
Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients

 ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Polysomnography
2.2. Statistical Analysis
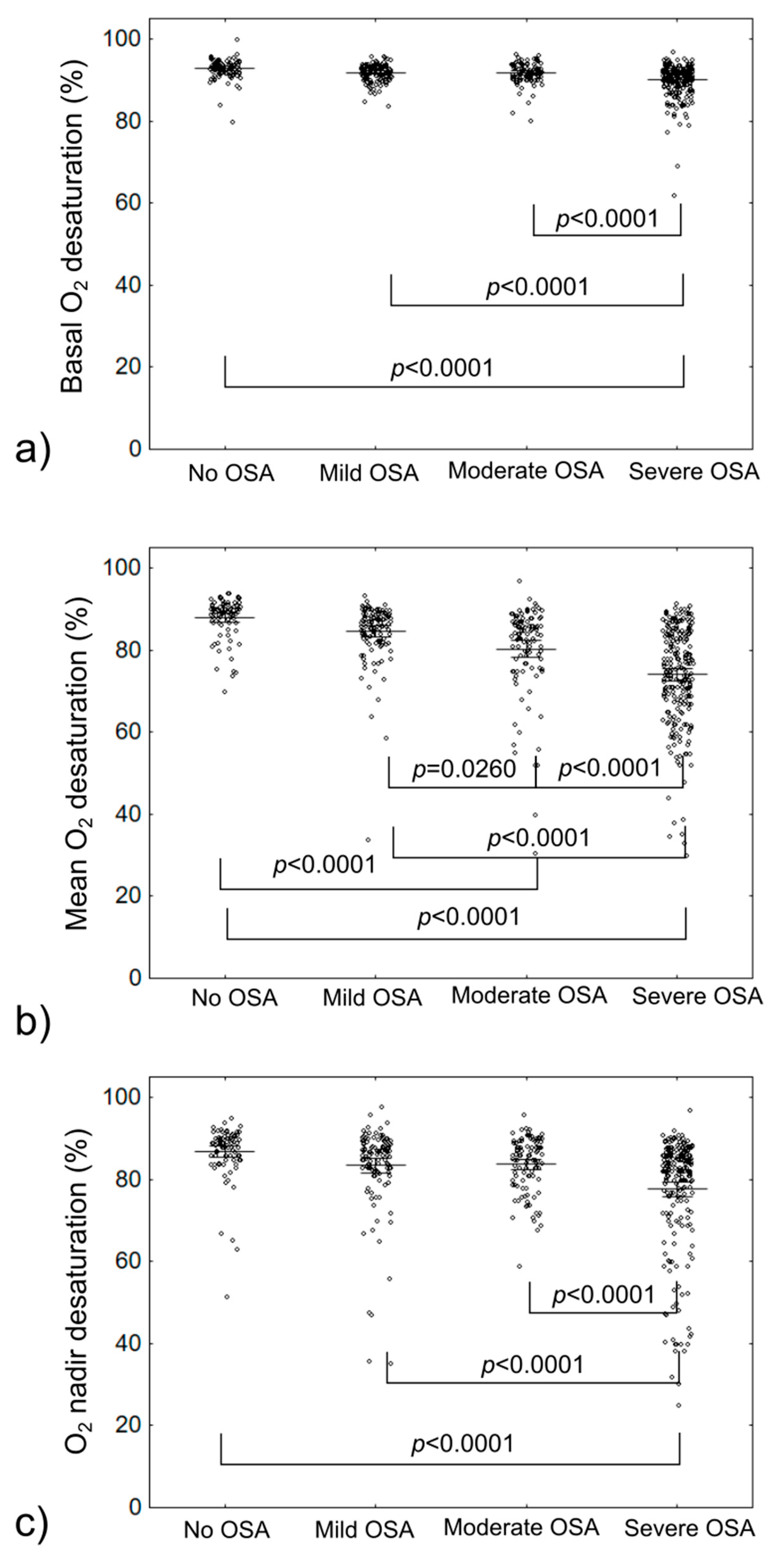
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.D.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Gabryelska, A.; Łukasik, Z.M.; Makowska, J.S.; Białasiewicz, P. Obstructive Sleep Apnea: From Intermittent Hypoxia to Cardiovascular Complications via Blood Platelets. Front. Neurol. 2018, 9, 635. [Google Scholar] [CrossRef]
- Marshall, N.S.; Wong, K.K.H.; Phillips, C.L.; Liu, P.Y.; Knuiman, M.W.; Grunstein, R.R. Is Sleep Apnea an Independent Risk Factor for Prevalent and Incident Diabetes in the Busselton Health Study? J. Clin. Sleep Med. 2009, 5, 15–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagayoshi, M.; Punjabi, N.M.; Selvin, E.; Pankow, J.S.; Shahar, E.; Iso, H.; Folsom, A.R.; Lutsey, P.L. Obstructive sleep apnea and incident type 2 diabetes. Sleep Med. 2016, 25, 156–161. [Google Scholar] [CrossRef] [Green Version]
- Anothaisintawee, T.; Reutrakul, S.; Van Cauter, E.; Thakkinstian, A. Sleep disturbances compared to traditional risk factors for diabetes development: Systematic review and meta-analysis. Sleep Med. Rev. 2016, 30, 11–24. [Google Scholar] [CrossRef]
- Tanno, S.; Tanigawa, T.; Saito, I.; Nishida, W.; Maruyama, K.; Eguchi, E.; Sakurai, S.; Osawa, H.; Punjabi, N.M. Sleep-related intermittent hypoxemia and glucose intolerance: A community-based study. Sleep Med. 2014, 15, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Karuga, F.F.; Szmyd, B.; Białasiewicz, P. HIF-1α as a Mediator of Insulin Resistance, T2DM, and Its Complications: Potential Links With Obstructive Sleep Apnea. Front. Physiol. 2020, 11, 1035. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Szmyd, B.; Szemraj, J.; Stawski, R.; Sochal, M.; Białasiewicz, P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1α protein. J. Clin. Sleep Med. 2020, 6, 1761–1768. [Google Scholar] [CrossRef]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia–inducible factor–1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Gabryelska, A.; Stawski, R.; Sochal, M.; Szmyd, B.; Białasiewicz, P. Influence of one-night CPAP therapy on the changes of HIF-1α protein in OSA patients: A pilot study. J. Sleep Res. 2020, 29, e12995. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Li, N.; Yao, X.; Zhou, L. Potential inflammatory markers in obstructive sleep apnea-hypopnea syndrome. Bosn. J. Basic Med. Sci. 2017, 17, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kendzerska, T.; Gershon, A.S.; Hawker, G.; Tomlinson, G.; Leung, R.S. Obstructive sleep apnea and incident diabetes a historical cohort study. Am. J. Respir. Crit. Care Med. 2014, 190, 218–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K.M.; Lutsey, P.L.; Ogilvie, R.P.; Pankow, J.S.; Bertoni, A.; Michos, E.D.; Punjabi, N.; Redline, S. Associations between polysomnography and actigraphy-based sleep indices and glycemic control among those with and without type 2 diabetes: The Multi-Ethnic Study of Atherosclerosis. Sleep 2018, 41, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Appleton, S.L.; Vakulin, A.; Wittert, G.A.; Martin, S.A.; Grant, J.F.; Taylor, A.W.; McEvoy, R.D.; Antic, N.A.; Catcheside, P.G.; Adams, R.J. The association of obstructive sleep apnea (OSA) and nocturnal hypoxemia with the development of abnormal HbA1c in a population cohort of men without diabetes. Diabetes Res. Clin. Pract. 2016, 114, 151–159. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]
- Labarca, G.; Campos, J.; Thibaut, K.; Dreyse, J.; Jorquera, J. Do T90 and SaO2 nadir identify a different phenotype in obstructive sleep apnea? Sleep Breath. 2019, 23, 1007–1010. [Google Scholar] [CrossRef]
- Muraki, I.; Tanigawa, T.; Yamagishi, K.; Sakurai, S.; Ohira, T.; Imano, H.; Kitamura, A.; Kiyama, M.; Sato, S.; Shimamoto, T.; et al. Nocturnal intermittent hypoxia and the development of type 2 diabetes: The Circulatory Risk in Communities Study (CIRCS). Diabetologia 2010, 53, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Hui, P.; Zhao, L.; Xie, Y.; Wei, X.; Ma, W.; Wang, J.; Hou, Y.; Ning, J.; Zhou, L.; Guo, Q.; et al. Nocturnal hypoxemia causes hyperglycemia in patients with obstructive sleep apnea and type 2 diabetes mellitus. Am. J. Med. Sci. 2016, 351, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Trzepizur, W.; Le Vaillant, M.; Meslier, N.; Pigeanne, T.; Masson, P.; Humeau, M.P.; Bizieux-Thaminy, A.; Goupil, F.; Chollet, S.; Ducluzeau, P.H.; et al. Independent association between nocturnal intermittent hypoxemia and metabolic dyslipidemia. Chest 2013, 143, 1584–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesarwi, O.A.; Sharma, E.V.; Jun, J.C.; Polotsky, V.Y. Metabolic dysfunction in obstructive sleep apnea: A critical examination of underlying mechanisms. Sleep Biol. Rhythms 2015, 13, 2–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, J.E.; Punjabi, N.M.; Wilding, J.P.; Alberti, K.G.M.M.; Zimmet, P.Z. Sleep-disordered breathing and type 2 diabetes. A report from the International Diabetes Federation Taskforce on Epidemiology and Prevention. Diabetes Res. Clin. Pract. 2008, 81, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Papale, M.; Parisi, G.; Spicuzza, L.; Rotolo, N.; Mulè, E.; Aloisio, D.; Manti, S.; Leonardi, S. Nocturnal non invasive ventilation in normocapnic cystic fibrosis patients: A pilot study: Non-invasive ventilation in cystic fibrosis. Acta Biomed. 2021, 92, e2021164. [Google Scholar]


{kind=link}
{kind=link}
| Parameter | All Participants | No OSA (n = 155; AHI < 5) | OSA (n = 394; AHI ≥ 5) | p-Value |
|---|---|---|---|---|
| Age (years) | 62.00 (57.00–68.00) | 61 (53.5–69) | 62 (57–68) | 0.1525 |
| Sex (male) | 56.60% | 47.62% | 58.28% | 0.0696 |
| BMI (kg/m2) | 31.13 (27.46–35.66) | 28.69 (25.61–31.65) | 31.56 (27.92–36.20) | <0.0001 |
| AHI (events/h) | 24.30 (9.00–49.50) | 2.1 (1–3.75) | 30.38 (14.3–52.89) | <0.0001 |
| Basal O2 (%) | 91.90 (90.00–93.20) | 93.2 (91.75–94.05) | 91.6 (90–93) | <0.0001 |
| Mean desaturation O2 (%) | 83.45 (74.10–88.00) | 89.8 (86.9–91) | 82 (72.9–87) | <0.0001 |
| O2 nadir (%) | 85.00 (79.90–88.10) | 88.9 (85–90.5) | 84 (78.1–87.9) | <0.0001 |
| DM2 | 19.50% | 10.71% | 21.08% | 0.0274 |
| Groups | |||||||
|---|---|---|---|---|---|---|---|
| Saturation Parameter | No OSA (AHI < 5) | Mild OSA | Moderate OSA | Severe OSA | Any OSA | p-Value | p-Value Adjusted |
| Basal O2 (%) | 93.20 (91.75–94.05) | 92.00 (90.90–93.40) | 92.00 (90.90–93.40) | 91.00 (88.80–92.30) | 91.6 (90.00–93.00) | <0.0001 <0.0001 * | <0.0001 <0.0001 * |
| Mean desaturation O2 (%) | 89.80 (86.90–91.00) | 86.50 (82.40–88.90) | 83.95 (76.90–87.00) | 75.25 (67.00–83.90) | 82.00 (72.90–87.00) | <0.0001 <0.0001 * | <0.0001 <0.0001 * |
| O2 nadir (%) | 88.90 (85.00–90.50) | 86.00 (82.10–88.90) | 85.10 (79.90–89.00) | 82.10 (75.00–86.20) | 84.00 (78.10–87.90) | <0.0001 <0.0001 | <0.0001 <0.0001 |
| Univariate Regression | Multivariate Regression | |||||
|---|---|---|---|---|---|---|
| HR | 95%CI | p | HR | 95%CI | p | |
| BMI | 1.1170 | 1.0826–1.1526 | <0.0001 | 1.1219 | 1.0824–1.1629 | <0.0001 |
| AHI | 1.0107 | 1.0036–1.0178 | 0.0032 | 1.0054 | 0.9980–1.0129 | 0.1542 |
| Basal O2 | 0.9326 | 0.8875–0.9799 | 0.0057 | 1.0262 | 0.9494–1.1091 | 0.5146 |
| Mean deasturatiom O2 | 0.9864 | 0.9729–1.0002 | 0.0531 | - | - | - |
| O2 nadir | 0.9844 | 0.9727–0.9961 | 0.0092 | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabryelska, A.; Chrzanowski, J.; Sochal, M.; Kaczmarski, P.; Turkiewicz, S.; Ditmer, M.; Karuga, F.F.; Czupryniak, L.; Białasiewicz, P. Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 3770. https://doi.org/10.3390/jcm10173770
Gabryelska A, Chrzanowski J, Sochal M, Kaczmarski P, Turkiewicz S, Ditmer M, Karuga FF, Czupryniak L, Białasiewicz P. Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients. Journal of Clinical Medicine. 2021; 10(17):3770. https://doi.org/10.3390/jcm10173770
Chicago/Turabian StyleGabryelska, Agata, Jędrzej Chrzanowski, Marcin Sochal, Piotr Kaczmarski, Szymon Turkiewicz, Marta Ditmer, Filip Franciszek Karuga, Leszek Czupryniak, and Piotr Białasiewicz. 2021. "Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients" Journal of Clinical Medicine 10, no. 17: 3770. https://doi.org/10.3390/jcm10173770
APA StyleGabryelska, A., Chrzanowski, J., Sochal, M., Kaczmarski, P., Turkiewicz, S., Ditmer, M., Karuga, F. F., Czupryniak, L., & Białasiewicz, P. (2021). Nocturnal Oxygen Saturation Parameters as Independent Risk Factors for Type 2 Diabetes Mellitus among Obstructive Sleep Apnea Patients. Journal of Clinical Medicine, 10(17), 3770. https://doi.org/10.3390/jcm10173770