Abstract
About 45:000 cancers are linked to HPV each year in the United States alone. The HPV vaccine prevents cancer and is highly effective, yet vaccination coverage remains low. Pharmacies can play a meaningful role in increasing HPV vaccination access due to their availability and convenience. However, little is known about pharmacists’ perceived barriers to HPV vaccination. The objective of this systematic review was to summarize existing literature on perceived barriers to administering HPV vaccination reported by pharmacists. Barriers identified from selected studies were synthesized and further grouped into patient, parental, (pharmacist’s) personal, and system/organization barrier groups. Six studies were included in this review. The cost of the HPV vaccine, insurance coverage and reimbursement were commonly reported perceived barriers. Adolescent HPV vaccination barriers related to parental concerns, beliefs, and inadequate knowledge about the HPV vaccine. Perceived (pharmacist’s) personal barriers were related to lack of information and knowledge about HPV vaccine and recommendations. At the system/organization level, barriers reported included lack of time/staff/space; difficulty in series completion; tracking and recall of patient; perceived competition with providers; and other responsibilities/vaccines taking precedence. Future strategies involving pharmacy settings in HPV-related cancer prevention efforts should consider research on multilevel pharmacy-driven interventions addressing barriers.
1. Introduction
Human Papillomavirus (HPV) is estimated to be the cause of 70% oropharynx, vaginal, and vulvar cancers, 60% of penile cancers, and 90% of anal and cervical cancers [1]. HPV-associated cancers are the only known cancers that can be prevented by receiving a vaccine. Yet, there are over 45,000 newly diagnosed HPV-related cancers in the United States each year [1]. The HPV vaccine has been shown to be safe and highly effective [2]. The Centers for Disease Control and Prevention (CDC) established HPV vaccination as a public health priority, yet vaccination coverage rates are less than the Healthy People 2020 goal that 80% of adolescents complete the vaccine series [3,4]. Nationally in 2017, less than 66% of adolescents received the first dose of the HPV vaccine, and only about 49% completed the series [5]. The HPV vaccine dosing schedule consists of a series of two or three doses, depending on the age of the patient at the start of the schedule [6]. For example, a patient that is under the age of 15 is recommended to receive two doses of the HPV vaccine administered 6–12 months apart. A patient starting the vaccine series on or after the 15th birthday is recommended to receive three doses of the HPV vaccine [6]. In this dosing schedule, the second vaccine should be administered 1–2 months after the first dose, and the third dose should be administered 6 months after the first dose [6].
Community pharmacies have the potential to play a meaningful role in increasing HPV vaccination rates. The President’s Cancer Panel [7] and National Vaccine Advisory Committee [8] released statements urging the increase in uptake of HPV vaccination rates by using pharmacies as a strategic site. Pharmacies are conveniently located for most families, including those in rural communities. In fact, most residents in the United States (91%) live within five miles of a pharmacy [9]. Additionally, pharmacies are typically open for extended hours and on weekends. Given the expanding scope of practice and evolving role of the pharmacist and pharmacy as playing a vital role in public health, due to their accessibility, cost-efficacy, and ability to provide education and shared responsibility, along with patient acceptance, they have been identified as crucial partners in vaccination administration [10].
During the ongoing COVID-19 pandemic, the U.S. Department of Health and Human Services (HHS) declared that pharmacists are allowed to administer childhood vaccines for children that are three years and above [11]. Most state laws also allow pharmacists to administer HPV vaccine to patients, with some states having varying age restrictions and/or prescription requirements (only two states do not allow pharmacists to administer the HPV vaccine at all) [12]. Pharmacists provide a convenient option for patients to receive the HPV vaccine. However, little is known about the current perceptions and barriers to administrating HPV vaccination among pharmacists. Therefore, this review aims to systematically examine the literature on pharmacists’ perceived barriers to administering the HPV vaccine as a mechanism for improving HPV vaccination uptake.
2. Methodology
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) [13].
2.1. Search Strategy
Electronic searches were created and completed by a research team member and health sciences librarian (A.W.) experienced with systematic searches in the following databases: PubMed [NLM], Web of Science [Thomson Reuters], Cochrane Central Register of Controlled Trials [Wiley], and Scopus [Elsevier]. The search strategy was created first in PubMed (Appendix A), and then translated for each database platform as applicable. MeSH terms and keywords were used to search concepts related to Human Papillomavirus, vaccines, barriers, and pharmacists. The searches were performed on 18 September 2020. Results were restricted to English language. There were no restrictions set on the year of publication for inclusion. Duplicate references were removed using Rayyan software [14]. The references cited in the included articles were reviewed for additional relevant articles.
2.2. Study Selection & Data Extraction
The titles and abstracts were first screened independently for eligibility by two researchers (S.G., O.O.). Then, the same researchers reviewed the full text of selected abstracts for further eligibility. Conflicts were resolved by a third researcher (J.M.M.). Study inclusion criteria include: (1) primary research article including qualitative, quantitative, and mixed-method studies, (2) reported outcome included perceived barrier to administering HPV vaccine (3) study population included pharmacists, pharmacy students, pharmacy technicians, and pharmacist representatives. Studies were excluded if the study objectives were unrelated to HPV vaccination. Two co-authors (O.O., J.M.M.) abstracted and synthesized all findings. Barrier type categorization was adapted from the findings reported in the included studies [15,16,17]. Some barriers extended, at least partially, across other barrier types. All barrier type classifications were discussed among co-authors, and a consensus was made for the final classification. Another co-author (S.M.C) reviewed the findings independently for accuracy. Any conflicts were resolved by deliberations among the co-authors.
3. Results
3.1. Literature Search and Study Characteristics
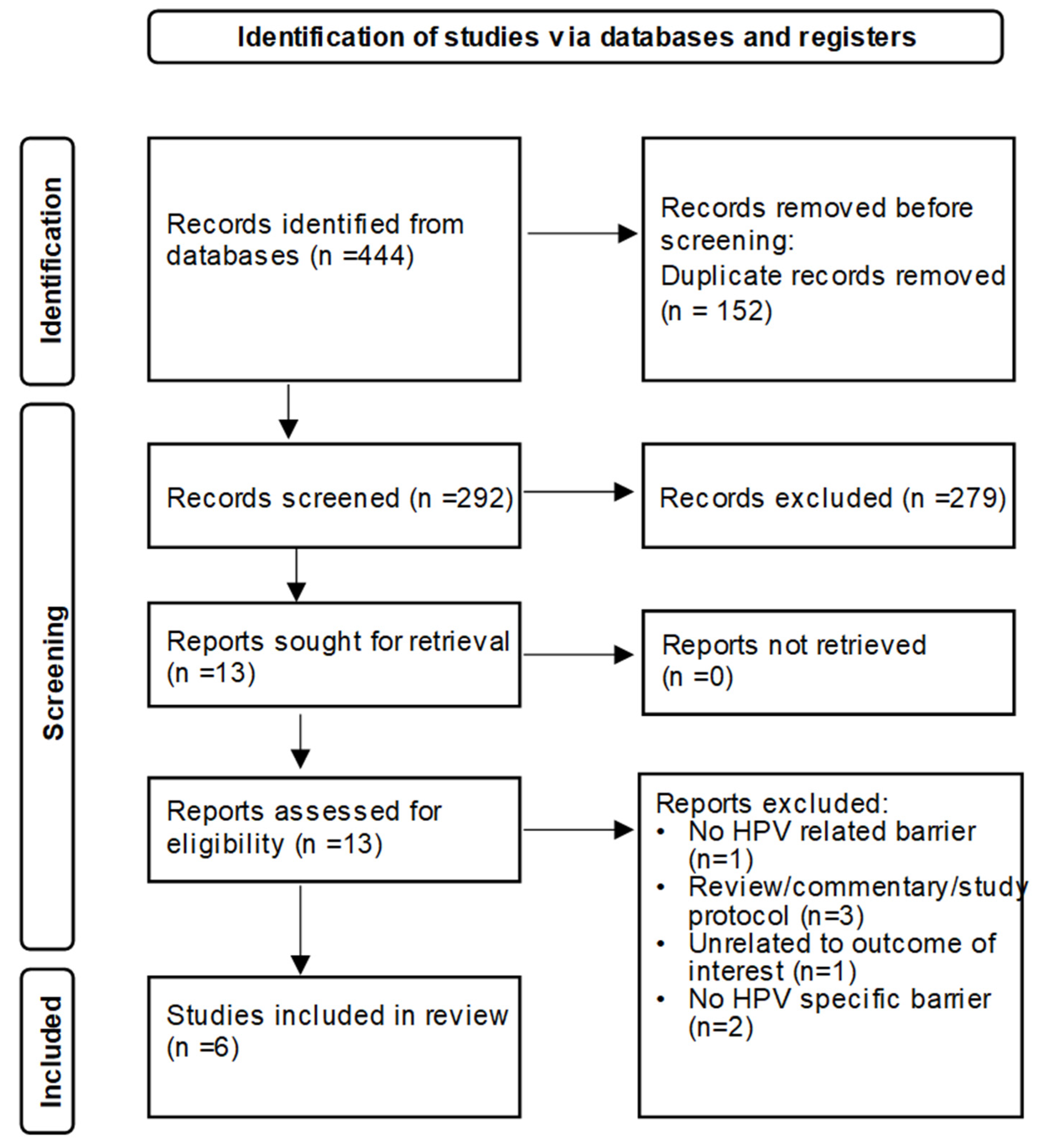
The electronic database searches yielded 444 articles; 292 titles and abstracts were selected, and 13 full-text studies were reviewed for inclusion. In the end, 6 out of 13 studies were selected for this review using the exclusion and inclusion criteria [15,16,17,18,19,20]. Figure 1 illustrates the PRISMA diagram detailing the search and selection process. Four of the studies [15,16,18,20] examined barriers related to HPV vaccine alone, while the remaining two studies [17,19] included other vaccines in addition to HPV. All included studies were carried out in the United States; however, geographical location and pharmacy setting differ across studies (Table 1). Table 2 presents an overview of the study designs, methodologies, and data reporting. While all the studies utilized a cross-sectional study design, the methodologies and results reporting varied widely across studies (Table 2). Table 3 presents a summary of the key findings for the included studies. These findings were further grouped by level of barrier into patient, parental, (pharmacist’s) personal, and system/organization barrier groups, which were adapted from the findings reported in the included studies (Table 4) [15,16,17]. Some barriers extended, at least partially, across other barrier types. For example, “financially-related” (or cost) barriers were reported across multiple barrier types [15,17,18,19,20]. To the patient a “financially-related” (or cost) barrier may be the out-of-pocket cost of the vaccine, which is distinct from the “financially-related” (or cost) barrier at the systems/organizational level, which may be more related to the financial burden of stocking the vaccine.
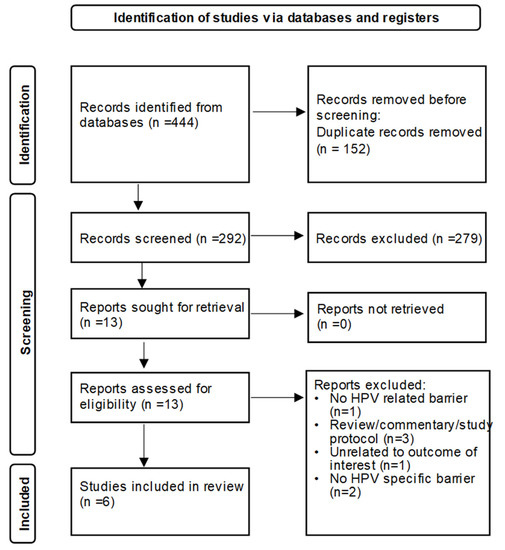
Figure 1.
PRISMA diagram showing search and selection.

Table 1.
Characteristics of included studies.
Table 2.
Overview of included study methodologies and data reporting.
Table 3.
Key findings of included studies.
Table 4.
Summary of key barriers grouped by level of barrier.
3.2. Barrier Levels
Patient: Four out of the six included studies reported patient-related barriers [15,16,17,19]. The most commonly reported barriers at the patient level were inadequate demand [15,16] and patient refusal [17]. Reasons for patient refusal reported in one of the studies included perceived safety concerns and financial reasons [17]. Other barriers included patients lacking insurance coverage [17] and difficulty overcoming financial barriers for an adolescent [19].
Parental: Three studies included parent-related barriers [15,18,20]. Across these studies, certain parental concerns and perceptions were reported as pharmacists perceived barriers to HPV vaccination. This included safety and efficacy concerns about the HPV vaccine [15], concerns that agreeing to vaccination means they are condoning premarital sex [15], and concerns that their children will engage in riskier sexual behaviors if they receive the vaccine [15]. Parental beliefs that their children are not at risk for HPV infection and that children are not old enough for the HPV vaccine were also reported as barriers [15]. Other key parent-related barriers reported include inadequate demand from parents [20], parental believe the cost is too high [15], perceived stigma about vaccination among parents of adolescents [18], parental consent [18], lack of knowledge [20], and inadequate education/understanding about HPV infection [15].
(Pharmacist’s) Personal: Three studies reported pharmacist’s personal barriers to HPV vaccination. [16,18,19]. In one of the studies, lack of information was reported as a barrier [16]. This included inadequate knowledge to educate and recommend the HPV vaccine and also a lack of information on subjects such as cost and storage of the vaccine [16]. Misinformation among pharmacists regarding HPV vaccination and administration was also reported as a barrier [16]. For instance, one pharmacist believed (incorrectly) that the HPV vaccination coverage in their (rural) area was good [16]. Another example of misinformation was evidenced by a pharmacist stating that Medicaid does not allow pharmacists to provide the HPV vaccine to those under 18, even with a prescription [16]. A third example of misinformation was evidenced by a pharmacist stating that adolescents are supposed to receive the HPV vaccine only at their doctor’s office [16]. The perception that HPV infection/mode of transmission is a sensitive subject was also cited as a barrier [16]. Other personal barriers include safety concerns about the potential adverse reaction after receiving the HPV vaccine [16,18], and the belief that the Advisory Committee on Immunization Practices (ACIP) recommendations are controversial [19].
System/Organization: Five out of the six studies reviewed reported system/organization level barriers [15,16,17,18,20]. Three of these studies reported lack of time and staffing as barriers to HPV vaccine administration [16,17,20]. For example, often times only one pharmacist may be present, which could result in major interruptions in work flow to stop and administer an HPV vaccine [16]. Two studies reported that a lack of physical space was also a barrier [16,20]. For example, a lack of consulting space to accommodate both parent and adolescent for HPV vaccine counseling and/or administration is a barrier [16]. Financial barriers related to vaccination cost, insurance reimbursement, and compensation were also frequently cited [15,17,18,20]; this included lack of insurance coverage of vaccine costs [15], difficulty in knowing whether insurance will reimburse for vaccine [17], and adequate compensation for vaccine purchase/supplies purchase/vaccine administration [17]. Other cost-related barriers included upfront cost of buying vaccine/supplies and lack of demand to justify cost of stocking vaccines [17].
At the organization level, other responsibilities/vaccines taking precedence over HPV vaccination was also reported as a barrier [17,20]. Other reported barriers were related to series completion which included lack of incentives for series completion [15,17], tracking and recall of patients [18], and remembering to screen patients for vaccine [17].
In one study, concerns that it may appear that pharmacists are in competition with health care providers to administer the vaccine was seen as a barrier [16]. Liability issues relating to adverse effects after vaccination [16], lack of educational materials to provide to parents [20]; and inadequate vaccine promotion/education were also reported as barriers [18].
4. Discussion
Community pharmacies could potentially play an important role in improving HPV vaccination rates due to their availability and accessibility. This review presents a summary of the literature on pharmacists’ perceived barriers to providing the HPV vaccine in a pharmacy setting. Based on the findings from the six included studies, pharmacists’ perceived barriers to HPV vaccination uptake exist at the patient, parental, pharmacist’s (personal), and system/organization levels. The existence of reported barriers at different levels suggests that efforts at improving HPV vaccination rates among pharmacies should be targeted at these levels.
Barriers related to the cost of the HPV vaccine and insurance coverage were frequently cited in the articles reviewed for this paper [15,17,18,19,20]. This is in concert with previous studies where vaccine cost and lack of insurance coverage have also been reported as specific barriers to HPV vaccination among health care providers [23,24]. Other studies have also reported that financial reasons may be a parental barrier for HPV vaccination for their children [25]. In fact, one study found that a lower proportion of parents were willing to vaccinate their children if the vaccine was not covered by insurance [25]. A number of options are available to cover the cost of HPV vaccine. Under the Affordable Care Act (ACA), most private insurance plans in the United States are required to cover immunizations recommended by ACIP without consumer cost-sharing [7]. Additionally, the Vaccine for Children (VFC) program is a federally funded program in the United States that covers vaccine costs for eligible children below 19 years of age (eligibility criteria include Medicaid-eligible, uninsured, underinsured, and American Indian or Alaska Native) [26]. A study among physicians reported that those participating in VFC program were less likely to indicate cost as a barrier to HPV vaccination [24,27]. Previous research showed that the VFC program led to increased vaccination for certain vaccines [28]. However, barriers such as state laws (only 34 states allow pharmacies to participate in VFC), inadequate reimbursement to cover actual costs, administrative burden and low demand from eligible persons may affect pharmacies’ participation in VFC or willingness to carry all vaccines [7,29]. Other sources that cover HPV vaccine cost in the United States include Merck assistance programs [30], Medicaid and Children’s Health Insurance Program (CHIP) [31]. Promotion and public education on these little or no-cost options for HPV vaccination could improve access.
Parents play an important role in HPV vaccination for their adolescent children. Results from this review showed that pharmacists perceived parental concerns, beliefs, and lack of knowledge as barriers to HPV vaccination [15,18,20]. Similar findings were reported from a study that examined perceived barriers to HPV vaccination among health care providers; the authors reported parental beliefs and misconceptions as a major barrier to HPV vaccination [32]. About one-third of parents in previous research reported that they were willing to allow their children to get the HPV vaccine in a pharmacy setting [33]. Likewise, another study showed that 44% of parents are willing to get an HPV vaccine from pharmacies for their children [34]. Improving parental awareness and clarity that pharmacists offer HPV vaccines for children may facilitate series completion [33]. Also, strategies to educate parents on the importance of the HPV vaccine and demystify misconceptions may positively influence parental decision to vaccinate their children. This may include additional training for pharmacists on ways to educate and provide effective HPV vaccine recommendations to parents [15].
Partnerships and collaboration agreements between health care providers and pharmacists, including strong provider recommendation and referral to pharmacies for subsequent HPV vaccine doses may increase parental awareness and vaccine uptake [33]. Physicians could help improve parental awareness as parents may prefer to learn about the availability of pharmacists to provide the HPV vaccination from their children’s physicians [33]. However, there is a lack of uniformity across states in the US and diverging opinions regarding authority to administer vaccines to children and adolescents that complicates the theoretical partnerships and collaboration agreements between health care providers and pharmacists. For instance, laws and regulations granting pharmacists the authority to administer HPV vaccine to all or certain adolescent age groups vary across states [12]. Also, there is a lack of consensus among professional organizations, like the American Academy of Pediatrics (AAP), and the US Department of Health and Human Services regarding whether pharmacists should be authorized to administer vaccines to children and adolescents [11,35]. In 2020, AAP released a statement that their organization believes that children should receive vaccines from a pediatrician, which opposes HHS authorization that allows pharmacists to administer childhood vaccines [36].
Three studies included in this review reported personal barriers among pharmacists to HPV vaccine administration [16,18,19]. The personal barriers were not religious or moral, but related primarily to inadequate knowledge to provide recommendations for HPV vaccination, or educate patients about the HPV vaccine (considering the sensitivity of HPV-related subject) [16,19]. This is promising as additional training on HPV vaccine recommendation strategies, coverage, and administration for practicing pharmacists, as well as student pharmacists, could help improve the pharmacists’ knowledge and comfort level in educating and administering the HPV vaccine [37].
At the organization level, remembering to screen [17] as well as tracking and recall of patients were identified as barriers to HPV vaccination [18]. In one of the studies reviewed, only 33 percent of participants reported that they utilized their state’s Immunization Information Systems (IIS) [18]. IIS can ensure timely immunization, clinical decision support, records consolidation, and data exchange among health care providers [38]. However, the operating and reporting for IIS requirements vary by state [39]. Another key organization level barrier reported was other responsibilities/vaccines taking precedence [17,20] over HPV vaccination and lack of time/staff/space [16,17,20]. The decision to prioritize and offer HPV vaccines by pharmacies may depend on the goals of the organization/management and may differ between independent versus chain pharmacies.
While the purpose of this review was to summarize existing literature related to the perceived barriers to administering HPV vaccination reported by pharmacists, some of the studies reported facilitators of HPV vaccination suggested by study participants [16,18,20]. Most frequently suggested facilitator was education about HPV vaccine [16,18,20]. As reported in one of the studies, education may involve providing education to patient/parent, pharmacists, and health care providers [20]. Another suggested way to improve HPV vaccination is advertising specifically through mass/social media [16,20]. Pharmacist providing stronger recommendation to patients about getting HPV vaccination was also reported as potential facilitator of HPV vaccination [20]. Partnership involving health care providers, schools [16,20] and public health organization [16] was reported as a facilitator. For instance, doctors may recommend that their patient get the HPV vaccine in a pharmacy or schools holding vaccine clinics [20]. Other facilitators reported by pharmacists include ease of accessibility of community pharmacies [16], clear guidelines from pharmacy/corporate management [18], vaccine promotion within and outside the pharmacy [18], adequate insurance coverage for vaccination [20], and state legislative authority to provide vaccination [18].
Evidence-based strategies to improve HPV vaccination rates that have previously been implemented in other settings, such as in primary care, may help to improve HPV vaccination in pharmacies. For instance, previous studies suggest that reminder and recall systems [40] and decision support systems [41] may be effective in improving HPV vaccination, which potentially could facilitate series completion. Alternatively, successful evidence-based strategies implemented in pharmacy settings to improve other vaccines could also be adapted to improving HPV vaccination rates. In one study, pharmacy-based interventions, including newspaper press releases, use of flyer advertisement, and personalized letters about herpes zoster infection and vaccination were shown to improve herpes zoster vaccination rates [42]. In another study, individuals who received a phone call intervention from pharmacists were more likely to receive their second dose of the recombinant zoster vaccine, thereby facilitating series completion [43]. Further research is needed to explore interventions unique and specific to improving HPV vaccination and series completion in pharmacies.
To our knowledge, this is the first study to review previously reported perceptions of barriers to HPV vaccine administration among pharmacists. Numerous commentaries and professional organizations suggest that pharmacies could play an important role in improving HPV vaccine uptake. The studies included in this review varied greatly in terms of study design, which made the synthesis of findings challenging. The search strategy employed to identify eligible studies for this review, encompassed publications on studies conducted worldwide. However, all the eligible studies included in this review were conducted in the United States. The perceived barriers that pharmacists experience may vary geographically within and outside of the United States. Therefore, generalizability of results may be limited. Nevertheless, many of these barriers are, to some extent, universal and therefore may provide direction for those investigating HPV vaccination barriers in different health care delivery systems. This literature search yielded only a few studies, which indicates that additional research is needed to explore pharmacist’s perceived barriers, especially at the system/organization levels. Because most of the studies included in this review relied primarily on quantitative survey-based data collection methods, it limits the ability to thoroughly understand pharmacists’ perceived barriers to HPV vaccine administration. A more comprehensive understanding of barriers to HPV vaccine administration is needed, especially to better understand how these barriers may impact various pharmacies in utilizing differing immunization delivery practices. Future work should include in-depth qualitative analyses of barriers among pharmacists practicing in a wide variety of settings.
In conclusion, pharmacies present an opportunity to increase HPV vaccination rates. Targeted public health efforts to increase HPV vaccination among pharmacies should consider a multilevel approach. Future strategies involving pharmacy settings in HPV-related cancer prevention efforts should consider research on pharmacy-driven interventions that addresses the barriers to administering the HPV vaccine at various levels.
Author Contributions
Conceptualization, J.M.M. and O.O.; methodology, A.Q.W., O.O. and J.M.M.; formal analysis, O.O., S.G. and J.M.M.; writing—original draft preparation, O.O., S.G. and A.Q.W.; writing—review and editing, J.M.M., S.M.C., J.D.G., N.B.Z. and L.C.K.; visualization, O.O.; supervision, J.M.M., L.C.K. and N.B.Z.; project administration, J.M.M.; funding acquisition, L.C.K., N.B.Z. and J.M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Tennessee Medical Center Cancer Institute Research Grant Awarded to L.C.K., N.B.Z., J.M.M.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Justin Gatwood reports vaccine-related research funding provided by Merck & Co. and GlaxoSmithKline.
Appendix A. PubMed Search Strategy
(Papillomavirus Infections[Mesh]) OR (HPV[tw] OR “human papilloma virus”[tw] or “human papillomavirus”[tw])
AND
(Immunization[Mesh] OR “Vaccination”[Mesh] OR “Immunization Programs”[Mesh] OR “Mass Vaccination”[Mesh] OR “Papillomavirus Vaccines”[Mesh]) OR (vaccin*[tw] OR immunization[tw])
AND
(Pharmacies[Mesh] OR “Pharmacy Technicians”[Mesh] OR “Pharmacy Residencies”[Mesh] OR “Students, Pharmacy”[Mesh] OR “Pharmacists”[Mesh] OR “Community Pharmacy Services”[Mesh]) OR (pharmac*[tw])
AND
barrier*[tw] OR challenge*[tw] OR constrain*[tw] OR difficult*[tw] OR interfer*[tw] OR obstruct*[tw] OR problem*[tw] OR restrain*[tw] OR restrict*[tw]
References
- Centers for Disease Control and Prevention. Cancers Associated with Human Papillomavirus, United States—2013–2017; USCS Data Brief; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/cancer/uscs/about/data-briefs/no18-hpv-assoc-cancers-UnitedStates-2013-2017.htm (accessed on 9 April 2021).
- Centers for Disease Control and Prevention. Human Papillomavirus (HPV): HPV Vaccination is Safe and Effective; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. Available online: https://www.cdc.gov/hpv/parents/vaccinesafety.html (accessed on 18 August 2021).
- Office of Disease Prevention and Health Promotion. Immunization and Infectious Diseases: IID-11.4 Increase the Percentage of Female Adolescents Aged 13 through 15 Years Who Receive 2 or 3 Doses of Human Papillomavirus (HPV) Vaccine as Recommended; Office of Disease Prevention and Health Promotion: Washington, DC, USA, 2020. Available online: https://www.healthypeople.gov/2020/data-search/Search-the-Data#objid=4657 (accessed on 25 April 2021).
- Office of Disease Prevention and Health Promotion. Immunization and Infectious Diseases: IID-11.5 Increase the Percentage of Male Adolescents Aged 13 through 15 Years Who Receive 2 or 3 Doses of Human Papillomavirus (HPV) Vaccine as Recommended; Office of Disease Prevention and Health Promotion: Washington, DC, USA, 2020. Available online: https://www.healthypeople.gov/2020/data-search/Search-the-Data#objid=10676 (accessed on 25 April 2021).
- Walker, T.Y.; Elam-Evans, L.D.; Yankey, D.; Markowitz, L.E.; Williams, C.L.; Mbaeyi, S.A.; Fredua, B.; Stokley, S. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Years-United States, 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 909–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Human Papillomavirus (HPV): HPV Vaccine Schedule and Dosing; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019. Available online: https://www.cdc.gov/hpv/hcp/schedules-recommendations.html (accessed on 18 August 2021).
- President’s Cancer Panel. HPV Vaccination for Cancer Prevention: Progress, Opportunities, and a Renewed Call to Action. A Report to the President of the United States from the Chair of the President’s Cancer Panel; President’s Cancer Panel: Bethesda, MD, USA, 2018. Available online: https://prescancerpanel.cancer.gov/report/hpvupdate/pdf/PresCancerPanel_HPVUpdate_Nov2018.pdf (accessed on 9 April 2021).
- National Vaccine Advisory Committee. Overcoming Barriers to Low HPV Vaccine Uptake in the United States: Recommendations from the National Vaccine Advisory Committee: Approved by the National Vaccine Advisory Committee on 9 June 2015. Public Health Rep. 2016, 131, 17–25. [Google Scholar] [CrossRef] [Green Version]
- National Association of Chain Drug Stores (NACDS). Face-to-Face with Community Pharmacies. Available online: https://www.nacds.org/pdfs/about/rximpact-leavebehind.pdf (accessed on 26 July 2021).
- Shen, A.K.; Peterson, A. The pharmacist and pharmacy have evolved to become more than the corner drugstore: A win for vaccinations and public health. Hum. Vaccines Immunother. 2020, 16, 1178–1180. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. HHS Expands Access to Childhood Vaccines during COVID-19 Pandemic. 2020. Available online: https://www.hhs.gov/about/news/2020/08/19/hhs-expands-access-childhood-vaccines-during-covid-19-pandemic.html (accessed on 19 April 2021).
- National Alliance of State Pharmacy Associations. Pharmacist Immunization Authority. 2020. Available online: https://naspa.us/resource/pharmacist-authority-to-immunize/ (accessed on 19 April 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hastings, T.J.; Hohmann, L.A.; McFarland, S.J.; Teeter, B.S.; Westrick, S.C. Pharmacists’ attitudes and perceived barriers to Human Papillomavirus (HPV) vaccination services. Pharmacy 2017, 5, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, G. Exploring opportunities to leverage pharmacists in rural areas to promote administration of Human Papillomavirus vaccine. Prev. Chronic Dis. 2020, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berce, P.C.; Bernstein, R.S.; MacKinnon, G.E.; Sorum, S.; Martin, E.; MacKinnon, K.J.; Rein, L.E.; Schellhase, K.G. Immunizations at Wisconsin Pharmacies: Results of a statewide vaccine registry analysis and pharmacist survey. Vaccine 2020, 38, 4448–4456. [Google Scholar] [CrossRef]
- Islam, J.Y.; Gruber, J.F.; Kepka, D.; Kunwar, M.; Smith, S.B.; Rothholz, M.C.; Brewer, N.T.; Smith, J.S. Pharmacist insights into adolescent Human Papillomavirus vaccination provision in the United States. Hum. Vaccines Immunother. 2019, 15, 1839–1850. [Google Scholar] [CrossRef] [PubMed]
- Skiles, M.P.; Cai, J.; English, A.; Ford, C.A. Retail pharmacies and adolescent vaccination—An exploration of current issues. J. Adolesc. Health 2011, 48, 630–632. [Google Scholar] [CrossRef]
- Tolentino, V.; Unni, E.; Montuoro, J.; Bezzant-Ogborn, D.; Kepka, D. Utah pharmacists’ knowledge, attitudes, and barriers regarding Human Papillomavirus vaccine recommendation. J. Am. Pharm. Assoc. 2018, 58, S16–S23. [Google Scholar] [CrossRef]
- Hurley, L.P.; Bridges, C.B.; Harpaz, R.; Allison, M.A.; O’Leary, S.T.; Crane, L.A.; Brtnikova, M.; Stokley, S.; Beaty, B.L.; Jimenez-Zambrano, A.; et al. US physicians’ perspective of adult vaccine delivery. Ann. Intern. Med. 2014, 160, 161–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dillman, D.A. Mail and Internet Surveys: The Tailored Design Method; Wiley & Sons: New York, NY, USA, 1999. [Google Scholar]
- Holman, D.M.; Benard, V.; Roland, K.B.; Watson, M.; Liddon, N.; Stokley, S. Barriers to Human Papillomavirus vaccination among US adolescents: A systematic review of the literature. JAMA Pediatrics 2014, 168, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCave, E.L. Influential factors in HPV vaccination uptake among providers in four states. J. Community Health 2010, 35, 645–652. [Google Scholar] [CrossRef]
- Barnack, J.L.; Reddy, D.M.; Swain, C. Predictors of Parents’ Willingness to Vaccinate for Human Papillomavirus and Physicians’ Intentions to Recommend the Vaccine. Women’s Health Issues 2010, 20, 28–34. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Vaccine For Children (VFC) Program. 2016. Available online: https://www.cdc.gov/vaccines/programs/vfc/about/index.html (accessed on 18 August 2021).
- Malo, T.L.; Hassani, D.; Staras, S.A.; Shenkman, E.A.; Giuliano, A.R.; Vadaparampil, S.T. Do Florida Medicaid providers’ barriers to HPV vaccination vary based on VFC program participation? Matern. Child Health J. 2013, 17, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Walsh, B.; Doherty, E.; O’Neill, C. Since the start of the vaccines for children program, uptake has increased, and most disparities have decreased. Health Aff. 2016, 35, 356–364. [Google Scholar] [CrossRef] [Green Version]
- Dullea, E.; Knock, K. Successes and Barriers to Pharmacists’ Participation in the Vaccines for Children (VFC) Program in the US. Immunize Colorado. 2020. Available online: https://teamvaccine.com/2020/08/04/successes-and-barriers-to-pharmacists-participation-in-the-vaccines-for-children-vfc-program-in-the-u-s/ (accessed on 20 April 2021).
- Merck Helps. Gardasil 9. Available online: https://www.merckhelps.com/GARDASIL%209 (accessed on 18 August 2021).
- The Henry J. Kaiser Family Foundation. The HPV Vaccine: Access and Use in the U.S. 2018. Available online: https://files.kff.org/attachment/fact-sheet-the-hpv-vaccine-access-and-use-in-the-u-s (accessed on 18 August 2021).
- Javanbakht, M.; Stahlman, S.; Walker, S.; Gottlieb, S.; Markowitz, L.; Liddon, N.; Plant, A.; Guerry, S. Provider perceptions of barriers and facilitators of HPV vaccination in a high-risk community. Vaccine 2012, 30, 4511–4516. [Google Scholar] [CrossRef]
- Calo, W.A.; Gilkey, M.B.; Shah, P.; Marciniak, M.W.; Brewer, N.T. Parents’ willingness to get Human Papillomavirus vaccination for their adolescent children at a pharmacy. Prev. Med. 2017, 99, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.D.; Calo, W.A.; Marciniak, M.W.; Golin, C.E.; Sleath, B.L.; Brewer, N.T. Service quality and parents’ willingness to get adolescents HPV vaccine from pharmacists. Prev. Med. 2018, 109, 106–112. [Google Scholar] [CrossRef]
- American Academy of Paediatrics. AAP: HHS Action on Pharmacy Vaccination ‘Misguided’. 2020. Available online: https://www.aappublications.org/news/2020/08/19/immunization081920 (accessed on 26 April 2021).
- American Academy of Paediatrics. American Academy of Pediatrics Opposes HHS Action on Childhood Vaccines; Calls It ‘Incredibly Misguided’. 2020. Available online: https://services.aap.org/en/news-room/news-releases/aap/2020/american-academy-of-pediatrics-opposes-hhs-action-on-childhood-vaccines-calls-it-incredibly-misguided/ (accessed on 26 April 2021).
- Omecene, N.E.; Patterson, J.A.; Bucheit, J.D.; Andersot, A.N.; Rogers, D.; Goode, J.V.; Caldas, L.M. Implementation of pharmacist-administered pediatric vaccines in the United States: Major barriers and potential solutions for the outpatient setting. Pharm. Pract. 2019, 17. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Immunization Information Systems. 2019. Available online: https://www.cdc.gov/vaccines/programs/iis/about.html (accessed on 18 August 2021).
- Martin, D.W.; Lowery, N.E.; Brand, B.; Gold, R.; Horlick, G. Immunization information systems: A decade of progress in law and policy. J. Public Health Manag. Pract. 2015, 21, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rand, C.M.; Brill, H.; Albertin, C.; Humiston, S.G.; Schaffer, S.; Shone, L.P.; Blumkin, A.K.; Szilagyi, P.G. Effectiveness of centralized text message reminders on Human Papillomavirus immunization coverage for publicly insured adolescents. J. Adolesc. Health 2015, 56, S17–S20. [Google Scholar] [CrossRef] [PubMed]
- Fiks, A.G.; Grundmeier, R.W.; Mayne, S.; Song, L.; Feemster, K.; Karavite, D.; Hughes, C.C.; Massey, J.; Keren, R.; Bell, L.M.; et al. Effectiveness of decision support for families, clinicians, or both on HPV vaccine receipt. Pediatrics 2013, 131, 1114–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Ford, L.J.; Uroza, S.F.; Jaber, N.; Smith, C.T.; Randolph, R.; Lane, S.; Foster, S.L. Effect of pharmacist intervention on herpes zoster vaccination in community pharmacies. J. Am. Pharm. Assoc. 2013, 53, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Tyler, R.; Kile, S.; Strain, O.; Kennedy, C.A.; Foster, K.T. Impact of pharmacist intervention on completion of recombinant zoster vaccine series in a community pharmacy. J. Am. Pharm. Assoc. 2021, 61, S12–S16. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).