Willingness to Pay for Seasonal Influenza Vaccination among Children, Chronic Disease Patients, and the Elderly in China: A National Cross-Sectional Survey


 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Study Sample Characteristics
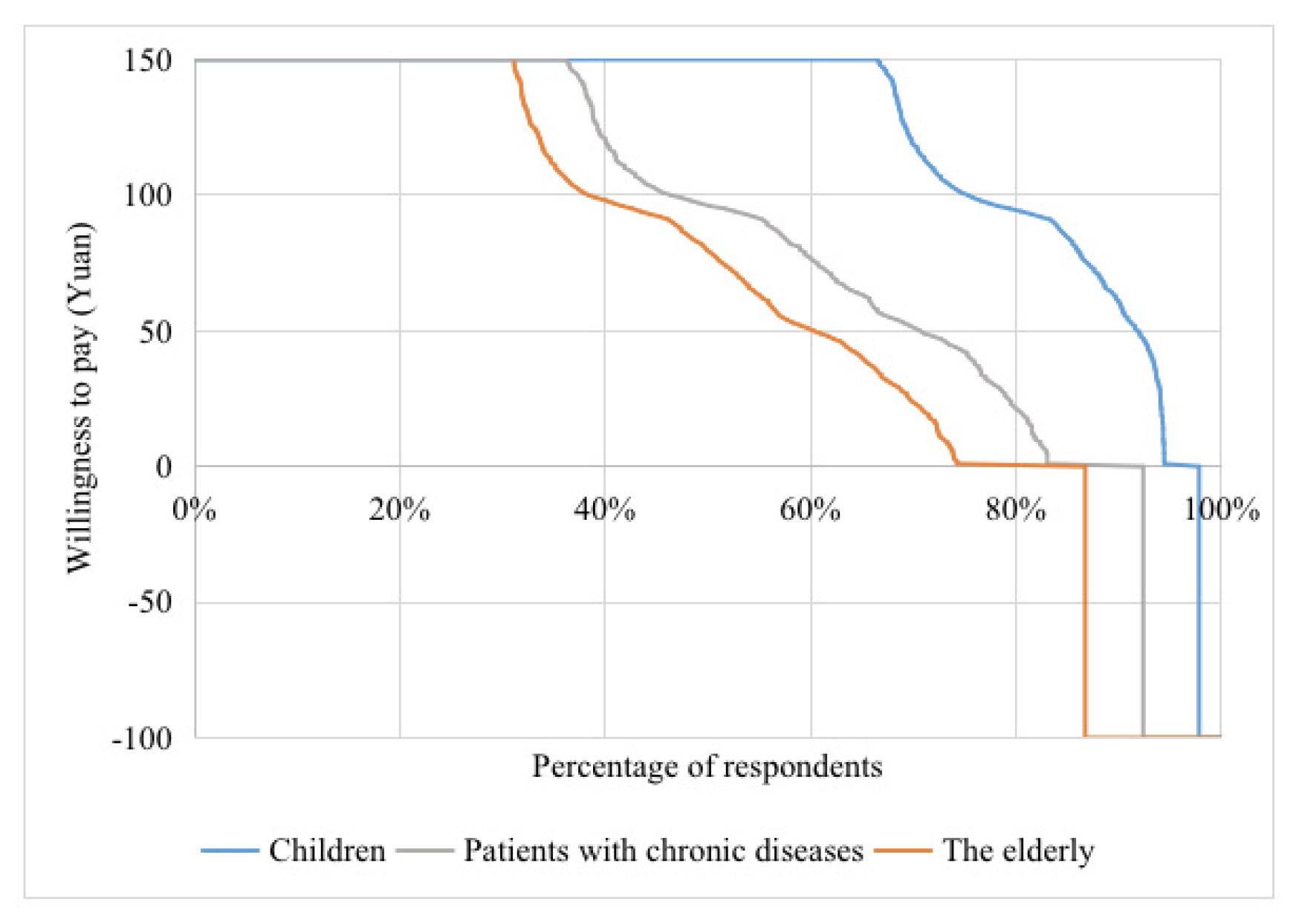
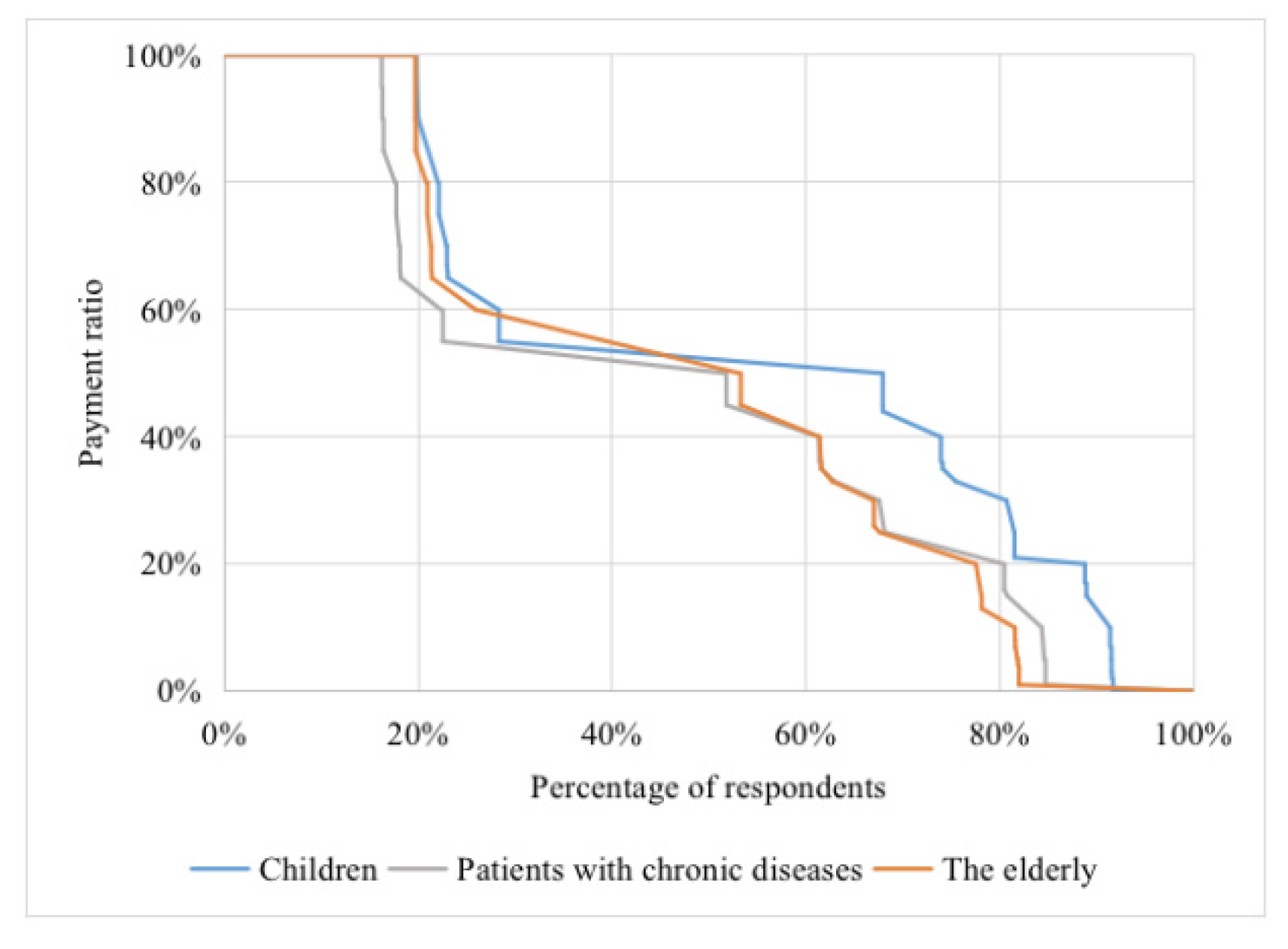
3.2. Willingness to Pay
3.3. Recommended Financing Sources
3.4. Influencing Factors of WTP
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Factors | Children | Chronic Disease Patients | The Elderly | |
|---|---|---|---|---|
| Complacency | Perceived high possibility of catching influenza | −0.91 (3.36) | 9.79 (5.77) | 14.63 * (4.36) |
| Perceived high severity of influenza | 13.84 * (3.77) | −0.05 (5.71) | 2.50 (4.11) | |
| Perceived high importance of influenza vaccination | 55.58 * (5.24) | 47.29 * (6.83) | 41.94 * (4.78) | |
| Having knowledge of the priority groups for influenza vaccination (Children, chronic disease patients, the elderly) | 13.32 * (3.36) | 17.79 * (5.46) | 20.30 * (3.86) | |
| Considering that individuals should participate in payment | 56.13 * (3.85) | 69.35 * (6.12) | 93.35 * (4.35) | |
| Convenience | Price hinder vaccination behavior | −66.04 * (4.08) | −49.57 * (5.49) | −44.54 * (4.03) |
| Distance and time consumed hinder vaccination behavior | −3.31 (4.71) | −2.39 (6.42) | −5.69 (5.16) | |
| Having shortage of influenza vaccines in clinics | −3.10 (3.66) | 6.05 (5.67) | 4.54 (4.24) | |
| Confidence | Perceived high safety of influenza vaccination | 8.18 (4.38) | 5.35 (6.37) | 8.00 (4.67) |
| Perceived high efficacy of influenza vaccination | 3.35 (4.25) | −1.86 (6.41) | 6.99 (4.61) | |
| Having trust in doctors’ vaccination advice | 2.99 (5.52) | 21.25 * (7.79) | 23.40 * (5.15) | |
| Having doubts about vaccination | −10.40 * (3.42) | −2.46 (5.26) | −12.59 * (4.25) | |
| Willing to vaccinate but have not done it | 23.66 * (3.22) | 10.19 (5.47) | 24.01 * (4.14) | |
Appendix B
| Factors | Children | Chronic Disease Patients | The Elderly | |
|---|---|---|---|---|
| Complacency | Perceived high possibility of catching influenza | −0.34 (0.51) | 2.45 (1.25) | 2.39 * (0.84) |
| Perceived high severity of influenza | 1.75 * (0.57) | −1.11 (1.26) | 0.33 (0.81) | |
| Perceived high importance of influenza vaccination | 6.08 * (0.82) | 6.98 * (1.54) | 4.25 * (0.97) | |
| Having knowledge of the priority groups for influenza vaccination (Children, chronic disease patients, the elderly) | 1.68 * (0.51) | 3.09 * (1.18) | 2.69 * (0.74) | |
| Considering that individuals should participate in payment | 7.58 * (0.59) | 12.95 * (1.38) | 15.13 * (0.90) | |
| Convenience | Price hinder vaccination behavior | −10.88 * (0.61) | −13.96 * (1.23) | −11.96 * (0.81) |
| Distance and time consumed hinder vaccination behavior | −0.86 (0.70) | −1.78 (1.38) | −1.63 (0.99) | |
| Having shortage of influenza vaccines in clinics | −0.40 (0.55) | 1.29 (1.25) | 1.24 (0.83) | |
| Confidence | Perceived high safety of influenza vaccination | 1.13 (0.67) | −0.22 (1.41) | 1.48 (0.92) |
| Perceived high efficacy of influenza vaccination | 0.07 (0.65) | −0.16 (1.41) | 0.80 (0.91) | |
| Having trust in doctors’ vaccination advice | 0.64 (0.84) | 3.57 * (1.74) | 3.99 * (1.04) | |
| Having doubts about vaccination | −1.07 * (0.51) | −0.17 (1.16) | −2.14 * (0.84) | |
| Willing to vaccinate but have not done it | 2.68 * (0.48) | 1.57 (1.18) | 2.47 * (0.78) | |
References
- World Health Organization. Influenza (Seasonal) Fact Sheet November 2018. Available online: http://www.who.int/mediacentre/factsheets/fs211/en/ (accessed on 20 April 2020).
- Li, L.; Liu, Y.; Wu, P.; Peng, Z.; Wang, X.; Chen, T.; Wong, J.; Yang, J.; Bond, H.S.; Wang, L.; et al. Influenza-associated excess respiratory mortality in China, 2010–2015: A population-based study. Lancet Public Health 2019, 4, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Osterholm, M.T.; Kelley, N.S.; Sommer, A.; Belongia, E.A. Efficacy and effectiveness of influenza vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 36–44. [Google Scholar] [CrossRef]
- Influenza, V.T.; National Immunization Advisory Committee and Technical Working Group. Technical guidelines for seasonal influenza vaccination in China (2019–2020). Chin. J. Prev. Med. 2020, 54, 21–36. (In Chinese) [Google Scholar] [CrossRef]
- Lai, X.; Fang, H. Immunization schedules and financing strategies in the U.S, the U.K, Germany and Japan and their experience for China. Natl. Med. J. China 2020, 100, 85–89. (In Chinese) [Google Scholar]
- Zhou, L.; Su, Q.; Xu, Z.; Feng, A.; Jin, H.; Wang, S.; Feng, Z. Seasonal Influenza Vaccination Coverage Rate of Target Groups in Selected Cities and Provinces in China by Season (2009/10 to 2011/12). PLoS ONE 2013, 8, e73724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blank, P.R.; Schwenkglenks, M.; Szucs, T.D. Vaccination coverage rates in eleven European countries during two consecutive influenza seasons. J. Infect. 2009, 58, 446–458. [Google Scholar] [CrossRef]
- Tian, C.W.; Wang, H.; Wang, W.M.; Luo, X.M. Influenza vaccination coverage among US children from 2004/2005 to 2015/2016. J. Public Health 2019, 41, e62–e69. [Google Scholar] [CrossRef]
- Rizzo, C.; Rezza, G.; Ricciardi, W. Strategies in recommending influenza vaccination in Europe and US. Hum. Vaccines Immunother. 2018, 14, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Atkins, K.E.; Feng, L.; Pang, M.; Zheng, Y.; Liu, X.; Cowling, B.J.; Yu, H. Seasonal influenza vaccination in china: Landscape of diverse regional reimbursement policy, and budget impact analysis. Vaccine 2016, 34, 5724–5735. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Vaccines against influenza WHO position paper. Wkly. Epidemiol. Rec. 2012, 87, 461–476. [Google Scholar]
- The General Office of the State Council. Notice on the Reform Plan for the Division of Central and Local Financial Governance and Expenditure Responsibilities in the Healthcare Sector. Available online: http://www.gov.cn/zhengce/content/2018-08/13/content_5313489.htm (accessed on 11 January 2019).
- Hanemann, M.W. Willingness to pay and willingness to accept: How much can they differ? Am. Econ. Rev. 1991, 81, 635–647. [Google Scholar] [CrossRef]
- Mitchell, R.C.; Carson, R.T. Using Surveys to Value Public Goods: The Contingent Valuation Method; Johns Hopkins University Press: Baltimore, MD, USA, 1989; pp. 295–297. [Google Scholar]
- Klose, T. The contingent valuation method in health care. Health Policy 1999, 47, 97–123. [Google Scholar] [CrossRef]
- Olsen, J.A.; Donaldson, C. Helicopters, hearts, and hips: Using willingness-to-pay to set priorities for public sector health care programmes. Soc. Sci. Med. 1998, 46, 1–12. [Google Scholar] [CrossRef]
- Strategic Advisory Group of Experts. Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf?ua=1January (accessed on 15 April 2019).
- Department of Population and Employment Statistics, National Bureau of Statistics of China. China Population & Employment Statistics Yearbook 2019; China Statistics Press: Beijing, China, 2019. [Google Scholar]
- Jiang, M.; Li, P.; Wang, W.; Zhao, M.; Atif, N.; Zhu, S.; Fang, Y. Cost-effectiveness of quadrivalent versus trivalent influenza vaccine for elderly population in China. Vaccine 2020, 38, 1057–1064. [Google Scholar] [CrossRef]
- Hou, Z.; Chang, J.; Yue, D.; Fang, H.; Meng, Q.; Zhang, Y. Determinants of willingness to pay for self-paid vaccines in China. Vaccine 2014, 32, 4471–4477. [Google Scholar] [CrossRef] [PubMed]
- Penfold, R.B.; Rusinak, D.; Lieu, T.A.; Shefer, A.; Messonnier, M.; Lee, G.M. Financing and systems barriers to seasonal influenza vaccine delivery in community settings. Vaccine 2011, 29, 9632–9639. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, N.; Schaetti, C.; Grize, L.; Purohit, V.; Joseph, S.; Schindler, C.; Kudale, A.; Weiss, M.G. Sociocultural determinants of anticipated acceptance of pandemic influenza vaccine in Pune, India: A community survey using mixed-methods. Int. J. Public Health 2017, 62, 103–115. [Google Scholar] [CrossRef]
- Crainich, D.; Eeckhoudt, L.; Menegatti, M. Vaccination as a trade-off between risks. Ital. Econ. J. 2019, 5, 455–472. [Google Scholar] [CrossRef]
- Yoo, B.K.; Berry, A.; Kasajima, M.; Szilagyi, G. Association between Medicaid reimbursement and child influenza vaccination rates. Pediatrics 2010, 126, e998–e1010. [Google Scholar] [CrossRef]
- Asgary, A. Assessing households’ willingness to pay for an immediate pandemic influenza vaccination programme. Scand. J. Public Health 2012, 40, 412–417. [Google Scholar] [CrossRef]
- Ibuka, Y.; Bessho, S.I. Subsidies for influenza vaccination, vaccination rates, and health outcomes among the elderly in japan. Jpn. World Econ. 2015, 36, 56–66. [Google Scholar] [CrossRef]
- Yang, J.; Atkins, K.E.; Feng, L.; Baguelin, M.; Wu, P.; Yan, H.; Lau, E.H.Y.; Wu, J.T.; Liu, Y.; Cowling, B.J.; et al. Cost-effectiveness of introducing national seasonal influenza vaccination for adults aged 60 years and above in mainland China: A modelling analysis. BMC Med. 2020, 18, 90. [Google Scholar] [CrossRef] [PubMed]
- Folland, S.; Goodman, A.C.; Stano, M. Epidemiology and Economics: HIV/AIDS in Africa. In The Economics of Health and Health Care, 7th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2012; pp. 531–548. [Google Scholar]
- Wilder-Smith, A.; Longini, I.; Zuber, P.L.; Bärnighausen, T.; Edmunds, W.J.; Dean, N.; Spicher, V.M.; Benissa, M.R.; Gessner, B.D. The public health value of vaccines beyond efficacy: Methods, measures and outcomes. BMC Med. 2017, 15, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Toxvaerd, F. The economics of vaccination. J. Theor. Biol. 2014, 363, 105–117. [Google Scholar] [CrossRef]
- Han, M.; Shi, X.; Cai, C.; Zhang, Y.; Xu, W. Evolution of non-communicable disease prevention and control in China. Glob. Health Promot. 2017, 26, 90–95. [Google Scholar] [CrossRef]



| Characteristics | Children Aged 6–59 Months, n (%) | Chronic Disease Patients Aged 18–59 Years, n (%) | Elderly Aged above 60 Years, n (%) | p-Value |
|---|---|---|---|---|
| Sociodemographics | ||||
| Age (years) | – | |||
| <1 | 1768 (26.5) | – | – | – |
| 1 | 1959 (29.4) | – | – | – |
| 2 | 1241 (18.6) | – | – | – |
| 3–5 | 1700 (25.5) | – | – | – |
| 18–39 | – | 72 (4.1) | – | – |
| 40–49 | – | 313 (18.0) | – | – |
| 50–59 | – | 1350 (77.9) | – | – |
| 60–69 | – | – | 2045 (53.1) | – |
| 70–79 | – | – | 1491 (38.7) | – |
| ≥80 | – | – | 313 (8.2) | – |
| Age of respondent (years) | – | |||
| <30 | 2049 (30.7) | – | – | – |
| 30–39 | 3039 (45.6) | – | – | – |
| 40–49 | 569 (8.5) | – | – | – |
| ≥50 | 1011 (15.2) | – | – | – |
| Relationship between respondent and child | – | |||
| Father | 1122 (16.8) | – | – | – |
| Mother | 4405 (66.1) | – | – | – |
| Grandfather | 213 (3.2) | – | – | – |
| Grandmother | 928 (13.9) | – | – | – |
| Gender | <0.01 * | |||
| Male | 3497 (52.4) | 596 (34.4) | 1515 (39.4) | – |
| Female | 3171 (47.6) | 1139 (65.6) | 2334 (60.6) | – |
| Marital status | <0.01 * | |||
| Married | – | 1575 (90.8) | 2909 (75.6) | – |
| Unmarried/divorced/widowed | – | 160 (9.2) | 940 (24.4) | – |
| Education level a | <0.01 * | |||
| Elementary school and below | 674 (10.1) | 618 (35.6) | 2146 (55.8) | – |
| Junior high school | 1710 (25.6) | 580 (33.4) | 915 (23.8) | – |
| High school/vocational school | 1503 (22.5) | 361 (20.8) | 583 (15.1) | – |
| Junior college | 1250 (18.7) | 108 (6.2) | 125 (3.3) | – |
| Four-year college and above | 1531 (23.1) | 68 (4.0) | 80 (2.0) | – |
| Household monthly per capita income (thousand yuan) b,c | 2.7 (2.8) | 1.8 (2.4) | 1.7 (1.6) | <0.01 * |
| Place of residence | <0.01 * | |||
| Urban | 3854 (57.8) | 904 (52.1) | 2107 (54.7) | – |
| Rural | 2814 (42.2) | 831 (47.9) | 1742 (45.3) | – |
| Basic medical insurance type a | <0.01 * | |||
| Medical insurance for urban and rural residents | 4081 (61.2) | 1212 (69.9) | 2551 (66.3) | – |
| Urban employee medical insurance | 2380 (35.7) | 492 (28.4) | 1189 (30.9) | – |
| Without basic medical insurance | 207 (3.1) | 31 (1.7) | 109 (2.8) | – |
| Self-reported health status | <0.01 * | |||
| Good | 5812 (87.2) | 596 (34.4) | 1578 (41.0) | – |
| Fair or poor | 856 (12.8) | 1139 (65.6) | 2271 (59.0) | – |
| Had influenza-like illness in the past year | <0.01 * | |||
| Yes | 3049 (45.7) | 291 (16.8) | 489 (12.7) | – |
| No | 3619 (54.3) | 1444 (83.2) | 3360 (87.3) | – |
| Province | <0.01 * | |||
| Beijing | 668 (10.0) | 153 (8.8) | 332 (8.6) | – |
| Shanghai | 602 (9.0) | 158 (9.1) | 332 (8.6) | – |
| Jilin | 681 (10.2) | 170 (9.8) | 391 (10.2) | – |
| Yunnan | 629 (9.5) | 155 (8.9) | 308 (8.0) | – |
| Shandong | 626 (9.4) | 172 (9.9) | 355 (9.2) | – |
| Guangdong | 621 (9.3) | 153 (8.8) | 334 (8.7) | – |
| Jiangxi | 621 (9.3) | 165 (9.5) | 330 (8.6) | – |
| Gansu | 742 (11.1) | 225 (13.0) | 577 (15.0) | – |
| Chongqing | 848 (12.7) | 222 (12.8) | 576 (15.0) | – |
| Henan | 630 (9.5) | 162 (9.4) | 314 (8.1) | – |
| Knowledge and perception of influenza and vaccination | ||||
| Perceived high possibility of catching influenza | <0.01 * | |||
| Yes | 3056 (45.8) | 537 (31.0) | 1032 (26.8) | – |
| No | 3612 (54.2) | 1198 (69.0) | 2817 (73.2) | – |
| Perceived high severity of influenza | <0.01 * | |||
| Yes | 4982 (74.7) | 1170 (67.4) | 2508 (65.2) | – |
| No | 1686 (25.3) | 565 (32.6) | 1341 (34.8) | – |
| Perceived high importance of influenza vaccination | <0.01 * | |||
| Yes | 6000 (90.0) | 1367 (78.8) | 2819 (73.2) | – |
| No | 668 (10.0) | 368 (21.2) | 1030 (26.8) | – |
| Knowledge of priority groups (children, chronic disease patients, elderly) | <0.01 * | |||
| Yes | 3834 (57.5) | 687 (39.6) | 1505 (39.1) | – |
| No | 2834 (42.5) | 1048 (60.4) | 2344 (60.9) | – |
| Price hinders vaccination | <0.01 * | |||
| Yes | 1159 (17.4) | 628 (36.2) | 1353 (35.2) | – |
| No | 5509 (82.6) | 1107 (63.8) | 2496 (64.8) | – |
| Distance and time hinder vaccination | <0.01 * | |||
| Yes | 838 (12.6) | 326 (18.8) | 562 (14.6) | – |
| No | 5830 (87.4) | 1409 (81.2) | 3287 (85.4) | – |
| Shortage of influenza vaccines in clinics | 0.07 | |||
| Yes | 3165 (47.5) | 789 (45.5) | 1746 (45.4) | – |
| No | 3503 (52.5) | 946 (54.5) | 2103 (54.6) | – |
| Perceived high safety of influenza vaccination | <0.01 * | |||
| Yes | 5376 (80.6) | 1252 (72.2) | 2587 (67.2) | – |
| No | 1292 (19.4) | 483 (27.8) | 1262 (32.8) | – |
| Perceived high efficacy of influenza vaccination | <0.01 * | |||
| Yes | 5315 (79.7) | 1258 (72.5) | 2522 (65.5) | – |
| No | 1353 (20.3) | 477 (27.5) | 1327 (34.5) | – |
| Trust in doctors’ vaccination advice | <0.01 * | |||
| Yes | 6057 (90.8) | 1500 (86.5) | 3208 (83.3) | – |
| No | 611 (9.2) | 235 (13.5) | 641 (16.7) | – |
| Doubts about vaccination | <0.01* | |||
| Yes | 4014 (60.2) | 624 (36.0) | 1000 (26.0) | – |
| No | 2654 (39.8) | 1111 (64.0) | 2849 (74.0) | – |
| Willing to vaccinate but have not done it | <0.01 * | |||
| Yes | 3425 (51.4) | 567 (32.7) | 1071 (27.8) | – |
| No | 3243 (48.6) | 1168 (67.3) | 2778 (72.2) | – |
| Willingness to Pay | Children | Chronic Disease Patients | Elderly |
|---|---|---|---|
| Willingness to pay (yuan) a,b | 127.5 (39.2) | 96.5 (53.7) | 88.1 (56.8) |
| Expected self-payment ratio assuming total cost is 50 yuan (%) a,b | 51.7 (29.7) | 43.7 (31.4) | 44.9 (33.6) |
| Willingness to pay for total cost assuming it is 50 yuan, n (%) b | 6052 (92.8) | 1208 (75.4) | 2349 (70.4) |
| Financing Sources | Children | Chronic Disease Patients | Elderly |
|---|---|---|---|
| Should individuals, medical insurance, or the government pay for influenza vaccination? | |||
| Individuals, n (%) | 5285 (81.0) | 1275 (79.5) | 2565 (76.8) |
| Medical insurance, n (%) | 6152 (94.3) | 1528 (95.3) | 3155 (94.5) |
| Government, n (%) | 6187 (94.8) | 1536 (95.8) | 3189 (95.5) |
| Total | 6524 | 1603 | 3339 |
| Factors | Children | Chronic Disease Patients | Elderly | |
|---|---|---|---|---|
| Complacency | Perceived high possibility of catching influenza | −2.09 (3.14) | 10.12 (5.17) | 11.32 * (3.97) |
| Perceived high severity of influenza | 10.87 * (3.54) | −4.58 (5.22) | 1.56 (3.85) | |
| Perceived high importance of influenza vaccination | 37.73 * (5.08) | 28.84 * (6.35) | 20.12 * (4.59) | |
| Knowledge of priority groups for influenza vaccination (children, chronic disease patients, elderly) | 10.41 * (3.14) | 12.76 * (4.88) | 12.73 * (3.52) | |
| Considering that individuals should participate in payment | 47.02 * (3.65) | 53.49 * (5.63) | 71.70 * (4.14) | |
| Convenience | Price hinders vaccination behavior | −67.50 * (3.81) | −57.63 * (4.97) | −56.68 * (3.73) |
| Distance and time hinder vaccination behavior | −5.34 (4.37) | −7.35 (5.70) | −7.73 (4.70) | |
| Shortage of influenza vaccines in clinics | −2.49 (3.42) | 5.34 (5.18) | 5.85 (3.93) | |
| Confidence | Perceived high safety of influenza vaccination | 7.00 (4.14) | −0.89 (5.82) | 7.03 (4.37) |
| Perceived high efficacy of influenza vaccination | 0.41 (4.02) | −0.65 (5.82) | 3.81 (4.31) | |
| Trust in doctors’ vaccination advice | 3.94 (5.22) | 14.73 * (7.19) | 18.90 * (4.93) | |
| Doubts about vaccination | −6.64 * (3.19) | −0.68 (4.79) | −10.16 * (4.00) | |
| Willing to vaccinate but have not done it | 16.64 * (3.01) | 6.49 (4.86) | 11.70 * (3.70) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, X.; Rong, H.; Ma, X.; Hou, Z.; Li, S.; Jing, R.; Zhang, H.; Peng, Z.; Feng, L.; Fang, H. Willingness to Pay for Seasonal Influenza Vaccination among Children, Chronic Disease Patients, and the Elderly in China: A National Cross-Sectional Survey. Vaccines 2020, 8, 405. https://doi.org/10.3390/vaccines8030405
Lai X, Rong H, Ma X, Hou Z, Li S, Jing R, Zhang H, Peng Z, Feng L, Fang H. Willingness to Pay for Seasonal Influenza Vaccination among Children, Chronic Disease Patients, and the Elderly in China: A National Cross-Sectional Survey. Vaccines. 2020; 8(3):405. https://doi.org/10.3390/vaccines8030405
Chicago/Turabian StyleLai, Xiaozhen, Hongguo Rong, Xiaochen Ma, Zhiyuan Hou, Shunping Li, Rize Jing, Haijun Zhang, Zhibin Peng, Luzhao Feng, and Hai Fang. 2020. "Willingness to Pay for Seasonal Influenza Vaccination among Children, Chronic Disease Patients, and the Elderly in China: A National Cross-Sectional Survey" Vaccines 8, no. 3: 405. https://doi.org/10.3390/vaccines8030405