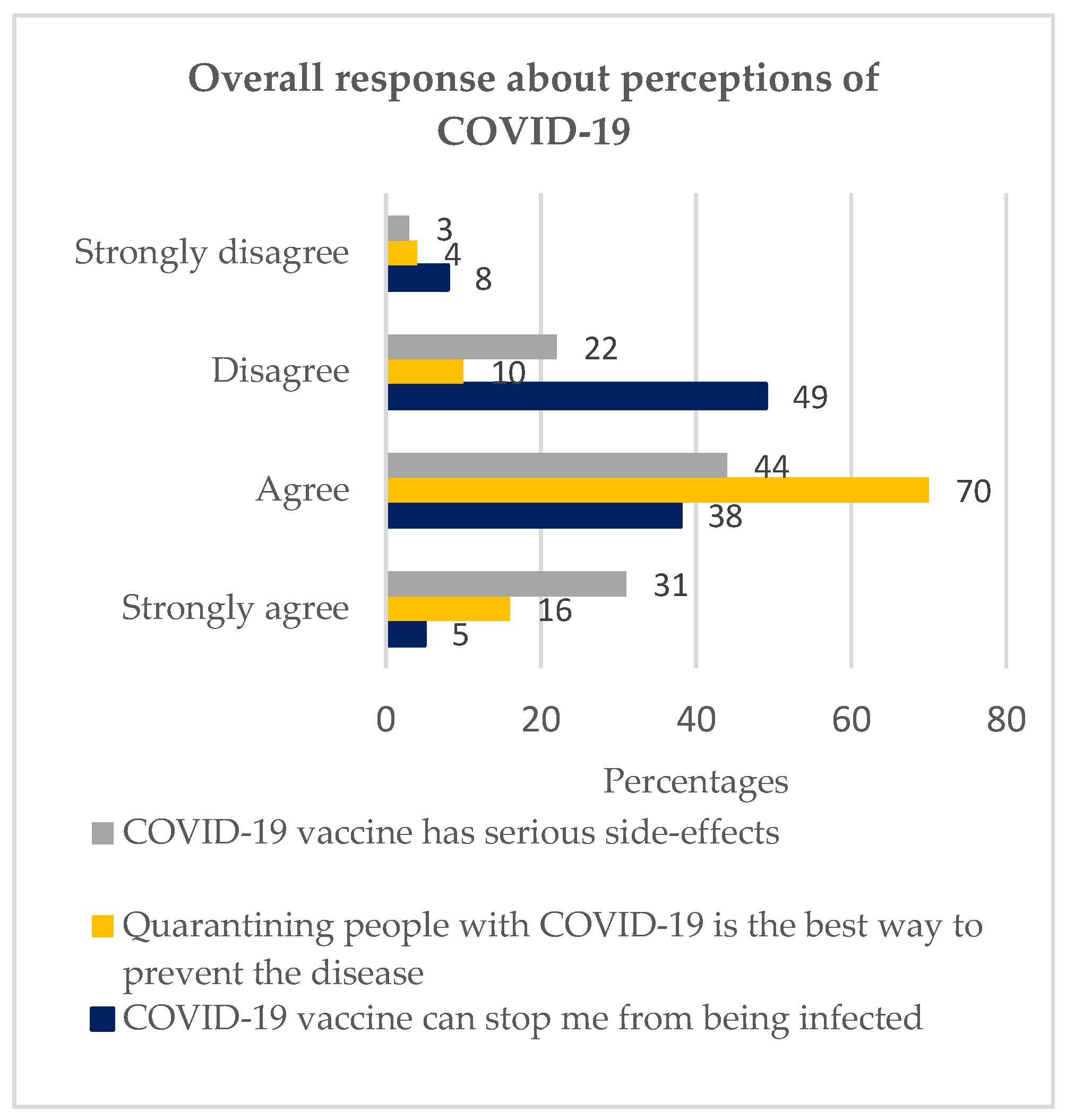
3.3. Perceptions of COVID-19
3.3.1. I Believe That the COVID-19 Vaccine Can Stop Me from Being Infected
3.3.2. Quarantining People with COVID-19 Is the Best Way to Prevent the Disease
3.3.3. COVID-19 Vaccine Has Serious Side-Effects
4. Discussion
5. Conclusions
5.1. Study Strengths
- This is the first study to highlight vaccine apprehension in Soweto among the youths.
- The quantitative study design embraced a larger population, hence highlighting the solid state of the attitudes and perceptions on the COVID-19 vaccine.
- The study design objectively and accurately brought out the levels of attitudes and perceptions of COVID-19 vaccines that correlate with vaccine hesitancy.
- The study uniquely depicted the different levels of COVID-19 vaccine hesitancy based on the responses received.
5.2. Study Limitations
- The quantitative study design was limited to giving reasons behind negative attitudes and poor perceptions,
- The study did not capture the vaccination status of the participants. However, most youths were obliged to vaccinate due to mandatory vaccination policy in schools and corporate environments [30].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous signs in COVID-19 patients: A review. Dermatol. Ther. 2020, 33, 5. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.Y.; Thone, M.N.; Kwon, Y.J. COVID-19 vaccines: The status and perspectives in delivery points of view. Adv. Drug Deliv. Rev. 2021, 170, 1–25. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 March 2023).
- South African Statistics. SA Population Reaches 58.8 Million. 2019. Available online: https://www.statssa.gov.za/?p=12362 (accessed on 20 March 2023).
- El-Elimat, T.; AbuAlSamen, M.M.; Almomani, B.A.; Al-Sawalha, N.A.; Alali, F.Q. Acceptance and attitudes toward COVID-19 vaccines: A cross-sectional study from Jordan. PLoS ONE 2021, 16, e0250555. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Centre, I.A. A Brief History of Vaccination. 2020. Available online: https://www.immune.org.nz/vaccines/vaccine-development/brief-history-vaccination (accessed on 10 January 2023).
- Hussein, I.E.; Echams, N.; Echams, S.; Sayegh, S.E.; Badran, R.; Eraad, M.; Egerges-Geagea, A.; Eleone, A.; Ejurjus, A. Vaccines Through Centuries: Major Cornerstones of Global Health. Front. Public Health 2015, 3, 269. [Google Scholar] [CrossRef]
- GAVI. There Are Four Types of COVID-19 Vaccines: Here’s How They Work. 2020. Available online: https://www.gavi.org/vaccineswork/there-are-four-types-covid-19-vaccines-heres-how-they-work?gclid=Cj0KCQjw1tGUBhDXARIsAIJx01nD5DN6MAM18M-pTk-MnaUH5szKCDoYxXOk_PP1xy70YuQ7-M0yd4UaAvrAEALw_wcB (accessed on 3 February 2023).
- Statistics, D.S. Stat SA. Available online: http://www.statssa.gov.za/?page_id=4286&id=11317 (accessed on 3 April 2023).
- Cooper, S.; van Rooyen, H.; Wiysonge, C.S. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert Rev. Vaccines 2021, 20, 921–933. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Behavioural Considerations for Acceptance and Uptake of COVID-19 Vaccines; World Health Organization: Geneva, Switzerland, 2020; p. 18. [Google Scholar]
- Ateghang-Awankem, B.; DeLuca, L.; Shadzeka, E.; Anchang, K.Y. Good Participatory Practice, Clinical Trials Awareness and COVID-19 Vaccine Acceptance in Sub-Sahara Africa. Am. J. Public Health Res. 2021, 9, 90–95. [Google Scholar] [CrossRef]
- Millán, D.L.M.; Carrión-Nessi, F.S.; Bernard, M.D.M.; Marcano-Rojas, M.V.; Ávila, D.O.; Fernández, J.M.D.; Labrador, F.R.C.; Rodríguez, A.Q.; Vega, S.G.; Tami, A.; et al. Knowledge, Attitudes, and Practices Regarding COVID-19 among Healthcare Workers in Venezuela: An Online Cross-Sectional Survey. Front. Public Health 2021, 9, 633723. [Google Scholar] [CrossRef]
- Varghese, G.M.; John, R.; Manesh, A.; Karthik, R.; Abraham, O.C. Clinical management of COVID-19. Indian J. Med. Res. 2018, 151, 517–520. [Google Scholar] [CrossRef]
- Kollamparambil, U.; Oyenubi, A. Behavioural response to the Covid-19 pandemic in South Africa. PLoS ONE 2021, 16, e0250269. [Google Scholar] [CrossRef]
- Afifi, T.O.; Salmon, S.; Taillieu, T.; Stewart-Tufescu, A.; Fortier, J.; Driedger, S.M. Older adolescents and young adults willingness to receive the COVID-19 vaccine: Implications for informing public health strategies. Vaccine 2021, 39, 3473–3479. [Google Scholar] [CrossRef] [PubMed]
- Kabamba Nzaji, M.; Kabamba Ngombe, L.; Ngoie Mwamba, G.; Banza Ndala, D.B.; Mbidi Miema, J.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmatic Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Olum, R.; Chekwech, G.; Wekha, G.; Nassozi, D.R.; Bongomin, F. Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals, Uganda. Front. Public Health 2020, 8, 181. [Google Scholar] [CrossRef] [PubMed]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, attitudes, and perceptions of COVID-19 vaccine and refusal to receive COVID-19 vaccine among healthcare workers in northeastern Ethiopia. BMC Public Health 2022, 22, 1–14. [Google Scholar] [CrossRef]
- WHO. Effective Vaccine Management. 2013. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/supply-chain/effective-vaccine-management-(evm) (accessed on 29 November 2021).
- South African Statistics. South African Government’s Handling of COVID-19: Study Shows Declining Trust. The Conversation. 2021. Available online: https://theconversation.com/south-african-governments-handling-of-covid-19-study-shows-declining-trust-163372 (accessed on 19 October 2021).
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel—Implications for vaccination implementation policies. Isr. J. Health Policy Res. 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Stata. Stata User’s Guide, Statistica; A Stata Press Publication: College Station, TX, USA, 2013; Volume 13. [Google Scholar]
- Steenberg, B.; Myburgh, N.; Sokani, A.; Ngwenya, N.; Mutevedzi, P.; Madhi, S.A. COVID-19 Vaccination Rollout: Aspects of Acceptability in South Africa. Vaccines 2022, 10, 1379. [Google Scholar] [CrossRef]
- Khan, M.S.R.; Watanapongvanich, S.; Kadoya, Y. COVID-19 Vaccine Hesitancy among the Younger Generation in Japan. Int. J. Environ. Res. Public Health 2021, 18, 11702. [Google Scholar] [CrossRef]
- Mahmoud, M.; Alanazi, M.M.; Albarrak, M.S.; Aljarba, N.K.; Almutairi, N.G. The Percentage of Vaccine Hesitancy among Married Individuals in Times of the COVID-19 Pandemic: A Cross Sectional Study in Riyadh City, Kingdom of Saudi Arabia. Saudi J. Heal. Syst. Res. 2021, 2, 20–26. [Google Scholar] [CrossRef]
- Estrela, M.; Silva, T.M.; Roque, V.; Gomes, E.R.; Figueiras, A.; Roque, F.; Herdeiro, M.T. Unravelling the drivers behind COVID-19 vaccination hesitancy and refusal among teachers: A nationwide study. Vaccine 2020, 40, 5464–5470. [Google Scholar] [CrossRef]
- Watermeyer, J.; Scott, M.; Kapueja, L.; Ware, L.J. To trust or not to trust: An exploratory qualitative study of personal and community perceptions of vaccines amongst a group of young community healthcare workers in Soweto, South Africa. Health Policy Plan. 2022, 37, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Lippman, S.A.; Treves-Kagan, S.; Gilvydis, J.M.; Naidoo, E.; Khumalo-Sakutukwa, G.; Darbes, L.; Raphela, E.; Ntswane, L.; Barnhart, S. Informing Comprehensive HIV Prevention: A Situational Analysis of the HIV Prevention and Care Context, North West Province South Africa. PLoS ONE 2014, 9, e102904. [Google Scholar] [CrossRef]
- Kim, A.W.; Burgess, R.; Chiwandire, N.; Kwinda, Z.; Tsai, A.C.; Norris, S.A.; Mendenhall, E. Perceptions, risk and understandings of the COVID-19 pandemic in urban South Africa. S. Afr. J. Psychiatry 2021, 27, 1580. [Google Scholar] [CrossRef]
- World Health Organization. Statement for Healthcare Professionals: How COVID-19 Vaccines Are Regulated for Safety and Effectiveness (Revised March 2022). 2022, pp. 1–16. Available online: https://www.who.int/news/item/17-05-2022-statement-for-healthcare-professionals-how-covid-19-vaccines-are-regulated-for-safety-and-effectiveness (accessed on 16 March 2023).
- Van Khuc, Q.; Nguyen, T.; Nguyen, T.; Pham, L.; Le, D.-T.; Ho, H.-H.; Truong, T.-B.; Tran, Q.-K. Young Adults’ Intentions and Rationales for COVID-19 Vaccination Participation: Evidence from a Student Survey in Ho Chi Minh City, Vietnam. Vaccines 2021, 9, 794. [Google Scholar] [CrossRef]
- Midi, H.; Sarkar, S.; Rana, S. Collinearity diagnostics of binary logistic regression model. J. Interdiscip. Math. 2010, 13, 253–267. [Google Scholar] [CrossRef]
- Bandura, A. Perceived self-efficacy in the exercise of control over AIDS infection. Eval. Program Plan. 1990, 13, 9–17. [Google Scholar] [CrossRef]
- Bosire, E.N.; Chiseri, K.; Comeau, D.L.; Richter, L.; Stein, A.D.; Norris, S.A. A qualitative study of risks and protective factors against pregnancy among sexually-active adolescents in Soweto, South Africa. PLoS Glob. Public Health 2021, 1, e0000044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Response | Non-Hesitancy n (%) | Hesitancy n (%) | Total (380) n (%) | p-Value |
|---|---|---|---|---|---|
| Age | 18–24 years | 55 (70) | 179 (59) | 234 (62) | 0.099 |
| 25–35 years | 24 (30) | 122 (41) | 146 (38) | ||
| Sex | Male | 37 (47) | 114 (38) | 151 (40) | 0.147 |
| Female | 42 (53) | 187 (62) | 229 (60) | ||
| Education | Primary or None | 0 (0) | 3 (1) | 3 (1) | 0.385 |
| Secondary | 65 (82) | 259 (86) | 324 (85) | ||
| Tertiary | 14 (18) | 39 (13) | 53 (14) | ||
| Marital status | Not in union/not married/ single | 77 (98) | 288 (96) | 365 (96) | 0.468 |
| In union/married | 2 (2) | 13 (4) | 15 (4) | ||
| Ethnic group | Black | 79 (100) | 290 (96) | 369 (97) | 0.226 |
| Colored | 0 (0) | 2 (1) | 2 (1) | ||
| Non-South Africans | 0 (0) | 9 (3) | 9 (2) | ||
| Religion | Roman Catholic church | 2 (3) | 19(6) | 21 (6) | 0.531 |
| Evangelical Charismatic | 8 (10) | 36 (12) | 44 (11) | ||
| African Independent Church | 20 (25) | 53 (18) | 73 (19) | ||
| Christian protestant | 27 (34) | 112 (37) | 139 (37) | ||
| Muslim | 1 (1) | 7 (2) | 8 (2) | ||
| African tradition 1 | 18 (23) | 57 (19) | 75 (20) | ||
| Other | 3 (4) | 17 (6) | 20 (5) | ||
| Source of information | Family members | 17 (22) | 47 (16) | 64 (17) | 0.558 |
| Friends | 3 (4) | 6 (2) | 9 (2) | ||
| Healthcare workers | 1(1) | 11 (4) | 12 (3) | ||
| Internet | 34 (44) | 150 (51) | 184 (50) | ||
| Radio/School | 3 (4) | 10 (3) | 13 (4) | ||
| TV | 19 (25) | 71 (24) | 90 (24) | ||
| Level of significance is at p-value less than or equal to 0.05 | |||||
| “If a Teacher Is COVID-19 Positive, They Should Be Allowed to Continue Teaching.” | ||||
|---|---|---|---|---|
| Responses | Non-hesitant | Summary | Hesitant | Summary |
| n (%) | n (%) | n (%) | n (%) | |
| Strongly agree | 2 (4) | 17 (33) | 6 (12) | 34 (67) |
| Agree | 15 (29) | 28 (55) | ||
| Disagree | 39 (12) | 62 (19) | 122 (37) | 267 (81) |
| Strongly disagree | 23 (7) | 145 (44) | ||
| “I prefer to break physical contact with people living with COVID-19.” | ||||
| Strongly agree | 2 (1) | 53 (19) | 39 (14) | 227 (81) |
| Agree | 51 (8) | 188 (67) | ||
| Disagree | 23 (64) | 26 (26) | 64 (64) | 74 (74) |
| Strongly disagree | 3 (10) | 10 (10) | ||
| “It is better to develop immunity by getting sick rather than getting the vaccine.” | ||||
| Strongly agree | 7 (6) | 42 (36) | 24 (21) | 75 (64) |
| Agree | 35 (30) | 51 (44) | ||
| Disagree | 34 (13) | 37 (14) | 180 (68) | 226 (86) |
| Strongly disagree | 3 (1) | 46 (18) | ||
| “I believe that the COVID-19 vaccine can stop me from being infected.” | ||||
| Strongly agree | 2 (1) | 13 (8) | 19 (12) | 151 (92) |
| Agree | 11 (7) | 132 (80) | ||
| Disagree | 53 (25) | 66 (31) | 132 (61) | 150 (69) |
| Strongly disagree | 13 (6) | 18 (8) | ||
| “Quarantining people with COVID-19 is the best way to prevent the disease.” | ||||
| Strongly agree | 4 (1) | 55 (17) | 55 (17) | 272 (83) |
| Agree | 51 (16) | 217 (66) | ||
| Disagree | 17 (32) | 24 (45) | 21 (40) | 29 (55) |
| Strongly disagree | 7 (13) | 8 (15) | ||
| “COVID-19 vaccine has serious side-effects.” | ||||
| Strongly agree | 20 (7) | 48 (17) | 96 (34) | 236 (83) |
| Agree | 28 (10) | 140 (49) | ||
| Disagree | 22 (23) | 31 (32) | 60 (63) | 65 (68) |
| Strongly disagree | 9 (9) | 5 (5) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muthoni, J.; Otwombe, K.; Thaele, D.; Choge, I.; Steenberg, B.; Cutland, C.; Madhi, S.A.; Sokani, A.; Myburgh, N. COVID-19 Vaccination Hesitancy among Youths in Soweto, South Africa. Vaccines 2023, 11, 960. https://doi.org/10.3390/vaccines11050960
Muthoni J, Otwombe K, Thaele D, Choge I, Steenberg B, Cutland C, Madhi SA, Sokani A, Myburgh N. COVID-19 Vaccination Hesitancy among Youths in Soweto, South Africa. Vaccines. 2023; 11(5):960. https://doi.org/10.3390/vaccines11050960
Chicago/Turabian StyleMuthoni, Jelioth, Kennedy Otwombe, Dineo Thaele, Isaac Choge, Bent Steenberg, Clare Cutland, Shabir A. Madhi, Andile Sokani, and Nellie Myburgh. 2023. "COVID-19 Vaccination Hesitancy among Youths in Soweto, South Africa" Vaccines 11, no. 5: 960. https://doi.org/10.3390/vaccines11050960
APA StyleMuthoni, J., Otwombe, K., Thaele, D., Choge, I., Steenberg, B., Cutland, C., Madhi, S. A., Sokani, A., & Myburgh, N. (2023). COVID-19 Vaccination Hesitancy among Youths in Soweto, South Africa. Vaccines, 11(5), 960. https://doi.org/10.3390/vaccines11050960