
Elderly Patients and Insect Venom Allergy: Are the Clinical Pictures and Immunological Parameters of Venom Allergy Age-Dependent?
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Methods
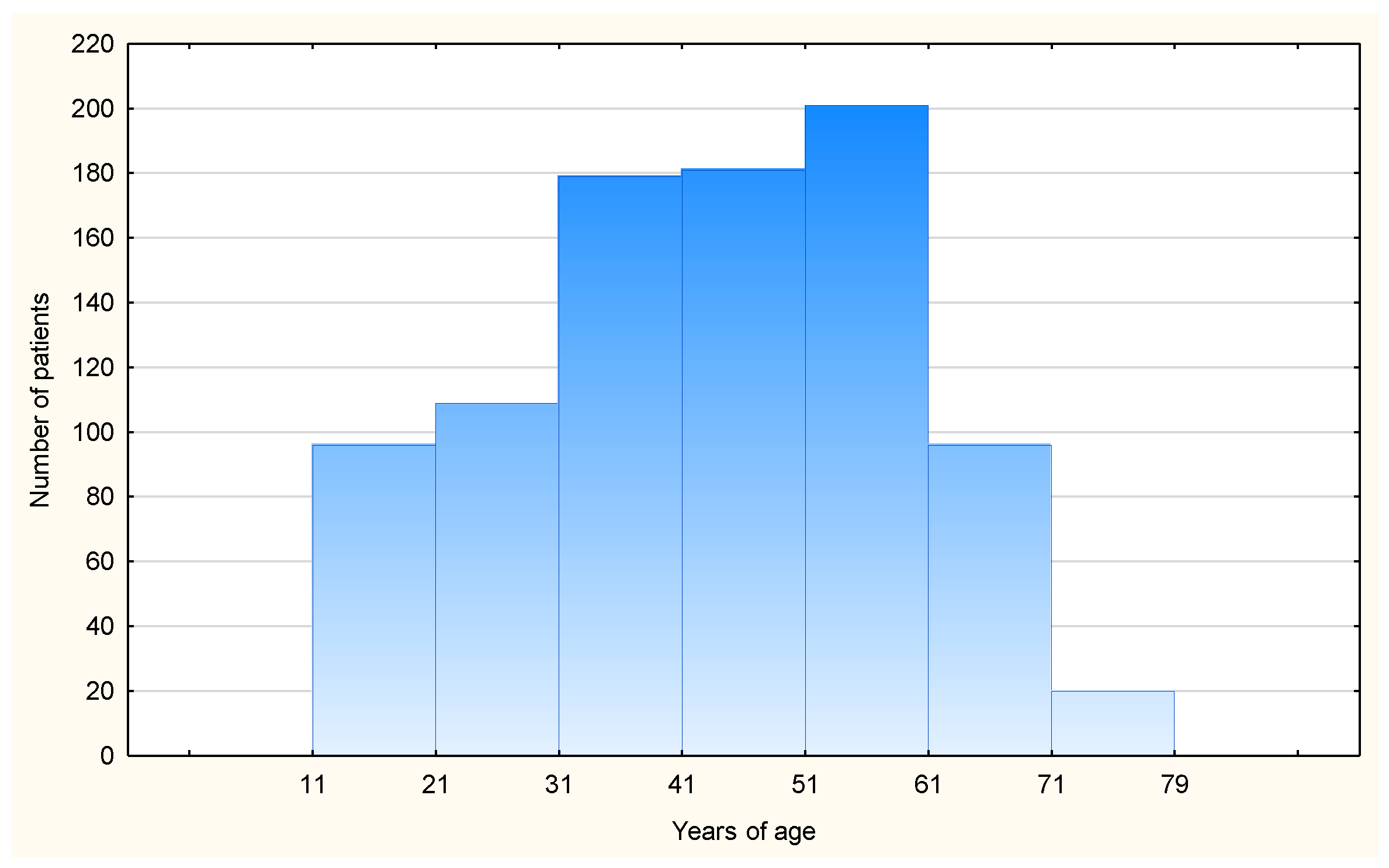
2.1. Database and Cohort
- •
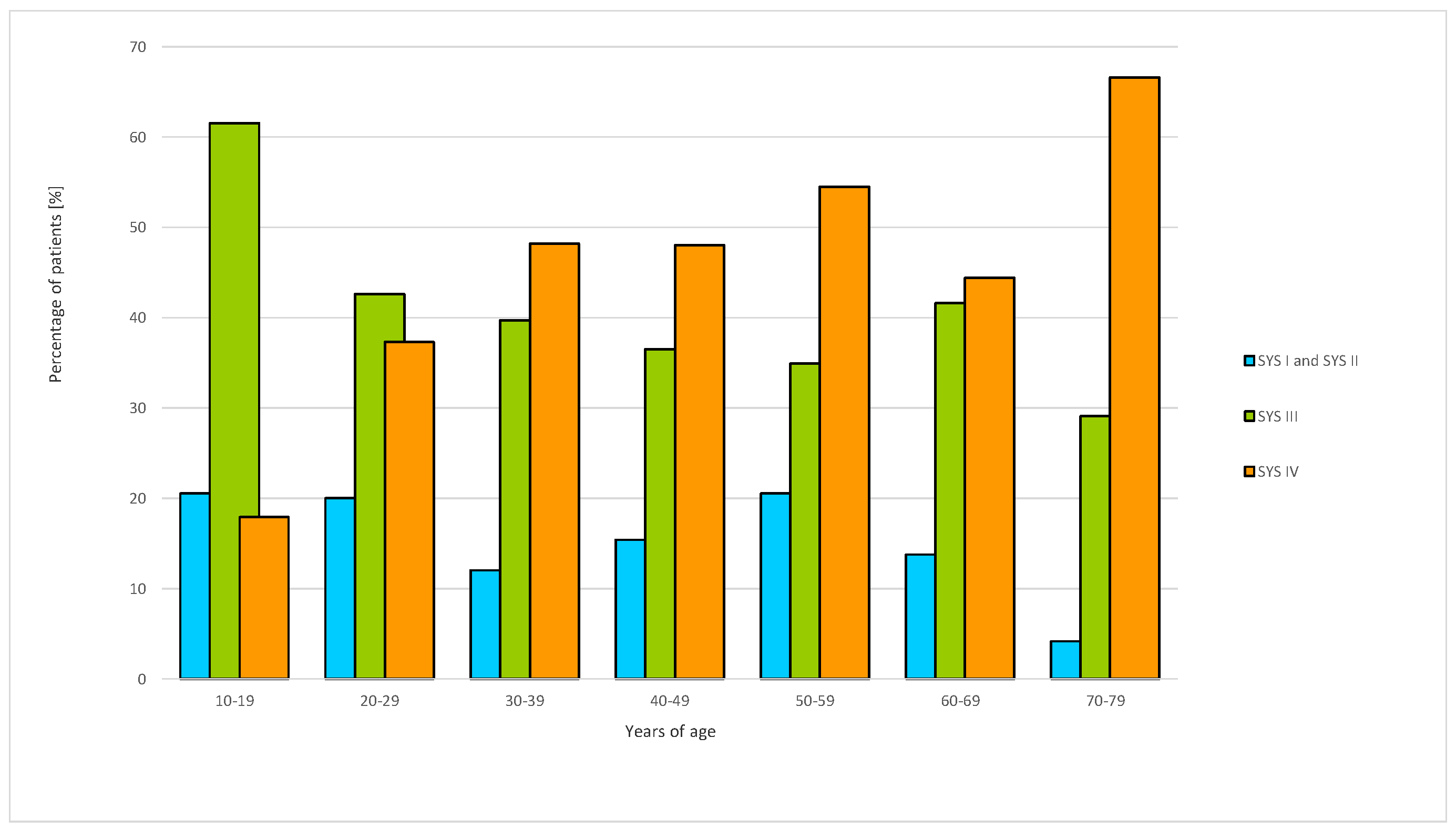
- The severity of reactions was determined using the Müller scale (grades I–IV). The assessment of the severity of HVA reactions is based on the four-grade Müller scale: grade I (urticaria, itching, malaise); grade II (grade I symptoms + angioedema, abdominal pain, nausea, tightness in the chest); grade III (grade I and II symptoms + dyspnea, respiratory symptoms); and grade IV (grade I, II, and III symptoms + cardiovascular symptoms, loss of consciousness, cyanosis).
- •
- The species of the causative insect.
- •
- The presence of accompanying diseases and their treatment.
2.2. Diagnostic Procedures
2.3. Statistical Analysis
3. Results
3.1. Severity of HVA Reactions in Young and Elderly Patients
3.2. ACE and Beta Inhibitors and the Severity of HVA
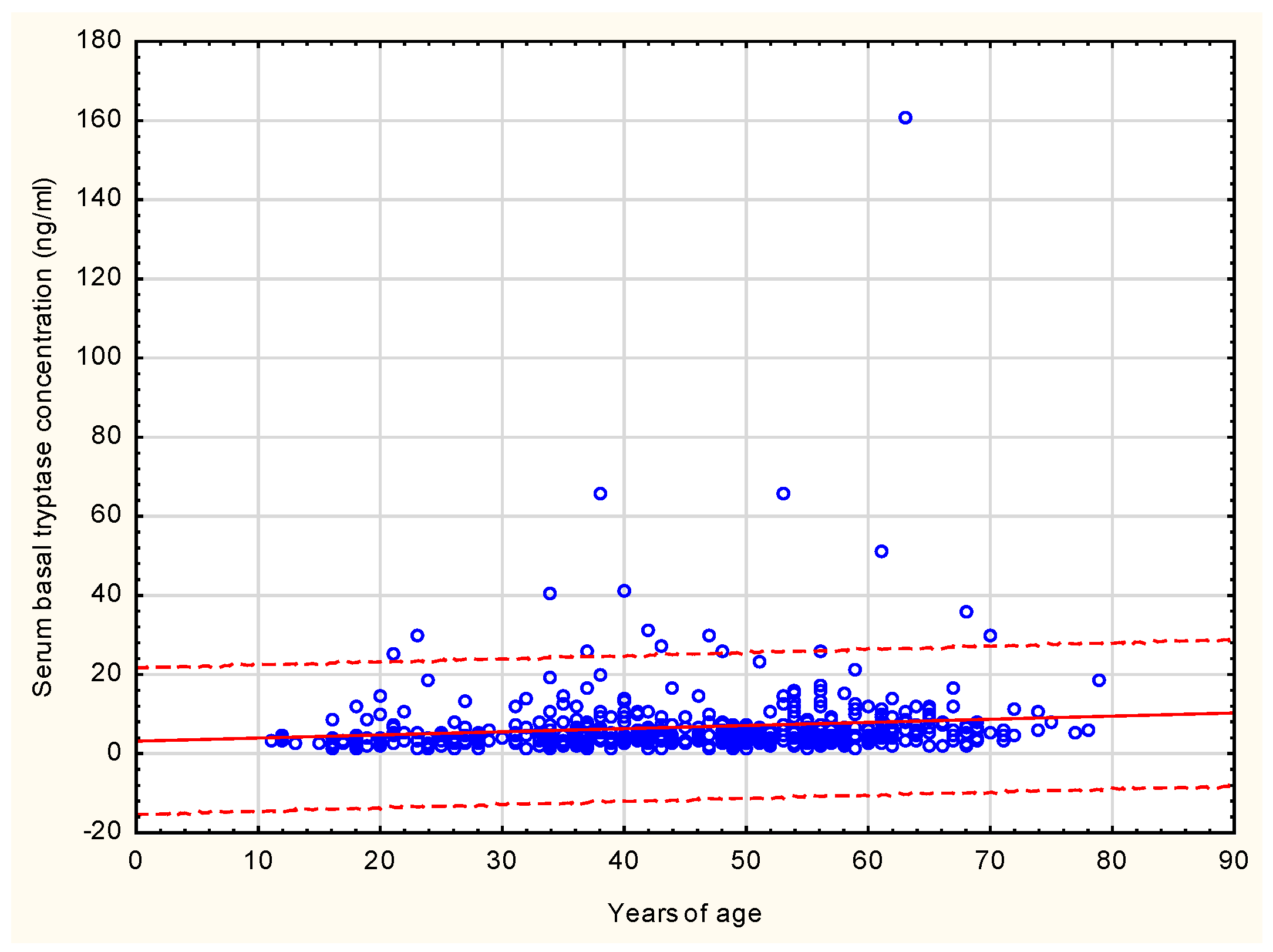
3.3. sBT and Immunological Features Characterizing Elderly HVA Patients (IDT, Venom Specific sIgE)
3.4. Molecular Diagnostic HVA (sIgE against Api m 1, 2, 4, 5, 10, Ves v 1, Ves v 5)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aurich, S.; Dölle-Bierke, S.; Francuzik, W.; Bilo, M.B.; Christoff, G.; Fernandez-Rivas, M.; Hawranek, T.; Pföhler, C.; Poziomkowska-Gȩsicka, I.; Renaudin, J.M.; et al. Anaphylaxis in elderly patients-data from the European anaphylaxis registry. Front. Immunol. 2019, 10, 750. [Google Scholar] [CrossRef] [PubMed]
- Worm, M.; Francuzik, W.; Renaudin, J.M.; Bilo, M.B.; Cardona, V.; Scherer-Hofmeier, K.; Köhli, A.; Bauer, A.; Christoff, G.; Cichocka-Jarosz, E.; et al. Factors increasing the risk for a severe reaction in anaphylaxis: An analysis of data from The European Anaphylaxis Registry. Allergy 2018, 73, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Rueff, F.; Przybilla, B.; Biló, M.B.; Müller, U.; Scheipl, F.; Aberer, W.; Birnbaum, J.; Bodzenta-Lukaszyk, A.; Bonifazi, F.; Bucher, C.; et al. Predictors of severe systemic anaphylactic reactions in patients with Hymenoptera venom allergy: Importance of baseline serum tryptase-a study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J. Allergy Clin. Immunol. 2009, 124, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Feás, X.; Vidal, C.; Remesar, S. What We Know about Sting-Related Deaths? Human Fatalities Caused by Hornet, Wasp and Bee Stings in Europe (1994–2016). Biology 2022, 2, 282. [Google Scholar] [CrossRef] [PubMed]
- Worm, M.; Moneret-Vautrin, A.; Scherer, K.; Lang, R.; Fernandez-Rivas, M.; Cardona, B.; Kowalski, L.M.; Jutel, M.; Poziomkowska-Gesicka, I.; Papadopoulos, N.G.; et al. First European data from the network of severe allergic reactions (NORA). Allergy 2014, 69, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Bilo, M.B.; Bonifazi, F. The natural history and epidemiology of insect venom allergy: Clinical implications. Clin. Exp. Allergy 2009, 39, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Nittner-Marszalska, M.; Liebhart, J.; Małolepszy, J.; Gietkiewicz, K.; Mendrala, W. The results of research on the prevalence of allergy to Hymenoptera venom in Southwestern Poland. Pol. Arch. Med. Wewn. 1998, 100, 245–251. [Google Scholar]
- Brown, S.G.A. Clinical features and severity grading of anaphylaxis. J. Allergy Clin. Immunol. 2004, 114, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Gowland, M.H.; Sharma, V.; Ierodiakonou, D.; Harper, N.; Garcez, T.; Pumphrey, R.; Boyle, R.J. Increase in anaphylaxis-related hospitalizations but no increase in fatalities: An analysis of United Kingdom national anaphylaxis data, 1992–2012. J. Allergy Clin. Immunol. 2015, 135, 956–963. [Google Scholar] [CrossRef]
- Campbell, R.L.; Hagan, J.B.; Li, J.T.; Vukov, S.C.; Kanthala, A.R.; Smith, V.D.; Manivannan, V.; Bellolio, M.F.; Decker, W.W. Anaphylaxis in emergency department patients 50 or 65 years or older. Ann. Allergy Asthma Immunol. 2011, 106, 401–406. [Google Scholar] [CrossRef]
- Lieberman, P.; Simons, F.E.R. Anaphylaxis and cardiovascular disease: Therapeutic dilemmas. Clin. Exp. Allergy 2015, 45, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Hess, E.P.; Nestler, D.M.; Bellamkonda Athmaram, V.R.; Bellolio, M.F.; Decker, W.W.; Li, J.T.C.; Hagan, J.B.; Manivannan, V.; Vukov, S.C.; et al. Antihypertensive medication use is associated with increased organ system involvement and hospitalization in emergency department patients with anaphylaxis. J. Allergy Clin. Immunol. 2013, 131, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.; Pace, A.J.; Koller, B.H. Age-induced reprogramming of mast cell degranulation. J. Immunol. 2005, 175, 5701–5707. [Google Scholar] [CrossRef] [PubMed]
- Sturm, G.J.; Varga, E.M.; Roberts, G.; Mosbech, H.; Bilò, M.B.; Akdis, C.A.; Antolín-Amérigo, D.; Cichocka-Jarosz, E.; Gawlik, R.; Jakob, T.; et al. EAACI guidelines on allergen immunotherapy: Hymenoptera venom allergy. Allergy 2018, 73, 744–764. [Google Scholar] [CrossRef] [PubMed]
- Pawelec, G. Age and immunity: What is “immunosenescence”? Exp. Gerontol. 2018, 105, 4–9. [Google Scholar] [CrossRef]
- Williams, M.E.; Rosenthal, T.; Naughton, B. Geriatria: Kontakt z pacjentem w starszym wieku; Wydawnictwo Czelej Sp. z oo: Lublin, 2009; pp. 1–19. ISBN 978-83-606-0863-0. [Google Scholar]
- Biló, M.B.; Rueff, F.; Mosbech, H.; Bonifazi, F.; Oude-Elberink, J.N.G. Diagnosis of Hymenoptera venom allergy, EAACI Interest Group on Insect Venom Hypersensitivity. Allergy 2005, 11, 1339–1349. [Google Scholar] [CrossRef]
- Vidal, C. The Asian wasp Vespa velutina nigrithorax: Entomological and allergological characteristics. Clin. Exp. Allergy 2022, 52, 489–498. [Google Scholar] [CrossRef]
- van der Linden, P.W.; Hack, C.E.; Struyvenberg, A.; van der Zwan, J.K. Insect-sting challenge in 324 subjects with a previous anaphylactic reaction: Current criteria for insect-venom hypersensitivity do not predict the occurrence and the severity of anaphylaxis. J. Allergy Clin. Immunol. 1994, 94, 151–159. [Google Scholar] [CrossRef]
- Arzt, L.; Bokanovic, D.; Schwarz, I.; Schrautzer, C.; Massone, C.; Horn, M.; Aberer, W.; Sturm, G. Hymenoptera stings in the head region induce impressive, but not severe sting reactions. Allergy 2016, 11, 1632–1634. [Google Scholar] [CrossRef]
- Pumphrey, R.S. Lessons for management of anaphylaxis from a study of fatal reactions. Clin. Exp. Allergy. 2000, 30, 1144–1150. [Google Scholar] [CrossRef]
- Guenova, E.; Volz, T.; Eichner, M.; Hoetzenecker, W.; Caroli, U.; Griesinger, G.; Mitev, V.; Biedermann, T. Basal serum tryptase as risk assessment for severe Hymenoptera sting reactions in elderly. Allergy 2010, 65, 919–923. [Google Scholar] [CrossRef] [PubMed]
- Bonadonna, P.; Perbellini, O.; Passalacqua, G.; Caruso, B.; Colarossi, S.; Dal Fior, D.; Castellani, L.; Bonetto, C.; Frattini, F.; Dama, A. Clonal mast cell disorders in patients with systemic reactions to hymenoptera stings and increased serum tryptase levels. J. Allergy Clin. Immunol. 2009, 123, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Kucharewicz, I.; Bodzenta-Lukaszyk, A.; Szymanski, W.; Mroczko, B.; Szmitkowski, M. Basal serum tryptase level correlates with severity of hymenoptera sting and age. J. Investig. Allergol. Clin. Immunol. 2007, 17, 65–69. [Google Scholar] [PubMed]
- Niedoszytko, M.; de Monchy, J.; van Doormaal, J.J.; Jassem, E.; Oude Elberink, J.N. Mastocytosis and insect venom allergy: Diagnosis, safety and efficacy of venom immunotherapy. Allergy 2009, 64, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Stoevesandt, J.; Hain, J.; Kerstan, A.; Trautmann, A. Over- and underestimated parameters in severe Hymenoptera venom-induced anaphylaxis: Cardiovascular medication and absence of urticaria/angioedema. J. Allergy Clin. Immunol. 2012, 130, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Scichilone, N.; Callari, A.; Augugliaro, G.; Marchese, M.; Togias, A.; Bellia, V. The impact of age on prevalence of positive skin prick tests and specific IgE tests. Respir. Med. 2011, 105, 651–658. [Google Scholar] [CrossRef]
- Mediaty, A.; Neuber, K. Total and specific serum IgE decreases with age in patients with allergic rhinitis, asthma and insect allergy but not in patients with atopic dermatitis. Immun. Aging 2005, 2, 9. [Google Scholar] [CrossRef]
- Scichilone, N.; Augugliaro, G.; Togias, A.; Bellia, V. Should atopy be assessed in elderly patients with respiratory symptoms suggestive of asthma? Expert Rev. Respir. Med. 2010, 4, 585–589. [Google Scholar] [CrossRef]
- Cardona, V.; Guilarte, M.; Luengo, O.; Labrador-Horrillo, M.; Sala-Cunill, A.; Garriga, T. Allergic diseases in the elderly. Clin. Transl. Allergy. 2011, 1, 11. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Patients <60 Years of Age N = 750 | Patients ≥ 60 Years of Age N = 132 | p |
|---|---|---|---|
| Gender women/men | 395/355 | 88/44 | p = 0.03 |
| Age [years] median (min–max) | 40 (11.0–59.0) | 64 (60.0–79.0) | |
| Ischemic heart disease n (%) | 12 (1.60) | 13 (9.84) | p = 0.00 |
| Arterial hypertension n (%) | 150 (20.00) | 76 (57.57) | p = 0.00 |
| Diabetes n (%) | 7 (0.93) | 18 (13.63) | p = 0.00 |
| Allergy n (%) | 124 (16.53) | 27 (20.45) | p = 0.27 |
| Thyroid diseases | 68 (9.06) | 27 (20.45) | p = 0.00 |
| Beta-blockers | 41 (5.46) | 32 (24.24) | p = 0.00 |
| ACEi | 52 (6.93) | 28 (21.21) | p = 0.00 |
| ARBs | 39 (5.2) | 25 (18.9) | p = 0.00 |
| Parameters | Patients <60 Years of Age N = 750 | Patients ≥ 60 Years of Age N = 132 | p |
|---|---|---|---|
| Bee venom allergy | 211 (28.14%) | 35 (26.52%) | p = 0.78 |
| Wasp venom allergy | 514 (68.53%) | 94 (71.21%) | |
| Bee and wasp venom allergy | 25 (3.33%) | 3 (2.27%) | |
| Total IgE median (min-max) | 63.50 (5.44–1670.00) | 59.10 (4.20–4590.00) | p = 0.49 |
| Insect specific IgE mean (min–max) sIgE Api m 1 | 5.01 (0.00–64.90) | 6.39 (0.00–67.80) | p* = 0.66 |
| Insect specific IgE mean (min-max) sIgE Api m 2 | 1.59 (0.00–23.20) | 1.98 (0.00–20.87) | p* = 0.33 |
| Insect specific IgE mean (min-max) sIgE Api m 5 | 0.48 (0.00–3.00) | 0.71 (0.00–7.77) | p* = 0.07 |
| Insect specific IgE mean (min-max) sIgE Api m 10 | 2.98 (0.00–47.70) | 4.98 (0.01–86.30) | p* = 0.15 |
| Insect specific IgE ean (min-max) sIgE Ves v1 | 5.89 (0.00–100.00) | 9.50 (0.00–100.00) | p* = 0.004 |
| Insect specific IgE mean (min-max) sIgE Ves v5 | 7.23 (0.00–100.00) | 6.91 (0.00–100.00) | p* = 0.009 |
| IDT (diameter) [mm] median (min-max) | 11.00 (0.00–24.00) | 11.00 (0.00–20.00) | p = 0.65 |
| IDT (area) [mm2] median (min-max) | 94.00 (0.00–1838.00) | 94.00 (0.00–307.00) | p = 0.67 |
| sBT [ng/mL] median (min-max) | 4.31 (1.00–65.80) | 6.01 (1.98–16,100) | p = 0.000 |
| Parameters | The Elderly Patients ≤64 Years of Age N = 819 | The Elderly Patients ≥ 65 Years of Age N = 63 | p |
|---|---|---|---|
| Age [years] median; (min-max) | 42 (11–64) | 68 (65–79) | |
| Gender women/men | 380/46 | 19/30 | p = 0.001 |
| Insect specific IgE median; (min-max) | 4.1 (0.00–101.0) | 3.0 (0.0–91.8) | p > 0.05 |
| Total IgE median; (min-max) | 65.7 (4.2–4590.0) | 55.5 (9.1–967.0) | p > 0.05 |
| IDT (diameter) [mm] median; (min-max) | 11.0 (0.0–24.0) | 12.0 (0.0–20.0) | p > 0.05 |
| IDT (area) [mm2] median; (min-max) | 94.0 (0.0–1838.0) | 112.0 (0.0–240.0) | p > 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawłowicz, R.; Bożek, A.; Dor-Wojnarowska, A.; Rosiek-Biegus, M.; Kopeć, A.; Gillert-Smutnicka, M.; Sobieszczańska, M.; Nittner-Marszalska, M. Elderly Patients and Insect Venom Allergy: Are the Clinical Pictures and Immunological Parameters of Venom Allergy Age-Dependent? Vaccines 2024, 12, 394. https://doi.org/10.3390/vaccines12040394
Pawłowicz R, Bożek A, Dor-Wojnarowska A, Rosiek-Biegus M, Kopeć A, Gillert-Smutnicka M, Sobieszczańska M, Nittner-Marszalska M. Elderly Patients and Insect Venom Allergy: Are the Clinical Pictures and Immunological Parameters of Venom Allergy Age-Dependent? Vaccines. 2024; 12(4):394. https://doi.org/10.3390/vaccines12040394
Chicago/Turabian StylePawłowicz, Robert, Andrzej Bożek, Anna Dor-Wojnarowska, Marta Rosiek-Biegus, Agnieszka Kopeć, Małgorzata Gillert-Smutnicka, Małgorzata Sobieszczańska, and Marita Nittner-Marszalska. 2024. "Elderly Patients and Insect Venom Allergy: Are the Clinical Pictures and Immunological Parameters of Venom Allergy Age-Dependent?" Vaccines 12, no. 4: 394. https://doi.org/10.3390/vaccines12040394