
Decrease in Incidence Rate of Hospitalizations Due to AIDS-Defining Conditions but Not to Non-AIDS Conditions in PLWHIV on cART in 2008–2018 in Italy



 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Baseline Patients’ Characteristics
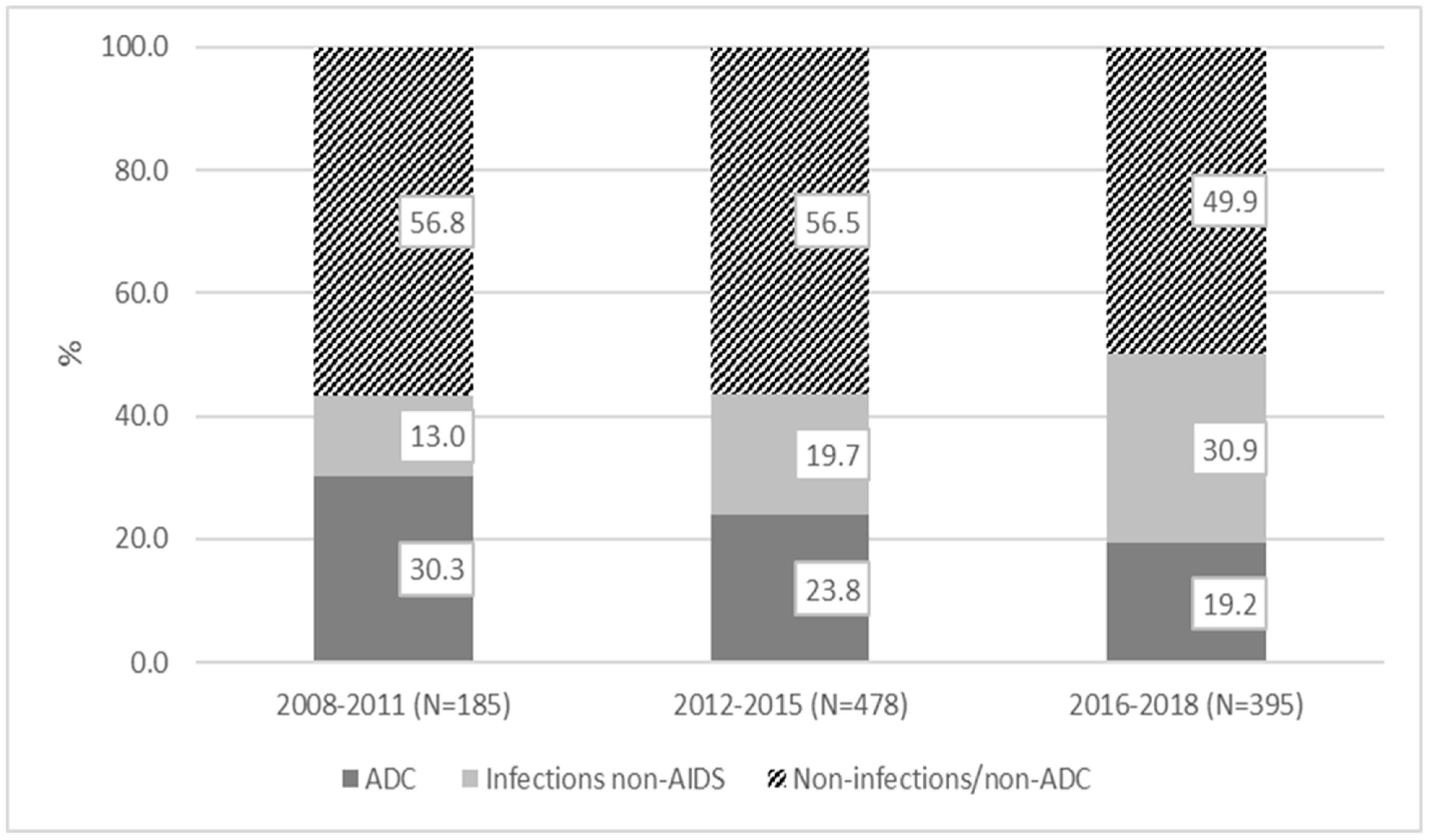
3.2. Hospitalizations: Rates, Reasons
3.3. Factors Associated with Hospitalizations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Palella, F.J., Jr.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV outpatient study investigators. N. Engl. J. Med. 1998, 338, 853–860. [Google Scholar] [CrossRef]
- Lazar, R.; Kersanske, L.; Xia, Q.; Daskalakis, D.; Braunstein, S.L. Hospitalization Rates among People With HIV/AIDS in New York City, 2013. Clin. Infect. Dis. 2017, 65, 469–476. [Google Scholar] [CrossRef]
- Lakoh, S.; Jiba, D.F.; Kanu, J.E.; Poveda, E.; Salgado-Berreira, A.; Sahr, F.; Sesay, M.; Deen, G.F.; Sesay, T.; Gashau, W.; et al. Causes of hospitalization and predictors of HIV-associated mortality at the main referral hospital in Sierra Leone: A prospective study. BMC Public Health 2019, 19, 1320. [Google Scholar] [CrossRef] [Green Version]
- Notiziario dell’Istituto Superiore di sanità. Available online: http://www.salute.gov.it/imgs/C_17_notizie_3963_0_file.pdf (accessed on 19 October 2019).
- INSIGHT START Study Group; Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fätkenheuer, G.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar]
- Bellino, S.; Borghetti, A.; Lombardi, F.; Camoni, L.; Ciccullo, A.; Baldin, G.; Belmonti, S.; Moschese, D.; LaMonica, S.; Cauda, R.; et al. Trends of hospitalisations rates in a cohort of HIV-infected persons followed in an Italian hospital from 1998 to 2016. Epidemiol. Infect. 2019, 147, e89. [Google Scholar] [CrossRef] [Green Version]
- Seng, R.; Mutuon, P.; Riou, J.; Duvivier, C.; Weiss, L.; Lelievre, J.D.; Meyer, L.; Vittecoq, D.; Zbar, O.Z.D.; Frenkiel, J.; et al. Hospitalization of HIV positive patients: Significant demand affecting all hospital sectors. Rev. Epidemiol. Sante Publique 2018, 66, 7–17. [Google Scholar] [CrossRef]
- de Castro-Lima, V.A.C.; Borges, I.C.; Joelsons, D.; Sale, V.V.T.; Guimaraes, T.; Li Ho, Y.; Costa, S.F.; Moura, M.L.N. Impact of human immunodeficiency virus infection on mortality of patients who acquired healthcare associated-infection in critical care unit. Medicine 2019, 98, e15801. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.J.; Milovanovic, M.; Cichowitz, C.; Kinghorn, A.; Martinson, N.A.; Variava, E. Readmission and death following hospitalization among people with HIV in South Africa. PLoS ONE 2019, 14, e0218902. [Google Scholar] [CrossRef] [PubMed]
- Colasanti, J.; Del Rio, C. Declining Hospitalizations among Persons with Human Immunodeficiency Virus: Time to Leave No Patient Behind. Clin. Infect. Dis. 2020, 71, 1624–1626. [Google Scholar] [CrossRef]
- d’Arminio Monforte, A.; Diaz-Cuervo, H.; De Luca, A.; Maggiolo, F.; De Luca, A.; Bonora, S.; Castagna, A.; Girardi, E.; Antinori, A.; Caputo, S.L.; et al. Evolution of major non-HIV-related comorbidities in HIV-infected patients in the Italian Cohort of Individuals, Naïve for Antiretrovirals (ICONA) Foundation Study cohort in the period 2004–2014. HIV Med. 2019, 20, 99–109. [Google Scholar] [CrossRef]
- Maggi, P.; Santoro, C.R.; Nofri, M.; Ricci, E.; De Gennaro, N.; Bellacosa, C.; Schiaroli, E.; Orofino, G.; Menzaghi, B.; di Biagio, A.; et al. Clusterization of co-morbidities and multi-morbidities among persons living with HIV: A cross-sectional study. BMC Infect. Dis. 2019, 19, 555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prosperi, M.C.; Cozzi-Lepri, A.; Castagna, A.; Mussini, C.; Murri, A.; Giacometti, A.; Torti, C.; Costantini, A.; Narciso, P.; Ghinelli, F.; et al. Incidence of malignancies in HIV-infected patients and prognostic role of current CD4 cell count: Evidence from a large Italian cohort study. Clin. Infect. Dis. 2010, 50, 1316–1321. [Google Scholar] [CrossRef]
- Navon, L. Hospitalization Trends and Comorbidities among People with HIV/AIDS Compared with the Overall Hospitalized Population, Illinois, 2008–2014. Public Health Rep. 2018, 133, 442–451. [Google Scholar] [CrossRef] [Green Version]
- Mussini, C.; Galli, L.; Lepri, A.C.; De Luca, A.; Antinori, A.; Libertone, R.; Angarano, G.; Bonfanti, P.; Castagna, A.; Monforte, A.D.; et al. Incidence, timing, and determinants of bacterial pneumonia among HIV-infected patients: Data from the ICONA Foundation Cohort. J. Acquir. Immune Defic. Syndr. 2013, 63, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.; Rossotti, R.; Moioli, M.C.; Merli, M.; Valsecchi, P.; Zuccaro, V.; Vecchia, M.; Grecchi, C.; Patruno, S.F.A.; Sacchi, P.; et al. The impact of HIV infection and men who have sex with men status on hepatitis A infection: The experience of two tertiary centres in Northern Italy during the 2017 outbreak and in the 2009–2016 period. J. Viral Hepat. 2019, 26, 761–765. [Google Scholar] [CrossRef]
- Spagnuolo, V.; Poli, A.; Galli, L.; Nozza, S.; Bossolasco, S.; Cernuschi, M.; Maillard, M.; Hasson, H.; Gianotti, N.; Guffanti, M.; et al. Incidence and predictors of serological treatment response in early and late syphilis among people living with HIV. Open Forum Infect. Dis. 2018, 6, ofy324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guaraldi, G.; Malagoli, A.; Calcagno, A.; Mussi, C.; Celesia, B.M.; Carli, F.; de Socio, G.V.; Cattelan, A.M.; Orofino, G.; Riva, A.; et al. The increasing burden and complexity of multi-morbidity and polypharmacy in geriatric HIV patients: A cross sectional study of people aged 65–74 years and more than 75 years. BMC Geriatr. 2018, 18, 99. [Google Scholar] [CrossRef] [Green Version]
- Retornaz, F.; Petit, N.; Darque, A.; de Decker, L.; Farcet, A.; Chiche, L.; Ravaux, I.; Enel, P. Frailty phenotype in older people living with HIV: Concepts, prevention and issues. Le phénotype de fragilité chez les personnes vieillissantes avec le VIH: Concepts, prévention et enjeux de prise en charge. Geriatr. Psychol. Neuropsychiatr. Vieil. 2019, 17, 123–128. [Google Scholar] [PubMed]
- Yehia, B.R.; Fleishman, J.A.; Wilson, L.; Hicks, P.L.; Gborkorquellie, T.T.; Gebo, K.A.; HIV Research Network. Incidence of and risk factors for bacteraemia in HIV-infected adults in the era of highly active antiretroviral therapy. HIV Med. 2011, 12, 535–543. [Google Scholar] [CrossRef]
- Borges, A.H.; Neuhaus, J.; Sharma, S.; Neaton, J.D.; Henry, K.; Anagnostou, O.; Staub, T.; Emery, S.; Lundgren, J.D.; INSIGHT SMART; et al. The Effect of Interrupted/Deferred Antiretroviral Therapy on Disease Risk: A SMART and START Combined Analysis. J. Infect. Dis. 2019, 219, 254–263. [Google Scholar] [CrossRef]
- Kalichman, S.C.; Ramachandran, B.; Catz, S. Adherence to combination antiretroviral therapies in HIV patients of low literacy. J. Gen Intern. Med. 1999, 14, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.S.; Davis, T.C.; Osborn, C.Y.; Skripkauskas, S.; Bennett, C.L.; Makoul, G.L. Literacy, self-efficacy, and HIV medication adherence. Patient Educ. Couns. 2007, 65, 253–260. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| All Enrolled | Non-Hospitalized | Hospitalized | |||||
|---|---|---|---|---|---|---|---|
| N = 9524 | N = 8777 | N = 747 | p-Value ** | ||||
| Follow-up (years), median (IQR) | 3.3 | 1.6–5.7 | 3.2 | 1.5–5.6 | 4.7 | 2.5–7.0 | <0.01 |
| Sex, n (%) | |||||||
| Female | 1829 | 1.2 | 1639 | 18.7 | 190 | 25.4 | <0.01 |
| Male | 7695 | 80.8 | 7138 | 81.3 | 557 | 74.6 | |
| Age at first ART (years), median (IQR) | 39 | 32–48 | 39 | 31–47 | 43 | 35–51 | <0.01 |
| Ethnicity, n (%) | |||||||
| Asian | 116 | 1.2 | 109 | 1.2 | 7 | 0.9 | 0.637 |
| Black | 815 | 8.6 | 742 | 8.5 | 73 | 9.8 | |
| Caucasian | 7901 | 83 | 7289 | 83 | 612 | 81.9 | |
| Hispanic/Latino | 509 | 5.3 | 466 | 5.3 | 43 | 5.8 | |
| Other/unknwon | 183 | 2 | 171 | 1.9 | 12 | 1.6 | |
| Nationality, n (%) | |||||||
| Italian | 7414 | 77.9 | 6838 | 77.9 | 576 | 77.1 | 0.614 |
| Other | 2110 | 22.2 | 1939 | 22.1 | 171 | 22.9 | |
| HIV risk factor, n (%) | |||||||
| Heterosexual | 3675 | 38.6 | 3350 | 38.2 | 326 | 43.5 | <0.01 |
| IDU | 647 | 6.8 | 554 | 6.3 | 93 | 12.4 | |
| MSM | 4572 | 48 | 4299 | 49 | 273 | 36.5 | |
| Other/Unknown | 630 | 6.6 | 574 | 6.5 | 56 | 7.5 | |
| Education, n (%) | |||||||
| Primary | 444 | 4.7 | 386 | 4.4 | 58 | 7.8 | <0.01 |
| Secondary | 1544 | 16.2 | 1379 | 15.7 | 165 | 22.1 | |
| High | 2845 | 29.9 | 2661 | 30.3 | 184 | 24.6 | |
| Degree | 1196 | 12.5 | 1117 | 12.7 | 79 | 10.6 | |
| Unknown | 3495 | 36.7 | 3234 | 36.9 | 261 | 34.9 | |
| Occupation, n (%) | |||||||
| Housewife | 183 | 1.9 | 152 | 1.7 | 31 | 4.1 | <0.01 |
| Unemployed | 1162 | 12.2 | 1.044 | 11.9 | 118 | 15.8 | |
| Disabled | 21 | 0.2 | 19 | 0.2 | 2 | 0.3 | |
| Self-employed | 1261 | 13.2 | 1182 | 13.5 | 79 | 10.6 | |
| Employee | 3764 | 39.5 | 3482 | 39.7 | 282 | 37.7 | |
| Occasional worker | 263 | 2.8 | 239 | 2.7 | 24 | 3.2 | |
| Retired | 261 | 2.7 | 213 | 2.4 | 48 | 6.4 | |
| Student | 320 | 3.4 | 311 | 3.5 | 9 | 1.2 | |
| Other/Unknown | 2289 | 24 | 2.135 | 24.3 | 154 | 20.6 | |
| Smoke use, n (%) | |||||||
| No smoker | 4830 | 50.7 | 4475 | 51 | 355 | 47.5 | 0.177 |
| Smoker | 3800 | 39.9 | 3480 | 39.7 | 320 | 42.8 | |
| Unknown | 894 | 9.4 | 822 | 9.4 | 72 | 9.6 | |
| Alcohol use, n (%) | |||||||
| Abstainer | 3999 | 42 | 3647 | 41.6 | 352 | 47.1 | <0.01 |
| Abuse | 14 | 0.2 | 14 | 0.2 | 0 | 0 | |
| Drinker | 3509 | 36.8 | 3271 | 37.3 | 238 | 31.9 | |
| Unknown | 2002 | 21 | 1845 | 21 | 158 | 21 | |
| Family history of cardiovascular disease, n (%) | |||||||
| No | 5178 | 54.4 | 4785 | 54.5 | 393 | 52.6 | 0.405 |
| Yes | 1393 | 14.6 | 1287 | 14.7 | 106 | 14.2 | |
| Unknown | 2953 | 31 | 2705 | 30.8 | 248 | 33.2 | |
| Hepatitis C *, n (%) | |||||||
| Negative | 7925 | 83.2 | 7341 | 83.6 | 584 | 78.2 | <0.01 |
| Positive | 937 | 9.8 | 813 | 9.3 | 124 | 16.6 | |
| Unknown | 662 | 7 | 623 | 7.1 | 39 | 5.2 | |
| Hepatitis B *, n (%) | |||||||
| Negative | 8053 | 8.6 | 7.414 | 84.5 | 639 | 85.5 | <0.01 |
| Positive | 430 | 4.5 | 379 | 4.3 | 51 | 6.8 | |
| Unknown | 1041 | 10.9 | 984 | 11.2 | 57 | 7.6 | |
| Zenith HIV viral load (log10 copies/mL), median (IQR) | 4.9 | 4.3–5.4 | 4.9 | 4.3–5.4 | 5 | 4.5–5.6 | <0.01 |
| Nadir CD4, median (IQR) | 300 | 150–433 | 308 | 163–439 | 186 | 54–322 | <0.01 |
| HIV viral load copies/mL (classes) *, n (%) | |||||||
| ≤50 | 201 | 2.1 | 186 | 2.1 | 15 | 2 | 0.671 |
| 51–10,000 | 2099 | 22 | 1.947 | 22.2 | 152 | 20.4 | |
| >10,000 | 7187 | 75.5 | 6.609 | 75.3 | 578 | 77.4 | |
| Missing | 37 | 0.4 | 35 | 0.4 | 2 | 0.3 | |
| HIV viral load (copies/mL) *, median (IQR) | 48,959 | 10,756–186,200 | 48,168 | 10,584–181,170 | 61,830 | 12,675–264,700 | |
| CD4 cell count (classes) *, n (%) | |||||||
| ≤200 | 2571 | 27 | 2260 | 25.8 | 311 | 41.6 | <0.01 |
| 201–350 | 1861 | 19.5 | 1727 | 19.7 | 134 | 17.9 | |
| 351–500 | 2032 | 21.3 | 1918 | 2.9 | 114 | 15.3 | |
| >500 | 3032 | 3.8 | 2846 | 3.4 | 186 | 24.9 | |
| Missing | 28 | 0.3 | 26 | 0.3 | 2 | 0.3 | |
| CD4 (cell count) *, median (IQR) | 371 | 183–560 | 379 | 193–566 | 268 | 77–500 | <0.01 |
| Time from HIV diagnosis to first ART (months), median (IQR) | 2.3 | 0.8–21.2 | 2.3 | 0.8–20.4 | 2.1 | 0.7–34.3 | 0.702 |
| Time at Risk (Years) | Subjects | Number of Hospitalizations | IR * 100 | 95%CI | p-Value | ||
|---|---|---|---|---|---|---|---|
| L | U | ||||||
| All hospitalizations | |||||||
| 2008–2011 | 3191 | 2187 | 185 | 5.80 | 5.02 | 6.70 | ref |
| 2012–2015 | 15,118 | 6400 | 478 | 3.16 | 2.89 | 3.46 | <0.01 |
| 2016–2018 | 17,858 | 8687 | 395 | 2.21 | 2.00 | 2.44 | <0.01 |
| AIDS-defining conditions | |||||||
| 2008–2011 | 3191 | 2187 | 56 | 1.76 | 1.35 | 2.28 | ref |
| 2012–2015 | 15,118 | 6400 | 114 | 0.75 | 0.63 | 0.91 | <0.01 |
| 2016–2018 | 17,858 | 8687 | 76 | 0.43 | 0.34 | 0.53 | <0.01 |
| Infections non-ADC | |||||||
| 2008–2011 | 3191 | 2187 | 24 | 0.75 | 0.50 | 1.12 | ref |
| 2012–2015 | 15,118 | 6400 | 94 | 0.62 | 0.51 | 0.76 | 0.428 |
| 2016–2018 | 17,858 | 8687 | 122 | 0.68 | 0.57 | 0.82 | 0.68 |
| Non-infections/non-ADC | |||||||
| 2008–2011 | 3191 | 2187 | 105 | 3.29 | 2.72 | 3.98 | |
| 2012–2015 | 15,118 | 6400 | 270 | 1.79 | 1.59 | 2.01 | <0.01 |
| 2016–2018 | 17,858 | 8687 | 197 | 1.10 | 0.96 | 1.27 | <0.01 |
| Univariate | Multivariable | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Factors | IRR | p-Value | (5% Conf. | Interval) | IRR | p-Value | (95% Conf | Interval) | |
| Period | 2008–2011 (ref.) | ||||||||
| 2012–2015 | 0.55 | 0.000 | 0.42 | 0.71 | 0.71 | 0.019 | 0.54 | 0.95 | |
| 2016–2018 | 0.38 | 0.000 | 0.29 | 0.5 | 0.57 | 0.000 | 0.42 | 0.76 | |
| Sex | Male vs. Female | 0.69 | 0.001 | 0.55 | 0.85 | 0.78 | 0.052 | 0.61 | 1.00 |
| Class age (years) | ≤35 (ref.) | ||||||||
| 36–42 | 1.1 | 0.519 | 0.83 | 1.45 | 1.07 | 0.642 | 0.81 | 1.40 | |
| 43–51 | 1.27 | 0.060 | 0.99 | 1.63 | 1.19 | 0.161 | 0.93 | 1.52 | |
| ≥52 | 1.76 | 0.000 | 1.37 | 2.26 | 1.63 | 0.000 | 1.28 | 2.08 | |
| Natonality | Other vs. Italian | 1.19 | 0.116 | 0.96 | 1.48 | 1.13 | 0.280 | 0.91 | 1.40 |
| HIV risk factor | Heterosexual (ref.) | ||||||||
| IDU | 1.99 | 0.000 | 1.46 | 2.71 | 1.56 | 0.010 | 1.11 | 2.19 | |
| MSM | 0.74 | 0.003 | 0.61 | 0.9 | 1.15 | 0.235 | 0.91 | 1.46 | |
| Other/Unknown | 1.01 | 0.973 | 0.72 | 1.41 | 0.99 | 0.954 | 0.71 | 1.38 | |
| Family history of cardiovascular disease | No (ref.) | ||||||||
| Yes | 1.33 | 0.005 | 1.09 | 1.63 | 1.30 | 0.010 | 1.07 | 1.60 | |
| Unknown | 0.82 | 0.110 | 0.64 | 1.05 | 0.84 | 0.168 | 0.66 | 1.08 | |
| CD4 (cells/mm3) | ≤200 (ref.) | ||||||||
| 201–350 | 0.4 | 0.000 | 0.32 | 0.5 | 0.45 | 0.000 | 0.35 | 0.57 | |
| 351–500 | 0.23 | 0.000 | 0.18 | 0.28 | 0.29 | 0.000 | 0.23 | 0.37 | |
| >500 | 0.16 | 0.000 | 0.13 | 0.19 | 0.24 | 0.000 | 0.19 | 0.30 | |
| Missing | 0.47 | 0.023 | 0.24 | 0.9 | 0.48 | 0.313 | 0.12 | 2.00 | |
| HIV viral load (copies/mL) | ≤50 (ref.) | ||||||||
| 51–10,000 | 2.39 | 0.000 | 1.99 | 2.88 | 1.62 | 0.000 | 1.32 | 1.97 | |
| >10,000 | 3.43 | 0.000 | 2.77 | 4.27 | 1.72 | 0.000 | 1.35 | 2.20 | |
| Missing | 2.45 | 0.003 | 1.36 | 4.42 | 1.59 | 0.490 | 0.43 | 5.93 | |
| Hepatitis C coinfection | Negative (ref.) | ||||||||
| Positive | 1.55 | 0.037 | 1.03 | 2.33 | 1.03 | 0.900 | 0.66 | 1.59 | |
| Unknown | 0.7 | 0.022 | 0.51 | 0.95 | 0.73 | 0.036 | 0.55 | 0.98 | |
| Time from HIV diagnosis to first ART (months) | 0–2 (ref.) | ||||||||
| 2–20 | 0.52 | 0.000 | 0.42 | 0.65 | 0.76 | 0.019 | 0.60 | 0.96 | |
| >20 | 0.92 | 0.436 | 0.74 | 1.14 | 1.15 | 0.219 | 0.92 | 1.44 | |
| Factors | ADC | Infection NON-AIDS-Defining | Non-Infection/NON-ADC | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IRR | P > z | 95% CI | IRR | P > z | 95% CI | IRR | P > z | 95% CI | |||||
| Period | 2008–2011 (ref.) | ||||||||||||
| 2012–2015 | 0.69 | 0.150 | 0.42 | 1.14 | 1.10 | 0.696 | 0.67 | 1.80 | 0.64 | 0.007 | 0.46 | 0.89 | |
| 2016–2018 | 0.49 | 0.011 | 0.28 | 0.85 | 1.44 | 0.162 | 0.86 | 2.41 | 0.42 | 0.000 | 0.30 | 0.59 | |
| Sex | Male vs. Female | 1.25 | 0.322 | 0.81 | 1.93 | 0.60 | 0.009 | 0.41 | 0.88 | 0.71 | 0.036 | 0.52 | 0.98 |
| Class age (years) | ≤35 (ref.) | ||||||||||||
| 36–42 | 1.38 | 0.268 | 0.78 | 2.44 | 1.08 | 0.707 | 0.72 | 1.61 | 0.93 | 0.679 | 0.65 | 1.32 | |
| 43–51 | 1.35 | 0.171 | 0.88 | 2.09 | 1.08 | 0.695 | 0.73 | 1.60 | 1.18 | 0.316 | 0.85 | 1.65 | |
| ≥52 | 1.39 | 0.153 | 0.89 | 2.17 | 1.06 | 0.777 | 0.70 | 1.60 | 2.02 | 0.000 | 1.45 | 2.80 | |
| Nationality | Other vs Italian | 1.20 | 0.362 | 0.81 | 1.77 | 1.45 | 0.029 | 1.04 | 2.03 | 0.95 | 0.748 | 0.71 | 1.28 |
| HIV risk factor | Heterosexual (ref.) | ||||||||||||
| IDU | 0.72 | 0.316 | 0.37 | 1.38 | 1.77 | 0.027 | 1.07 | 2.94 | 1.87 | 0.005 | 1.21 | 2.88 | |
| MSM | 1.18 | 0.465 | 0.76 | 1.84 | 1.46 | 0.047 | 1.00 | 2.12 | 1.05 | 0.754 | 0.78 | 1.41 | |
| Other/Unknown | 1.00 | 0.997 | 0.55 | 1.81 | 0.66 | 0.245 | 0.33 | 1.32 | 1.11 | 0.602 | 0.75 | 1.63 | |
| Family history of cardiovascular disease | No (ref.) | ||||||||||||
| Yes | 0.94 | 0.764 | 0.64 | 1.39 | 1.02 | 0.909 | 0.74 | 1.39 | 1.66 | 0.000 | 1.30 | 2.13 | |
| Unknown | 0.45 | 0.018 | 0.23 | 0.87 | 1.04 | 0.863 | 0.70 | 1.54 | 0.96 | 0.802 | 0.70 | 1.32 | |
| CD4 (cells/mm3) | ≤200 (ref.) | ||||||||||||
| 201–350 | 0.23 | 0.000 | 0.14 | 0.39 | 0.77 | 0.269 | 0.49 | 1.22 | 0.57 | 0.000 | 0.42 | 0.78 | |
| 351–500 | 0.10 | 0.000 | 0.06 | 0.18 | 0.39 | 0.000 | 0.23 | 0.66 | 0.45 | 0.000 | 0.32 | 0.63 | |
| >500 | 0.06 | 0.000 | 0.03 | 0.10 | 0.35 | 0.000 | 0.22 | 0.58 | 0.37 | 0.000 | 0.27 | 0.52 | |
| Missing | 0.87 | 0.899 | 0.10 | 7.46 | 0.32 | 0.145 | 0.07 | 1.49 | 0.32 | 0.050 | 0.10 | 1.00 | |
| HIV viral load (copies/mL) | ≥50 (ref.) | ||||||||||||
| 51–10,000 | 1.97 | 0.001 | 1.33 | 2.94 | 1.69 | 0.008 | 1.14 | 2.49 | 1.47 | 0.003 | 1.14 | 1.89 | |
| >10,000 | 2.75 | 0.000 | 1.80 | 4.20 | 1.77 | 0.018 | 1.10 | 2.83 | 1.20 | 0.304 | 0.85 | 1.70 | |
| Missing | 0.93 | 0.945 | 0.11 | 7.83 | 2.97 | 0.145 | 0.69 | 12.82 | 2.14 | 0.137 | 0.78 | 5.86 | |
| Hepatitis C coinfection | Negative (ref.) | ||||||||||||
| Positive | 1.18 | 0.742 | 0.44 | 3.12 | 1.38 | 0.300 | 0.75 | 2.52 | 0.93 | 0.798 | 0.53 | 1.62 | |
| Unknown | 1.05 | 0.898 | 0.52 | 2.10 | 0.90 | 0.671 | 0.55 | 1.48 | 0.62 | 0.008 | 0.44 | 0.88 | |
| Time from HIV diagnosis to first ART (months) | 0–2 (ref.) | ||||||||||||
| 2–20 | 0.41 | 0.002 | 0.23 | 0.72 | 0.76 | 0.185 | 0.51 | 1.14 | 0.92 | 0.560 | 0.69 | 1.22 | |
| >20 | 1.16 | 0.537 | 0.73 | 1.85 | 1.35 | 0.084 | 0.96 | 1.90 | 1.11 | 0.442 | 0.85 | 1.47 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nozza, S.; Timelli, L.; Saracino, A.; Gianotti, N.; Lazzaretti, C.; Tavelli, A.; Puoti, M.; Lo Caputo, S.; Antinori, A.; Monforte, A.d.; et al. Decrease in Incidence Rate of Hospitalizations Due to AIDS-Defining Conditions but Not to Non-AIDS Conditions in PLWHIV on cART in 2008–2018 in Italy. J. Clin. Med. 2021, 10, 3391. https://doi.org/10.3390/jcm10153391
Nozza S, Timelli L, Saracino A, Gianotti N, Lazzaretti C, Tavelli A, Puoti M, Lo Caputo S, Antinori A, Monforte Ad, et al. Decrease in Incidence Rate of Hospitalizations Due to AIDS-Defining Conditions but Not to Non-AIDS Conditions in PLWHIV on cART in 2008–2018 in Italy. Journal of Clinical Medicine. 2021; 10(15):3391. https://doi.org/10.3390/jcm10153391
Chicago/Turabian StyleNozza, Silvia, Laura Timelli, Annalisa Saracino, Nicola Gianotti, Claudia Lazzaretti, Alessandro Tavelli, Massimo Puoti, Sergio Lo Caputo, Andrea Antinori, Antonella d’Arminio Monforte, and et al. 2021. "Decrease in Incidence Rate of Hospitalizations Due to AIDS-Defining Conditions but Not to Non-AIDS Conditions in PLWHIV on cART in 2008–2018 in Italy" Journal of Clinical Medicine 10, no. 15: 3391. https://doi.org/10.3390/jcm10153391
APA StyleNozza, S., Timelli, L., Saracino, A., Gianotti, N., Lazzaretti, C., Tavelli, A., Puoti, M., Lo Caputo, S., Antinori, A., Monforte, A. d., Mussini, C., Girardi, E., & on behalf of ICONA Foundation Study Group. (2021). Decrease in Incidence Rate of Hospitalizations Due to AIDS-Defining Conditions but Not to Non-AIDS Conditions in PLWHIV on cART in 2008–2018 in Italy. Journal of Clinical Medicine, 10(15), 3391. https://doi.org/10.3390/jcm10153391