
Case Report: Long-Term Survival of a Patient with Cerebral Metastasized Ovarian Carcinoma Treated with a Personalized Peptide Vaccine and Anti-PD-1 Therapy

 , , , and
, , , and 
Abstract
:1. Introduction
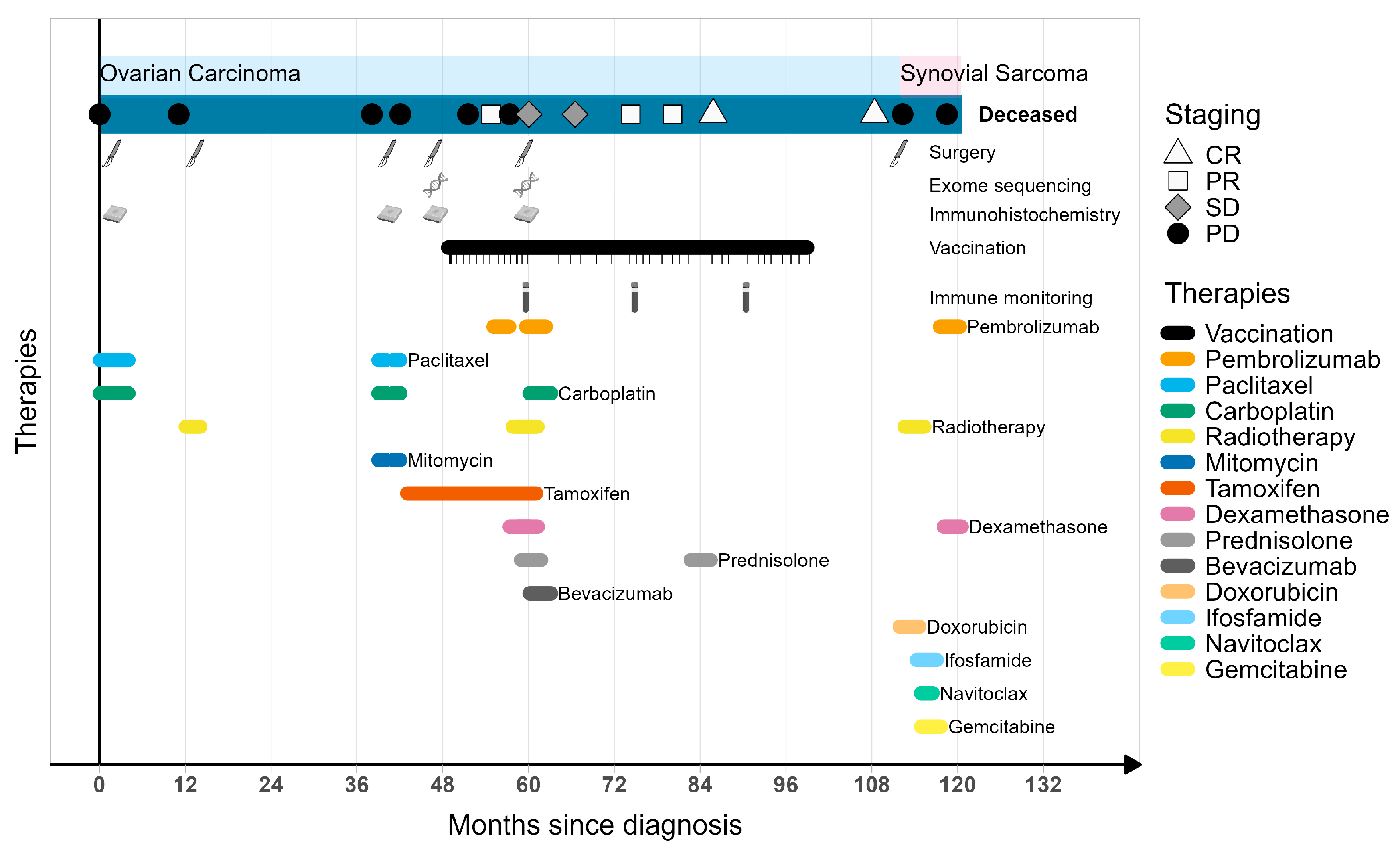
2. Case Description
3. Materials and Methods
3.1. Vaccination
3.2. Detection of Antigen-Specific T-Cell Responses
3.3. Immunohistochemistry
4. Results
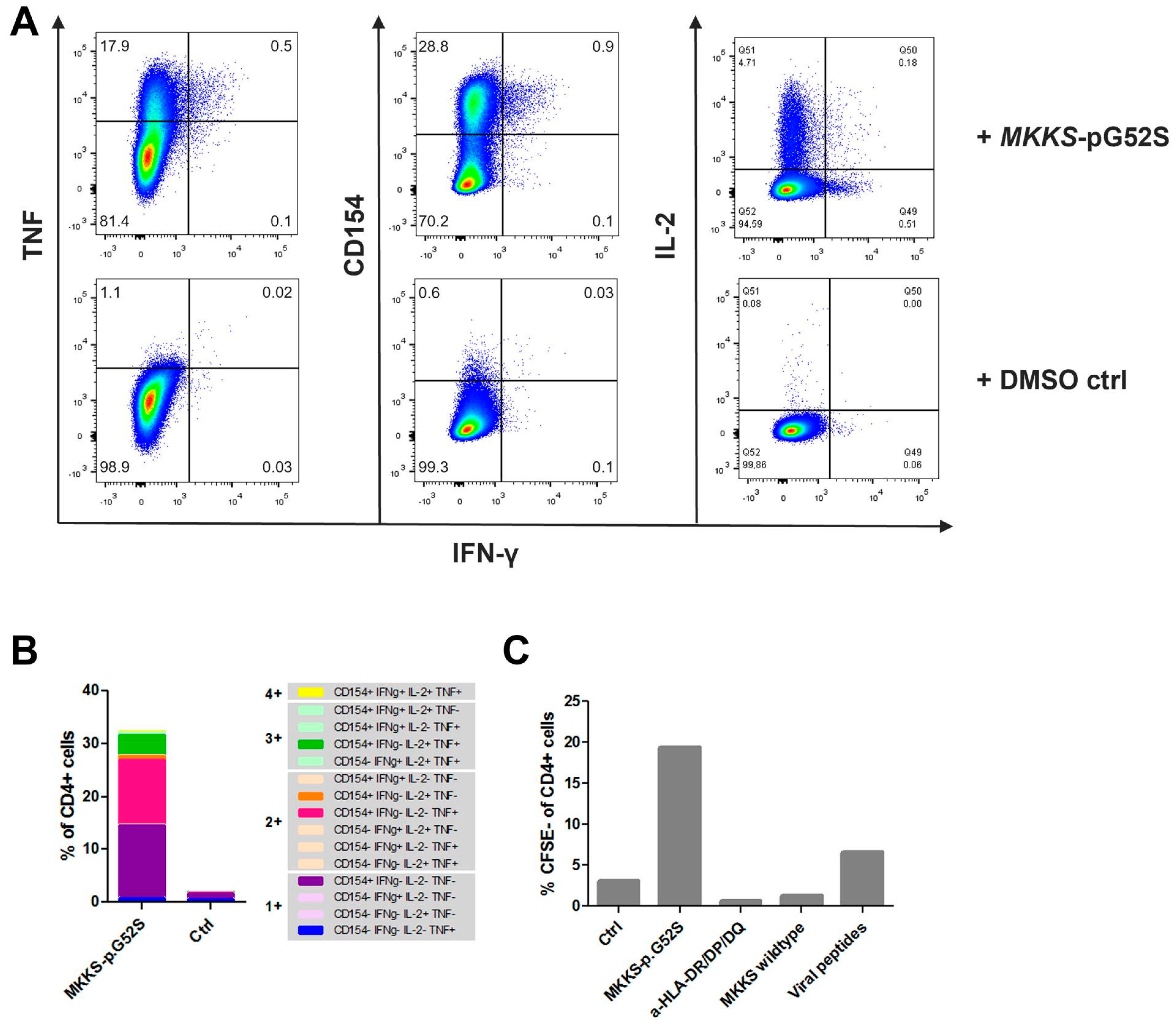
4.1. Immune Monitoring of Vaccine-Induced T-Cell Responses
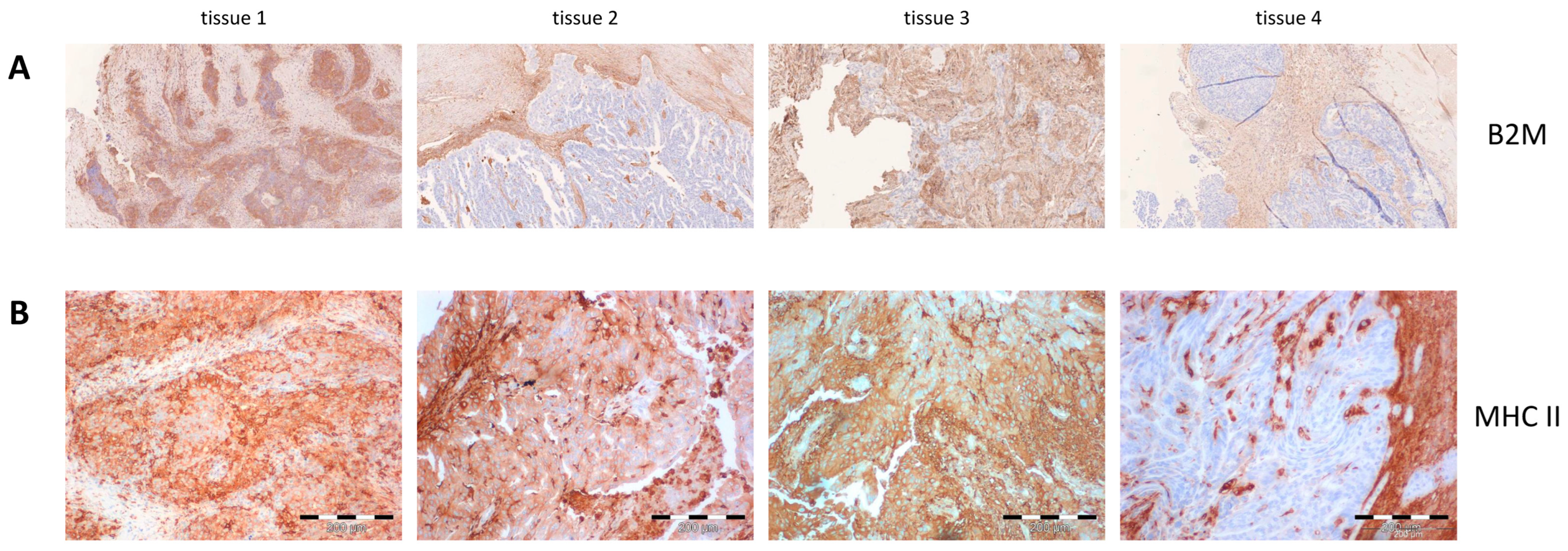
4.2. HLA Expression
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reid, B.M.; Permuth, J.B.; Sellers, T.A. Epidemiology of ovarian cancer: A review. Cancer Biol. Med. 2017, 14, 9–32. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Rassy, E.; Vermorken, J.B.; Assi, T.; Kattan, J.; Boussios, S.; Smith-Gagen, J. The outcome of patients with serous papillary peritoneal cancer, fallopian tube cancer, and epithelial ovarian cancer by treatment eras: 27 years data from the SEER registry. Cancer Epidemiol. 2021, 75, 102045. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 30, 672–705. [Google Scholar] [CrossRef]
- Poveda, A.M.; Selle, F.; Hilpert, F.; Reuss, A.; Savarese, A.; Vergote, I.; Witteveen, P.; Bamias, A.; Scotto, N.; Mitchell, L.; et al. Bevacizumab Combined With Weekly Paclitaxel Pegylated Liposomal Doxorubicin, or Topotecan in Platinum-Resistant Recurrent Ovarian Cancer: Analysis by Chemotherapy Cohort of the Randomized Phase III AURELIA Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 3836–3838. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet. Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Covens, A.; Carey, M.; Bryson, P.; Verma, S.; Fung Kee Fung, M.; Johnston, M. Systematic review of first-line chemotherapy for newly diagnosed postoperative patients with stage II, III, or IV epithelial ovarian cancer. Gynecol. Oncol. 2002, 85, 71–80. [Google Scholar] [CrossRef] [PubMed]
- van Altena, A.M.; Karim-Kos, H.E.; de Vries, E.; Kruitwagen, R.F.; Massuger, L.F.; Kiemeney, L.A. Trends in therapy and survival of advanced stage epithelial ovarian cancer patients in the Netherlands. Gynecol. Oncol. 2012, 125, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Steinberga, I.; Jansson, K.; Sorbe, B. Quality Indicators and Survival Outcome in Stage IIIB-IVB Epithelial Ovarian Cancer Treated at a Single Institution. Vivo 2019, 33, 1521–1530. [Google Scholar] [CrossRef]
- Hamanishi, J.; Mandai, M.; Ikeda, T.; Minami, M.; Kawaguchi, A.; Murayama, T.; Kanai, M.; Mori, Y.; Matsumoto, S.; Chikuma, S.; et al. Safety and Antitumor Activity of Anti-PD-1 Antibody Nivolumab, in Patients With Platinum-Resistant Ovarian Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 4015–4022. [Google Scholar] [CrossRef]
- Zamarin, D.; Burger, R.A.; Sill, M.W.; Powell, D.J., Jr.; Lankes, H.A.; Feldman, M.D.; Zivanovic, O.; Gunderson, C.; Ko, E.; Mathews, C.; et al. Randomized Phase II Trial of Nivolumab Versus Nivolumab and Ipilimumab for Recurrent or Persistent Ovarian Cancer: An NRG Oncology Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.B.; Disis, M.L. Development of Therapeutic vaccines for ovarian cancer. Gynecol. Oncol. 2013, 130, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Borella, F.; Bertero, L.; Morrone, A.; Gambella, A.; Bovetti, M.; Cosma, S.; Carosso, A.; Katsaros, D.; Gemmiti, S.; Preti, M.; et al. Brain Metastases from Ovarian Cancer: Current Evidence in Diagnosis Treatment, and Prognosis. Cancers 2020, 12, 2156. [Google Scholar] [CrossRef]
- Zelba, H.; McQueeney, A.; Rabsteyn, A.; Bartsch, O.; Kyzirakos, C.; Kayser, S.; Harter, J.; Latzer, P.; Hadaschik, D.; Battke, F.; et al. Adjuvant Treatment for Breast Cancer Patients Using Individualized Neoantigen Peptide Vaccination-A Retrospective Observation. Vaccines 2022, 10, 1882. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Hu, Z.; Keskin, D.B.; Shukla, S.A.; Sun, J.; Bozym, D.J.; Zhang, W.; Luoma, A.; Giobbie-Hurder, A.; Peter, L.; et al. An immunogenic personal neoantigen vaccine for patients with melanoma. Nature 2017, 547, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Rojas, L.A.; Sethna, Z.; Soares, K.C.; Olcese, C.; Pang, N.; Patterson, E.; Lihm, J.; Ceglia, N.; Guasp, P.; Chu, A.; et al. Personalized RNA neoantigen vaccines stimulate T cells in pancreatic cancer. Nature 2023, 618, 144–150. [Google Scholar] [CrossRef]
- Sahin, U.; Derhovanessian, E.; Miller, M.; Kloke, B.P.; Simon, P.; Löwer, M.; Bukur, V.; Tadmor, A.D.; Luxemburger, U.; Schrörs, B.; et al. Personalized RNA mutanome vaccines mobilize poly-specific therapeutic immunity against cancer. Nature 2017, 547, 222–226. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- Dadmarz, R.D.; Ordoubadi, A.; Mixon, A.; Thompson, C.O.; Barracchini, K.C.; Hijazi, Y.M.; Steller, M.A.; Rosenberg, S.A.; Schwartzentruber, D.J. Tumor-infiltrating lymphocytes from human ovarian cancer patients recognize autologous tumor in an MHC class II-restricted fashion. Cancer J. Sci. Am. 1996, 2, 263–272. [Google Scholar]
- Kruse, B.; Buzzai, A.C.; Shridhar, N.; Braun, A.D.; Gellert, S.; Knauth, K.; Pozniak, J.; Peters, J.; Dittmann, P.; Mengoni, M.; et al. CD4+ T cell-induced inflammatory cell death controls immune-evasive tumours. Nature 2023, 618, 1033–1040. [Google Scholar] [CrossRef]
- Wang, H.; Liu, B.; Wei, J. Beta2-microglobulin(B2M) in cancer immunotherapies: Biological function, resistance and remedy. Cancer Lett. 2021, 517, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Ning, Q.; Yang, L.; Mo, Z.; Tang, S. Mechanisms of immune escape in the cancer immune cycle. Int. Immunopharmacol. 2020, 86, 106700. [Google Scholar] [CrossRef]
- Reis, B.; Attig, J.; Dziadek, S.; Graefe, N.; Heller, A.; Rieder, N.; Gomes, B. Tumor beta2-microglobulin and HLA-A expression is increased by immunotherapy and can predict response to CIT in association with other biomarkers. Front. Immunol. 2024, 15, 1285049. [Google Scholar] [CrossRef]
- Zaretsky, J.M.; Garcia-Diaz, A.; Shin, D.S.; Escuin-Ordinas, H.; Hugo, W.; Hu-Lieskovan, S.; Torrejon, D.Y.; Abril-Rodriguez, G.; Sandoval, S.; Barthly, L.; et al. Mutations Associated with Acquired Resistance to PD-1 Blockade in Melanoma. N. Engl. J. Med. 2016, 375, 819–829. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Lu, B.; Melisko, M.; Price Hiller, J.; Bondarenko, I.; Brunt, A.M.; Sergii, G.; Petrakova, K.; Peoples, G.E. Efficacy and Safety Analysis of Nelipepimut-S Vaccine to Prevent Breast Cancer Recurrence: A Randomized Multicenter Phase III Clinical Trial. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 4248–4254. [Google Scholar] [CrossRef]
- Walter, S.; Weinschenk, T.; Stenzl, A.; Zdrojowy, R.; Pluzanska, A.; Szczylik, C.; Staehler, M.; Brugger, W.; Dietrich, P.Y.; Mendrzyk, R.; et al. Multipeptide immune response to cancer vaccine IMA901 after single-dose cyclophosphamide associates with longer patient survival. Nat. Med. 2012, 18, 1254–1261. [Google Scholar] [CrossRef] [PubMed]
- Blumendeller, C.; Boehme, J.; Frick, M.; Schulze, M.; Rinckleb, A.; Kyzirakos, C.; Kayser, S.; Kopp, M.; Kelkenberg, S.; Pieper, N.; et al. Use of plasma ctDNA as a potential biomarker for longitudinal monitoring of a patient with metastatic high-risk upper tract urothelial carcinoma receiving pembrolizumab and personalized neoepitope-derived multipeptide vaccinations: A case report. J. Immunother. Cancer 2021, 9, e001406. [Google Scholar] [CrossRef]
- Zelba, H.; Rabsteyn, A.; Bartsch, O.; Kyzirakos, C.; Kayser, S.; Seibold, M.; Harter, J.; Latzer, P.; Hadaschik, D.; Battke, F.; et al. Case Report: Targeting of individual somatic tumor mutations by multipeptide vaccination tailored for HLA class I and II presentation induces strong CD4 and CD8 T-cell responses in a patient with metastatic castration sensitive prostate cancer. Front. Immunol. 2023, 14, 1271449. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Neoantigenic Peptide | Gene and Variant | Predicted HLA Restriction | Variant Allele Frequency in the Lymph Node Metastasis (2014; Tissue 3) | Variant Allele Frequency in the Brain Metastasis (2015; Tissue 4) |
|---|---|---|---|---|
| PYRTKIY | GAN, NM_022041.3: c.179A>T; p.N60I | C*05:01 | 0.94 | 0.94 |
| KQLHNGFGSY | MKKS, NM_018848.3: c.154G>A; p.G52S | A*32:01, C*14:02 | 0.76 | 1.00 |
| SMSAETMEL | BTN3A2, NM_001197247.2: c.170C>G; p.T57S | A*02:01, A*32:01, | 0.50 | 0.81 |
| AETANLEEQL | ARL6IP1, NM_015161.1: c.53G>A; p.S18N | C*14:02 | 0.46 | 0.93 |
| DPSTLGSL | SYT6, NM_205848.3: c.125T>C; p.F42S | B*44:02 | 0.32 | 0.30 |
| EHAKAVVSFRHIQRRAA | CCHCR1, NM_001105564:c.A2178C:p.L726F (somatic) and c.2184G>T:p.Q728H (single nucleotide polymorphism) | HLA class II | 0.44 | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zelba, H.; Kyzirakos, C.; Kayser, S.; Shao, B.; Reinhardt, A.; Pieper, N.; Rabsteyn, A.; Döcker, D.; Armeanu-Ebinger, S.; Kloor, M.; et al. Case Report: Long-Term Survival of a Patient with Cerebral Metastasized Ovarian Carcinoma Treated with a Personalized Peptide Vaccine and Anti-PD-1 Therapy. Vaccines 2024, 12, 397. https://doi.org/10.3390/vaccines12040397
Zelba H, Kyzirakos C, Kayser S, Shao B, Reinhardt A, Pieper N, Rabsteyn A, Döcker D, Armeanu-Ebinger S, Kloor M, et al. Case Report: Long-Term Survival of a Patient with Cerebral Metastasized Ovarian Carcinoma Treated with a Personalized Peptide Vaccine and Anti-PD-1 Therapy. Vaccines. 2024; 12(4):397. https://doi.org/10.3390/vaccines12040397
Chicago/Turabian StyleZelba, Henning, Christina Kyzirakos, Simone Kayser, Borong Shao, Annekathrin Reinhardt, Natalia Pieper, Armin Rabsteyn, Dennis Döcker, Sorin Armeanu-Ebinger, Matthias Kloor, and et al. 2024. "Case Report: Long-Term Survival of a Patient with Cerebral Metastasized Ovarian Carcinoma Treated with a Personalized Peptide Vaccine and Anti-PD-1 Therapy" Vaccines 12, no. 4: 397. https://doi.org/10.3390/vaccines12040397