Influenza Vaccination Hesitancy among Healthcare Workers in South Al Batinah Governorate in Oman: A Cross-Sectional Study


 , , and
, , and
Abstract
:1. Introduction
2. Methodology
3. Results
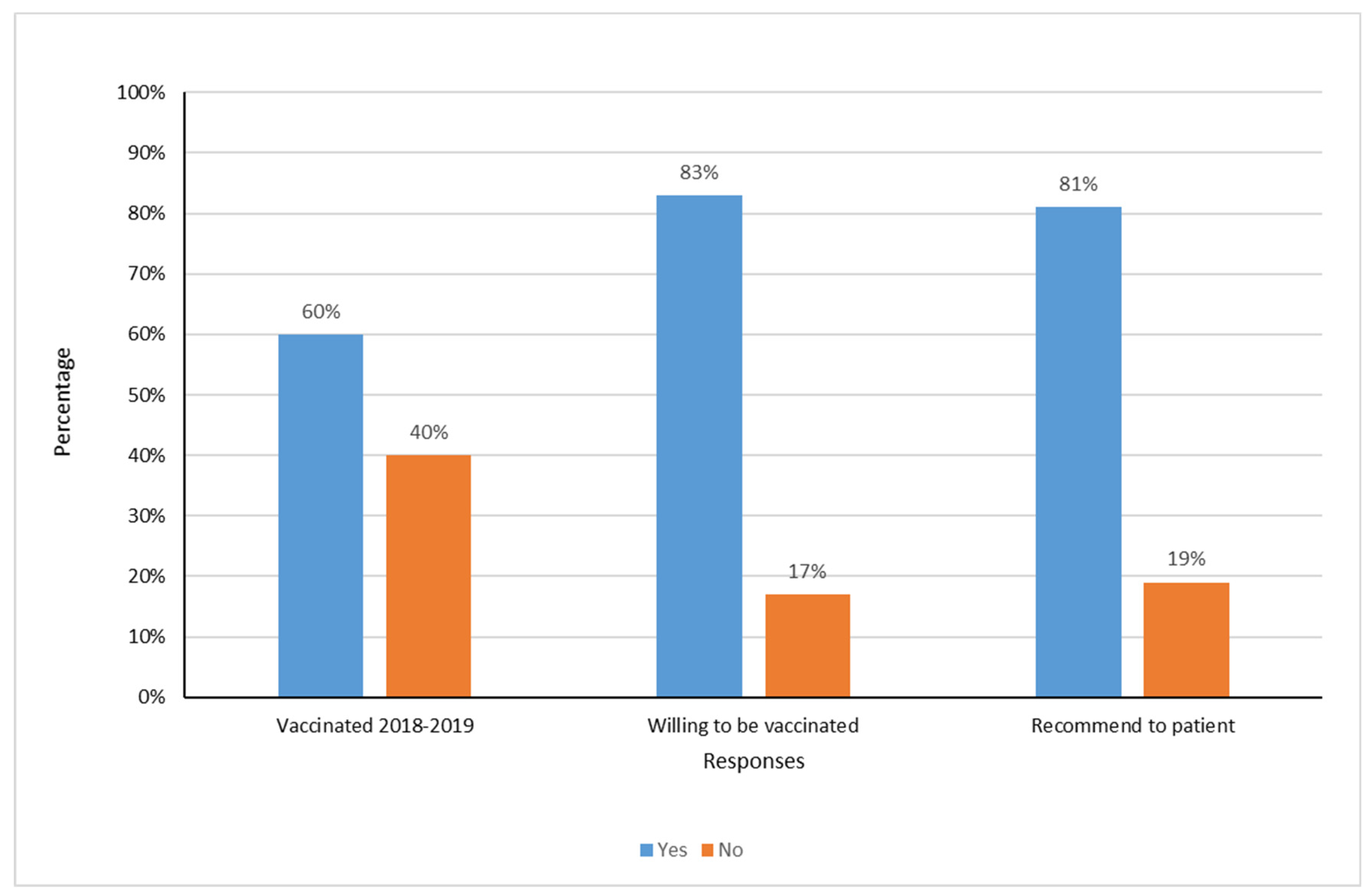
3.1. Influenza Vaccination Status
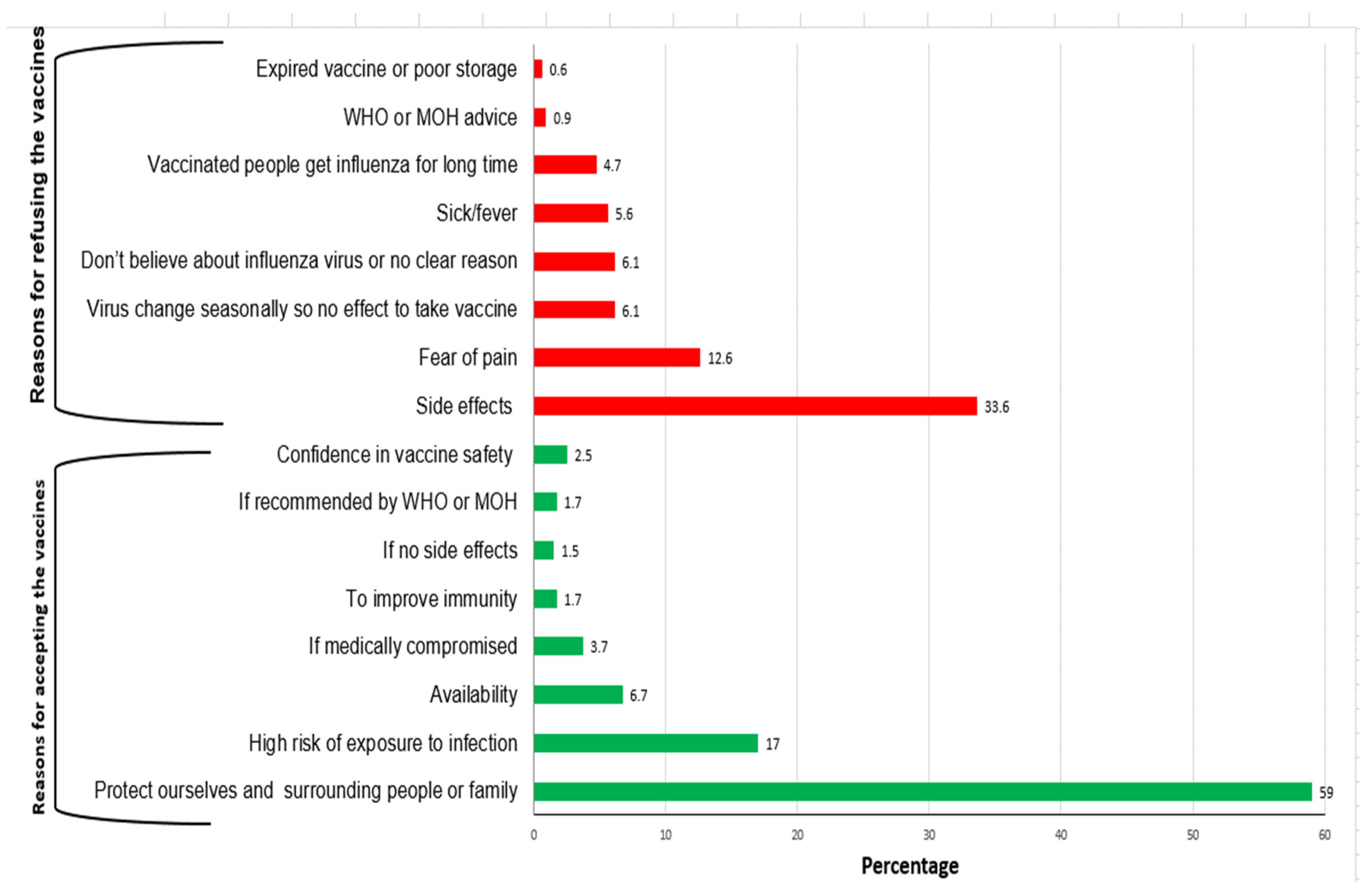
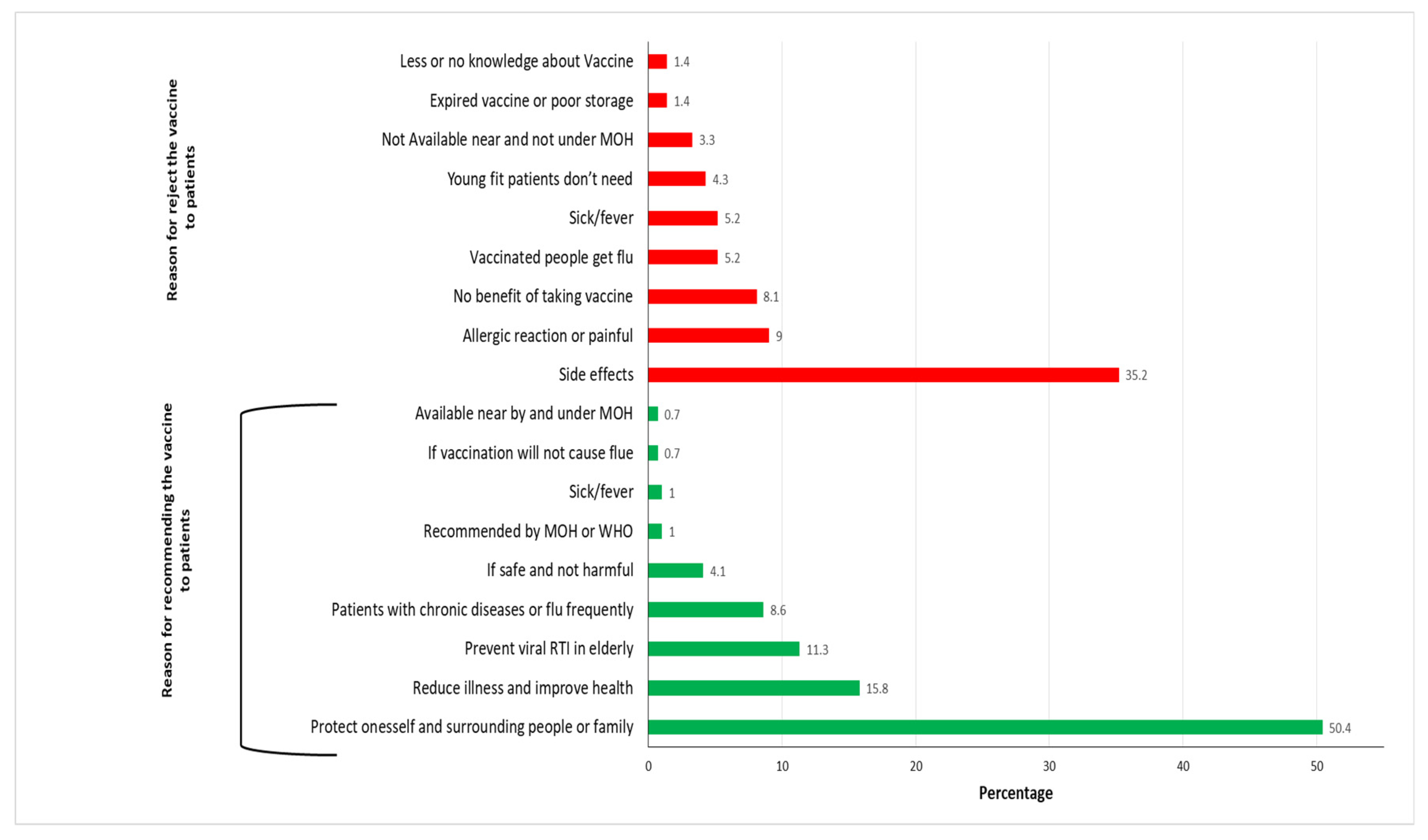
3.2. Willingness to Be Vaccinated and/or Recommend Vaccination to Patients
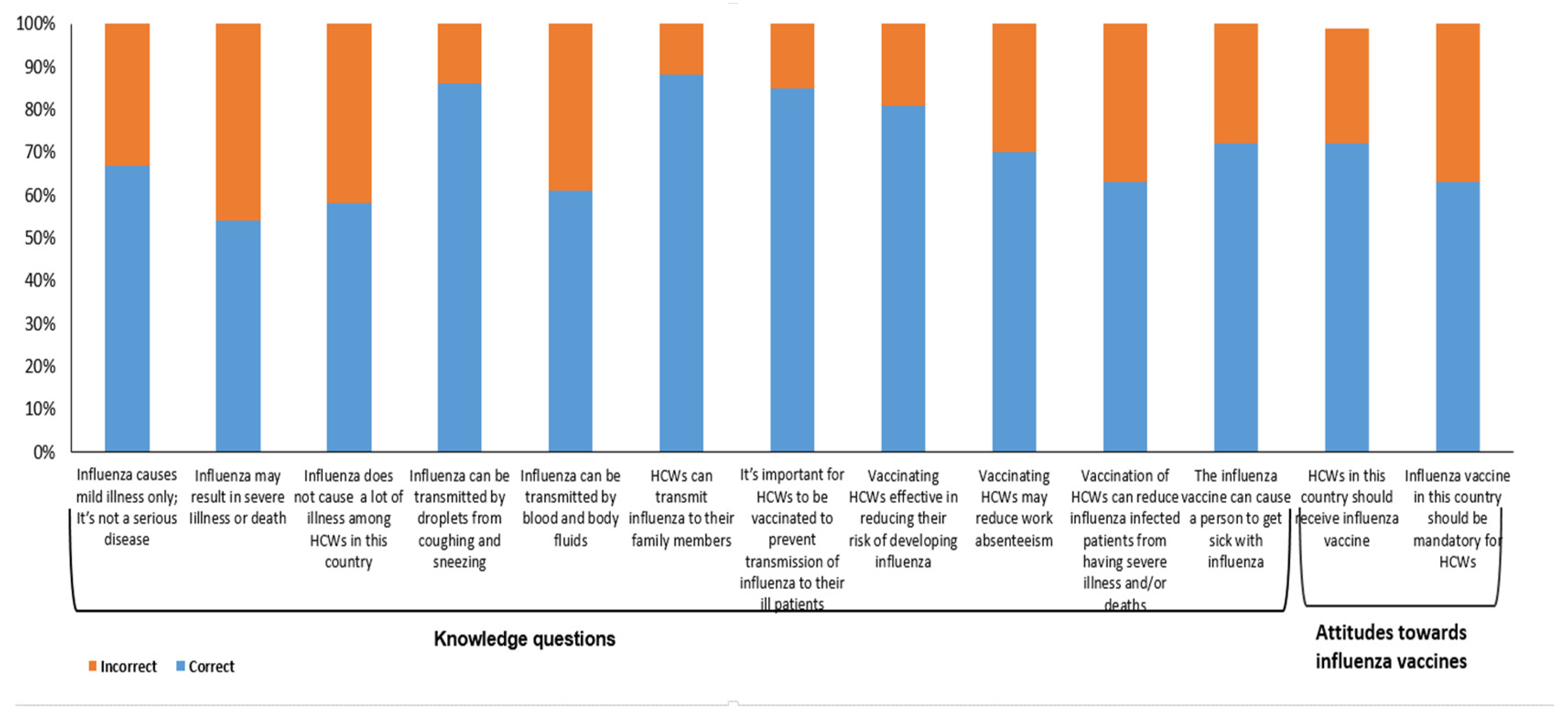
3.3. Knowledge about Influenza Vaccine
3.4. Association between Socio-Demographic Factors, Knowledge Scores, Attitudes and Influenza Vaccine Uptake in the 2018–2019 Season
3.5. The Association between Socio-Demographic Factors, Knowledge Scores and Attitudes with the Willingness to Recommend Influenza Vaccination in Patients
4. Discussion
5. Conclusions and the Way Forward
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Influenza Strategy 2019–2030. Available online: https://apps.who.int/iris/bitstream/handle/10665/311184/9789241515320-eng.pdf?ua=1 (accessed on 5 July 2020).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Stott, D.J.; Kerr, G.; Carman, W.F. Nosocomial transmission of influenza. Occup. Med. (Lond.) 2002, 52, 249–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voirin, N.; Barret, B.; Metzger, M.-H.; Vanhems, P. Hospital-acquired influenza: A synthesis using the Outbreak Reports and Intervention Studies of Nosocomial Infection (ORION) statement. J. Hosp. Infect. 2009, 71, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Doaa, M.A.-H.; Rima, M.A.B.; Badr, A.A.A.; Seif, S.A.A.; Hanan, S.A.K.; Al-Jardani, A.K.; al Yaqubi, F.M.; al Abaidani, I.S. Estimating the burden of influenza-associated hospitalization and deaths in Oman (2012–2015). Influenza Other Respir. Viruses 2018, 12, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Lietz, J.; Westermann, C.; Nienhaus, A.; Schablon, A. The Occupational Risk of Influenza A (H1N1) Infection among Healthcare Personnel during the 2009 Pandemic: A Systematic Review and Meta-Analysis of Observational Studies. PLoS ONE 2016, 11, e0162061. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza vaccination in healthcare workers: A comprehensive critical appraisal of the literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef] [Green Version]
- Dawn, C.; Jenkin, H.M.; Kathleen, F.M.; Philipp Lambach, J.; Nguyen-Van-Tam, S. A Rapid Evidence Appraisal of Influenza Vaccination in Health Workers: An Important Policy in an Area of Imperfect Evidence. In Press. Vaccine: X Journal Homepage. Available online: www.elsevier.com/locate/jvacxhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC6668237/pdf/main.pdf (accessed on 23 May 2020).
- Voirin, N.; Payet, C.; Barrat, A.; Cattuto, C.; Khanafer, N.; Regis, C.; Kim, B.; Comte, B.; Casalegno, J.; Lina, B.; et al. Combining high-resolution contact data with virological data to investigate influenza transmission in a tertiary care hospital. Infect. Control Hosp. Epidemiol. 2015, 36, 254–260. [Google Scholar] [CrossRef]
- Pagani, L.; Thomas, Y.; Huttner, B.; Sauvan, V.; Notaridis, G.; Kaiser, L.; Iten, A.; Pittet, D.; Harbarth, S. Transmission and effect of multiple clusters of seasonal influenza in a Swiss geriatric hospital. J. Am. Geriatr. Soc. 2015, 63, 739–744. [Google Scholar] [CrossRef]
- Valley-Omar, Z.; Nindo, F.; Mudau, M.; Hsiao, M.; Martin, D.P. Phylogenetic Exploration of Nosocomial Transmission Chains of 2009 Influenza A/H1N1 among Children Admitted at Red Cross War Memorial Children’s Hospital, Cape Town, South Africa in 2011. PLoS ONE. 2015, 10, e0141744. [Google Scholar] [CrossRef] [Green Version]
- Pereira, M.; Williams, S.; Restrick, L.; Cullinan, P.; Hopkinson, N.S.; London Respiratory, N. Healthcare worker influenza vaccination and sickness absence—An ecological study. Clin. Med. (Lond.) 2017, 17, 484–489. [Google Scholar] [CrossRef]
- International Council of Nurses. Available online: https://www.icn.ch/news/more-600-nurses-die-covid-19-worldwide (accessed on 23 May 2020).
- Paterson, P.; Meurice, F.; Lawrence, R.; Stanberry, S.G.; Susan, L.R.; Heidi, J.L. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meeting of the Strategic Advisory Group of Experts on Immunization, April 2012—Conclusions and Recommendations. Wkly Epidemiol. Rec. 2012, 87, 201–216. Available online: http://www.who.int/wer/2012/wer8721.pdf (accessed on 4 January 2019).
- Vaccines against Influenza. In WHO Position Paper; WHO: Geneva, Switzerland, 2012; Volume 87, pp. 461–476. Available online: https://www.who.int/wer/2012/wer8747.pdf (accessed on 14 May 2019).
- WHO. Principles and Considerations for Adding a Vaccine to a National Immunization Program: From Decision to Implementation and Monitoring; World Health Organization: Geneva, Switzerland, 2014; Available online: http://www.who.int/immunization/documents/general/ISBN_978_92_4_15068_92 (accessed on 14 May 2019).
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Piotr, K.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- To, K.W.; Lai, A.; Lee, K.C.; Koh, D.; Lee, S.S. Increasing the coverage of influenza vaccination in healthcare workers: Review of challenges and solutions. J. Hosp. Infect. 2016, 94, 133–142. [Google Scholar] [CrossRef]
- Neli, M.E.; Gabriela, S.T.; Tatina, T.T. Seasonal influenza vaccination: Knowledge, attitude and practice in Varna, Bulgaria. Ther. Adv. Vaccines Immunother. 2019, 7, 1–9. [Google Scholar]
- Gülten, E.; Özer Türk, D.; Erol, A.; Özel, D. The Knowledge, Attitudes and Beliefs of the Healthcare Workers about Influenza Infection and Vaccination at a Public Hospital in Turkey. Infect. Dis. Clin. Microbiol. 2019, 2, 87–96. [Google Scholar] [CrossRef]
- Abu-Gharbieh, E.; Fahmy, S.; Rasool, B.A.; Khan, S. Influenza Vaccination: Healthcare Workers Attitude in Three Middle East Countries. Int. J. Med. Sci. 2010, 7, 319–325. [Google Scholar] [CrossRef] [Green Version]
- Morales, K.F.; Menning, L.; Lambach, P. The faces of influenza vaccine recommendation: A Literature review of the determinants and barriers to health providers’ recommendation of influenza vaccine in pregnancy. Vaccine 2020, 38, 4805–4815. Available online: http://creativecommons.org/licenses/by-nc-nd/3.0/igo/ (accessed on 12 April 2020). [CrossRef]
- AlMarzooqi, L.M.; AlMajidi, A.A.; AlHammadi, A.A.; AlAli, N.; Khansaheb, H.H. Knowledge, attitude, and practice of influenza vaccine immunization among primary healthcare providers in Dubai health authority, 2016–2017. Hum. Vaccines Immunother. 2018, 14, 2999–3004. [Google Scholar] [CrossRef]
- Hosamirudsari, H.; Rezaee Kanavee, A.; Ghanbari, M.; Akbarpour, S.; Alimohamadi, Y. Assessment of the belief and attitudes of Iranian healthcare personnel’s toward the influenza infection and influenza vaccination. J. Prev. Med. Hyg. 2019, 60, E178–E183. [Google Scholar] [CrossRef] [PubMed]
- Elawad, K.H.; Farag, E.A.; Abuelgasim, D.A.; Smatti, M.K.; Al-Romaihi, H.E.; al Thani, M.; al Mujalli, H.; Shehata, Z.; Alex, M.; al Thani, A.A.; et al. Improving Influenza Vaccination Rate among Primary Healthcare Workers in Qatar. Vaccines 2017, 5, 36. [Google Scholar] [CrossRef] [Green Version]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, W.M.; Chow, A.; Hein, A.A.; Lee, L.T.; Leo, Y.S.; Ho, H.J. Factors influencing seasonal influenza vaccination uptake among health care workers in an adult tertiary care hospital in Singapore: A cross-sectional survey. Am. J. Infect. Control 2019, 47, 133–138. [Google Scholar] [CrossRef]
- Bellia, C.; Setbon, M.; Zylberman, P.; Flahault, A. Healthcare worker compliance with seasonal and pandemic influenza vaccination. Influenza Other. Respir. Viruses. 2013, 7 (Suppl. 2), 97–104. [Google Scholar] [CrossRef] [Green Version]
- Durando, P.; Alicino, C.; Dini, G.; Barberis, I.; Bagnasco, A.M.; Iudici, R.; Zanini, M.; Martini, M.; Toletone, A.; Paganino, C.; et al. Determinants of adherence to seasonal influenza vaccination among healthcare workers from an Italian region: Results from a cross-sectional study. BMJ Open 2016, 6, e010779. [Google Scholar] [CrossRef] [PubMed]
- Amodio, E.; Anastasi, G.; Marsala, M.G.; Torregrossa, M.V.; Romano, N.; Firenze, A. Vaccination against the 2009 pandemic influenza A (H1N1) among healthcare workers in the major teaching hospital of Sicily (Italy). Vaccine 2011, 29, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Alshammari, T.M.; Yusuff, K.B.; Aziz, M.M.; Subaie, G.M. Healthcare professionals’ knowledge, attitude and acceptance of influenza vaccination in Saudi Arabia: A multicenter cross-sectional study. BMC Health Serv. Res. 2019, 19, 229. [Google Scholar] [CrossRef]
- La Torre, G.; Mannocci, A.; Ursillo, P.; Bontempi, C.; Firenze, A.; Panico, M.G.; Sferrazza, A.; Ronga, C.; D’Anna, A.; Amodio, E.; et al. Prevalence of influenza vaccination among nurses and ancillary workers in Italy: Systematic review and meta-analysis. Hum. Vaccines 2011, 7, 728–733. [Google Scholar] [CrossRef]
- Alsh ammari, T.M.; Aljofan, M.; Subaie, G.; Hussain, T. Knowledge, awareness, attitude, and practice of health-care professionals toward hepatitis B disease and vaccination in Saudi Arabia. Hum Vaccines Immunother. 2019, 15, 2816–2823. [Google Scholar] [CrossRef]
- Hogan, V.; Lenehan, M.; Hogan, M.; Natin, D.P. Influenza vaccine uptake and attitudes of healthcare workers in Ireland. Occup. Med. (Lond.) 2019, 69, 494–499. [Google Scholar] [CrossRef]
- Haridi, H.K.; Salman, K.A.; Basaif, E.A.; Al-Skaibi, D.K. Influenza vaccine uptake, determinants, motivators, and barriers of the vaccine receipt among healthcare workers in a tertiary care hospital in Saudi Arabia. J. Hosp. Infect. 2017, 96, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Hirve, S.; Kieny, M.P. Seasonal vaccines—Critical path to pandemic influenza response. Vaccine 2017, 35, 851–852. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Study Population n = 390 * | Vaccine Taken n = 213 (54.6%) | Vaccine Not Taken n = 140 (35.9%) | χ2 | p | |||
|---|---|---|---|---|---|---|---|---|
| Age (years) | ||||||||
| n | % | n | % | n | % | |||
| 18–29 | 9 | 2.3 | 1 | 11.1 | 7 | 77.7 | 11.1 | 0.05 |
| 25–29 | 89 | 22.8 | 42 | 47.1 | 30 | 33.7 | ||
| 30–34 | 131 | 33.6 | 72 | 55.0 | 49 | 37.4 | ||
| 35–39 | 97 | 24.9 | 57 | 58.7 | 34 | 35.0 | ||
| 40–49 | 52 | 13.3 | 35 | 67.3 | 14 | 26.9 | ||
| 50–59 | 12 | 3.1 | 6 | 50.0 | 6 | 50.0 | ||
| Gender | ||||||||
| Male | 86 | 22.1 | 36 | 41.9 | 38 | 44.2 | 5.4 | 0.021 |
| Female | 304 | 77.9 | 177 | 58.2 | 102 | 33.6 | ||
| Occupation | ||||||||
| Nurse | 173 | 44.4 | 110 | 63.6 | 53 | 30.6 | 13.9 | 0.016 |
| Doctor/resident/intern | 108 | 27.7 | 60 | 55.6 | 39 | 36.1 | ||
| Pharmacist | 37 | 9.5 | 18 | 48.6 | 16 | 43.2 | ||
| Lab technician | 33 | 8.5 | 11 | 33.3 | 14 | 42.4 | ||
| X-ray technician | 23 | 5.9 | 5 | 21.7 | 12 | 52.2 | ||
| Others | 16 | 4.1 | 7 | 43.7 | 4 | 25.0 | ||
| Working department | ||||||||
| General/internal medicine | 103 | 26.4 | 67 | 65.0 | 30 | 29.1 | 27.81 | 0.033 |
| Emergency department | 18 | 4.6 | 9 | 50.0 | 6 | 33.3 | ||
| Obstetrics/gynecology | 18 | 4.6 | 11 | 61.1 | 7 | 38.8 | ||
| Adult intensive care unit | 7 | 1.8 | 6 | 85.7 | 0 | 0 | ||
| Neonatal intensive care unit | 2 | 0.5 | 1 | 50.0 | 1 | 50.0 | ||
| Pediatrics | 16 | 4.1 | 8 | 50.0 | 8 | 50.0 | ||
| Radiology | 22 | 5.6 | 5 | 22.7 | 4 | 18.2 | ||
| Surgery | 9 | 2.3 | 5 | 55.6 | 4 | 44.5 | ||
| Other | 192 | 49.2 | 98 | 51.0 | 73 | 38.0 | ||
| Did not answer | 3 | 0.8 | 0 | 0 | ||||
| Volume of patients | ||||||||
| <=10 | 49 | 12.6 | 21 | 42.9 | 23 | 46.9 | 12.7 | 0.013 |
| 11–20 | 62 | 15.9 | 41 | 66.1 | 15 | 24.2 | ||
| 21–30 | 73 | 18.7 | 52 | 71.2 | 20 | 27.4 | ||
| 31–40 | 54 | 13.8 | 28 | 51.9 | 20 | 37.0 | ||
| >40 | 139 | 35.6 | 68 | 48.9 | 56 | 40.3 | ||
| Did not answer | 13 | 3.3 | - | - | - | - | ||
| Highest education level | ||||||||
| College or university | 247 | 63.3 | 133 | 53.8 | 89 | 36.0 | 0.46 | 0.927 |
| Master’s degree | 37 | 9.5 | 21 | 56.8 | 15 | 40.6 | ||
| Doctorate | 7 | 1.8 | 4 | 57.1 | 3 | 42.9 | ||
| Other | 95 | 24.4 | 54 | 56.8 | 31 | 32.6 | ||
| Did not answer | 4 | 1.0 | - | - | - | - | ||
| Influenza Vaccine Uptake | Willingness to Vaccinate | Recommend to Patients | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Unadjusted Odds Ratio | 95% CI | p Value | Adjusted Odds Ratio | 95% CI | p Value | Unadjusted Odds Ratio | 95% CI | p Value | Adjusted Odds Ratio | 95% CI | p Value | Unadjusted Odds Ratio | 95% CI | p Value | Adjusted Odds Ratio | 95% CI | p Value |
| Females * versus males | 1.54 | 0.91–2.57 | 0.08 | 1.53 | 0.93–2.53 | 0.09 | 0.56 | 0.24–1.17 | 0.11 | 0.44 | 0.19–0.99 | 0.046 | 0.99 | 0.50–1.88 | 0.97 | |||
| Age > 30 years * versus < 30 years | 1.27 | 0.78–2.08 | 0.3 | 1.04 | 0.63–1.71 | 0.89 | 1.54 | 0.83–2.81 | 0.13 | 1.31 | 0.67–2.58 | 0.44 | 2.03 | 1.13–3.61 | <0.001 | 0.88 | 0.43–1.83 | 0.74 |
| Nurses and doctors * versus others | 1.75 | 1.09–2.79 | 0.01 | 1.32 | 0.80–2.18 | 0.3 | 2.49 | 1.39–4.42 | <0.001 | 1.78 | 0.90–3.54 | 0.1 | 3.32 | 1.88–5.80 | <0.001 | 1.9 | 0.96–3.76 | 0.07 |
| University and above education * versus and below | 0.79 | 0.48–1.30 | 0.33 | 0.78 | 0.47–2.19 | 0.33 | 0.45 | 0.20–0.94 | 0.03 | 0.52 | 0.23–1.17 | 0.12 | 0.31 | 0.12–0.68 | <0.001 | 0.43 | 0.18–1.03 | 0.06 |
| General medicine, emergency medicine and intensive care * versus others | 1.92 | 1.20–3.10 | 0.004 | 1.71 | 1.05–2.78 | 0.03 | 1.75 | 0.94–3.45 | 0.07 | 1.15 | 0.62–2.57 | 0.7 | 2.66 | 1.36–5.51 | 0.002 | 1.91 | 0.88–4.14 | 0.1 |
| >30 patients daily versus < 30 patients | 0.75 | 0.42–1.31 | 0.27 | 0.75 | 0.42–1.31 | 0.27 | 0.97 | 0.56–1.67 | 0.91 | |||||||||
| >10 years of service * versus < 10 years of service | 0.83 | 0.54–1.28 | 0.38 | 1.25 | 0.72–2.20 | 0.39 | 2.43 | 1.39–4.31 | <0.001 | 2.79 | 1.39–5.59 | 0.004 | ||||||
| Vaccinated in 2018–2019 * versus not vaccinated | 3.27 | 1.84–5.88 | <0.001 | 1.78 | 1.17–2.76 | 0.008 | 1.88 | 1.09–3.25 | 0.02 | 1.03 | 0.68–1.54 | 0.89 | ||||||
| Knowledge score > 7 * versus < 7 | 1.35 | 0.88–2.08 | 0.15 | 1.1 | 0.71–1.72 | 0.68 | 2.28 | 1.26–4.25 | 0.004 | 1.12 | 0.57–2.20 | 0.75 | 2.4 | 1.34–4.39 | 0.002 | 1.14 | 0.57–2.24 | 0.72 |
| HCWs should receive influenza vaccine (yes * versus no) | 1.72 | 1.07–2.77 | 0.02 | 1.06 | 0.61–1.85 | 0.82 | 8.37 | 4.54–15.56 | <0.001 | 5.5 | 2.73–11.09 | <0.001 | 7.9 | 4.38–14.36 | <0.001 | 4.69 | 2.20–9.99 | <0.001 |
| Influenza vaccine should be mandatory (yes * versus no) | 2.04 | 1.30–3.18 | <0.001 | 1.9 | 1.17–3.10 | 0.01 | 4.47 | 2.49–8.16 | <0.001 | 2.02 | 1.02–3.98 | 0.04 | 3.11 | 1.78–5.44 | <0.001 | 1.17 | 0.56–2.43 | 0.68 |
| Willingness to be vaccinated | 7.26 | 3.88–13.49 | <0.001 | 3.25 | 1.61–6.59 | <0.001 | ||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awaidy, S.T.A.; K. Al Mayahi, Z.; Kaddoura, M.; Mahomed, O.; Lahoud, N.; Abubakar, A.; Zaraket, H. Influenza Vaccination Hesitancy among Healthcare Workers in South Al Batinah Governorate in Oman: A Cross-Sectional Study. Vaccines 2020, 8, 661. https://doi.org/10.3390/vaccines8040661
Awaidy STA, K. Al Mayahi Z, Kaddoura M, Mahomed O, Lahoud N, Abubakar A, Zaraket H. Influenza Vaccination Hesitancy among Healthcare Workers in South Al Batinah Governorate in Oman: A Cross-Sectional Study. Vaccines. 2020; 8(4):661. https://doi.org/10.3390/vaccines8040661
Chicago/Turabian StyleAwaidy, Salah T. Al, Zayid K. Al Mayahi, Malak Kaddoura, Ozayr Mahomed, Nathalie Lahoud, Abdinasir Abubakar, and Hassan Zaraket. 2020. "Influenza Vaccination Hesitancy among Healthcare Workers in South Al Batinah Governorate in Oman: A Cross-Sectional Study" Vaccines 8, no. 4: 661. https://doi.org/10.3390/vaccines8040661
APA StyleAwaidy, S. T. A., K. Al Mayahi, Z., Kaddoura, M., Mahomed, O., Lahoud, N., Abubakar, A., & Zaraket, H. (2020). Influenza Vaccination Hesitancy among Healthcare Workers in South Al Batinah Governorate in Oman: A Cross-Sectional Study. Vaccines, 8(4), 661. https://doi.org/10.3390/vaccines8040661