

Distinct Adverse Reactions to mRNA, Inactivated Virus, and Adenovirus Vector COVID-19 Vaccines: Insights from a Cohort Study on Atopic and Non-Atopic Subjects in Brazil
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. SPT with Airborne Allergens and D. farinae-Specific IgE ELISA
2.3. Statistical Analysis
3. Results
3.1. Atopic and Non-Atopic Groups
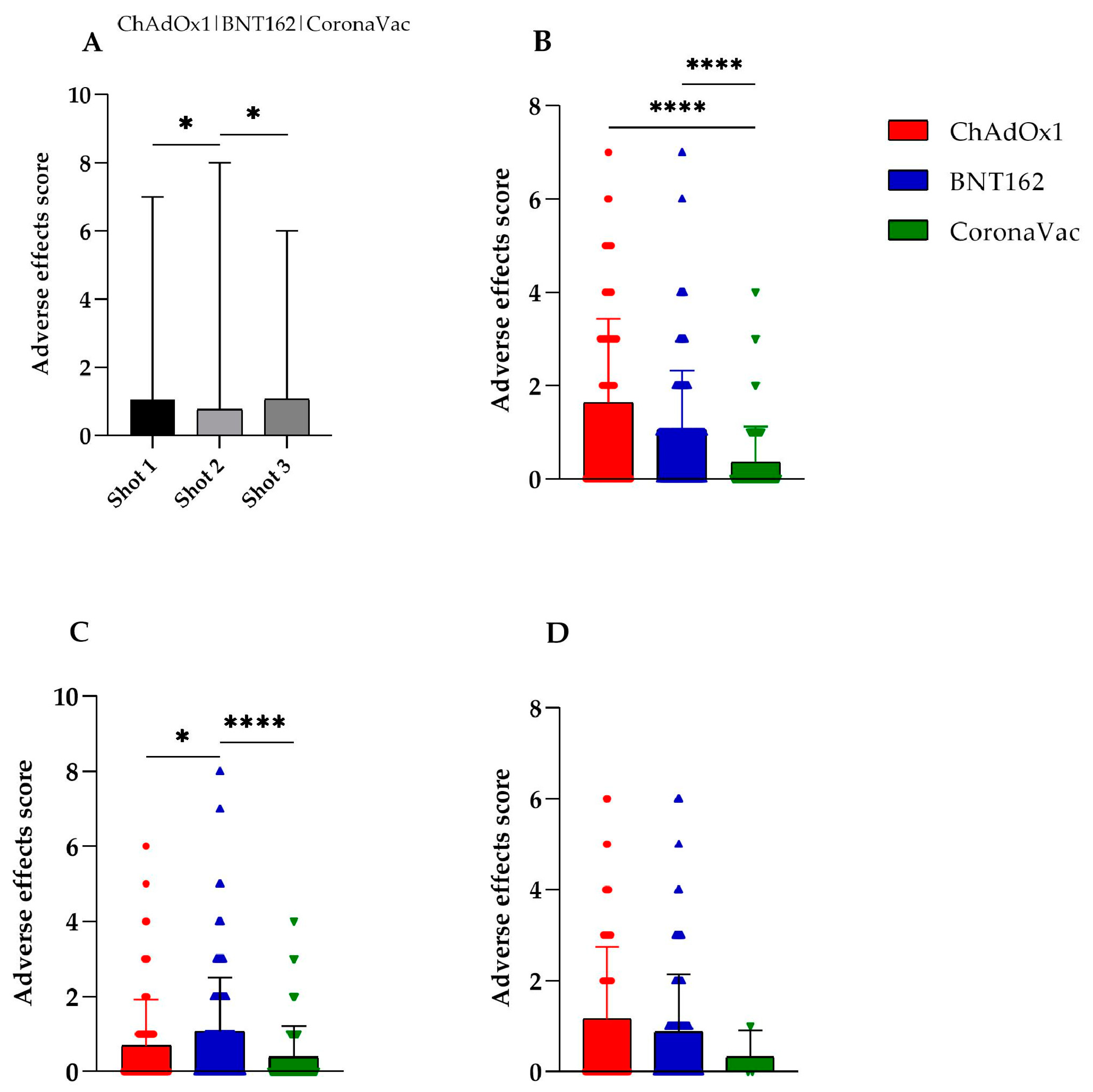
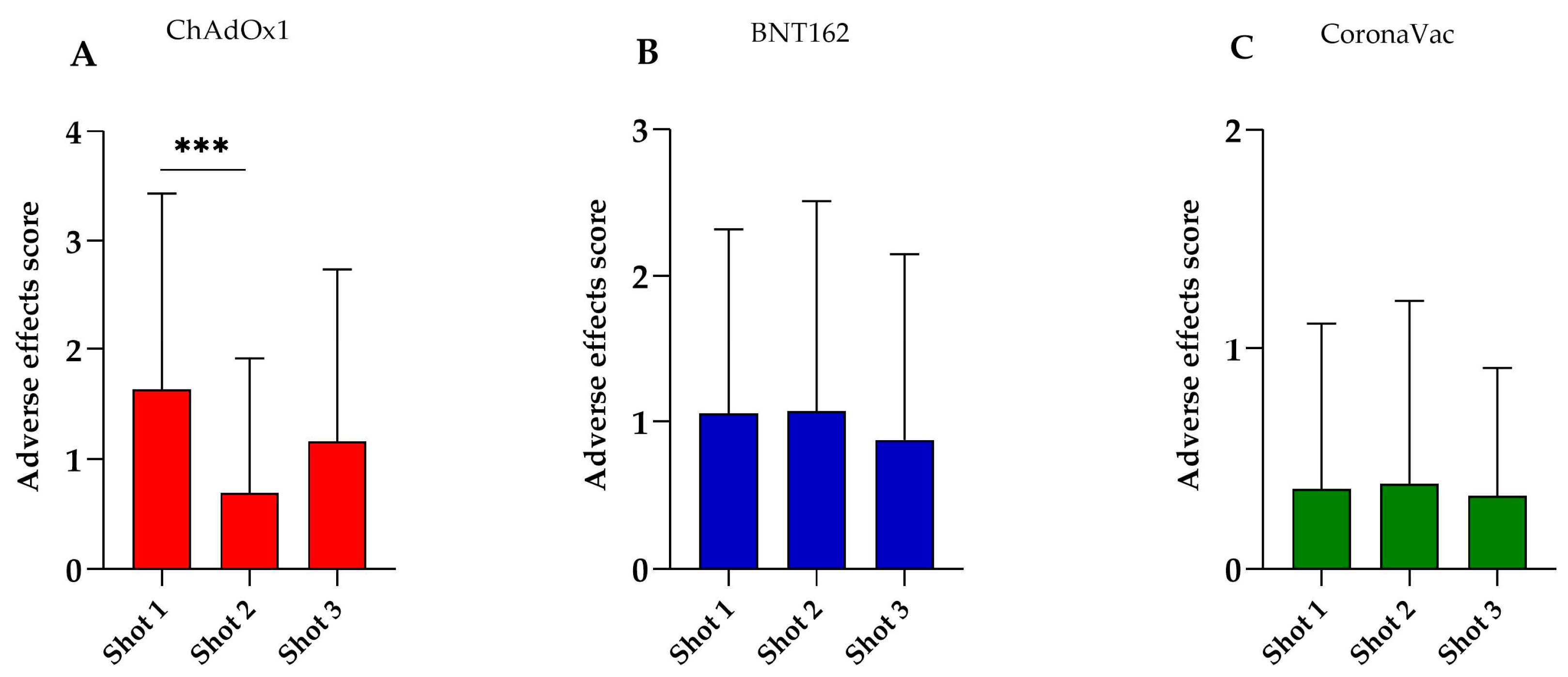
3.2. Adverse Effects of the COVID-19 Vaccines
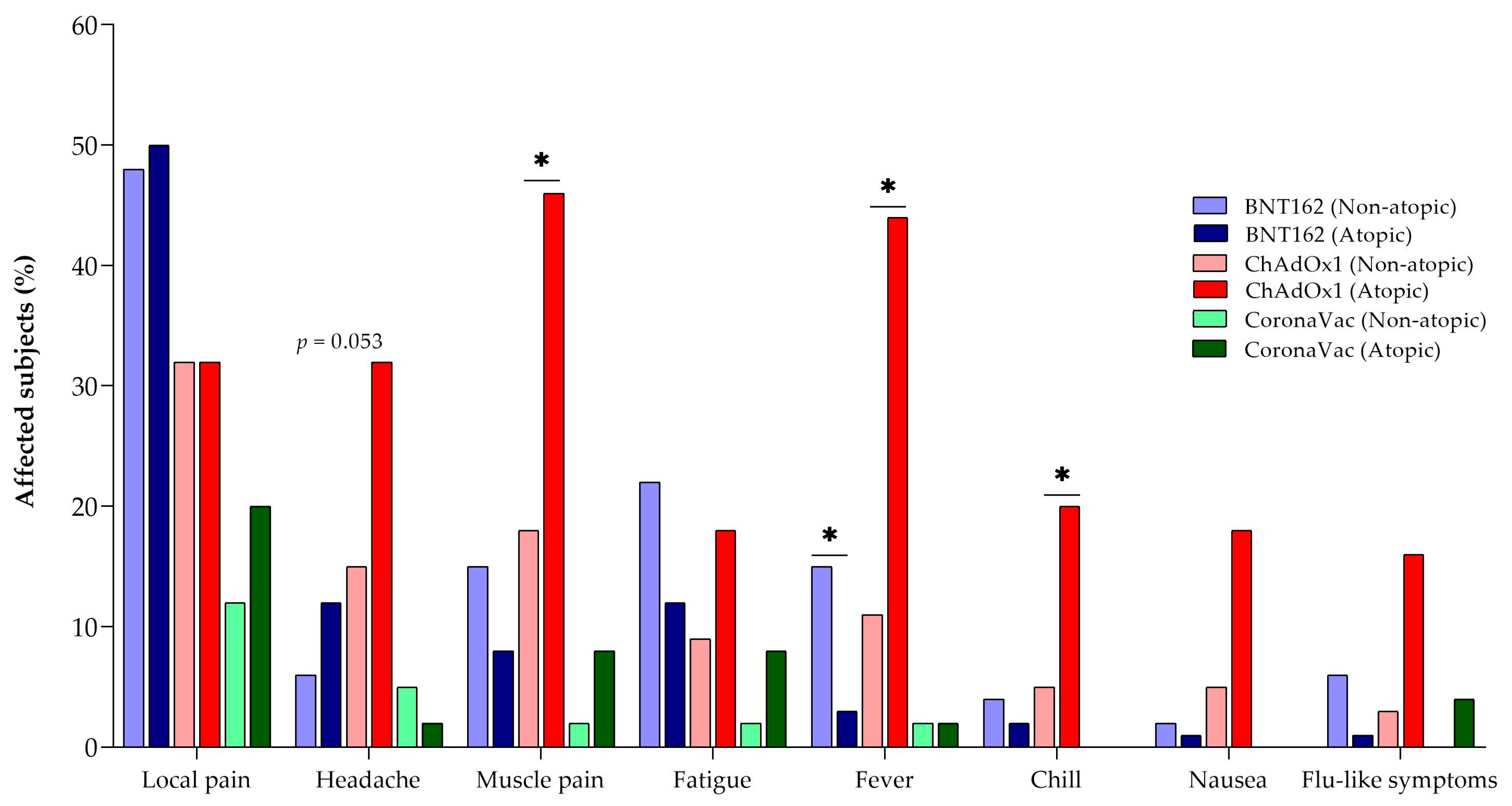
3.3. Adverse Effects of the COVID-19 Vaccines in Atopic and Non-Atopic Subjects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, K.L.; Best, E.; Crawford, N.W.; Giles, M.; Koirala, A.; Macartney, K.; Russell, F.; Teh, B.W.; Wen, S.C. Progress and pitfalls in the quest for effective SARS-CoV-2 (COVID-19) vaccines. Front. Immunol. 2020, 11, 2410. [Google Scholar] [CrossRef] [PubMed]
- Corey, L.; Miner, M.D. Accelerating clinical trial development in vaccinology: COVID-19 and beyond. Curr. Opin. Immunol. 2022, 76, 102206. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.; Meißner, J.; Grabski, E.; Sun, Y.; Vieths, S.; Hildt, E. Regulatory concepts to guide and promote the accelerated but safe clinical development and licensure of COVID-19 vaccines in Europe. Allergy 2022, 77, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Le, T.T.; Cramer, J.P.; Chen, R.; Mayhew, S. Evolution of the COVID-19 vaccine development landscape. Nat. Rev. Drug. Discov. 2020, 19, 667–668. [Google Scholar] [CrossRef] [PubMed]
- Eterafi, M.; Fouladi, N.; Golizadeh, M.; Shaker, H.; Matin, S.; Safarzadeh, E. Reported side-effects following Oxford/AstraZeneca COVID-19 vaccine in the north-west province, Iran: A cross-sectional study. PLoS ONE 2024, 19, e0296669. [Google Scholar] [CrossRef] [PubMed]
- Firouzabadi, N.; Ghasemiyeh, P.; Moradishooli, F.; Mohammadi-Samani, S. Update on the effectiveness of COVID-19 vaccines on different variants of SARS-CoV-2. Int. Immunopharmacol. 2023, 117, 109968. [Google Scholar] [CrossRef] [PubMed]
- Mallapaty, S.; Callaway, E.; Kozlov, M.; Ledford, H.; Pickrell, J.; Van Noorden, R. How COVID vaccines shaped 2021 in eight powerful charts. Nature 2021, 600, 580–583. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef]
- Gálvez, N.M.S.; Pacheco, G.A.; Schultz, B.M.; Melo-González, F.; Soto, J.A.; Duarte, L.F.; González, L.A.; Rivera-Pérez, D.; Ríos, M.; Berrios, R.V.; et al. Differences in the immune response elicited by two immunization schedules with an inactivated SARS-CoV-2 vaccine in a randomized phase 3 clinical trial. eLife 2022, 11, 81477. [Google Scholar] [CrossRef]
- Ortega, M.M.; da Silva, L.T.; Candido, É.D.; Zheng, Y.; Tiyo, B.T.; Ferreira, A.E.F.; Corrêa-Silva, S.; Scagion, G.P.; Leal, F.B.; Chalup, V.N.; et al. Salivary, serological, and cellular immune response to the CoronaVac vaccine in health care workers with or without previous COVID-19. Sci. Rep. 2022, 12, 10125. [Google Scholar] [CrossRef]
- Graña, C.; Ghosn, L.; Evrenoglou, T.; Jarde, A.; Minozzi, S.; Bergman, H.; Buckley, B.S.; Probyn, K.; Villanueva, G.; Henschke, N.; et al. Efficacy and safety of COVID-19 vaccines. Cochrane. Database Syst. Rev. 2022, 12, Cd015477. [Google Scholar] [CrossRef]
- Luxi, N.; Giovanazzi, A.; Arcolaci, A.; Bonadonna, P.; Crivellaro, M.A.; Cutroneo, P.M.; Ferrajolo, C.; Furci, F.; Guidolin, L.; Moretti, U.; et al. Allergic Reactions to COVID-19 Vaccines: Risk Factors, Frequency, Mechanisms and Management. BioDrugs 2022, 36, 443–458. [Google Scholar] [CrossRef]
- Desai, A.P.; Desai, A.P.; Loomis, G.J. Relationship between pre-existing allergies and anaphylactic reactions post mRNA COVID-19 vaccine administration. Vaccine 2021, 39, 4407–4409. [Google Scholar] [CrossRef]
- Yoshida, M.; Kobashi, Y.; Shimazu, Y.; Saito, H.; Yamamoto, C.; Kawamura, T.; Wakui, M.; Takahashi, K.; Ito, N.; Nishikawa, Y.; et al. Time course of adverse reactions following BNT162b2 vaccination in healthy and allergic disease individuals aged 5–11 years and comparison with individuals aged 12–15 years: An observational and historical cohort study. Eur. J. Pediatr. 2023, 182, 123–133. [Google Scholar] [CrossRef]
- Bian, S.; Li, L.; Wang, Z.; Cui, L.; Xu, Y.; Guan, K.; Zhao, B. Allergic Reactions After the Administration of COVID-19 Vaccines. Front. Public Health 2022, 10, 878081. [Google Scholar] [CrossRef]
- Nittner-Marszalska, M.; Rosiek-Biegus, M.; Kopeć, A.; Pawłowicz, R.; Kosińska, M.; Łata, A.; Szenborn, L. Pfizer-BioNTech COVID-19 vaccine tolerance in allergic versus non-allergic individuals. Vaccine 2021, 9, 553. [Google Scholar] [CrossRef]
- Wang, J.; Zhou, Y.; Zhang, H.; Hu, L.; Liu, J.; Wang, L.; Wang, T.; Zhang, H.; Cong, L.; Wang, Q. Pathogenesis of allergic diseases and implications for therapeutic interventions. Signal Transduct. Target Ther. 2023, 8, 138. [Google Scholar] [CrossRef]
- Uzer, F.; Cilli, A. Acute asthma exacerbation after SARS-CoV-2 vaccine (Sinovac®): A case report. Med. Gas Res. 2022, 12, 67–68. [Google Scholar] [CrossRef]
- Johansson, S.G.; Bieber, T.; Dahl, R.; Friedmann, P.S.; Lanier, B.Q.; Lockey, R.F.; Motala, C.; Ortega Martell, J.A.; Platts-Mills, T.A.; Ring, J.; et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J. Allergy Clin. Immunol. 2004, 113, 832–836. [Google Scholar] [CrossRef]
- Testera-Montes, A.; Salas, M.; Palomares, F.; Ariza, A.; Torres, M.J.; Rondón, C.; Eguiluz-Gracia, I. Local Respiratory Allergy: From Rhinitis Phenotype to Disease Spectrum. Front. Immunol. 2021, 12, 691964. [Google Scholar] [CrossRef]
- Breiteneder, H.; Peng, Y.Q.; Agache, I.; Diamant, Z.; Eiwegger, T.; Fokkens, W.J.; Traidl-Hoffmann, C.; Nadeau, K.; O’Hehir, R.E.; O’Mahony, L.; et al. Biomarkers for diagnosis and prediction of therapy responses in allergic diseases and asthma. Allergy 2020, 75, 3039–3068. [Google Scholar] [CrossRef]
- Mersha, T.B.; Afanador, Y.; Johansson, E.; Proper, S.P.; Bernstein, J.A.; Rothenberg, M.E.; Khurana Hershey, G.K. Resolving Clinical Phenotypes into Endotypes in Allergy: Molecular and Omics Approaches. Clin. Rev. Allergy 2021, 60, 200–219. [Google Scholar] [CrossRef]
- Wang, X.; Sima, Y.; Zhao, Y.; Zhang, N.; Zheng, M.; Du, K.; Wang, M.; Wang, Y.; Hao, Y.; Li, Y.; et al. Endotypes of chronic rhinosinusitis based on inflammatory and remodeling factors. J. Allergy Clin. Immunol. 2023, 151, 458–468. [Google Scholar] [CrossRef]
- Fernandes, J.F.; Taketomi, E.A.; Mineo, J.R.; Miranda, D.O.; Alves, R.; Resende, R.O.; Ynoue, L.H.; Sung, S.S.; Silva, D.A. Antibody and cytokine responses to house dust mite allergens and Toxoplasma gondii antigens in atopic and non-atopic Brazilian subjects. Clin. Immunol. 2010, 136, 148–156. [Google Scholar] [CrossRef]
- Meltendorf, S.; Vogel, K.; Thurm, C.; Prätsch, F.; Reinhold, A.; Färber, J.; Heuft, H.G.; Kaasch, A.J.; Hachenberg, T.; Weinzierl, S.; et al. IL-13 determines specific IgE responses and SARS-CoV-2 immunity after mild COVID-19 and novel mRNA vaccination. Eur. J. Immunol. 2022, 52, 1972–1979. [Google Scholar] [CrossRef]
- Correa, A.S.; Miranda, J.S.; Oliveira, L.A.R.; Moreira, P.F.S.; Vieira, F.A.M.; Cunha-Junior, J.P.; Resende, R.O.; Taketomi, E.A. Identification of carboxymethyl (CM)-binding proteins derived from Lolium multiflorum pollen extract and antibody reactivity in Brazilian allergic patients. Braz. J. Med. Biol. 2023, 56, e12957. [Google Scholar] [CrossRef]
- Resende, R.O.; Ynoue, L.H.; Miranda, J.S.; de Almeida, K.C.; Silva, D.A.O.; Sopelete, M.C.; Alves, R.; Gennari-Cardoso, M.L.; Taketomi, E.A. IgE, IgG1, and IgG4 Reactivity to Dermatophagoides pteronyssinus Glycosylated Extract in Allergic Patients. BioMed Res. Int. 2019, 2019, 9840890. [Google Scholar] [CrossRef]
- Almeida, K.C.; Silva, D.A.; Gennari-Cardoso, M.L.; Cunha-Júnior, J.P.; Alves, R.; Ynoue, L.H.; Resende, R.O.; Sung, S.J.; Taketomi, E.A. Responses of IgE, IgG1, and IgG4 to concanavalin A-binding Blomia tropicalis antigens in allergic patients. Braz. J. Med. Biol. 2006, 39, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, L.; Llinás-Caballero, K. The Relationship of Parasite Allergens to Allergic Diseases. Curr. Allergy Asthma Rep. 2023, 23, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.L.; Grabenstein, J.D.; Braun, M.M. Answering Key Questions About COVID-19 Vaccines. JAMA 2020, 324, 2027–2028. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Yesuf, E.A.; Riad, A.; Sofi-Mahmudi, A.; Sudhakar, M.; Mekonnen, A.; Endalkachew, S.; Mama, F.; Muhidin, S.; Ayele, B.; Yahya, M.; et al. Self-reported side effects of the Oxford AstraZeneca COVID-19 vaccine among healthcare workers in Ethiopia, Africa: A cross-sectional study. Front. Public Health 2022, 10, 937794. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomized, controlled, phase 2/3 trial. Lancet 2020, 396, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Caminati, M.; Guarnieri, G.; Batani, V.; Scarpieri, E.; Finocchiaro, A.; Chieco-Bianchi, F.; Senna, G.; Vianello, A. COVID-19 vaccination in patients with severe asthma on biologic treatment: Safety, tolerability, and impact on disease control. Vaccine 2021, 9, 853. [Google Scholar] [CrossRef]
- Atayik, E.; Aytekіn, G.J.M. Are allergic diseases a risk factor for systemic side effects after COVID-19 vaccines? medRxiv 2022, 22269704. [Google Scholar] [CrossRef]
- Cao, C.; Qiu, F.; Lou, C.; Fang, L.; Liu, F.; Zhong, J.; Sun, W.; Ding, W.; Yu, X.; Xu, Q.; et al. Safety of inactivated SARS-CoV-2 vaccines in patients with allergic diseases. Respir. Res. 2022, 23, 133. [Google Scholar] [CrossRef]
- Cabanillas, B.; Akdis, C.; Novak, N. Allergic reactions to the first COVID-19 vaccine: A potential role of Polyethylene glycol. Allergy 2021, 76, 1617–1618. [Google Scholar] [CrossRef] [PubMed]
- Sokolowska, M.; Eiwegger, T.; Ollert, M.; Torres, M.J.; Barber, D.; Del Giacco, S.; Jutel, M.; Nadeau, K.C.; Palomares, O.; Rabin, R.L.; et al. EAACI statement on the diagnosis, management and prevention of severe allergic reactions to COVID-19 vaccines. Allergy 2021, 76, 1629–1639. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.B.; Perkins, G.; Ryoo, D.; Lee, M.; Tunbridge, M.; Yuson, C.; Smith, W.; Hissaria, P.; Le, T.-T. AstraZeneca ChAdOx1-S COVID-19 vaccine can be safely administered in patients with EDTA allergy. Allergy Asthma Clin. Immunol. 2022, 18, 22. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Atopic 1 | Non-Atopic 1 | Total | p |
|---|---|---|---|---|
| Participants [n (%)] | 166 (54.4%) | 139 (45.6%) | 305 | - |
| Male [n (%)] | 63 (37.9%) | 37 (26.6%) | 100 | 0.0381 |
| Female [n (%)] | 103 (62.1%) | 102 (73.3%) | 205 | |
| Age (years, mean) | 30.7 | 35.0 | - | 0.0240 |
| Allergic rhinitis [n (%)] | 116 (69.8%) | 53 (38.2%) | 169 | 0.4819 |
| Asthma [n (%)] | 1 (0.6%) | 1 (0.7%) | 2 | |
| Allergic rhinitis and asthma [n (%)] | 16 (9.6%) | 4 (2.8%) | 20 | |
| D. farinae wheal size (mm, mean) | 5.5 | 0 | - | 0.0001 |
| D. farinae-specific IgE (mean) | 2.4 | 0.7 | - | 0.0001 |
| Adverse Effect | BNT162 | ChAdOx1 | CoronaVac |
|---|---|---|---|
| Local pain | 61 (49.6%) | 31 (31.9%) | 14 (16.5%) |
| Headache | 13 (10.5%) | 22 (22.7%) | 3 (3.5%) |
| Muscle pain | 14 (11.4%) | 30 (30.9%) | 5 (5.9%) |
| Fatigue | 20 (16.3%) | 13 (13.4%) | 5 (5.9%) |
| Fever | 10 (8.1%) | 25 (25.8%) | 2 (2.3%) |
| Chill | 4 (3.2%) | 12 (12.4%) | 0 (0%) |
| Lymph node enlargement | 1 (0.8%) | 1 (1%) | 0 (0%) |
| Nausea | 2 (1.6%) | 11 (11.3%) | 0 (0%) |
| Flu-like symptoms | 4 (3.2%) | 9 (9.3%) | 2 (2.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, L.A.R.; Correa, A.S.; de Jesus, T.A.; Bortolini, M.J.S.; Taketomi, E.A.; Resende, R.d.O. Distinct Adverse Reactions to mRNA, Inactivated Virus, and Adenovirus Vector COVID-19 Vaccines: Insights from a Cohort Study on Atopic and Non-Atopic Subjects in Brazil. Vaccines 2024, 12, 408. https://doi.org/10.3390/vaccines12040408
Oliveira LAR, Correa AS, de Jesus TA, Bortolini MJS, Taketomi EA, Resende RdO. Distinct Adverse Reactions to mRNA, Inactivated Virus, and Adenovirus Vector COVID-19 Vaccines: Insights from a Cohort Study on Atopic and Non-Atopic Subjects in Brazil. Vaccines. 2024; 12(4):408. https://doi.org/10.3390/vaccines12040408
Chicago/Turabian StyleOliveira, Laura Alves Ribeiro, Alessandro Sousa Correa, Thiago Alves de Jesus, Miguel Junior Sordi Bortolini, Ernesto Akio Taketomi, and Rafael de Oliveira Resende. 2024. "Distinct Adverse Reactions to mRNA, Inactivated Virus, and Adenovirus Vector COVID-19 Vaccines: Insights from a Cohort Study on Atopic and Non-Atopic Subjects in Brazil" Vaccines 12, no. 4: 408. https://doi.org/10.3390/vaccines12040408
APA StyleOliveira, L. A. R., Correa, A. S., de Jesus, T. A., Bortolini, M. J. S., Taketomi, E. A., & Resende, R. d. O. (2024). Distinct Adverse Reactions to mRNA, Inactivated Virus, and Adenovirus Vector COVID-19 Vaccines: Insights from a Cohort Study on Atopic and Non-Atopic Subjects in Brazil. Vaccines, 12(4), 408. https://doi.org/10.3390/vaccines12040408