

Association between Vitamin D Deficiency and Serologic Response to Hepatitis B Virus Vaccination among Heavy Industry Workers

Abstract
1. Introduction
2. Methods
2.1. Study Site and HBV Vaccination Policy
2.2. Study Eligibility Criteria
2.3. Study Design, Definition, and Outcomes
2.4. Statistical Analysis
2.5. Institutional Review Board Statement
3. Results
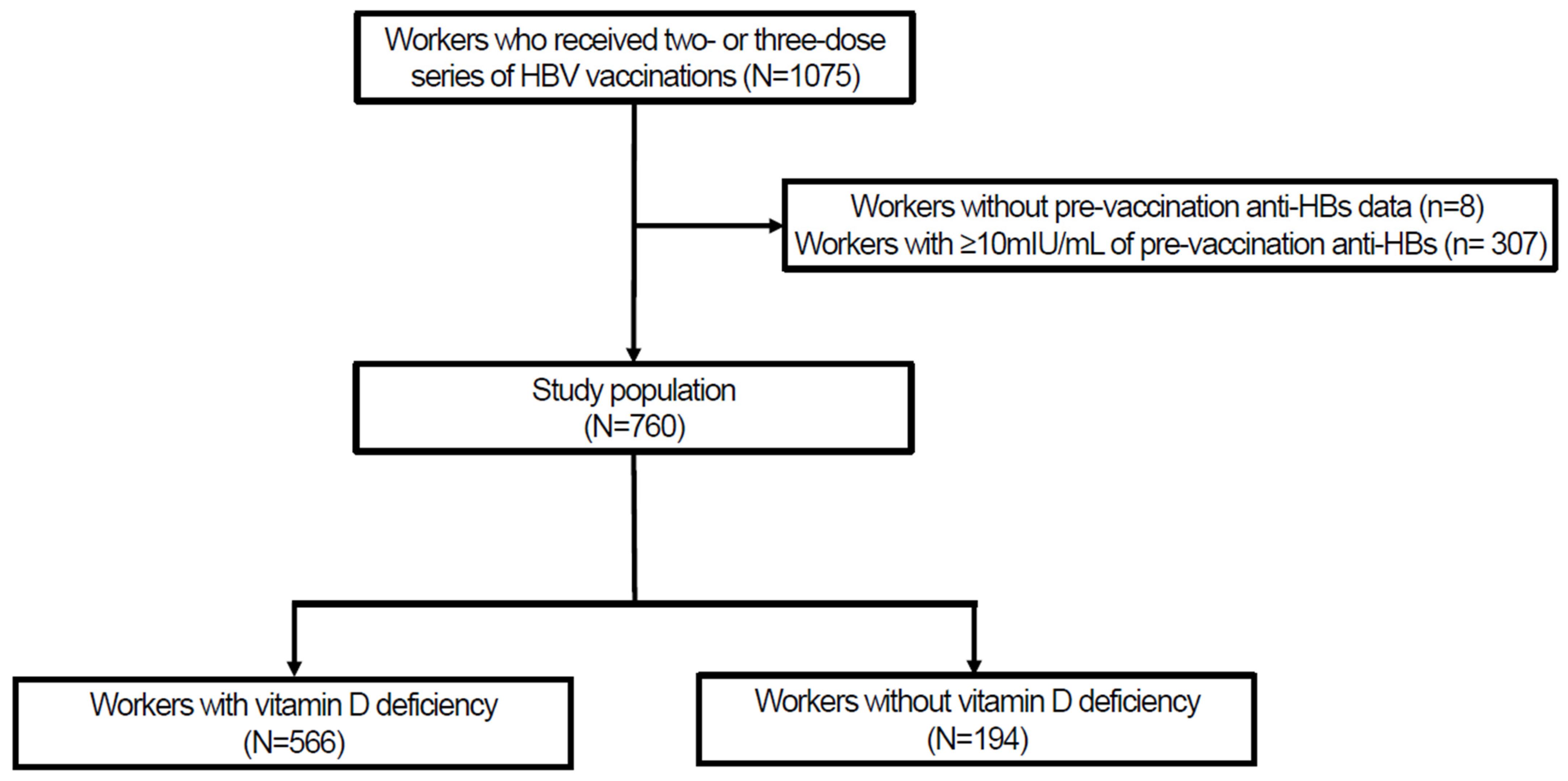
3.1. Study Population
3.2. Immune Response after HBV Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nguyen, M.H.; Wong, G.; Gane, E.; Kao, J.-H.; Dusheiko, G. Hepatitis B Virus: Advances in Prevention, Diagnosis, and Therapy. Clin. Microbiol. Rev. 2020, 33, e00046-19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Hepatitis B. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b# (accessed on 9 June 2024).
- Körber, N.; Pohl, L.; Weinberger, B.; Grubeck-Loebenstein, B.; Wawer, A.; Knolle, P.A.; Roggendorf, H.; Protzer, U.; Bauer, T. Hepatitis B Vaccine Non-Responders Show Higher Frequencies of CD24highCD38high Regulatory B Cells and Lower Levels of IL-10 Expression Compared to Responders. Front. Immunol. 2021, 12, 713351. [Google Scholar] [CrossRef] [PubMed]
- Di Lello, F.A.; Martínez, A.P.; Flichman, D.M. Insights into induction of the immune response by the hepatitis B vaccine. World J. Gastroenterol. 2022, 28, 4249–4262. [Google Scholar] [CrossRef]
- Kim, D.Y. History and future of hepatitis B virus control in South Korea. Clin. Mol. Hepatol. 2021, 27, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Korean Infectious Disease Prevention and Control Act, Hepatitis B. Available online: https://www.law.go.kr/%EB%B2%95%EB%A0%B9/%EA%B0%90%EC%97%BC%EB%B3%91%EC%9D%98%EC%98%88%EB%B0%A9%EB%B0%8F%EA%B4%80%EB%A6%AC%EC%97%90%EA%B4%80%ED%95%9C%EB%B2%95%EB%A5%A0 (accessed on 9 June 2024).
- The Korean Society of Infectious Diseases. Vaccinations for Adults, 3rd ed.; Koonja Publishing Inc.: Paju, Republic of Korea, 2019; pp. 361–372. [Google Scholar]
- Aranow, C. Vitamin D and the immune system. J. Investig. Med. 2011, 59, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Ghaseminejad-Raeini, A.; Ghaderi, A.; Sharafi, A.; Nematollahi-Sani, B.; Moossavi, M.; Derakhshani, A.; Sarab, G.A. Immunomodulatory actions of vitamin D in various immune-related disorders: A comprehensive review. Front. Immunol. 2023, 14, 950465. [Google Scholar] [CrossRef]
- Youssry, S.; Shalaby, T.; Maher, A.-S.; Ghoneim, H. Association of hepatitis B vaccine response to vitamin D supplementation and ultraviolet B (UVB) exposure during different time intervals in experimental animals. Immunol. Res. 2022, 70, 537–545. [Google Scholar] [CrossRef]
- Enioutina, E.Y.; Bareyan, D.; Daynes, R.A. TLR ligands that stimulate the metabolism of vitamin D3 in activated murine dendritic cells can function as effective mucosal adjuvants to subcutaneously administered vaccines. Vaccine 2008, 26, 601–613. [Google Scholar] [CrossRef]
- Zitt, E.; Sprenger-Mähr, H.; Knoll, F.; Neyer, U.; Lhotta, K. Vitamin D deficiency is associated with poor response to active hepatitis B immunisation in patients with chronic kidney disease. Vaccine 2012, 30, 931–935. [Google Scholar] [CrossRef]
- Dabrowska-Leonik, N.; Sawicka-Powierza, J.; Bernatowska, E.; Pac, M.; Bernat-Sitarz, K.; Heropolitanska-Pliszka, E.; Pietrucha, B.; WolskaKusnierz, B.; Lewandowicz-Uszynska, A.; Mikoluc, B. Lack of relationship between 25-hydoxyvitamin D concentration and a titer of antibodies to hepatitis B surface antigen in children under 12 years of age. PLoS ONE 2022, 17, e0277473. [Google Scholar] [CrossRef]
- Kashi, D.S.; Oliver, S.J.; Wentz, L.M.; Roberts, R.; Carswell, A.T.; Tang, J.C.Y.; Jackson, S.; Izard, R.M.; Allan, D.; Rhodes, L.E.; et al. Vitamin D and the hepatitis B vaccine response: A prospective cohort study and a randomized, placebo-controlled oral vitamin D3 and simulated sunlight supplementation trial in healthy adults. Eur. J. Nutr. 2021, 60, 475–491. [Google Scholar] [CrossRef]
- Hafner-Giessauf, H.; Horn, S.; Schwantzer, G.; Sprenger-Mähr, H.; Lhotta, K.; Rosenkranz, A.R.; Zitt, E. Cholecalciferol supplementation to improve the hepatitis B vaccination response in hemodialysis patients: A first randomized open label pilot study (DeVitaHep). Vaccine 2021, 39, 7562–7568. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef]
- Park, J.-H.; Hong, I.Y.; Chung, J.W.; Choi, H.S. Vitamin D status in South Korean population: Seven-year trend from the KNHANES. Medicine 2018, 97, e11032. [Google Scholar] [CrossRef] [PubMed]
- Elecsys Anti-HBs II. Available online: https://assets.roche.com/f/173850/x/0c123ae9f7/anti-hbsii-08498598190-en-can.pdf (accessed on 9 June 2024).
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Sadarangani, S.P.; Whitaker, J.A.; Poland, G.A. “Let there be light”: The role of vitamin D in the immune response to vaccines. Expert. Rev. Vaccines 2015, 14, 1427–1440. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, A.P.; Dragunsky, E.M.; Chumakov, K.M. 1,25-Dihydroxyvitamin D3 Enhances Systemic and Mucosal Immune Responses to Inactivated Poliovirus Vaccine in Mice. J. Infect. Dis. 2006, 193, 598–600. [Google Scholar] [CrossRef]
- Surman, S.L.; Penkert, R.R.; Jones, B.G.; Sealy, R.E.; Hurwitz, J.L. Vitamin Supplementation at the Time of Immunization with a Cold-Adapted Influenza Virus Vaccine Corrects Poor Mucosal Antibody Responses in Mice Deficient for Vitamins A and D. Clin. Vaccine Immunol. 2016, 23, 219–227. [Google Scholar] [CrossRef]
- Vaghari-Tabari, M.; Mohammadzadeh, I.; Qujeq, D.; Majidinia, M.; Alemi, F.; Younesi, S.; Mahmoodpoor, A.; Maleki, M.; Yousefi, B.; Asemi, Z. Vitamin D in respiratory viral infections: A key immune modulator? Crit. Rev. Food Sci. Nutr. 2023, 63, 2231–2246. [Google Scholar] [CrossRef]
- Goncalves-Mendes, N.; Talvas, J.; Dualé, C.; Guttmann, A.; Corbin, V.; Marceau, G.; Sapin, V.; Brachet, P.; Evrard, B.; Laurichesse, H.; et al. Impact of Vitamin D Supplementation on Influenza Vaccine Response and Immune Functions in Deficient Elderly Persons: A Randomized Placebo-Controlled Trial. Front. Immunol. 2019, 10, 65. [Google Scholar] [CrossRef]
- Cesur, F.; Atasever, Z.; Özoran, Y. Impact of vitamin D3 supplementation on COVID-19 vaccine response and immunoglobulin G antibodies in deficient women: A randomized controlled trial. Vaccine 2023, 41, 2860–2867. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, M.E.; Talbot, H.K.; Zhu, Y.; Griffin, M.R.; Spencer, S.; Shay, D.K.; Coleman, L.A. Vitamin D is not associated with serologic response to influenza vaccine in adults over 50 years old. Vaccine 2013, 31, 2057–2061. [Google Scholar] [CrossRef] [PubMed]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Papadopoli, R.; De Sarro, C.; Torti, C.; Pileggi, C.; Pavia, M. Is There Any Opportunity to Provide an HBV Vaccine Booster Dose before Anti-Hbs Titer Vanishes? Vaccines 2020, 8, 227. [Google Scholar] [CrossRef] [PubMed]
- Gara, N.; Abdalla, A.; Rivera, E.; Zhao, X.; Werner, J.M.; Liang, T.J.; Hoofnagle, J.H.; Rehermann, B.; Ghany, M.G. Durability of Antibody Response Against Hepatitis B Virus in Healthcare Workers Vaccinated as Adults. Clin. Infect. Dis. 2014, 60, 505–513. [Google Scholar] [CrossRef] [PubMed]
- McMahon, B.J.; Dentinger, C.M.; Bruden, D.; Zanis, C.; Peters, H.; Hurlburt, D.; Bulkow, L.; Fiore, A.E.; Bell, B.P.; Hennessy, T.W. Antibody Levels and Protection after Hepatitis B Vaccine: Results of a 22-Year Follow-Up Study and Response to a Booster Dose. J. Infect. Dis. 2009, 200, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Morris, J.; Bressler, S.; Thompson, G.; Lecy, D.; Rudolph, K.; Bulkow, L.; Hennessy, T.; et al. Protection and antibody levels 35 years after primary series with hepatitis B vaccine and response to a booster dose. Hepatology 2022, 76, 1180–1189. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.X.; Boland, G.J.; van Hattum, J.; de Gast, G.C. Long-term persistence of T cell memory to HBsAg after hepatitis B vaccination. World J. Gastroenterol. 2004, 10, 260–263. [Google Scholar] [CrossRef]
- Awad, G.; Roch, T.; Stervbo, U.; Kaliszczyk, S.; Stittrich, A.; Hörstrup, J.; Cinkilic, O.; Appel, H.; Natrus, L.; Gayova, L.; et al. Robust hepatitis B vaccine-reactive T cell responses in failed humoral immunity. Mol. Ther. Methods Clin. Dev. 2021, 21, 288–298. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Unadjusted | After PS Matching (1:2) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall (760) | Without Vit. D Deficiency (194) | With Vit. D Deficiency (566) | p-Value | ASMD | Without Vit. D Deficiency (194) | With Vit. D Deficiency (388) | p-Value | ASMD | |
| Serum 25-OH Vitamin D (ng/mL) | 16.79 ± 6.62, 15.97 (12.35–20.16) | 25.30 ± 5.75, 24.29 (22.39–27.40) | 13.87 ± 3.76, 14.26 (11.29–16.99) | <0.001 | 2.350 | 25.30 ± 5.75, 23.24 (21.65–27.01) | 13.99 ± 3.77, 14.47 (11.29–17.17) | <0.001 | 2.323 |
| Age (years) | 29.74 ± 4.40, 29 (26–33) | 30.60 ± 4.39, 30 (27–34) | 29.44 ± 4.37, 29 (26–33) | 0.002 | 0.265 | 30.60 ± 4.39, 30 (27–34) | 30.33 ± 4.18, 30 (27–34) | 0.449 | 0.063 |
| Birth year 1995 or later | 24 (3.2) | 5 (2.6) | 19 (3.4) | 0.592 | 0.046 | 5 (2.6) | 9 (2.3) | >0.999 | 0.017 |
| Sex (male) | 687 (90.4) | 178 (91.8) | 509 (89.9) | 0.572 | 0.063 | 178 (91.8) | 348 (89.7) | 0.426 | 0.070 |
| Anti-HBs titer prior to vaccination (mIU/mL) | 3.44 ± 2.18, 2 (2–4.49) | 3.45 ± 2.24, 2 (2–4.86) | 3.43 ± 2.16, 2 (2–4.36) | 0.929 | 0.007 | 3.45 ± 2.24, 2 (2–4.86) | 3.50 ± 2.22, 2 (2–4.51) | 0.330 | 0.021 |
| Received two doses of the HBV vaccination | 168 (22.1) | 44 (22.7) | 124 (21.9) | 0.841 | 0.019 | 44 (22.7) | 83 (21.4) | 0.723 | 0.031 |
| Timing of selected Anti-HBs measurement | 0.053 | 0.202 | 0.940 | 0.032 | |||||
| The following year after vaccination | 476 (62.6) | 134 (69.1) | 342 (60.4) | 134 (69.1) | 263 (67.8) | ||||
| Two years after vaccination | 271 (35.7) | 59 (30.4) | 212 (37.5) | 59 (30.4) | 122 (31.4) | ||||
| Three years after vaccination | 13 (1.7) | 1 (0.5) | 12 (2.1) | 1 (0.5) | 3 (0.8) | ||||
| Body mass index (kg/m2) | 24.59 ± 3.55, 24.21 (22.13–26.78) | 25.01 ± 3.60, 24.29 (22.39–27.40) | 24.45 ± 3.51, 24.16 (21.93–26.59) | 0.060 | 0.156 | 25.01 ± 3.60, 24.29 (22.39–27.40) | 24.48 ± 3.54, 24.48 (22.35–26.88) | 0.747 | 0.049 |
| Current smoking | 267 (35.1) | 58 (29.9) | 209 (36.9) | 0.077 | 0.149 | 58 (29.9) | 120 (30.9) | 0.799 | 0.022 |
| Hemoglobin A1c (%) | 5.34 ± 0.54, 5.3 (5.1–5.5) | 5.40 ± 0.68, 5.3 (5.1–5.5) | 5.32 ± 0.48, 5.3 (5.1–5.5) | 0.073 | 0.136 | 5.40 ± 0.68, 5.3 (5.1–5.5) | 5.36 ± 0.55, 5.3 (5.2–5.5) | 0.064 | |
| Presence of diabetes mellitus | 0.179 | 0.121 | 0.687 | 0.032 | |||||
| Normal | 683 (89.9) | 168 (86.6) | 515 (91.0) | 168 (86.6) | 343 (88.4) | ||||
| Prediabetes | 66 (8.7) | 23 (11.9) | 43 (7.6) | 23 (11.9) | 38 (9.5) | ||||
| Diabetes mellitus | 11 (1.4) | 3 (1.5) | 8 (1.4) | 3 (1.5) | 8 (1.9) | ||||
| Metabolic syndrome | 62 (8.2) | 20 (10.3) | 42 (7.4) | 0.205 | 0.102 | 20 (10.3) | 54 (9.3) | 0.521 | 0.053 |
| Chronic kidney disease ≥ stage 3 | 0 (0.0) | 0 (0.0) | 0 (0.0) | >0.999 | N/A | 0 (0.0) | 0 (0.0) | >0.999 | N/A |
| Non-Matched | PS-Matched | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Overall (760) | Without Vit. D Deficiency (194) | With Vit. D Deficiency (566) | OR (95% CI) | p-Value | Without Vit. D Deficiency (194) | With Vit. D Deficiency (388) | OR (95% CI) | p-Value | |
| Primary outcome | |||||||||
| Non-responder | 87 (11.4) | 11 (5.7) | 76 (13.4) | 2.58 (1.34–4.97) | 0.005 | 11 (5.7) | 55 (14.2) | 2.74 (1.40–5.38) | 0.003 |
| Secondary outcome | |||||||||
| Anti-HBs response (1og transformation, mIU/mL) | 2.19 ± 0.84, 2.41 (1.70–3.00) | 2.25 ± 0.75, 2.43 (1.70–3.00) | 2.18 ± 0.87, 2.41 (1.70–3.00) | N/A | 0.684 | 2.25 ± 0.75, 2.43 (1.70–3.00) | 2.15 ± 0.88, 2.39 (1.66–3.00) | N/A | 0.494 |
| Immune Response | Univariate | Binary Logistic Model | ||||
|---|---|---|---|---|---|---|
| Non-Responder | Responder | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (per year) | 30.49 ± 4.58, 31 (27–34) | 29.64 ± 4.37, 29 (26–33) | 1.05 (0.99–1.10) | 0.090 * | 1.06 (1.01–1.13) | 0.038 |
| Birth year ≥ 1995 | 5 (20.8) | 19 (79.2) | 2.10 (0.76–5.77) | 0.151 * | 1.59 (0.48–1.13) | 0.450 |
| Sex (male) | 83 (12.1) | 604 (87.9) | 2.37 (0.84–6.67) | 0.102 * | 1.83 (0.62–5.47) | 0.276 |
| Anti-HBs titer prior to vaccination (per 1 mIU/mL) | 2.21 ± 0.73, 2 (2–2) | 3.60 ± 2.26, 2 (2–4.93) | 0.49 (0.35–0.67) | <0.001 * | 0.47 (0.33–0.65) | <0.001 |
| Received two doses of the HBV vaccination | 37 (22.0) | 131 (78.0) | 3.06 (1.92–4.88) | <0.001 * | 3.22 (1.93–5.37) | <0.001 |
| Timing of Anti-HBs measurement | 0.314 | |||||
| The following year after vaccination | 49 (10.3) | 427 (89.7) | Reference | |||
| Two years after vaccination | 38 (14.0) | 233 (86.0) | 1.42 (0.90–2.24) | |||
| Three years after vaccination | 0 (0.0) | 13 (100.0) | N/A | |||
| Vitamin D deficiency | 76 (13.4) | 490 (86.6) | 2.58 (1.34–4.97) | 0.005 * | 3.20 (1.60–6.38) | 0.001 |
| Body mass index (per 1 kg/m2) | 24.81 ± 3.46, 24.22 (22.25–27.15) | 24.56 ± 3.56, 24.20 (22.10–26.61) | 1.02 (0.96–1.08) | 0.550 | ||
| Current smoking | 41 (15.4) | 226 (84.6) | 1.76 (1.12–2.77) | 0.014 * | 1.83 (1.12–2.99) | 0.015 |
| Hemoglobin A1c (per 1%) | 5.39 ± 0.58, 5.3 (5.2–5.5) | 5.33 ± 0.53, 5.3 (5.1–5.5) | 1.16 (0.83–1.62) | 0.373 | ||
| Presence of diabetes mellitus | 0.155 | |||||
| Normal | 73 (10.7) | 610 (89.3) | Reference | |||
| Prediabetes | 12 (18.2) | 54 (81.8) | 1.86 (0.95–3.63) | |||
| Diabetes mellitus | 2 (18.2) | 9 (81.8) | 1.86 (0.39–8.76) | |||
| Metabolic syndrome | 11 (17.7) | 51 (82.3) | 1.77 (0.88–3.53) | 0.108 * | 2.07 (0.95–4.53) | 0.068 |
| Immune Response | Univariate | Binary Logistic Model | ||||
|---|---|---|---|---|---|---|
| Non-Responder (50) | Responder (542) | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age (per year) | 30.88 ± 4.53 31.5 (28–35) | 29.66 ± 4.27, 29 (26–33) | 1.07 (1.00–1.14) | 0.057 * | 1.11 (1.03–1.20) | 0.008 |
| Birth year ≥ 1995 | 3 (27.3) | 8 (72.7) | 4.26 (1.09–16.6) | 0.037 * | 5.02 (1.05–24.12) | 0.044 |
| Sex (male) | 48 (9.0) | 483 (91.0) | 2.92 (0.70–12.38) | 0.143 * | 2.83 (0.63–12.82) | 0.176 |
| Anti-HBs titer prior to vaccination (per 1 mIU/mL) | 2.25 ± 0.79 2 (2–2) | 3.62 ± 2.27 2(2–4.94) | 0.51 (0.34–0.75) | 0.001 * | 0.48 (0.31–0.73) | 0.001 |
| Timing of Anti-HBs measurement | 0.447 | |||||
| The following year after vaccination | 28 (7.5) | 346 (92.5) | Reference | |||
| Two years after vaccination | 22 (10.6) | 186 (89.4) | 1.46 (0.81–2.63) | |||
| Three years after vaccination | 0 (0.0) | 10 (100.0) | N/A | |||
| Vitamin D deficiency | 45 (10.2) | 397 (89.8) | 3.29 (1.28–8.44) | 0.013 * | 3.90 (1.46–10.41) | 0.007 |
| Body mass index (per 1 kg/m2) | 24.96 ± 3.49, 24.01 (22.27–27.14) | 24.61 ± 3.61, 24.18 (22.16–26.60) | 1.03 (0.95–1.11) | 0.512 | ||
| Current smoking | 30 (14.0) | 185 (86.0) | 2.90 (1.60–5.24) | <0.001 * | 3.01 (1.61–5.62) | 0.001 |
| Hemoglobin A1c (per 1%) | 5.38 ± 0.70, 5.4 (5.1–5.5) | 5.34 ± 0.57 5.3 (5.1–5.5) | 1.10 (0.73–1.67) | 0.636 | ||
| Presence of diabetes mellitus | 0.814 | |||||
| Normal | 44 (8.2) | 492 (91.8) | Ref | |||
| Prediabetes | 5 (10.6) | 42 (89.4) | 1.33 (0.50–3.54) | |||
| Diabetes mellitus | 1 (11.1) | 9 (88.9) | 1.40 (0.17–11.43) | |||
| Metabolic syndrome | 6 (11.8) | 45 (88.2) | 1.51 (0.61–3.73) | 0.376 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-H.; Chae, C.-H. Association between Vitamin D Deficiency and Serologic Response to Hepatitis B Virus Vaccination among Heavy Industry Workers. Vaccines 2024, 12, 723. https://doi.org/10.3390/vaccines12070723
Kim S-H, Chae C-H. Association between Vitamin D Deficiency and Serologic Response to Hepatitis B Virus Vaccination among Heavy Industry Workers. Vaccines. 2024; 12(7):723. https://doi.org/10.3390/vaccines12070723
Chicago/Turabian StyleKim, Si-Ho, and Chang-Ho Chae. 2024. "Association between Vitamin D Deficiency and Serologic Response to Hepatitis B Virus Vaccination among Heavy Industry Workers" Vaccines 12, no. 7: 723. https://doi.org/10.3390/vaccines12070723
APA StyleKim, S.-H., & Chae, C.-H. (2024). Association between Vitamin D Deficiency and Serologic Response to Hepatitis B Virus Vaccination among Heavy Industry Workers. Vaccines, 12(7), 723. https://doi.org/10.3390/vaccines12070723