Response of Sport Horses to Different Formulations of Equine Influenza Vaccine

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Horses
2.2. Vaccines
2.3. Vaccination
2.4. Collection of Samples
2.5. Serology
2.6. Statistical Analysis
3. Results
3.1. Pre-Existing Immune Status
3.2. Reaction to Vaccination
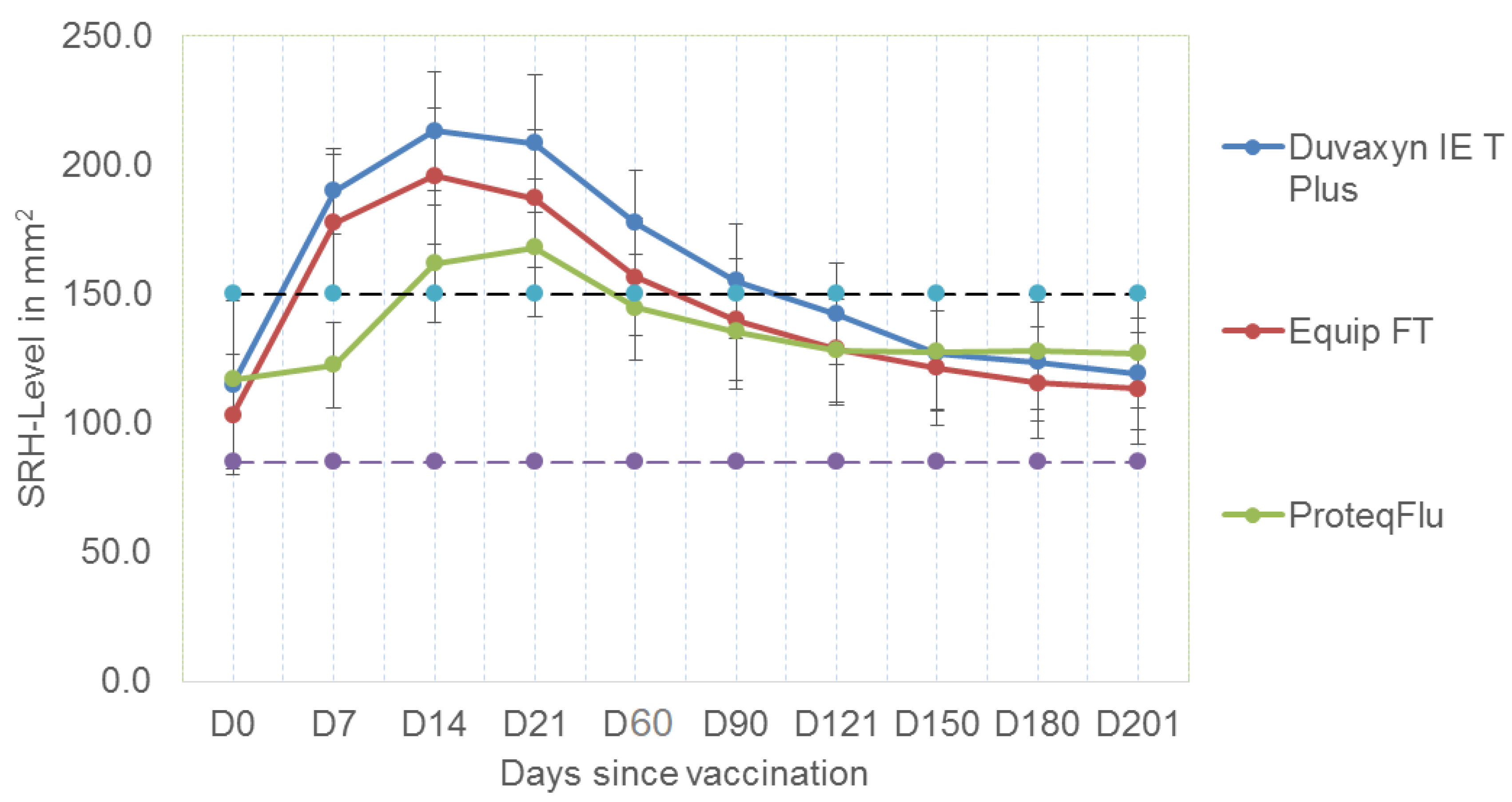
3.3. Immune Response to Booster Vaccination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cullinane, A.; Newton, J.R. Equine influenza—A global perspective. Vet. Microbiol. 2013, 167, 205–214. [Google Scholar] [CrossRef]
- Paillot, R. A systematic review of recent advances in equine influenza vaccination. Vaccines 2014, 2, 797. [Google Scholar] [CrossRef]
- Gildea, S.; Garvey, M.; Lyons, P.; Lyons, R.; Gahan, J.; Walsh, C.; Cullinane, A. Multifocal equine influenza outbreak with vaccination breakdown in thoroughbred racehorses. Pathogens 2018, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Gildea, S.; Lyons, P.; Lyons, R.; Gahan, J.; Garvey, M.; Cullinane, A. Annual booster vaccination and the risk of equine influenza to Thoroughbred racehorses. Equine Vet. J. 2020, 52, 509–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mumford, J.A.; Wood, J. Establishing an acceptability threshold for equine influenza vaccines. Dev. Biol. Stand. 1992, 79, 137–146. [Google Scholar]
- Mumford, J.; Jessett, D.; Rollinson, E.; Hannant, D.; Draper, M. Duration of protective efficacy of equine influenza immunostimulating complex/tetanus vaccines. Vet. Rec. 1994, 134, 158–162. [Google Scholar] [CrossRef]
- Mumford, J.A.; Jessett, D.; Dunleavy, U.; Wood, J.; Hannant, D.; Sundquist, B.; Cook, R.F. Antigenicity and immunogenicity of experimental equine influenza ISCOM vaccines. Vaccine 1994, 12, 857–863. [Google Scholar] [CrossRef]
- Newton, J.R.; Verheyen, K.; Wood, J.L.; Yates, P.J.; Mumford, J.A. Equine influenza in the United Kingdom in 1998. Vet. Rec. 1999, 145, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Newton, J.R.; Townsend, H.G.; Wood, J.L.; Sinclair, R.; Hannant, D.; Mumford, J.A. Immunity to equine influenza: Relationship of vaccine-induced antibody in young Thoroughbred racehorses to protection against field infection with influenza A/equine-2 viruses (H3N8). Equine Vet. J. 2000, 32, 65–74. [Google Scholar] [CrossRef]
- Mumford, J.A. Collaborative study for the establishment of three European Pharmacopoeia Biological Reference Preparations for equine influenza horse antiserum. Pharmeuropa 2000, 1, 7–21. [Google Scholar]
- Daly, J.; Daas, A.; Behr-Gross, M.E. Collaborative study for the establishment of a candidate equine influenza subtype 2 American-like strain A/EQ/South Africa/4/03-horse antiserum biological reference preparation. Pharmeuropa Bio/Biol. Stand. Programme EDQM 2007, 2007, 7–14. [Google Scholar]
- Mumford, J.A. Epidemiology and vaccinology of equine influenza, quality control of equine influenza vaccines. In Proceedings of the International Symposium Organised by the European Directorate for the Quality of Medicines (EDQM), Council of Europe, Budapest, Hungary, 10–11 December 2001; EDQM: Strasbourg, France, 2001; pp. 7–12. [Google Scholar]
- Gildea, S.; Arkins, S.; Walsh, C.; Cullinane, A. A comparison of antibody responses to commercial equine influenza vaccines following primary vaccination of Thoroughbred weanlings—A randomised blind study. Vaccine 2011, 29, 9214–9223. [Google Scholar] [CrossRef] [PubMed]
- Gildea, S.; Arkins, S.; Walsh, C.; Cullinane, A. A comparison of antibody responses to commercial equine influenza vaccines following annual booster vaccination of National Hunt horses—A randomised blind study. Vaccine 2011, 29, 3917–3922. [Google Scholar] [CrossRef] [PubMed]
- Gildea, S.; Arkins, S.; Cullinane, A. A comparative antibody study of the potential susceptibility of Thoroughbred and non-Thoroughbred horse populations in Ireland to equine influenza virus. Influenza Other Respir. Viruses 2010, 4, 363–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gildea, S.; Quinlivan, M.; Arkins, S.; Cullinane, A. The molecular epidemiology of equine influenza in Ireland from 2007–2010 and its international significance. Equine Vet. J. 2012, 44, 387–392. [Google Scholar] [CrossRef] [PubMed]
- R CoreTeam. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Heldens, J.G.M.; Weststrate, M.W.; van den Hoven, R. Area under the curve calculations as a tool to compare the efficacy of equine influenza vaccines—A retrospective analysis of three independent field trials. J. Immunol. Methods 2002, 264, 11–17. [Google Scholar] [CrossRef]
- Cullinane, A.; Gahan, J.; Walsh, C.; Nemoto, M.; Entenfellner, J.; Olguin-Perglione, C.; Garvey, M.; Huang Fu, T.Q.; Venner, M.; Yamanaka, T.; et al. Evaluation of current equine influenza vaccination protocols prior to shipment, guided by OIE standards. Vaccines 2020, 8, 107. [Google Scholar] [CrossRef] [Green Version]
- Daly, J.M.; Yates, P.J.; Newton, J.R.; Park, A.; Henley, W.; Wood, J.L.N.; Davis-Poynter, N.; Mumford, J.A. Evidence supporting the inclusion of strains from each of the two co-circulating lineages of H3N8 equine influenza virus in vaccines. Vaccine 2004, 22, 4101–4109. [Google Scholar] [CrossRef]
- de la Rua-Domenech, R.; Reid, S.W.; Gonzalez-Zariquiey, A.E.; Wood, J.L.; Gettinby, G. Modelling the spread of a viral infection in equine populations managed in Thoroughbred racehorse training yards. Prev. Vet. Med. 1999, 47, 61–77. [Google Scholar] [CrossRef]
- Park, A.W.; Wood, J.L.; Newton, J.R.; Daly, J.; Mumford, J.A.; Grenfell, B.T. Optimising vaccination strategies in equine influenza. Vaccine 2003, 21, 2862–2870. [Google Scholar] [CrossRef]
- Newton, J.R.; Park, A.W.; Wood, J.L.N. Maximizing the benefits of vaccination against equine influenza. In Equine Respiratory Diseases; Lekeux, P., Ed.; International Veterinary Information Service: Ithaca, NY, USA, 2004. [Google Scholar]
- Andersen, S.A.; Petersen, H.H.; Ersbøll, A.K.; Falk-Rønne, J.; Jacobsen, S. Vaccination elicits a prominent acute phase response in horses. Vet. J. 2012, 191, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Gershwin, L.J.; Netherwood, K.A.; Norris, M.S.; Behrens, N.E.; Shao, M.X. Equine IgE responses to non-viral vaccine components. Vaccine 2012, 30, 7615–7620. [Google Scholar] [CrossRef] [PubMed]
- Gärtner, B.C.; Meyer, T. Vaccination in elite athletes. Sports Med. 2014, 44, 1361–1376. [Google Scholar] [CrossRef] [Green Version]
- Minke, J.M.; Toulemonde, C.E.; Coupier, H.; Guigal, P.M.; Dinic, S.; Sindle, T.; Jessett, D.; Black, L.; Bublot, M.; Pardo, M.C.; et al. Efficacy of a canarypox-vectored recombinant vaccine expressing the hemagglutinin gene of equine influenza H3N8 virus in the protection of ponies from viral challenge. Am. J. Vet. Res. 2007, 68, 213–219. [Google Scholar] [CrossRef]
- Crouch, C.F.; Daly, J.; Hannant, D.; Wilkins, J.; Francis, M.J. Immune responses and protective efficacy in ponies immunised with an equine influenza ISCOM vaccine containing an ‘American lineage’ H3N8 virus. Vaccine 2004, 23, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Bryant, N.A.; Paillot, R.; Rash, A.S.; Medcalf, E.; Montesso, F.; Ross, J.; Watson, J.; Jeggo, M.; Lewis, N.S.; Newton, J.R.; et al. Comparison of two modern vaccines and previous influenza infection against challenge with an equine influenza virus from the Australian 2007 outbreak. Vet. Res. 2010, 41, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paillot, R.; Kydd, J.H.; Sindle, T.; Hannant, D.; Edlund Toulemonde, C.; Audonnet, J.C.; Minke, J.M.; Daly, J.M. Antibody and IFN-gamma responses induced by a recombinant canarypox vaccine and challenge infection with equine influenza virus. Vet. Immunol. Immunopathol. 2006, 112, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Paillot, R.; Grimmett, H.; Elton, D.; Daly, J.M. Protection, systemic IFNgamma, and antibody responses induced by an ISCOM-based vaccine against a recent equine influenza virus in its natural host. Vet. Res. 2008, 39, 21. [Google Scholar] [CrossRef] [Green Version]
- Paillot, R.; Prowse, L.; Montesso, F.; Huang, C.M.; Barnes, H.; Escala, J. Whole inactivated equine influenza vaccine: Efficacy against a representative clade 2 equine influenza virus, IFNgamma synthesis and duration of humoral immunity. Vet. Microbiol. 2013, 162, 396–407. [Google Scholar] [CrossRef]
- OIE. Expert surveillance panel on equine influenza vaccine composition—Conclusions and recommendations. Off. Int. Epizoot. Bull. 2010, 2, 44–45. [Google Scholar]


{kind=link}
| Vaccine Producer | Nature | Adjuvant | Virus Strains | Tetanus Toxoid |
|---|---|---|---|---|
| Duvaxyn IE-T Plus (Elanco)® | Inactivated whole virus | Carbomer Aluminium hydroxide | A/eq/Prague/56 (H7N7) A/eq/Suffolk/89 (H3N8) A/eq/Newmarket/1/93 (H3N8) | >150 I.U. |
| Equip FT (Zoetis)® | Subunit | ISCOM Quillaic acid derivative Aluminium-phosphate | A/eq/Newmarket/77 (H7N7) A/eq/Kentucky/98 (H3N8) A/eq/Borlange/91 (H3N8) | 100 Lf |
| ProteqFlu TE (Merial)® | Canarypox-recombinant | Carbomer | A/eq/Ohio/03 (H3N8) A/eq/Richmond/1/07 (H3N8) | >30 I.U. |
| Vaccine | D0 | D7 | D14 | D21 | D60 | D90 | D121 | D150 | D180 | D201 |
|---|---|---|---|---|---|---|---|---|---|---|
| Duvaxyn IET Plus | 35 | 34 | 32 | 34 | 29 | 30 | 30 | 23 | 23 | 20 |
| Equip FT® | 34 | 33 | 34 | 33 | 26 | 26 | 26 | 20 | 20 | 15 |
| Proteq Flu Te® | 34 | 34 | 31 | 30 | 23 | 23 | 23 | 18 | 18 | 14 |
| Total | 103 | 101 | 97 | 97 | 78 | 79 | 79 | 61 | 61 | 49 |
| Vaccine | Nature | Vaccine Virus Strains | Amino Acid Identity (%) | |
|---|---|---|---|---|
| A/eq/South Africa/4/03 | A/eq/Meath/1/07 | |||
| Duvaxyn IE-T Plus (Elanco)® | Inactivated whole virus | A/eq/Prague/56 (H7N7) A/eq/Suffolk/89 (H3N8) A/eq/Newmarket/1/93 (H3N8) | 47.69 97.27 96.96 * | 47.51 96.90 96.96 * |
| Equip FT (Zoetis)® | Subunit | A/eq/Newmarket/77(H7N7) A/eq/Kentucky/98 (H3N8) A/eq/Borlange/91 (H3N8) | 47.51 96.04 * 92.70 * | 47.34 96.04 * 92.40 * |
| ProteqFlu TE (Merial)® | Canarypox-recombinant | A/eq/Ohio/03 (H3N8) A/eq/Richmond/1/07 (H3N8) | 100 98.90 | 98.90 100 |
| Time Points | 95% Confidence Interval | p Value | |
|---|---|---|---|
| Lower | Upper | ||
| D0–D7 | |||
| EquipFT-Duvaxyn IE-T Plus | −11.61 | 14.22 | >0.9 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −81.04 | −55.4 | <0.001 * |
| ProteqFLU TE-EquipFT | −82.44 | −56.61 | <0.001 * |
| D0–D14 | |||
| EquipFT-Duvaxyn IE-T Plus | −25.42 | 12.9 | 0.7 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −72.83 | −33.6 | <0.001 * |
| ProteqFLU TE-EquipFT | −66.3 | −27.7 | <0.001 * |
| D0–D21 | |||
| EquipFT-Duvaxyn IE-T Plus | −27.1 | 7.50 | 0.4 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −62.2 | −26.75 | <0.001 * |
| ProteqFLU TE-EquipFT | −52.7 | −16.71 | <0.001 * |
| D0–D60 | |||
| EquipFT-Duvaxyn IE-T Plus | −24.73 | 11.16 | 0.7 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −54.48 | −17.38 | <0.001 * |
| ProteqFLU TE-EquipFT | −48.17 | −4.18 | <0.01 * |
| D0–D90 | |||
| EquipFT-Duvaxyn IE-T Plus | −18.59 | 14.72 | >0.9 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −41.14 | −6.69 | <0.01 * |
| ProteqFLU TE-EquipFT | −48.17 | −4.18 | <0.01 * |
| D0–D121 | |||
| EquipFT-Duvaxyn IE-T Plus | −15.55 | 14.69 | >0.9 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −34.14 | −2.86 | 0.016 * |
| ProteqFLU TE-EquipFT | −34.22 | −1.9 | 0.02 * |
| D0–D150 | |||
| EquipFT-Duvaxyn IE-T Plus | −4.98 | 24.16 | 0.3 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −18.04 | 12.27 | 0.9 |
| ProteqFLU TE-EquipFT | −28.26 | 3.05 | 0.1 |
| D0–D180 | |||
| EquipFT-Duvaxyn IE-T Plus | −7.3 | 21.71 | 0.5 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −14.03 | 15.84 | >0.9 |
| ProteqFLU TE-EquipFT | −21.71 | 9.13 | 0.6 |
| D0–D201 | |||
| EquipFT-Duvaxyn IE-T Plus | −7.95 | 25.05 | 0.4 |
| ProteqFLU TE-Duvaxyn IE-T Plus | −14.2 | 19.5 | >0.9 |
| ProteqFLU TE-EquipFT | −23.9 | 12.0 | 0.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Entenfellner, J.; Gahan, J.; Garvey, M.; Walsh, C.; Venner, M.; Cullinane, A. Response of Sport Horses to Different Formulations of Equine Influenza Vaccine. Vaccines 2020, 8, 372. https://doi.org/10.3390/vaccines8030372
Entenfellner J, Gahan J, Garvey M, Walsh C, Venner M, Cullinane A. Response of Sport Horses to Different Formulations of Equine Influenza Vaccine. Vaccines. 2020; 8(3):372. https://doi.org/10.3390/vaccines8030372
Chicago/Turabian StyleEntenfellner, Johanna, Jacinta Gahan, Marie Garvey, Cathal Walsh, Monica Venner, and Ann Cullinane. 2020. "Response of Sport Horses to Different Formulations of Equine Influenza Vaccine" Vaccines 8, no. 3: 372. https://doi.org/10.3390/vaccines8030372
APA StyleEntenfellner, J., Gahan, J., Garvey, M., Walsh, C., Venner, M., & Cullinane, A. (2020). Response of Sport Horses to Different Formulations of Equine Influenza Vaccine. Vaccines, 8(3), 372. https://doi.org/10.3390/vaccines8030372