Abstract
Background: Vaccination is one of the most effective measures to prevent influenza illness and its complications. Since the 1980s, countries and territories in the Americas have progressively implemented influenza vaccination operations in high-risk priority groups—such as older adults, pregnant persons, persons with comorbidities and health workers. Methods: In this review, we present the history and progress of the seasonal influenza program in the Americas, how the program contributed to the efficient and timely roll-out of the COVID-19 vaccines during the pandemic, and how the program can be used to promote immunization operations across the life span for existing and future vaccines. Results: The influenza A(H1N1)pdm09 pandemic in 2009 and the COVID-19 pandemic in 2020–2023 underscored the importance of having a robust seasonal influenza vaccination program for pandemic preparedness and response. Overall, countries with existing seasonal influenza vaccination programs were better prepared and rolled out the delivery of COVID-19 vaccines more quickly and effectively compared to other countries where the influenza vaccination platform was weak or non-existent. Conclusions: Traditionally, national immunization programs of developing countries have been predominately focused on newborns, children younger than five years and school-aged children while often limiting their investment in effective adult vaccination programs; these programs are typically isolated to high-income countries. Countries in Latin America have been the exception, with strong influenza vaccination programs for adults regardless of national income level. The presence of functional and effective adult influenza vaccination programs can also facilitate the acceptance and uptake of other adult vaccines targeting priority groups at higher risk for severe illness or complications.
1. Introduction
Seasonal influenza epidemics pose a substantial burden of disease, affecting individuals of all ages and causing substantial morbidity and mortality. The World Health Organization (WHO) estimates that each year influenza causes 1 billion infections, including 3–5 million severe illnesses and 290,000–650,000 influenza-related deaths globally [1]. In the Americas, data reported from member states to SARInet plus—a Pan American Health Organization (PAHO) integrated respiratory illness surveillance network created in 2014 to monitor influenza and other respiratory viruses in the Americas—indicate that influenza contributes significantly to the respiratory disease burden in the Region [2]. It is estimated that between 716,000 and 829,000 influenza-associated respiratory hospitalizations and 41,007 to 71,710 influenza-associated deaths occur every year in the Region [3,4]. Preliminary findings from a 2022–2023 analysis covering 70% of the population, estimate approximately 55 million annual cases of mild influenza in the Americas. In 2020, SARInet plus was expanded to integrate COVID-19 surveillance into existing sentinel-based severe acute respiratory infection (SARI)/influenza-like illness (ILI) surveillance systems [5,6].
Vaccination is one of the most effective measures to prevent influenza illness and its complications. Safe and effective influenza vaccines are available and are routinely used globally [7]. Historically, the Americas has been one of the regions with the highest seasonal influenza vaccination coverage in the world [8], yet some countries struggled to sustain routine immunization services during the COVID-19 pandemic [9]. The first seasonal influenza vaccine was developed in the 1930s and introduced in the United States in 1945. Since 1980, countries and territories in the Americas have been progressively implementing and expanding influenza vaccination activities in priority groups—such as older adults, pregnant persons, children 6–23 months of age, persons with comorbidities and health workers—and integrating this vaccine into their national immunization programs [8,10,11]. The influenza A(H1N1)pdm09 pandemic in 2009 and the COVID-19 pandemic in 2020–2023 underscored the importance of having a robust influenza vaccination program for pandemic preparedness and response [12,13]. Countries with existing seasonal influenza vaccination programs targeting adult populations were better prepared and rolled out the COVID-19 vaccines more quickly in comparison to other countries where the influenza vaccination program was weak or non-existent [14,15,16]. Also, high-performing influenza vaccination programs have been shown to facilitate the acceptance and uptake of other vaccines among high-risk priority groups, such as pregnant persons, health workers and older adults [14,17,18].
In this review, we describe the progress of the seasonal influenza vaccination in the Americas and the lessons learned about building robust, sustainable life-course approach immunization programs and assess their role in facilitating the rollout of novel or existing vaccines during public health emergencies. Its purpose is to describe the key lessons learned about sustainable vaccine introduction, as well as examine how the program contributed to a timely roll-out of COVID-19 vaccines during the recent pandemic. We discuss how these experiences can serve as a blueprint for the introduction of new vaccines—for example, against the respiratory syncytial virus (RSV) or during preparedness and response operations to new epidemics and pandemics—for similar adult priority groups. We intend this review to be useful in delineating the next steps for advancing influenza vaccination programs in the Americas and in supporting other WHO regions in improving their own programs to reduce the burden of influenza morbidity and mortality globally through a life-course immunization approach.
2. Influenza Vaccination Program in the Americas
2.1. Influenza Vaccine Introduction
Seasonal influenza vaccination in the Americas was first introduced in the United States in 1945 [19] and in Canada and Chile in 1980 with a focus on older adults. Since then, countries in the Americas have been progressively introducing the vaccine to risk groups and expanding the vaccination activities to other priority groups. While in 2002 only seven countries in the Americas were vaccinating priority groups, in 2023, 41 (93%) out of the 44 countries and territories that report their data through the PAHO/WHO and the United Nations Children’s Fund (UNICEF) electronic Joint Reporting Form (eJRF) were using the vaccine in at least one priority group. Only Guyana, Haiti and Saint Vincent and the Grenadines do not have a seasonal influenza vaccination program targeting any priority group. Older adults and health workers were targeted for vaccination in 40 (98%) countries and territories, persons with chronic diseases in 36 (88%), pregnant persons in 35 (85%), and children older than 6 months in 30 (73%) countries [8,10,11] (Table 1 and Figure 1).

Table 1.
Seasonal influenza vaccination in the Americas, year of introduction, vaccine formulation and priority groups by country, 2023 (n = 44).
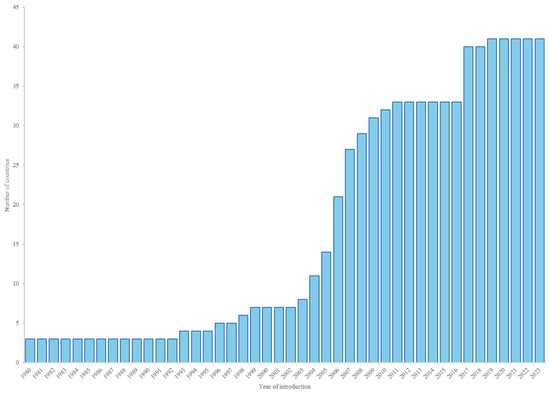
Figure 1.
Cumulative number of countries with seasonal influenza vaccination by year, Region of the Americas, 1980–2023. Source: eJRF.
2.2. Influenza Vaccine Formulations
Seasonal influenza vaccine composition is updated every year for both hemispheres to optimize the effectiveness of the vaccine with the circulating strains. In 2023, 27 (66%) countries/territories with a seasonal influenza vaccination program used the Northern Hemisphere vaccine formulation, while 14 (34%) used the Southern Hemisphere vaccine formulation (Table 1) [8]. To date, no country/territory in Latin America and the Caribbean has reported the public-sector use of live attenuated influenza vaccines (LAIV) to PAHO/WHO. These countries use only inactivated influenza vaccines. However, LAIV has been used in Canada for individuals aged 2–59 years [20] and in the United States for healthy non-pregnant people aged 2–49 years [21]. Since 2024, most of the countries in the Region are using trivalent vaccines (composed of two influenza A strains and one influenza B) following the recommendations of the WHO influenza vaccine composition advisory committee [22].
2.3. Procurement Through the PAHO Revolving Fund for Vaccines in the Americas
While Argentina, Brazil, Canada, Curaçao, Chile, Mexico, Sint Marteen, USA, and Venezuela produce or purchase influenza vaccines directly from manufacturers, 32 of the 41 (78%) countries/territories with seasonal influenza vaccination programs access influenza vaccines through the PAHO Revolving Fund for Access to Vaccines (RFV) [23]. This technical cooperation mechanism provides timely access to quality-assured vaccines and immunization supplies at affordable prices for countries and territories in Latin America and the Caribbean. By consolidating requirements from National Immunization Programs and orchestrating pooled procurement, the RFV leverages economies of scale to improve member states’ purchasing power and supports all procurement and logistics processes. The RFV has been instrumental in enabling rapid and equitable access to new vaccines and in supporting regional goals for disease elimination. Annually, more than 30 million doses of seasonal influenza vaccines are procured through the RFV mechanism. The RFV facilitated the distribution of vaccines for routine immunization programs and emergencies, including COVID-19 vaccines during the pandemic in collaboration with the COVAX facility.
2.4. Quality of Influenza Vaccination Monitoring Data
Despite significant improvements in influenza vaccination program efforts in recent years, the completeness and timeliness of influenza vaccination data remain suboptimal in many countries across the Region [8,11]. First, countries often rely on outdated census data, health workforce statistics, or rough estimations to determine the size of different target groups, such as pregnant persons or people with chronic conditions. Also, countries in Latin America and the Caribbean inconsistently report the number of vaccinated persons per season to PAHO—leaving gaps in the regional estimates of disease burden and vaccination coverage rates. Moreover, merging data from different sources—such as national vaccination registries, healthcare provider registers and surveys—can be challenging due to variations in data formats, definitions and collection methods within the same country. Finally, the demand for vaccination fluctuates each year, complicating efforts to monitor instances of stockout. On the other hand, regional-level information systems are designed to support interoperability between various systems. For example, great strides have been made in facilitating the joint analysis of seasonal influenza surveillance information systems and vaccination registration platforms to calculate regional vaccine effectiveness estimates.
2.5. Seasonal Influenza Vaccination Coverage by Priority Group
It is estimated that every year, more than 100 million doses of influenza vaccine are administered in the Americas using different strategies (e.g., primary care and health-based immunization, door-to-door outreach activities, vaccination campaigns). Target groups and eligible age groups considered for vaccination (e.g., older adults, people with comorbidities and children) vary across countries, which makes comparisons difficult. For instance, some countries target older adults aged 60 years and older, while others focus on persons aged 65 years or older. Countries and territories systematically report data on influenza vaccination programs and vaccination coverage on an annual basis to PAHO, WHO and the United Nations Children’s Fund (UNICEF) via the eJRF [8]. These data are then published annually in publicly accessible “Immunization in the Americas” brochures [11]. While the reported PAHO influenza vaccine coverage rate is the highest by any WHO Region, the Americas still fall short of global goals. According to the 2023 eJRF report, only Colombia, Cuba, Dominican Republic and Mexico achieved the 75% target coverage rate set by WHO for older adults. Regional median vaccination coverage achieved in 2023 among high-risk priority groups in the Region are presented in Table 2 [21].
Table 2.
Regional median influenza vaccination coverage reported by priority groups in the Americas, 2023.
2.6. Vaccination Week in the Americas
Vaccination Week in the Americas (VWA) is a yearly regional initiative that promotes the benefits of vaccination to all persons in the Region. In its 22-year history, more than 40 countries and territories reached 1.15 billion people during the VWA, according to country-level tallies compiled by PAHO. The initiative aims to close the most urgent immunity gaps and contribute to disease elimination efforts in the Americas, all while offering versatile plans for operational execution, communication, and political advocacy that can be adapted to each country’s priorities.
To date, more than 502 million doses of influenza vaccine have been delivered through this initiative across the Americas, with 47 million doses in 2023 alone [24]. Many countries in the Southern Hemisphere use the VWA platform to kick off their seasonal influenza vaccination activities. Also, between 2021 and 2023, approximately 150 million COVID-19 vaccine doses were administered across the Region under the umbrella of the VWA.
2.7. Vaccine Effectiveness and Impact Evaluation of Influenza Vaccination
Established in 2013, the Network for the Evaluation of the Effectiveness of the Vaccine in Latin America and the Caribbean-influenza (REVELAC-I) uses the test-negative design approach to estimate the vaccine effectiveness of influenza vaccines [25]. It leverages sentinel surveillance systems for severe acute respiratory infections (SARIs) at the country level to produce semiannual regional and national estimates of influenza vaccine effectiveness. It also evaluates the impact of the vaccination expressed as the number of influenza illnesses averted through vaccination. Such estimates can be used as inputs for economic analyses to evaluate the value of currently licensed and future vaccines to prevent viral respiratory illnesses. This well-established and flexible platform was expanded to estimate the effectiveness of other respiratory viruses’ vaccines, including those to prevent COVID-19. For the 2024 season, five countries (Argentina, Brazil, Chile, Paraguay, Uruguay) are collecting and analyzing SARI sentinel surveillance and immunization data to generate influenza and COVID-19 vaccines effectiveness against hospitalization. Estimates are stratified by vaccine type, age group and by circulating subtype of influenza virus and variant of SARS-CoV-2 [26]. Interim 2024 vaccine effectiveness estimates against influenza-associated hospitalization are 34.5% (95% confidence interval (CI): 26.4, 41.7) for any type of influenza, 37.2% (95% CI: 22.0, 49.5) for influenza A(H1N1)pdm09 and 36.5% (95% CI: 25.6, 45.7) for influenza A(H3N2) [27]. Mid-season and end-of-season influenza vaccine effectiveness estimates are reported twice a year to the Global Influenza Vaccine Effectiveness (GIVE) working group and presented at the meeting on the Composition of Influenza Virus Vaccines contributing to the recommendation for the viral composition of the next season’s influenza vaccine. Since January 2024, the network has been expanded further to generate effectiveness estimates on preventing severe disease in infants for the maternal RSV vaccine and for the infant receipt of RSV monoclonal antibodies (i.e., laboratory-made proteins that are administered to newborns to protect them against severe RSV disease).
2.8. Partnerships
PAHO maintains strong partnerships with the Ministries and Departments of Health of all 51 countries and territories of the Americas. In the context of influenza vaccination, PAHO is working closely with most member states to maintain the high performance of their existing program or prepare for the introduction of the seasonal influenza vaccine in the national immunization schedule. This close collaboration is essential for the ongoing collection and collation of complete, timely and reliable surveillance data on SARI and ILI events, which in turn allows the Region to assess viral circulation in both hemispheres and take appropriate action to prevent epidemics. Also, PAHO is in a technical and financial partnership with the U.S. Centers for Disease Control and Prevention (CDC), which has been a supporter of the SARInet and REVELAC-I networks since their inception.
3. Leveraging Seasonal Influenza Vaccination Programs for Pandemic Vaccination in the Americas
3.1. Seasonal Influenza Vaccination for Pandemic Preparedness and Response
The existence of seasonal influenza vaccination programs contributed to the response to both the 2009 influenza A(H1N1)pdm09 pandemic and the COVID-19 pandemic. An analysis of the 2009 pandemic revealed that countries with a pre-existing seasonal influenza vaccination program were able to more quickly roll-out the pandemic influenza A(H1N1)pdm09 vaccine [12]. Similarly, 12 months after the introduction of COVID-19 vaccines, countries with an influenza vaccination program had reached an average vaccination coverage of 47% of the total population with the primary series compared to 22% in countries without influenza programs [14]. During and after the COVID-19 pandemic, several assessments suggested that, among the potential predictors of COVID-19 vaccine introduction and roll-out success (i.e., national maturity levels for childhood, adolescent, and adult vaccinations; experience conducting emergency vaccination; tendency to be early adopters of new vaccines; degree of trust in the vaccine product; availability of human resources; income status) [14,15], only the presence of seasonal influenza vaccination programs were associated with a swift introduction capacity for COVID-19 vaccines and higher coverage levels [13]. These results are compatible with findings from COVID-19 vaccine post-introduction evaluations (c-PIE) conducted in 20 countries globally between 2021 and 2022 and supported by the findings of key-informant interviews with the WHO regional and country-level immunization officers [14,16]. The following factors were identified as essential for the successful introduction of the COVID-19 vaccines, according to the WHO technical guidelines for the National Deployment and Vaccination Plan (NDVP) [28].
3.2. Regulatory Pathways for Authorization, Vaccine Introduction and Roll-Out
Countries with seasonal influenza vaccination programs had more straightforward regulatory approvals or emergency authorization mechanisms for the pandemic COVID-19 vaccines and established procedures for importation and use in the target population. Data collected through standardized COVID-19 post-introduction evaluation conducted at national and subnational levels in LMIC indicated that 29% of countries with influenza vaccination programs encountered barriers to regulatory approval of COVID-19 vaccines compared to 40% of countries without an influenza vaccination program [14]. On the other hand, countries without influenza vaccination programs were often slower in their operations for vaccine introduction, distribution, and administration.
3.3. Vaccination in Priority Groups
Existing seasonal influenza vaccination strategies targeting priority groups in the adult population (i.e., older adults, health workers, pregnant persons, and adults with chronic conditions) played a crucial role in guiding effective operations and achieving high vaccination coverage of COVID-19 vaccines within these populations. For example, the COVID-19 vaccination coverage of at least one dose among health workers was 83% in countries with an influenza vaccination program compared to 69% in countries without health worker vaccination programs. Also, adults with comorbidities had higher COVID-19 vaccine uptake in countries with health worker vaccination programs than in countries without health worker vaccination programs [14]. In addition, influenza vaccination programs for older adults provided sources of data (e.g., nominal electronic immunization registries, collaboration with nursing homes and medical specialists) to identify and locate this population at the time of COVID-19 vaccination. Furthermore, the expertise of advisory committees on how to determine national priority groups for influenza vaccination was leveraged to determine the priority risk groups for COVID-19 vaccination.
3.4. National Technical Advisory Groups
The role of National Immunization Technical Advisory Groups (NITAG) as key experts responsible for providing independent, transparent, evidence-informed and timely recommendations on vaccines and immunizations to health authorities, was pivotal in guiding outbreak responses and aiding in COVID-19 pandemic recovery efforts. Most NITAGs in the Region served as the main advisory body guiding the immunization program on the introduction and use of COVID-19 vaccines. This responsibility included the definition of groups at higher risk for severe illness (or complications) who should be prioritized for vaccination [29]. Operational recommendations for reaching these groups also benefitted from the existing national guidance for influenza vaccination [14,16].
3.5. Experience in Vaccination Campaigns
Health staff already familiar with mass vaccination campaigns for both young children and older adults accelerated the deployment of COVID-19 vaccines. Their experience administering vaccines to multiple age groups facilitated the rapid scale-up of COVID-19 vaccination campaigns on a massive scale and under considerable political and societal pressure. Countries with a seasonal influenza vaccination program reported fewer problems with cold chain capacity (7%) compared to countries with no vaccination program (25%) [14]. Also, experience with influenza vaccination campaigns allowed COVID-19 vaccination events to be tailored to the needs of priority groups (e.g., convenient timing and location of the vaccination sites; transportation; accommodations while waiting). Public awareness and education campaigns on influenza vaccination—targeting both the general population and high-risk priority groups—served as a model for COVID-19 vaccination campaigns, helping to increase acceptance, uptake and coverage [14,16].
3.6. Vaccination Information Systems
The vaccination monitoring and recording systems developed for influenza—especially for the pediatric population—were adapted to track the distribution and administration of COVID-19 vaccines. In fact, some countries without pre-existing systems took advantage of the COVID-19 vaccine introduction to develop and implement nominal electronic immunization registries, use SMS reminders, conduct real-time data collection and reporting, and generate digital vaccination certificates; many of which are now being expanded to include other vaccines in their national immunization program (e.g., influenza, RSV). The introduction of influenza vaccines against influenza pandemic A(H1N1)pdm09 in 2009 and against COVID-19 highlighted the importance of monitoring and reporting adverse events following immunization, especially for new vaccines. PAHO has revised and updated the regional manual for the surveillance of Events Supposedly Attributable to Vaccination or Immunization (ESAVI) and established a regional strategy for conducting permanent and functioning ESAVI surveillance for all vaccines [30].
4. Influenza Vaccination as Part of the Life-Course Approach
The life-course approach to health provides a framework to understand the health and well-being of individuals and populations as the sum of capacities that are built, sustained, and recovered across both life stages and generations. Today, the life-course approach to immunization states that people should receive all recommended doses of vaccines throughout their lives to obtain the maximum benefits of protection against vaccine-preventable diseases at different ages, across generations, and in their communities [31,32]. Integrating vaccination programs for respiratory viruses into routine health services, such as adult scheduled immunization visits or antenatal care visits, can contribute to the lasting sustainability of vaccination programs at large. Below, we report examples of PAHO strategies and operations that contributed to strengthening national political and programmatic frameworks around life-course immunization using the influenza vaccination platform as a starting point.
4.1. Policy Recommendations from the WHO and PAHO Technical Advisory Groups
Since 2004, PAHO’s Technical Advisory Group (TAG) and WHO’s Strategic Advisory Group of Experts (SAGE) on immunization have built upon each other’s recommendations. In the context of COVID-19, the latest recommendations promote prioritization of high-risk groups (i.e., older adults, pregnant persons, persons with comorbidities, immunocompromised persons, health workers) for vaccination against respiratory infections [33,34,35,36]. Since 2021, both groups have recommended that the influenza vaccination platform be used to promote the rapid deployment and uptake of COVID-19 vaccinations, thus reducing the rates of severe disease, hospitalization, and death among priority populations. Additionally, coadministration of both influenza and COVID-19 vaccines during the same vaccination encounter, as recommended by WHO SAGE in October 2021 [37], could facilitate the implementation of integrated vaccine programmes, improve vaccination uptake, and decrease the overall burden on health services [38].
In November 2023, the TAG issued a statement where it strongly supported the SAGE recommendation that countries should integrate COVID-19 vaccination operations into their national immunization programs to maintain focus on achieving high vaccination coverage against the SARS-CoV-2 virus among priority groups and promote vaccination among all age groups [39]. During this same meeting, the TAG considered whether to recommend RSV vaccination among pregnant persons at 32–36 weeks of gestation to prevent disease in infants while minimizing the risk of preterm birth. The TAG did not issue comments on the coadministration of this vaccine with other antigens during pregnancy, but the US Centers for Disease Control and Prevention (CDC) states that the “RSVpreF vaccine can be administered to pregnant persons with other recommended vaccines, such as tetanus, diphtheria, and pertussis (Tdap), influenza, and COVID-19 vaccines” [40].
4.2. Addition of RSV to the SARInet Network
SARInet plus has long integrated RSV into national sentinel surveillance strategies, proving essential for providing comprehensive monitoring of virologic and epidemiological data to increase situational awareness and guide preventive measures [2,5]. The network improves coordination among national respiratory surveillance systems in both outpatient and hospital settings and incorporates RSV diagnostic testing at National Influenza Centers (NICs) and National Reference Laboratories (NRLs) contributing to the WHO Global Influenza Surveillance and Response System (GISRS).
SARInet plus supports public health decisions aimed at reducing RSV-related morbidity and mortality by analyzing trends, seasonal variations, and regional differences overall and in relation to the disease severity (i.e., RSV-related hospitalizations), focusing on high-risk groups like infants and older adults. Analyses dating back to 2010 have revealed significant regional variations in RSV seasonality, underscoring the need for tailored interventions [41]. Regional and climatic factors are known to influence RSV activity, typically starting in the south and moving northward with differing onset and peak times [42,43]. Understanding these patterns is crucial for optimizing interventions and mitigating the substantial burden of RSV across all age groups.
4.3. Latin American Center for Perinatology, Women and Reproductive Health (CLAP/WR) Network
Since 1983, CLAP/WR has promoted a standardized clinical record for maternal and perinatal care, known as the Perinatal Clinical Record, which includes information about vaccines administered during pregnancy [44]. This record is supported by the Perinatal Information System (SIP), available free of charge to all countries in the Americas. Nineteen health facilities in nine countries that are members of the “CLAP Network for Maternal Health Surveillance” regularly contribute their data to the Perinatal Clinical Record. The network maintains high-quality data on coverage with vaccines recommended for routine use during pregnancy, including COVID-19 vaccines. This platform has enabled the network to follow trends in vaccination coverage among pregnant persons, identify factors associated with the vaccine uptake and to monitor ESAVIs associated with various COVID-19 vaccination platforms used in these countries. More recently, the network has begun monitoring ESAVIs associated with RSV vaccination of pregnant persons in Argentina and Uruguay.
4.4. Behavioral and Social Drivers Studies
Behavioral and Social Drivers (BeSD) of vaccination are defined as beliefs and experiences specific to vaccination that are potentially modifiable to increase vaccine uptake [45]. The WHO developed the BeSD tool to help countries understand the reasons for low vaccine uptake, track trends over time, and reduce coverage inequities by gathering and using data to systematically design, implement, and evaluate tailored interventions [46]. In 2021 and 2022, PAHO used this methodology in countries of the Caribbean and Latin Americas to assess attitudes towards COVID-19 vaccines among health workers. By the end of 2024, PAHO will have implemented the Spanish version of the tool to collect perceptions around vaccination against influenza, COVID-19 and RSV among pregnant persons aged 18 years or older in Argentina. BeSD results can be used to inform the design and implementation of interventions that increase acceptance and confidence in vaccines in the persons at the highest risk of infection and severe disease.
Also, in 2024, PAHO published a performance monitoring tool to support countries in conducting a self-assessment of their national immunization program [47]. Results from these exercises will provide additional information about member states’ efforts and challenges in providing vaccination services to high-risk priority groups.
5. Discussion
The strong seasonal influenza vaccination program in the Americas, built over decades, prevents hundreds of thousands of illnesses, hospitalizations and influenza-associated deaths every year [48]. Following the 2009 A(H1N1) influenza and 2020–2023 COVID-19 pandemics, countries of the Americas have continued their efforts to sustain seasonal influenza vaccine uptake among priority groups at higher risk for severe illness (or complications), especially in the adult population and among pregnant persons. Countries have also continued strengthening their influenza surveillance systems, immunization platforms, and information systems—efforts which indirectly bolster preparedness for future pandemics [6,9,49]. Furthermore, influenza vaccination efforts have greatly contributed to the successful expansion of life-course immunization beyond childhood vaccines. It has facilitated the introduction of COVID-19 vaccines in the Americas and progressively reduced mortality due to vaccine-preventable diseases. Below, we outline six key recommendations that could support other WHO Regions in strengthening their seasonal influenza vaccination strategies.
- Promote high-level advocacy and collaboration between Ministries of Health, PAHO Immunization Program and Revolving Fund for Access to Vaccines, and their partners to promote and consistently finance seasonal influenza vaccination for the general population and among high-risk priority groups.
- Strengthen technical cooperation between these stakeholders to develop updated guidance and tools and to strengthen national capacities for timely vaccination in priority groups. These materials supported member states in their decision-making to strengthen national policies and programs for influenza vaccination and improved the reach and quality of their seasonal programs [50].
- Expand the seasonal influenza vaccination program to persons aged 6 months or older, with a focus on young children, older adults, pregnant persons, people with comorbidities and health workers. Such an approach of vaccinating multiple age groups concomitantly allowed countries to implement and promote the concept of immunization across the life course well before it was included as a strategic priority of the Immunization Agenda 2030. As more vaccines come through the pipeline to address more diseases and conditions, these lessons learned about how to facilitate vaccine acceptance and delivery across the life course will become more and more critical.
- Document lessons learned from the introduction and roll-out of the COVID-19 vaccines during the pandemic. Employing existing structures of the seasonal influenza vaccination programs—such as regulatory pathways, vaccination strategies, campaign planning and implementation, cold chain capacities, information systems, public awareness and trained health workers—was essential for a rapid introduction and roll-out of COVID-19 vaccines. Having a strong seasonal influenza vaccination program contributes to better preparedness and would support emergency response operations during the next pandemic.
- Improve the completeness, timeliness and accuracy of the data flow after vaccines are in use in populations—from needs assessments to data collection, analysis, interpretation and interoperability. This step can strengthen the completeness, timeliness and reliability of the information on influenza vaccination programs and therefore promote the use of evidence to inform policy decisions.
- Intensify maternal vaccination operations, which can benefit from the existing capacities of the influenza vaccination program to reach this population. For pregnant persons specifically, the option of receiving these additional vaccines in conjunction with the annual dose against influenza or RSV can facilitate acceptance and uptake. The integration of vaccination operations with other essential care and antenatal services is likely to further boost coverage rates.
As part of its ongoing efforts to support immunization operations and reduce the burden of vaccine-preventable diseases, the Americas will continue to improve national immunization programs against respiratory pathogens and contribute to the lasting sustainability of vaccination programs at large.
6. Conclusions
Influenza vaccination protects people at risk from developing severe disease. It reduces the burden of disease, including hospitalization and deaths. It also protects health workers by reducing transmission and helps maintain the health system during influenza epidemics and pandemics. Seasonal influenza vaccination provides a sustainable platform for life course immunization against influenza and other vaccine-preventable diseases and contributes to a foundation for pandemic preparedness and response.
Author Contributions
F.N. and M.G. drafted the manuscript. M.V.-G., B.d.M., J.J., P.C., A.R., M.R., A.V. (Andrea Vicari), M.H.O., S.G., A.V. (Alba Vilajeliu), E.L., J.P., J.C., A.L.F., E.A.-B., D.S.P. and A.M.R. provided detailed comments and suggestions. All authors have read and agreed to the published version of the manuscript.
Funding
This publication was supported by the Grant or Cooperative Agreement Number NU66GH002171, funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health and Human Services.
Acknowledgments
We express our sincere gratitude for the tireless effort and dedication of the immunization staff. Their commitment to public health remained strong even in the most challenging moments of the pandemic. Their collaboration and commitment have been fundamental to confront this global crisis. The solidarity and cooperation they demonstrated reflect the strength of our Region and are inspiring examples of Pan-Americanism.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Global Influenza Programme. Available online: https://www.who.int/teams/global-influenza-programme/surveillance-and-monitoring/burden-of-disease (accessed on 2 December 2024).
- Pan American Health Organization. Data|SARINET. Available online: https://sarinet.org/data/ (accessed on 2 December 2024).
- Palekar, R.S.; Rolfes, M.A.; Arriola, C.S.; Acosta, B.O.; Guidos, P.A.; Vargas, X.B.; Bancej, C.; Ramirez, J.B.; Baumeister, E.; Bruno, A.; et al. Burden of Influenza-Associated Respiratory Hospitalizations in the Americas, 2010–2015. PLoS ONE 2019, 14, e0221479. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of Global Seasonal Influenza-Associated Respiratory Mortality: A Modelling Study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization. Influenza and Other Respiratory Viruses: Surveillance in the Americas 2021, 4th ed.; Pan American Health Organization (PAHO): Bloomfield, NJ, USA, 2022; ISBN 978-92-75-12499-4. [Google Scholar]
- Vicari, A.S.; Olson, D.; Vilajeliu, A.; Andrus, J.K.; Ropero, A.M.; Morens, D.M.; Santos, I.J.; Azziz-Baumgartner, E.; Berman, S. Seasonal Influenza Prevention and Control Progress in Latin America and the Caribbean in the Context of the Global Influenza Strategy and the COVID-19 Pandemic. Am. J. Trop. Med. Hyg. 2021, 105, 93–101. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Vaccines Against Influenza: WHO Position Paper—May 2022. Available online: https://www.who.int/publications/i/item/who-wer9719 (accessed on 3 December 2024).
- World Health Organization. WHO/UNICEF Joint Reporting Process. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/immunization-analysis-and-insights/global-monitoring/who-unicef-joint-reporting-process (accessed on 3 December 2024).
- Nogareda, F.; Gharpure, R.; Contreras, M.; Velandia, M.; Lucia Pacis, C.; Elena Chevez, A.; Azziz-Baumgartner, E.; Salas, D. Seasonal Influenza Vaccination in the Americas: Progress and Challenges during the COVID-19 Pandemic. Vaccine 2023, 41, 4554–4560. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Immunization Data Portal. Available online: https://immunizationdata.who.int/global/wiise-detail-page (accessed on 3 December 2024).
- Pan American Health Organization. Immunization Brochure—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/tag/immunization-brochure (accessed on 3 December 2024).
- Porter, R.M.; Goldin, S.; Lafond, K.E.; Hedman, L.; Ungkuldee, M.; Kurzum, J.; Azziz-Baumgartner, E.; Nannei, C.; Bresee, J.S.; Moen, A. Does Having a Seasonal Influenza Program Facilitate Pandemic Preparedness? An Analysis of Vaccine Deployment during the 2009 Pandemic. Vaccine 2020, 38, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Volkmann, A.-M.; Goldin, S.; McMurren, B.; Gapare, C.; Anne Pratt, B.; Frost, L.; Desai, S. Leveraging Seasonal Influenza Health Worker Vaccination Programmes for COVID-19 Vaccine Introduction: A Global Qualitative Analysis. Vaccine 2024, 42, 125534. [Google Scholar] [CrossRef] [PubMed]
- McCarron, M. Lessons Learned from Leveraging Seasonal Influenza Vaccination Infrastructure in COVID-19 Vaccination. In Proceedings of the Global Exchange Forum on Integrated Immunization Programs and Enhanced Pandemic Preparedness, London, UK, 18–19 October 2023. [Google Scholar]
- Chelsey, G. The Impact of an Established Influenza Vaccination Program for Health Workers on COVID-19 Vaccine Rollout and Uptake in Low-, Lower Middle-, and Upper Middle-Income Countries. In Proceedings of the Options XII Conference, Brisbane, Australia, 29 September–2 October 2024. [Google Scholar]
- Centers for Disease Control and Prevention (CDC), The Task Force for Global Health Country COVID-19 Vaccine Introduction Evaluations (cPIE): Cross-Country Review of Findings. Available online: https://www.technet-21.org/en/resources/report/country-covid-19-vaccine-introduction-evaluations-cpie-cross-country-review-of-findings (accessed on 3 December 2024).
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 766. [Google Scholar] [CrossRef] [PubMed]
- McCarron, M.; Yau, T.S.; Griffin, C.; Marcenac, P.; Ebama, M.S.; Lafond, K.E.; Igboh, L.S.; Duca, L.M.; Bino, S.; Bettaieb, J.; et al. Do Pregnant Persons Want Influenza Vaccines? Knowledge, Attitudes, Perceptions, and Practices Toward Influenza Vaccines in 8 Low- and Middle-Income Countries. J. Infect. Dis. 2024, jiae340. [Google Scholar] [CrossRef] [PubMed]
- Burney, L.E. Influenza Immunization: Statement. Public Health Rep. Wash. DC 1896 1960, 75, 944. [Google Scholar] [CrossRef]
- NACI Recommendations on the Use of Live, Attenuated Influenza Vaccine (FluMist®): Supplemental Statement on Seasonal Influenza Vaccine for 2011–2012. Can. Commun. Dis. Rep. 2011, 37, 1–77. [CrossRef]
- Centers for Disease Control and Prevention (CDC). Live Attenuated Influenza Vaccine [LAIV] (The Nasal Spray Flu Vaccine). Available online: https://www.cdc.gov/flu/vaccine-types/nasalspray.html (accessed on 3 December 2024).
- Recommendations for Influenza Vaccine Composition. Available online: https://www.who.int/teams/global-influenza-programme/vaccines/who-recommendations (accessed on 3 December 2024).
- Pan American Health Organization. PAHO Revolving Fund—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/revolving-fund (accessed on 3 December 2024).
- Vaccination Week in the Americas 2023: Final Report—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/vaccination-week-americas-2023-final-report (accessed on 3 December 2024).
- Pan American Health Organization. Network for the Evaluation of Vaccine Effectiveness in Latin America and the Caribbean—Influenza, (REVELAC-i)—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/network-evaluation-vaccine-effectiveness-latin-america-and-caribbean-influenza-revelac-i (accessed on 3 December 2024).
- Nogareda, F.; Regan, A.K.; Couto, P.; Fowlkes, A.L.; Gharpure, R.; Loayza, S.; Leite, J.A.; Rodríguez, A.; Vicari, A.; Azziz-Baumgartner, E.; et al. Effectiveness of COVID-19 Vaccines against Hospitalisation in Latin America during Three Pandemic Waves, 2021–2022: A Test-Negative Case-Control Design. Lancet Reg. Health Am. 2023, 27, 100626. [Google Scholar] [CrossRef] [PubMed]
- Zeno, E.E.; Nogareda, F.; Regan, A.; Couto, P.; Rondy, M.; Jara, J.; Voto, C.; Rojas Mena, M.P.; Katz, N.; Del Valle Juarez, M.; et al. Interim Effectiveness Estimates of 2024 Southern Hemisphere Influenza Vaccines in Preventing Influenza-Associated Hospitalization—REVELAC-i Network, Five South American Countries, March–July 2024. MMWR Morb. Mortal. Wkly. Rep. 2024, 73, 861–868. [Google Scholar] [CrossRef]
- World Health Organization. Guidance on Developing a National Deployment and Vaccination Plan for COVID-19 Vaccines. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Vaccine-deployment-2021.1-eng (accessed on 3 December 2024).
- Henaff, L.; Zavadska, D.; Melgar, M.; Fihman, J.; Steffen, C.; Hombach, J. The Role of NITAGs in Government Decisions on Vaccine Use: Insights from the Fifth Global NITAG Network Meeting. Lancet Infect. Dis. 2024, 24, e214–e215. [Google Scholar] [CrossRef]
- Vacunación Segura En Las Américas. Experiencia Sobre La Vigilancia de Los Eventos Supuestamente Atribuibles a La Vacunación o Inmunización y La Interoperabilidad de Los Datos. Available online: https://iris.paho.org/handle/10665.2/57547 (accessed on 3 December 2024).
- World Health Organization. Our Work: Life Course. Available online: https://www.who.int/our-work/life-course (accessed on 3 December 2024).
- Pan American Health Organization. Building Better Immunity: A Life Course Approach to Healthy Longevity; PAHO: Durham, NC, USA, 2023; ISBN 978-92-75-12744-5. [Google Scholar]
- Pan American Health Organization. 16 TAG Final Report, 2004—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/documents/16-tag-final-report-2004 (accessed on 3 December 2024).
- Vaccines against Influenza WHO Position Paper—November 2012. Relev. Epidemiol. Hebd. 2012, 87, 461–476.
- Pan American Health Organization. The Immunization Program in the Context of the COVID-19 Pandemic—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/publications/immunization-program-context-covid-19-pandemic (accessed on 3 December 2024).
- World Health Organization. WHO SAGE Seasonal Influenza Vaccination Recommendations During the COVID-19 Pandemic. Available online: https://www.who.int/publications/m/item/who-sage-seasonal-influenza-vaccination-recommendations-during-the-covid-19-pandemic (accessed on 3 December 2024).
- World Health Organization. Coadministration of Seasonal Inactivated Influenza and COVID-19 Vaccines. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-coadministration-influenza-vaccines (accessed on 3 December 2024).
- World Health Organization. Considerations for Integrating COVID-19 Vaccination into Immunization. Available online: https://www.who.int/publications/i/item/9789240064454 (accessed on 3 December 2024).
- Vaccine-Preventable Diseases TAG—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/technical-advisory-group-vaccine-preventable-diseases (accessed on 3 December 2024).
- Fleming-Dutra, K.E.; Jones, J.M.; Roper, L.E.; Prill, M.M.; Ortega-Sanchez, I.R.; Moulia, D.L.; Wallace, M.; Godfrey, M.; Broder, K.R.; Tepper, N.K.; et al. Use of the Pfizer Respiratory Syncytial Virus Vaccine During Pregnancy for the Prevention of Respiratory Syncytial Virus–Associated Lower Respiratory Tract Disease in Infants: Recommendations of the Advisory Committee on Immunization Practices—United States, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 1115–1122. [Google Scholar] [CrossRef]
- Pan American Health Organization. Influenza Situation Report. Available online: https://app.powerbi.com/view?r=eyJrIjoiNDg2ZmU1NWYtZmJkMi00MjlmLThkNTYtOTc4MjNmMjc4YzBjIiwidCI6ImU2MTBlNzljLTJlYzAtNGUwZi04YTE0LTFlNGIxMDE1MTlmNyIsImMiOjR9 (accessed on 3 December 2024).
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal Variations in Seasonal Activity of Influenza and Respiratory Syncytial Virus (RSV): A Global Comparative Review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global Patterns in Monthly Activity of Influenza Virus, Respiratory Syncytial Virus, Parainfluenza Virus, and Metapneumovirus: A Systematic Analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef]
- Pan American Health Organization. Latin American Center for Perinatology, Women and Reproductive Health (CLP/WR)—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/clap (accessed on 3 December 2024).
- World Health Organization. Acceptance and Demand. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/demand (accessed on 3 December 2024).
- World Health Organization. Behavioural and Social Drivers of Vaccination: Tools and Practical Guidance for Achieving High Uptake, 1st ed.; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-004968-0. [Google Scholar]
- Pan American Health Organization. Performance Monitoring Tool for the National Expanded Program on Immunization—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/topics/immunization/performance-monitoring-tool-national-expanded-program-immunization (accessed on 3 December 2024).
- Pan American Health Organization. Myths and Truths About Seasonal Influenza and the Flu Vaccine—PAHO/WHO|Pan American Health Organization. Available online: https://www.paho.org/en/news/14-5-2019-myths-and-truths-about-seasonal-influenza-and-flu-vaccine (accessed on 3 December 2024).
- Ropero-Álvarez, A.M.; El Omeiri, N.; Kurtis, H.J.; Danovaro-Holliday, M.C.; Ruiz-Matus, C. Influenza Vaccination in the Americas: Progress and Challenges after the 2009 A(H1N1) Influenza Pandemic. Hum. Vaccines Immunother. 2016, 12, 2206–2214. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. Influenza Vaccination Toolkit. Available online: https://www.who.int/teams/global-influenza-programme/vaccines/influenza-vaccination-toolbox (accessed on 3 December 2024).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).