

Comparative Efficacy of Immune Checkpoint Inhibitors and Therapeutic Vaccines in Solid Tumors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
- -
- Study Design:
- Only randomized controlled trials (RCTs).
- Single arm and multi-arm RCTs comparing checkpoint inhibitors or vaccines against a control (placebo, standard of care, or another active treatment).
- -
- Population:
- Adult males and females (≥18 years) diagnosed with solid tumors (e.g., melanoma, non-small cell lung cancer, renal cell carcinoma, and breast cancer).
- -
- Interventions:
- Checkpoint inhibitors: Any immune checkpoint inhibitor targeting PD-1, PD-L1, CTLA-4, or other immune checkpoint pathways (e.g., pembrolizumab, nivolumab, ipilimumab, atezolizumab, or durvalumab).
- Vaccines: Any therapeutic cancer vaccine (e.g., peptide vaccines, dendritic cell vaccines, or mRNA vaccines) used as monotherapy or in combination with other treatments.
- Studies comparing checkpoint inhibitors versus vaccines, or against a control.
- -
- Comparators:
- Placebo, standard of care, or another active treatment (e.g., chemotherapy or targeted therapy).
- -
- Outcomes:
- Primary outcome: overall survival (OS), defined as the length of time from randomization (or start of treatment) until death from any cause. OS was chosen because it is less susceptible to measurement bias and variability in assessment criteria across trials. Studies must report OS or provide sufficient data to calculate OS (e.g., Kaplan–Meier curves, hazard ratios, or survival probabilities).
- -
- Time Frame:
- RCTs published between 1 January 2010 and 31 December 2024.
- Ongoing trials with preliminary results available by the end of 2025.
- -
- Language and Publication Status:
- Only studies published in English.
- Both peer-reviewed published studies and preprints with available full text data.
- -
- Sample Size:
- No restriction on sample size, but studies with fewer than 20 participants will be critically evaluated for risk of bias.
2.2.2. Exclusion Criteria
- -
- Non-randomized studies (e.g., observational studies, case reports, and retrospective analyses).
- -
- Studies involving pediatric populations (<18 years).
- -
- Studies focusing on hematologic malignancies or non-solid tumors.
- -
- Studies involving combination therapies where the effect of checkpoint inhibitors or vaccines cannot be isolated.
- -
- Studies without a control group or those comparing non-immunotherapy treatments.
- -
- Abstracts, conference proceedings, and studies without full-text availability unless sufficient data are provided.
- -
- Duplicate publications or secondary analyses of already included trials.
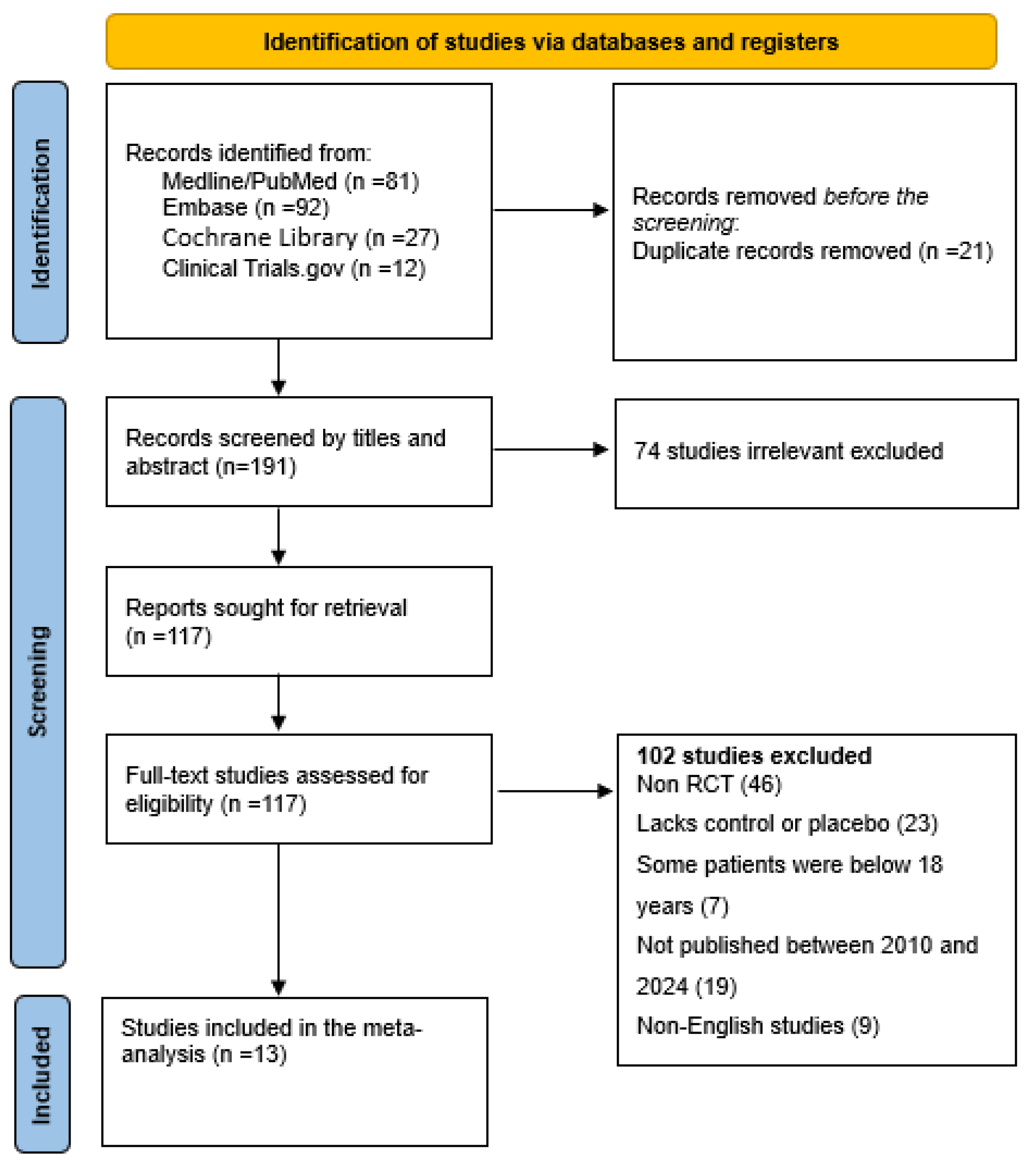
2.3. Search Strategy
2.4. Data Extraction
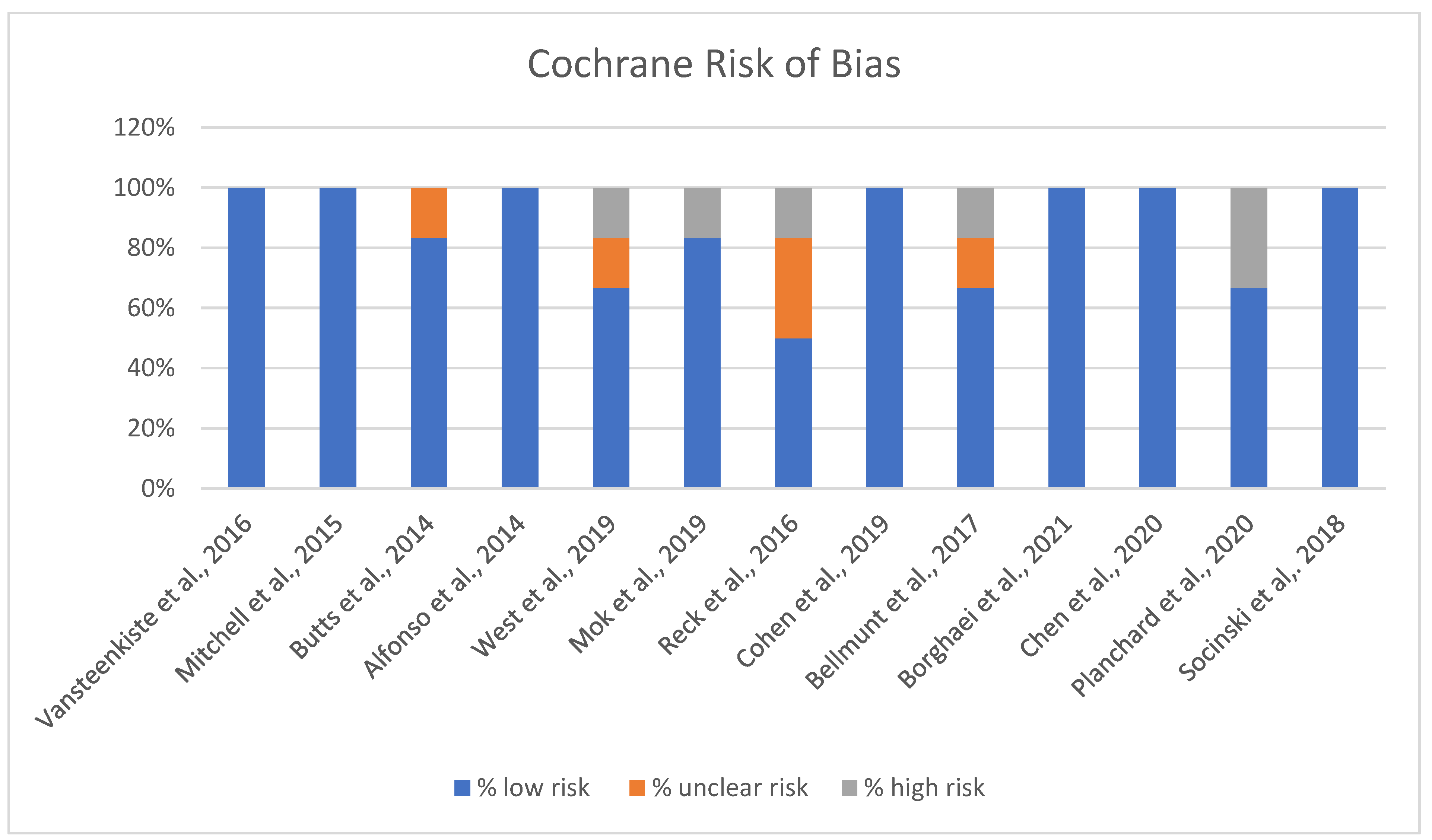
2.5. RoB Assessment
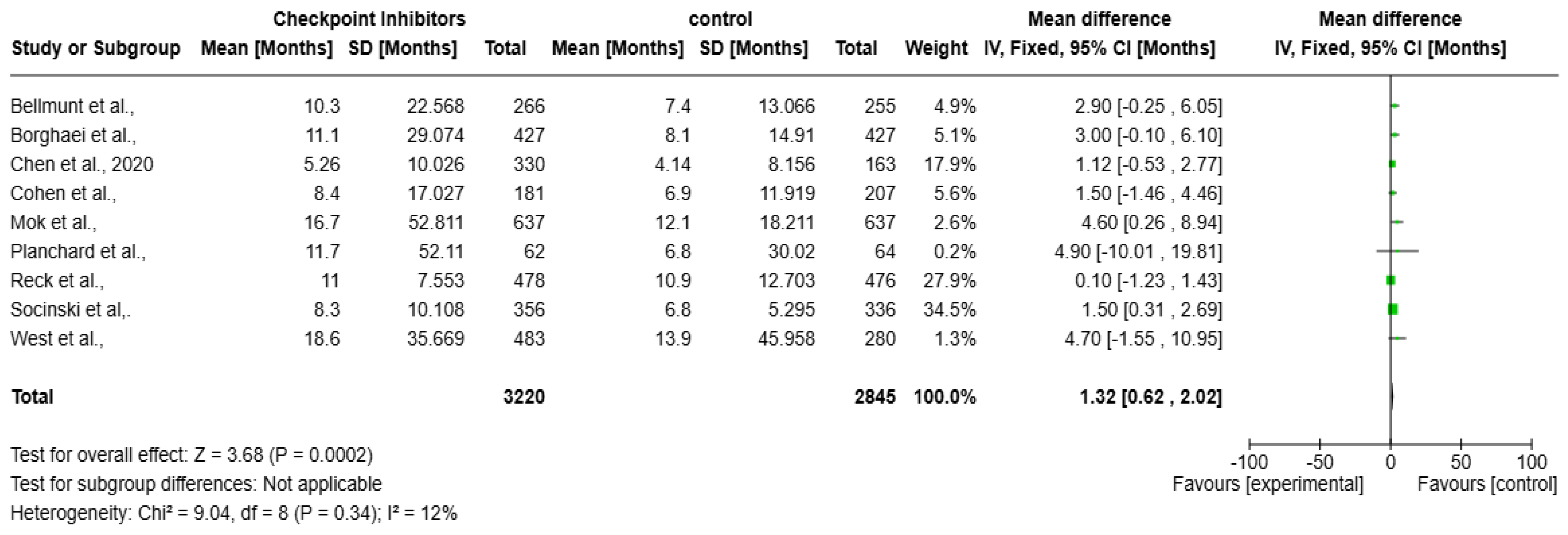
2.6. Statistical Analysis
3. Results
4. Discussion
5. Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ICIs | immune checkpoint inhibitors |
| OS | overall survival |
| RCTs | randomized controlled trials |
| PD-1 | programmed cell death protein 1 |
| CTLA-4 | cytotoxic T-lymphocyte-associated protein 4 |
| MAGE-A | melanoma antigen family A |
References
- Tadic, S.; Martínez, A. Nucleic acid cancer vaccines targeting tumor related angiogenesis. Could mRNA vaccines constitute a game changer? Front. Immunol. 2024, 15, 1433185. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarek, M.; Poznańska, J.; Fechner, F.; Michalska, N.; Paszkowska, S.; Napierała, A.; Mackiewicz, A. Cancer vaccine therapeutics: Limitations and effectiveness—A literature review. Cells 2023, 12, 2159. [Google Scholar] [CrossRef]
- Drew, L. How does a cancer vaccine work? Nature 2024, 627, S34–S35. [Google Scholar] [CrossRef] [PubMed]
- Grimmett, E.; Al-Share, B.; Alkassab, M.B.; Zhou, R.W.; Desai, A.; Rahim, M.M.; Woldie, I. Cancer vaccines: Past, present and future; a review article. Discover Oncology. Discov. Oncol. 2022, 13, 31. [Google Scholar] [CrossRef]
- Waldman, A.D.; Fritz, J.M.; Lenardo, M.J. A guide to cancer immunotherapy: From T cell basic science to clinical practice. Nat. Rev. Immunol. 2020, 20, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Cui, L.; Zhao, X.; Bai, H.; Cai, S.; Wang, G.; Zhao, Z.; Zhao, J.; Chen, S.; Song, J.; et al. Use of immunotherapy with programmed cell death 1 vs. programmed cell death ligand 1 inhibitors in patients with cancer: A systematic review and meta-analysis. JAMA Oncol. 2020, 6, 375–384. [Google Scholar] [CrossRef]
- Sun, Q.; Hong, Z.; Zhang, C.; Wang, L.; Han, Z.; Ma, D. Immune checkpoint therapy for solid tumours: Clinical dilemmas and future trends. Signal Transduct. Target. Ther. 2023, 8, 320. [Google Scholar] [CrossRef]
- Fitzsimmons, T.S.; Singh, N.; Walker, T.D.; Newton, C.; Evans, D.G.; Crosbie, E.J.; Ryan, N.A. Immune checkpoint inhibitors efficacy across solid cancers and the utility of PD-L1 as a biomarker of response: A systematic review and meta-analysis. Front. Med. 2023, 10, 1192762. [Google Scholar] [CrossRef]
- Zhao, J.; Chen, Y.; Ding, Z.Y.; Liu, J.Y. Safety and efficacy of therapeutic cancer vaccines alone or in combination with immune checkpoint inhibitors in cancer treatment. Front. Pharmacol. 2019, 10, 1184. [Google Scholar] [CrossRef]
- Tsao, L.C.; Force, J.; Hartman, Z.C. Mechanisms of therapeutic antitumor monoclonal antibodies. Cancer Res. 2021, 81, 4641–4651. [Google Scholar] [CrossRef]
- Batista-Duharte, A.; Hassouneh, F.; Alvarez-Heredia, P.; Pera, A.; Solana, R. Immune checkpoint inhibitors for vaccine improvements: Current status and new approaches. Pharmaceutics 2022, 14, 1721. [Google Scholar] [CrossRef] [PubMed]
- Vafaei, S.; Zekiy, A.O.; Khanamir, R.A.; Zaman, B.A.; Ghayourvahdat, A.; Azimizonuzi, H.; Zamani, M. Combination therapy with immune checkpoint inhibitors (ICIs); a new frontier. Cancer Cell Int. 2022, 22, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Vansteenkiste, J.F.; Cho, B.C.; Vanakesa, T.; De Pas, T.; Zielinski, M.; Kim, M.S.; Jassem, J.; Yoshimura, M.; Dahabreh, J.; Nakayama, H.; et al. Efficacy of the MAGE-A3 cancer immunotherapeutic as adjuvant therapy in patients with resected MAGE-A3-positive non-small-cell lung cancer (MAGRIT): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016, 17, 822–835. [Google Scholar] [CrossRef]
- Mitchell, P.; Thatcher, N.; Socinski, M.A.; Wasilewska-Tesluk, E.; Horwood, K.; Szczesna, A.; Martín, C.; Ragulin, Y.; Zukin, M.; Helwig, C.; et al. Tecemotide in unresectable stage III non small-cell lung cancer in the phase III START study: Updated overall survival and biomarker analyses. Ann. Oncol. 2015, 26, 1134–1142. [Google Scholar] [CrossRef]
- Butts, C.; Socinski, M.A.; Mitchell, P.L.; Thatcher, N.; Havel, L.; Krzakowski, M.; Nawrocki, S.; Ciuleanu, T.E.; Bosquée, L.; Trigo, J.M.; et al. Tecemotide (L-BLP25) versus placebo after chemoradiotherapy for stage III non-small-cell lung cancer (START): A randomised, double-blind, phase 3 trial. Lancet Oncol. 2014, 15, 59–68. [Google Scholar] [CrossRef]
- Alfonso, S.; Valdés-Zayas, A.; Santiesteban, E.R.; Flores, Y.I.; Areces, F.; Hernández, M.; Viada, C.E.; Mendoza, I.C.; Guerra, P.P.; García, E.; et al. A randomized, multicenter, placebo controlled clinical trial of racotumomab-alum vaccine as switch maintenance therapy in advanced non–small cell lung cancer patients. Clin. Cancer Res. 2014, 20, 3660–3671. [Google Scholar] [CrossRef]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Luft, A.; Szczesna, A.; Havel, L.; Kim, S.W.; Akerley, W.; Pietanza, M.C.; Wu, Y.L.; Zielinski, C.; Thomas, M.; et al. Phase III randomized trial of ipilimumab plus etoposide and platinum versus placebo plus etoposide and platinum in extensive-stage small-cell lung cancer. J. Clin. Oncol. 2016, 34, 3740–3748. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Cohen, E.E.; Soulières, D.; Le Tourneau, C.; Dinis, J.; Licitra, L.; Ahn, M.J.; Soria, A.; Machiels, J.P.; Mach, N.; Mehra, R.; et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): A randomised, open-label, phase 3 study. Lancet 2019, 393, 156–167. [Google Scholar] [CrossRef]
- Bellmunt, J.; De Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.; Burgio, M.A.; de Castro Carpeno, J.; Pluzanski, A.; Arrieta, O.; Frontera, O.A.; Chiari, R.; et al. Five-year outcomes from the randomized, phase III trials checkmate 017 and 057: Nivolumab versus docetaxel in previously treated non–small-cell lung cancer. J. Clin. Oncol. 2021, 39, 723–733. [Google Scholar] [CrossRef]
- Chen, L.T.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; Yeh, K.H.; et al. A phase 3 study of nivolumab in previously treated advanced gastric or gastroesophageal junction cancer (ATTRACTION-2): 2-year update data. Gastric Cancer 2020, 23, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Reinmuth, N.; Orlov, S.; Fischer, J.R.; Sugawara, S.; Mandziuk, S.; Marquez-Medina, D.; Novello, S.; Takeda, Y.; Soo, R.; et al. ARCTIC: Durvalumab with or without tremelimumab as third-line or later treatment of metastatic non-small-cell lung cancer. Ann. Oncol. 2020, 31, 609–618. [Google Scholar] [CrossRef]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez Abreu, D.; Moro-Sibilot, D.; Thomas, C.A.; Barlesi, F.; et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N. Engl. J. Med. 2018, 378, 2288–2301. [Google Scholar] [CrossRef] [PubMed]
- Sanmamed, M.F.; Chen, L. A paradigm shift in cancer immunotherapy: From enhancement to normalization. Cell 2018, 175, 313–326. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Vétizou, M.; Pitt, J.M.; Daillère, R.; Lepage, P.; Waldschmitt, N.; Flament, C.; Rusakiewicz, S.; Routy, B.; Roberti, M.P.; Duong, C.P.; et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 2015, 350, 1079–1084. [Google Scholar] [CrossRef] [PubMed]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Man Lei, Y.; Jabri, B.; Alegre, M.L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti–PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef]
- Chaput, N.; Lepage, P.; Coutzac, C.; Soularue, E.; Le Roux, K.; Monot, C.; Boselli, L.; Routier, E.; Cassard, L.; Collins, M.; et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann. Oncol. 2017, 28, 1368–1379. [Google Scholar] [CrossRef]
- Gulley, J.L.; Borre, M.; Vogelzang, N.J.; Ng, S.; Agarwal, N.; Parker, C.C.; Pook, D.W.; Rathenborg, P.; Flaig, T.W.; Carles, J.; et al. Phase III trial of PROSTVAC in asymptomatic or minimally symptomatic metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2019, 37, 1051–1061. [Google Scholar] [CrossRef] [PubMed]
- Duperret, E.K.; Liu, S.; Paik, M.; Trautz, A.; Stoltz, R.; Liu, X.; Ze, K.; Perales-Puchalt, A.; Reed, C.; Yan, J.; et al. A designer cross-reactive DNA immunotherapeutic vaccine that targets multiple MAGE-A family members simultaneously for cancer therapy. Clin. Cancer Res. 2018, 24, 6015–6027. [Google Scholar] [CrossRef]
- Kruit, W.H.; Suciu, S.; Dreno, B.; Mortier, L.; Robert, C.; Chiarion-Sileni, V.; Maio, M.; Testori, A.; Dorval, T.; Grob, J.J.; et al. Selection of immunostimulant AS15 for active immunization with MAGE-A3 protein: Results of a randomized phase II study of the European Organisation for Research and Treatment of Cancer Melanoma Group in Metastatic Melanoma. J. Clin. Oncol. 2013, 31, 2413–2420. [Google Scholar] [CrossRef]
- Blass, E.; Ott, P.A. Advances in the development of personalized neoantigen-based therapeutic cancer vaccines. Nat. Rev. Clin. Oncol. 2021, 18, 215–229. [Google Scholar] [CrossRef]
- Le, D.T.; Lutz, E.; Uram, J.N.; Sugar, E.A.; Onners, B.; Solt, S.; Zheng, L.; Diaz, L.A., Jr.; Donehower, R.C.; Jaffee, E.M.; et al. Evaluation of ipilimumab in combination with allogeneic pancreatic tumor cells transfected with a GM-CSF gene in previously treated pancreatic cancer. J. Immunother. 2013, 36, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, P.C.; Popa, X.; Martínez, O.; Mendoza, S.; Santiesteban, E.; Crespo, T.; Amador, R.M.; Fleytas, R.; Acosta, S.C.; Otero, Y.; et al. A phase III clinical trial of the epidermal growth factor vaccine CIMAvax-EGF as switch maintenance therapy in advanced non–small cell lung cancer patients. Clin. Cancer Res. 2016, 22, 3782–3790. [Google Scholar] [CrossRef]
- Kantoff, P.W.; Higano, C.S.; Shore, N.D.; Berger, E.R.; Small, E.J.; Penson, D.F.; Redfern, C.H.; Ferrari, A.C.; Dreicer, R.; Sims, R.B.; et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N. Engl. J. Med. 2010, 363, 411–422. [Google Scholar] [CrossRef]
- Cuzzubbo, S.; Mangsbo, S.; Nagarajan, D.; Habra, K.; Pockley, A.G.; McArdle, S.E. Cancer vaccines: Adjuvant potency, importance of age, lifestyle, and treatments. Front. Immunol. 2021, 11, 615240. [Google Scholar] [CrossRef] [PubMed]
- El-Sayes, N.; Vito, A.; Mossman, K. Tumor heterogeneity: A great barrier in the age of cancer immunotherapy. Cancers 2021, 13, 806. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Study Design | Sample Size (Exp/Con) | Age | Cancer Type | Interventions | Comparators | Overall Survival (OS) |
|---|---|---|---|---|---|---|---|
| Therapeutic vaccines: | |||||||
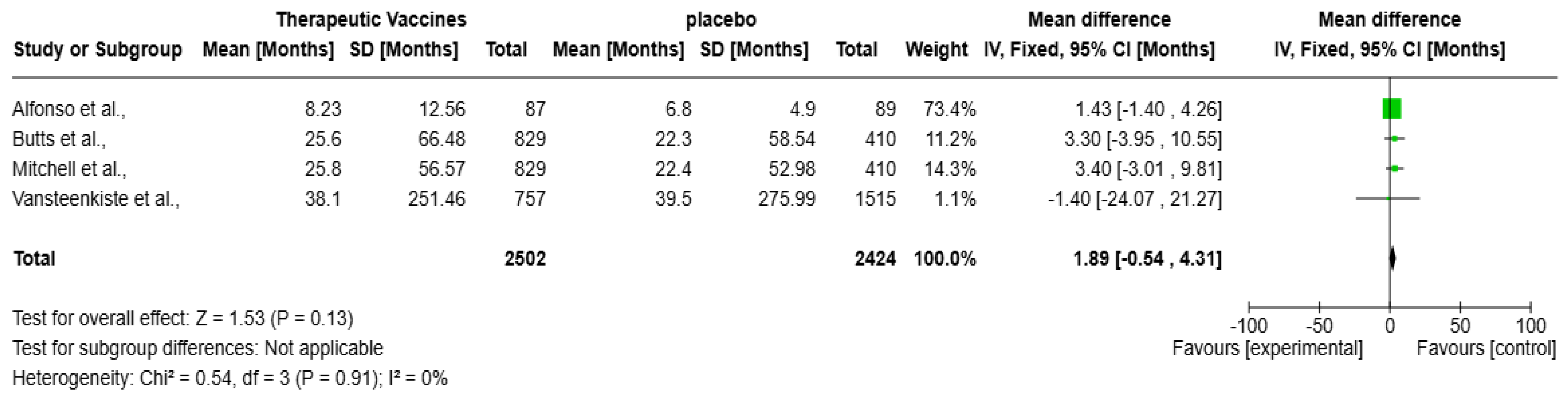
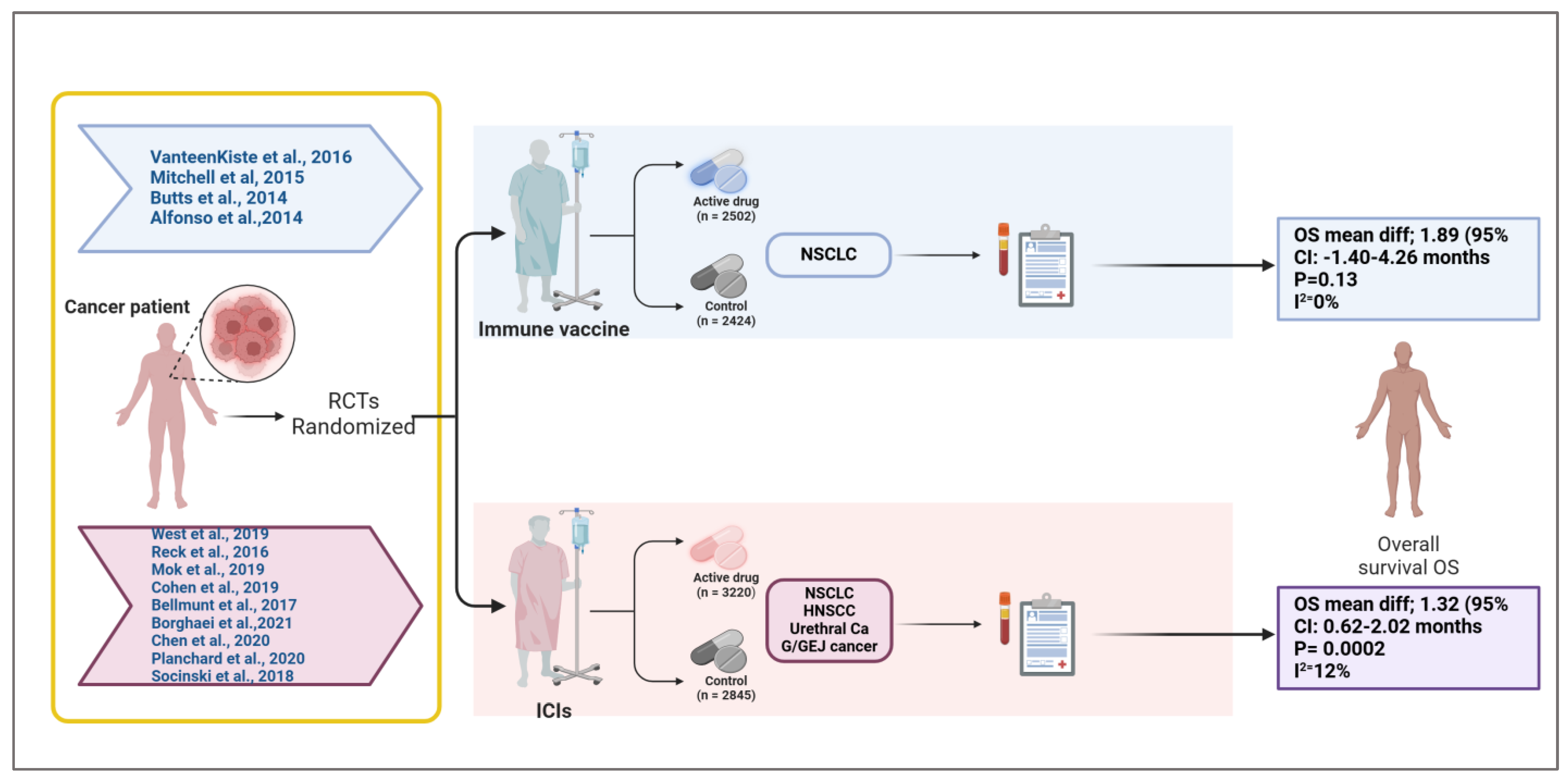
| Vansteenkiste et al., 2016 [13] | Randomized, double blind, placebo controlled trial | 2272 patients (1515 in the MAGE-A3 group, 757 in the placebo group | Patients aged at least 18 years | Stage IB, II, and IIIA non-small-cell lung cancer (NSCLC) with MAGE-A3-positive tumors | -MAGE-A3 immunotherapeutic: 13 intramuscular injections of recMAGE-A3 with AS15 immunostimulant -Placebo: Placebo injections | Placebo group | -MAGE-A3 group: 38.1 months (95% CI 27.9–48.4) -Placebo group: 39.5 months (95% CI 27.9–50.4) |
| Mitchell et al., 2015 [14] | Phase III, randomized controlled trial | 1239 patients (Experimental arm n = 829/Control arm n = 410) | Median Age: 61 years, Age Range: 19–89 years | Unresectable Stage III Non-Small-Cell Lung Cancer (NSCLC) | Tecemotide (806 μg lipopeptide) | Placebo (liposome-forming lipids only) | -Experimental: 25.8 mo (95% CI, (23.1–29.4) -Control: 22.4 mo (95% CI, 19.6–25.5) -Hazard Ratio (HR): 0.889 (95% CI: 0.770–1.027). |
| Butts et al., 2014 [15] | Phase 3, international, randomized, double blind trial | 1239 patients (829 to tecemotide, 410 to placebo) | ≥18 years | Unresectable stage III non-small cell lung cancer | -Tecemotide (806 μg lipopeptide) injections weekly for 8 weeks, then every 6 weeks until disease progression or withdrawal -Cyclophosphamide (300 mg/m2) administered once before tecemotide | Placebo (saline before placebo injections) | -Tecemotide: 25.6 months (95% CI 22.5–29.2) -Placebo: 22.3 months (95% CI 19.6–25.5) -Adjusted HR: 0.88 (95% CI 0.75–1.03), p = 0.123 |
| Alfonso et al., 2014 [16] | Randomized, double blind, placebo controlled phase II/III trial | 176 patients (87 (Racotumomab-Alum)/89 (Placebo) | ≥18 years | Stage IIIb/IV non-small cell lung cancer | Racotumomab-Alum (5 immunizations every 2 weeks, then reimmunizations every 4 weeks) | Placebo | -HR 0.63 (95% CI, 0.46–0.87) Log rank p value = 0.004 -Median OS (mo): Racotumomab-alum 8.23 (95% CI, 5.59–10.87); Placebo 6.80 (95% CI, 5.77–7.83) |
| Checkpoint inhibitors: | |||||||
| West et al., 2019 [17] | Multicenter, randomized, open label, phase 3 study | 763 (483 (Atezolizumab + Chemotherapy), 280 (Chemotherapy)) | 18 years or older | Stage IV non-squamous non-small cell lung cancer | Atezolizumab + Chemotherapy (Carboplatin + Nab-Paclitaxel) | Chemotherapy (Carboplatin + Nab-Paclitaxel) | -Intervention: 18.6 mo (95% CI, 16.0–21.2) -Control: 13.9 mo (95% CI, 12.0–18.7) -Hazard Ratio (HR): 0.79 (95% CI: 0.64–0.98; p = 0.033). |
| Reck et al., 2016 [18] | Phase III randomized controlled trial (RCT), double blind | 954 patients (Experimental arm n = 478/Control arm n = 476) | Median age: 62 years (range: 36–85 years). | Extensive-stage small cell lung cancer (ED-SCLC). | -Ipilimumab: 10 mg/kg every 3 weeks for four doses (starting from cycle 3). -Etoposide: 100 mg/m2 IV on days 1–3 of each cycle. -Platinum: Cisplatin (75 mg/m2) or carboplatin (AUC 5) on day 1 of each cycle. | -Placebo: Administered in the same schedule as ipilimumab, in combination with etoposide and platinum. | -Hazard Ratio (HR): 0.94 (95% CI: 0.81–1.09; p = 0.3775). -Median OS: 11.0 months (95% CI: 10.45–11.33) for ipilimumab arm vs. 10.9 months (95% CI: 10.02–11.50) for placebo arm. |
| Mok et al., 2019 [19] | Randomized, open label, controlled, phase 3 trial | 1274 patients (Experimental arm n = 637/Control arm n = 637) | Adults (≥18 years) | Locally advanced or metastatic non-small cell lung cancer (NSCLC) with PD-L1 expression (TPS ≥ 1%) | Pembrolizumab (PD-1 immune checkpoint inhibitor) | Chemotherapy (platinum-based) | -Pembrolizumab: Median OS = 16.7 months (95% CI, 13.9–19.7) -Chemotherapy: Median OS = 12.1 months (95% CI, 11.3–13.3) -Hazard Ratio (HR): 0.81 (95% CI, 0.71–0.93; p = 0.0018) |
| Cohen et al., 2019 [20] | Randomized, open label, phase 3 study | 388 patients (181 in pembrolizumab group, 207 in standard of care group) | adults ≥ 18 years implied | Recurrent or metastatic head and neck squamous cell carcinoma (HNSCC) | Pembrolizumab 200 mg every 3 weeks intravenously | Standard of care (methotrexate, docetaxel, or cetuximab intravenously) | Pembrolizumab: Median OS = 8.4 months (95% CI, 6.4–9.4) -Standard of Care: Median OS = 6.9 months (95% CI, 5.9–8.0) -Hazard Ratio (HR): 0.80 (95% CI, 0.65–0.98; nominal p = 0.0161) |
| Bellmunt et al., 2017 [21] | Open label, international, phase 3 trial | 521 patients (Experimental arm n = 266/Control arm n = 255) | Adults (≥18 years) | Advanced urothelial cancer (recurrent or progressed after platinum based chemotherapy) | Pembrolizumab (200 mg every 3 weeks) | Chemotherapy (investigator’s choice of paclitaxel, docetaxel, or vinflunine) | -Total Population: -Pembrolizumab: Median OS = 10.3 months (95% CI, 8.0–11.8) -Chemotherapy: Median OS = 7.4 months (95% CI, 6.1–8.3) -Hazard Ratio (HR): 0.73 (95% CI, 0.59–0.91; p = 0.002) -PD-L1 CPS ≥ 10% Subgroup: -Pembrolizumab: Median OS = 8.0 months (95% CI, 5.0–12.3) -Chemotherapy: Median OS = 5.2 months (95% CI, 4.0–7.4) -Hazard Ratio (HR): 0.57 (95% CI, 0.37–0.88; p = 0.005) |
| Borghaei et al., 2021 [22] | Randomized, open label, phase III trials | 854 patients (427 in nivolumab group, 427 in docetaxel group) | Median age of 61.0 years (range: 37–85) in nivolumab group, 64.0 years (range: 21–85) in docetaxel group | Advanced non- small cell lung cancer (NSCLC), including both squamous and nonsquamous histologies | Nivolumab (3 mg/kg once every 2 weeks) | Docetaxel (75 mg/m2 once every 3 weeks) | -Nivolumab Median OS = 11.1 months (95% CI, 9.2–13.1) -Docetaxel: Median OS = 8.1 months (95% CI, 7.2–9.2) -Hazard Ratio (HR): 0.68 (95% CI, 0.59 to 0.78) |
| Chen et al., 2020 [23] | Randomized, double blind, placebo controlled, phase 3 trial | 493 patients (330 in nivolumab group, 163 in placebo group) | Median age of 62 years (interquartile range [IQR]: 54–69) in nivolumab group, 61 years (IQR: 53–68) in placebo group | Unresectable advanced or recurrent gastric/gastroesophageal junction (G/GEJ) cancer | Nivolumab (3 mg/kg every 2 weeks) | Placebo | -Nivolumab Median OS = 5.26 (95% CI, 4.60–6.37) -Placebo: Median OS = 4.14 (95% CI, 3.42–4.86) -Hazard Ratio (HR): 0.62 (95% CI, 0.51–0.76) |
| Planchard et al., 2020 [24] | Phase 3 RCT | 126 patients (62 (Study A), 64 (Study B)) | Adults (≥65 years) | metastatic non-small cell lung cancer | Durvalumab (Study A), Durvalumab + Tremelimumab (Study B) | Standard of Care (SoC) | -Durvalumab Median OS = 11.7 (95% CI, 8.2–17.4) -SoC: Median OS = 6.8 (95% CI, 4.9–10.2) -Hazard Ratio (HR): 0.63 ((95% CI, 0.42–0.93) |
| Socinski et al., 2018 [25] | Randomized trial | 692 patients (356 (Atezolizumab + Bevacizumab + Carboplatin + Paclitaxel)/336 (Bevacizumab + Carboplatin + Paclitaxel)) | Above 18 | Non-Small Cell Lung Cancer (wild type population) | Atezolizumab + Bevacizumab + Carboplatin + Paclitaxel | Bevacizumab + Carboplatin + Paclitaxel | -Intervention: 8.3 mon ((95% CI, 7.7–9.8) -Control: 6.8 mon ((95% CI, 6.0–7.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babiker, R.; Wali, A.F.; El-Tanani, M.; Rabbani, S.A.; Rangraze, I.; Satyam, S.M.; Patni, M.A.; El-Tanani, Y. Comparative Efficacy of Immune Checkpoint Inhibitors and Therapeutic Vaccines in Solid Tumors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Vaccines 2025, 13, 423. https://doi.org/10.3390/vaccines13040423
Babiker R, Wali AF, El-Tanani M, Rabbani SA, Rangraze I, Satyam SM, Patni MA, El-Tanani Y. Comparative Efficacy of Immune Checkpoint Inhibitors and Therapeutic Vaccines in Solid Tumors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Vaccines. 2025; 13(4):423. https://doi.org/10.3390/vaccines13040423
Chicago/Turabian StyleBabiker, Rasha, Adil Farooq Wali, Mohamed El-Tanani, Syed Arman Rabbani, Imran Rangraze, Shakta Mani Satyam, Mohamed Anas Patni, and Yahia El-Tanani. 2025. "Comparative Efficacy of Immune Checkpoint Inhibitors and Therapeutic Vaccines in Solid Tumors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Vaccines 13, no. 4: 423. https://doi.org/10.3390/vaccines13040423
APA StyleBabiker, R., Wali, A. F., El-Tanani, M., Rabbani, S. A., Rangraze, I., Satyam, S. M., Patni, M. A., & El-Tanani, Y. (2025). Comparative Efficacy of Immune Checkpoint Inhibitors and Therapeutic Vaccines in Solid Tumors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Vaccines, 13(4), 423. https://doi.org/10.3390/vaccines13040423