
Behavioral, Emotional and Social Apathy in Alcohol-Related Cognitive Disorders

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Self-Reported Apathy | Total Sample | AUD | ARCI | KS | ||||
| (N = 71) | (N = 21) | (N = 25) | (N = 25) | |||||
| Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | |
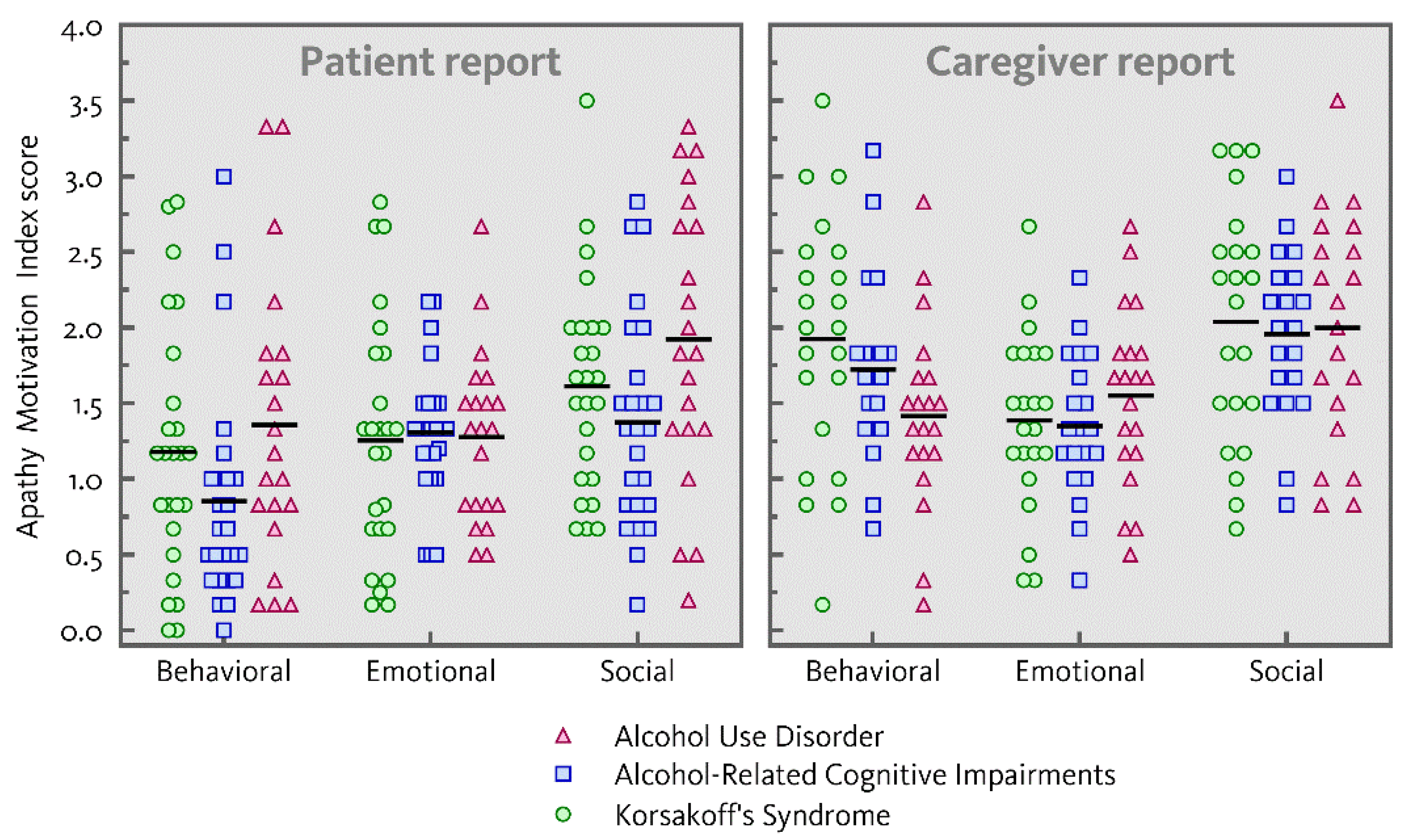
| Behavioral apathy | 1.12 (0.85) | 6.7 (5.0) | 1.36 (0.94) | 8.1 (5.7) | 0.85 (0.73) | 5.1 (4.4) | 1.18 (0.83) | 7.0 (4.8) |
| Emotional apathy | 1.28 (0.61) | 7.6 (3.7) | 1.28 (0.56) | 7.7 (3.4) | 1.31 (0.44) | 7.8 (2.7) | 1.26 (0.79) | 7.5 (4.8) |
| Social apathy | 1.62 (0.80) | 9.7 (4.8) | 1.92 (0.94) | 11.5 (5.6) | 1.37 (0.71) | 8.2 (4.2) | 1.61 (0.70) | 9.7 (4.2) |
| Caregiver-Reported Apathy | Total | AUD | ARCI | KS | ||||
| (N = 62) | (N = 20) | (N = 20) | (N = 22) | |||||
| Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | Mean (SD) | Total (SD) | |
| Behavioral apathy | 1.70 (0.71) | 10.2 (4.3) | 1.42 (0.62) | 8.5 (3.7) | 1.73 (0.60) | 10.4 (3.6) | 1.92 (0.82) | 11.5 (4.9) |
| Emotional apathy | 1.43 (0.55) | 8.6 (3.3) | 1.55 (0.59) | 9.3 (3.5) | 1.35 (0.48) | 8.1 (2.9) | 1.39 (0.58) | 8.3 (3.5) |
| Social apathy | 2.00 (0.70) | 12.0 (4.2) | 2.00 (0.76) | 12.0 (4.6) | 1.96 (0.54) | 11.8 (3.3) | 2.04 (0.79) | 12.2 (4.7) |
| AMI Subscale | Mean (SD) | Proposed Cut-Off Scores | |
|---|---|---|---|
| Moderate | Severe | ||
| Behavioral Activation | 1.58 (0.76) | ≥2.34 | ≥3.10 |
| Emotional Sensitivity | 1.05 (0.63) | ≥1.68 | ≥2.31 |
| Social Motivation | 1.69 (0.74) | ≥2.43 | ≥3.17 |
References
- Crews, F.T.; Buckley, T.; Dodd, P.R.; Ende, G.; Foley, N.; Harper, C.; He, J.; Innes, D.; Loh, E.W.; Pfefferbaum, A.; et al. Alcoholic neurobiology: Changes in dependence and recovery. Alcohol Clin. Exp. Res. 2005, 29, 1504–1513. [Google Scholar] [CrossRef] [PubMed]
- Harper, C. The neuropathology of alcohol-related brain damage. Alcohol Alcohol. 2009, 44, 136–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oscar-Berman, M.; Maleki, N. Alcohol dementia, Wernicke’s encephalopathy, and Korsakoff’s syndrome. In The Oxford Handbook of Adult Cognitive Disorders; Alosco, M.L., Stern, R.A., Eds.; Oxford University Press: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Walvoort, S.J.W.; Wester, A.J.; Egger, J.I.M. Neuropsychologische diagnostiek en cognitieve functies bij alcoholabstinentie [Neuropsychological assessment of cognitive functions and alcohol abstinence]. Tijdschr. Psychiatry 2013, 55, 101–111. [Google Scholar]
- Arts, N.J.M.; Walvoort, S.J.W.; Kessels, R.P.C. Korsakoff’s syndrome: A critical review. Neuropsychiatry Dis. Treat. 2017, 13, 2875–2890. [Google Scholar] [CrossRef] [Green Version]
- Marin, R.S. Apathy: A neuropsychiatric syndrome. J. Neuropsychiatry Clin. Neurosci. 1991, 3, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Starkstein, S.E.; Petracca, G.; Chemerinski, E.; Kremer, J. Syndromic validity of apathy in Alzheimer’s disease. Am. J. Psychiatry 2001, 158, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Ang, Y.S.; Lockwood, P.; Apps, M.A.; Muhammed, K.; Husain, M. Distinct subtypes of apathy revealed by the Apathy Motivation Index. PLoS ONE 2017, 12, e0169938. [Google Scholar] [CrossRef] [Green Version]
- Sockeel, P.; Dujardin, K.; Devos, D.; Deneve, C.; Destee, A.; Defebvre, L. The Lille apathy rating scale (LARS), a new instrument for detecting and quantifying apathy: Validation in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2006, 77, 579–584. [Google Scholar] [CrossRef] [Green Version]
- Robert, P.; Lanctôt, K.; Agüera-Ortiz, L.; Aalten, P.; Bremond, F.; Defrancesco, M.; Hanon, C.; David, R.; Dubois, B.; Dujardin, K.; et al. Is it time to revise the diagnostic criteria for apathy in brain disorders? The 2018 international consensus group. Eur. Psychiatry 2018, 54, 71–76. [Google Scholar] [CrossRef]
- Le Heron, C.; Holroyd, C.B.; Salamone, J.; Husain, M. Brain mechanisms underlying apathy. J. Neurol. Neurosurg. Psychiatry 2019, 90, 302–312. [Google Scholar] [CrossRef] [Green Version]
- Verdejo-Garcia, A.; Bechara, A.; Recknor, E.C.; Perez-Garcia, M. Executive dysfunction in substance dependent individuals during drug use and abstinence: An examination of the behavioral, cognitive and emotional correlates of addiction. J. Int. Neuropsychol. Soc. 2006, 12, 405–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, K.; Yang, Q.; Niu, Y.; Fan, F.; Chen, S.; Luo, X.; Tan, S.; Wang, Z.; Tong, J.; Yang, F.; et al. Cortical thickness in alcohol dependent patients with apathy. Front. Psychiatry 2020, 11, 364. [Google Scholar] [CrossRef]
- Gerridzen, I.J.; Moerman-Van den Brink, W.G.; Depla, M.F.; Verschuur, E.M.; Veenhuizen, R.B.; Van der Wouden, J.C.; Hertogh, C.M.; Joling, K.J. Prevalence and severity of behavioural symptoms in patients with Korsakoff syndrome and other alcohol-related cognitive disorders: A systematic review. Int. J. Geriatr. Psychiatry 2017, 32, 256–273. [Google Scholar] [CrossRef] [PubMed]
- Rensen, Y.C.M.; Egger, J.I.M.; Westhoff, J.; Walvoort, S.J.W.; Kessels, R.P.C. The effect of errorless learning on psychotic and affective symptoms, as well as aggression and apathy in patients with Korsakoff’s syndrome in long-term care facilities. Int. Psychoger. 2019, 31, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.P.C.; Moerman-van den Brink, W.G.; Rensen, Y.C.M.; Van Aken, L.; Walvoort, S.J.W.; Egger, J.I.M. The relation between behavioural, emotional and cognitive apathy and executive dysfunction in alcoholic Korsakoff’s syndrome. Arch. Clin. Psychiatry 2021, in press. [Google Scholar]
- Oey, M.J.; Brouwer, V.H.E.W.; Buijs, M.J.; Wijnia, J.W.; Postma, A.; Oudman, E. Unraveling apathy in Korsakoff syndrome patients receiving long-term care with and without cerebrovascular comorbidity. Alcohol. Clin. Exp. Res. 2021, 45, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Gerridzen, I.J.; Joling, K.J.; Depla, M.F.; Veenhuizen, R.B.; Verschuur, E.M.L.; Twisk, J.W.R.; Hertogh, C. Awareness and its relationships with neuropsychiatric symptoms in people with Korsakoff syndrome or other alcohol-related cognitive disorders living in specialized nursing homes. Int. J. Geriatr. Psychiatry 2019, 34, 836–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walvoort, S.J.; van der Heijden, P.T.; Wester, A.J.; Kessels, R.P.; Egger, J.I. Self-awareness of cognitive dysfunction: Self-reported complaints and cognitive performance in patients with alcohol-induced mild or major neurocognitive disorder. Psychiatry Res. 2016, 245, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Oslin, D.; Atkinson, R.M.; Smith, D.; Hendrie, H. Alcohol related dementia: Proposed clinical criteria. Int. J. Geriatr. Psychiatry 1998, 13, 203–212. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Disorders, 5th ed.; American Psychiatric Association: Washinton, DC, USA, 2013. [Google Scholar]
- Kopelman, M.D.; Thomson, A.D.; Guerrini, I.; Marshall, E.J. The Korsakoff syndrome: Clinical aspects, psychology and treatment. Alcohol Alcohol. 2009, 44, 148–154. [Google Scholar] [CrossRef]
- Arts, N.J.M.; Pitel, A.L.; Kessels, R.P.C. The contribution of mammillary body damage to Wernicke’s encephalopathy and Korsakoff’s syndrome. In Handbook of Clinical Neurology, (3rd Series): The Human Hypothalamus: Middle and Posterior Regions; Swaab, D.F., Kreier, F., Lucassen, P.J., Salehi, A., Buijs, R.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2021; Volume 180. [Google Scholar] [CrossRef]
- Schmand, B.; Lindeboom, J.; Van Harskamp, F. De Nederlandse Leestest Voor Volwassenen Handleiding [The Dutch National Adult Reading Test. Manual]; Pearson: Amsterdam, The Netherlands, 1992. [Google Scholar]
- Wechsler, D. WAIS-IV-NL Nederlandse Bewerking, Technische Handleiding [The Dutch-Language Version of the WAIS-IV: Administration and Scoring Manual]; Pearson: Amsterdam, The Netherlands, 2012. [Google Scholar]
- Haalboom, R.; Van Aken, L.; Walvoort, S.J.W.; Egger, J.I.M.; Kessels, R.P.C. Preserved intellectual functioning in Korsakoff’s syndrome? Actual and premorbid intelligence in patients with major or mild alcohol-related cognitive disorder. J. Subst. Use 2019, 24, 532–538. [Google Scholar] [CrossRef]
- Klar, V.S.; Ang, Y.S.; Lockwood, P.L.; Attaallah, B.; Dickson, S.; Drew, D.; Kienast, A.; Maio, M.R.; Plant, O.; Slavkova, E.; et al. Validity of a brief assessment of apathy: Caregiver version of the Apathy Motivation Index: Neuropsychiatry and behavioral neurology/assessment/measurement of neuropsychiatric/behavioral and psychological symptoms. Alzheimers Dement. 2020, 16. [Google Scholar] [CrossRef]
- Ang, Y.S.; Lockwood, P.L.; Kienast, A.; Plant, O.; Drew, D.; Slavkova, E.; Tamm, M.; Husain, M. Differential impact of behavioral, social and emotional apathy on Parkinson’s disease. Ann. Clin. Transl. Neurol. 2018, 5, 1286–1291. [Google Scholar] [CrossRef] [PubMed]
- Bruijnen, C.J.W.H.; Dijkstra, B.A.G.; Walvoort, S.J.W.; Budy, M.J.J.; Beurmanjer, H.; de Jong, C.A.J.; Kessels, R.P.C. Psychometric properties of the Montreal Cognitive Assessment (MoCA) in healthy participants aged 18–70. Int. J. Psychiatry Clin. Pract. 2020, 24, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Kolakowsky-Hayner, S. The Patient Competency Rating Scale. The Center for Outcome Measurement in Brain Injury. 2010. Available online: http://www.tbims.org/combi/pcrs (accessed on 19 May 2021).
- Hellebrekers, D.; Winkens, I.; Kruiper, S.; Van Heugten, C. Psychometric properties of the awareness questionnaire, patient competency rating scale and Dysexecutive Questionnaire in patients with acquired brain injury. Brain Inj. 2017, 31, 1469–1478. [Google Scholar] [CrossRef]
- Kirschner, M.; Rabinowitz, A.; Singer, N.; Dagher, A. From apathy to addiction: Insights from neurology and psychiatry. Prog. Neuropsychopharmacol. Biol. Psychiatry 2020, 101. [Google Scholar] [CrossRef]
- Lansdall, C.J.; Coyle-Gilchrist, I.T.S.; Jones, P.S.; Vázquez Rodríguez, P.; Wilcox, A.; Wehmann, E.; Dick, K.M.; Robbins, T.W.; Rowe, J.B. Apathy and impulsivity in frontotemporal lobar degeneration syndromes. Brain 2017, 140, 1792–1807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drew, D.S.; Muhammed, K.; Baig, F.; Kelly, M.; Saleh, Y.; Sarangmat, N.; Okai, D.; Hu, M.; Manohar, S.; Husain, M. Dopamine and reward hypersensitivity in Parkinson’s disease with impulse control disorder. Brain 2020, 143, 2502–2518. [Google Scholar] [CrossRef]
- Winhusen, T.M.; Somoza, E.C.; Lewis, D.F.; Kropp, F.B.; Horigan, V.E.; Adinoff, B. Frontal systems deficits in stimulant-dependent patients: Evidence of pre-illness dysfunction and relationship to treatment response. Drug Alcohol Depend. 2013, 127, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M.A.; Iudicello, J.E.; Morgan, E.E.; Kamat, R.; Heaton, R.K.; Grant, I.; TMARC Group. Apathy is associated with poorer abstinence self-efficacy in individuals with methamphetamine dependence. Addict. Behav. Rep. 2021, 13. [Google Scholar] [CrossRef]


| Characteristic | AUD | ARCI | KS | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| (N = 23) | (N = 25) | (N = 25) | ||||||
| N | Mean (SD) | Range | Mean (SD) | Range | Mean (SD) | Range | ||
| Age (years) | 73 | 56.7 (9.3) | 40–72 | 58.6 (8.3) | 40–75 | 61.5 (6.7) | 46–77 | 0.122 |
| Sex distribution (men/women) | 73 | 20/3 | 23/2 | 17/8 | 0.066 | |||
| Abstinence duration (days) 1 | 73 | 48 | 38–171 | 51 | 39–1096 | 152 | 39–6992 | 0.002 7 |
| NART IQ 2 | 60 | 88.5 (14.5) | 70–118 | 90.6 (14.1) | 60–116 | 94.7 (16.1) | 58–125 | 0.421 |
| Full-scale WAIS-IV IQ 3 | 62 | 87.4 (15.2) | 59–115 | 82.3 (12.1) | 55–97 | 80.5 (13.5) | 63–108 | 0.242 |
| Educational level 4 | 73 | 4 (5) | 1–6 | 5 (5) | 2–7 | 5 (5) | 2–7 | 0.321 |
| MoCA 5 Total score | 63 | 24.9 (3.3) | 18–30 | 22.5 (2.9) | 16–26 | 18.5 (3.9) | 12–24 | <0.001 8 |
| MoCA Memory Index Score | 63 | 11.8 (3.3) | 4–15 | 10.3 (3.0) | 4–15 | 6.1 (2.3) | 2–10 | <0.001 8 |
| PCRS 6 Total Score | 70 | 105.4 (10.2) | 84–130 | 101.1 (11.9) | 70–120 | 83.1 (21.6) | 45–114 | <0.001 9 |
| Patient-Reported Apathy (N = 69) | PCRS Total Score | MoCA Total Score |
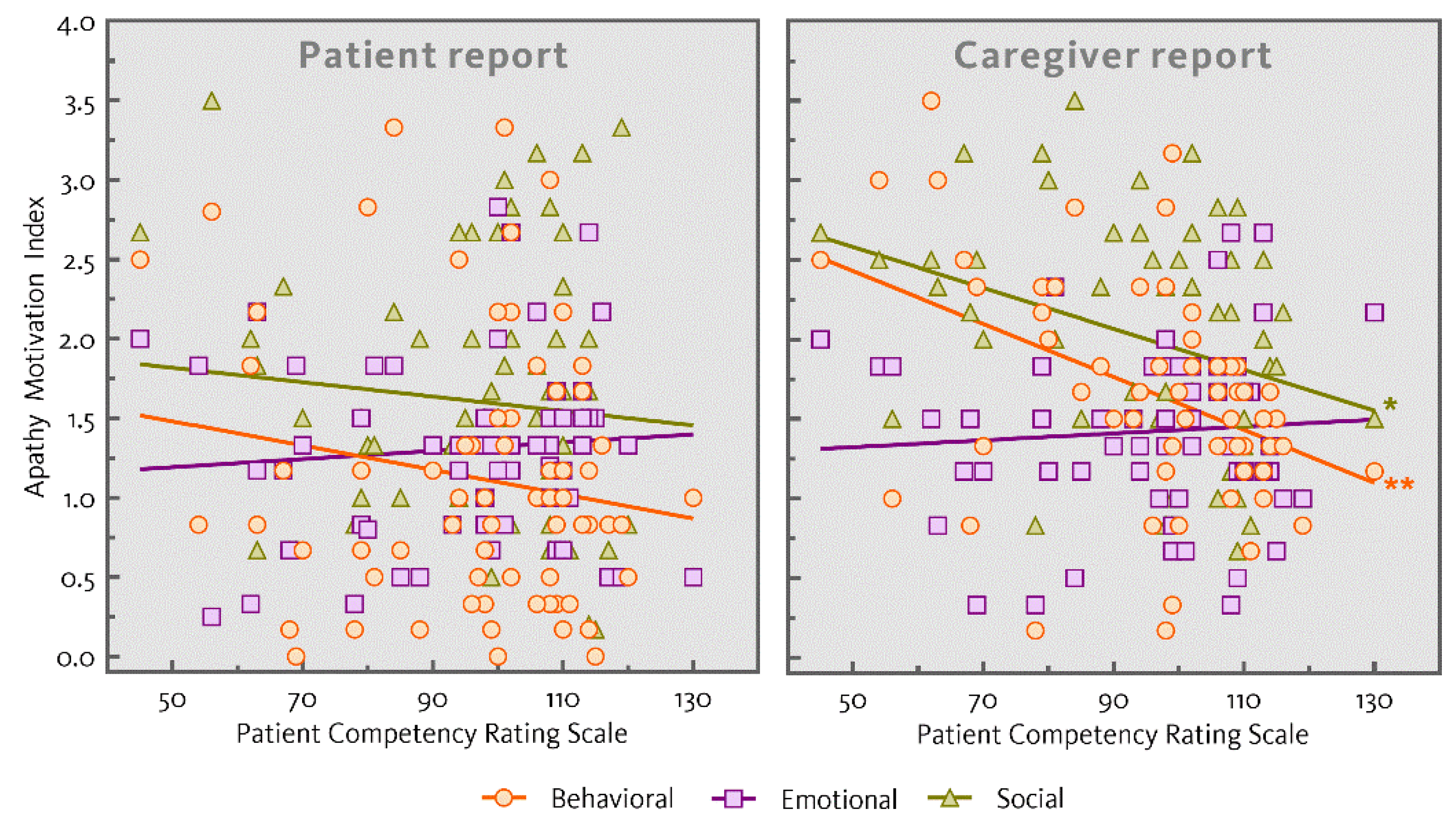
| Behavioral apathy | −0.161 | 0.066 |
| Emotional apathy | 0.079 | −0.063 |
| Social apathy | −0.102 | 0.188 |
| Caregiver-Reported Apathy (N = 59) | PCRS Total Score | MoCA Total Score |
| Behavioral apathy | −0.422 ** | −0.119 |
| Emotional apathy | 0.069 | 0.167 |
| Social apathy | −0.330 * | −0.179 |
| Level of Apathy | AUD | ARCI | KS | |||
|---|---|---|---|---|---|---|
| (N = 18) | (N = 20) | (N = 22) | ||||
| Patient-Reported | Informant-Reported | Patient-Reported | Informant-Reported | Patient-Reported | Informant-Reported | |
| Behavioral apathy | 1.44 (0.97) | 1.34 (0.60) | 0.74 (0.54) | 1.73 (0.60) | 1.18 (0.88) | 1.92 (0.82) |
| Emotional apathy | 1.28 (0.60) | 1.56 (0.61) | 1.30 (0.45) | 1.35 (0.48) | 1.21 (0.82) | 1.39 (0.58) |
| Social apathy | 1.98 (0.91) | 1.96 (0.79) | 1.36 (0.66) | 1.96 (0.54) | 1.64 (0.71) | 2.04 (0.79) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Dorst, M.E.G.; Rensen, Y.C.M.; Husain, M.; Kessels, R.P.C. Behavioral, Emotional and Social Apathy in Alcohol-Related Cognitive Disorders. J. Clin. Med. 2021, 10, 2447. https://doi.org/10.3390/jcm10112447
van Dorst MEG, Rensen YCM, Husain M, Kessels RPC. Behavioral, Emotional and Social Apathy in Alcohol-Related Cognitive Disorders. Journal of Clinical Medicine. 2021; 10(11):2447. https://doi.org/10.3390/jcm10112447
Chicago/Turabian Stylevan Dorst, Maud E. G., Yvonne C. M. Rensen, Masud Husain, and Roy P. C. Kessels. 2021. "Behavioral, Emotional and Social Apathy in Alcohol-Related Cognitive Disorders" Journal of Clinical Medicine 10, no. 11: 2447. https://doi.org/10.3390/jcm10112447
APA Stylevan Dorst, M. E. G., Rensen, Y. C. M., Husain, M., & Kessels, R. P. C. (2021). Behavioral, Emotional and Social Apathy in Alcohol-Related Cognitive Disorders. Journal of Clinical Medicine, 10(11), 2447. https://doi.org/10.3390/jcm10112447