
Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review


Abstract
:1. Introduction
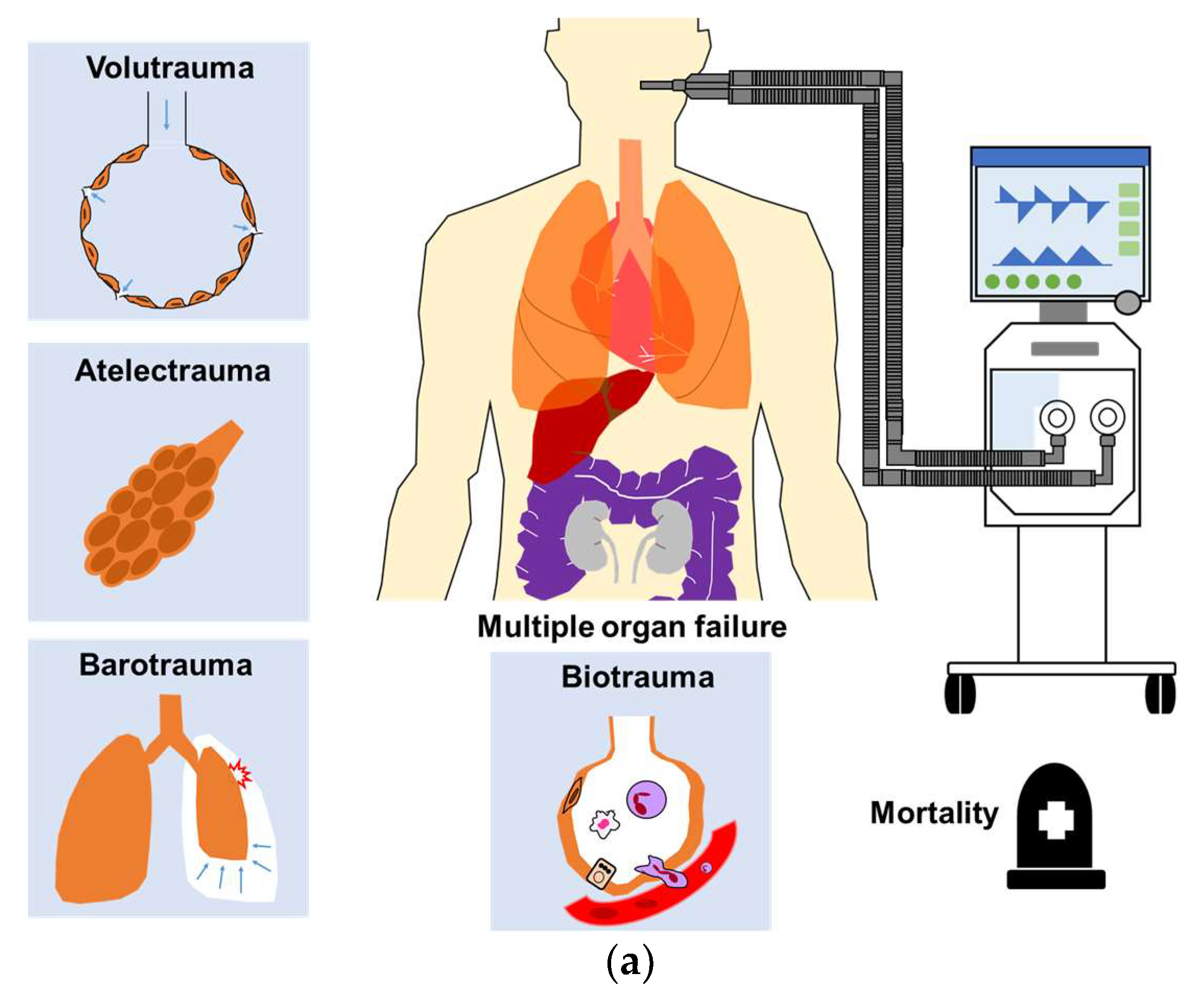
2. Ventilator-Induced Lung Injury
2.1. Introduction
2.2. Ventilator-Related Causes of VILI
2.3. Pathophysiology of the Lung Parenchyma Associated with VILI
3. Multiple Organ Failure Due to VILI
4. Mechanical Ventilator Settings during ECMO
4.1. Introduction
4.2. Modes of Mechanical Ventilation
4.3. Mechanical Power
4.4. Tidal Volume
4.5. Positive End-Expiratory Pressure
4.6. Plateau Pressure
4.7. Driving Pressure
4.8. Transpulmonary Pressure
4.9. Respiratory Rate
4.10. Fraction of Inspired Oxygenation
5. Uncertainties and Future Research
5.1. Introduction
5.2. Spontaneous Breathing during ECMO
5.3. Apneic and Near-Apneic Ventilation
5.4. Extracorporeal Carbon Dioxide Removal
5.5. Weaning from ECMO and Mechanical Ventilation
6. Collateral Effect of ECMO
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, B.T.; Chambers, R.C.; Liu, K.D. Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2017, 377, 562–572. [Google Scholar]
- Meyer, N.J.; Gattinoni, L.; Calfee, C.S. Acute respiratory distress syndrome. Lancet 2021, 398, 622–637. [Google Scholar]
- Gattinoni, L.; Tonetti, T.; Quintel, M. Intensive care medicine in 2050: Ventilator-induced lung injury. Intensive Care Med. 2018, 44, 76–78. [Google Scholar]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar]
- Curley, G.F.; Laffey, J.G.; Zhang, H.; Slutsky, A.S. Biotrauma and Ventilator-Induced Lung Injury: Clinical Implications. Chest 2016, 150, 1109–1117. [Google Scholar]
- Gattinoni, L.; Marini, J.J.; Collino, F.; Maiolo, G.; Rapetti, F.; Tonetti, T.; Vasques, F.; Quintel, M. The future of mechanical ventilation: Lessons from the present and the past. Crit. Care 2017, 21, 183. [Google Scholar]
- Brodie, D.; Bacchetta, M. Extracorporeal membrane oxygenation for ARDS in adults. N. Engl. J. Med. 2011, 365, 1905–1914. [Google Scholar]
- Combes, A.; Schmidt, M.; Hodgson, C.L.; Fan, E.; Ferguson, N.D.; Fraser, J.F.; Jaber, S.; Pesenti, A.; Ranieri, M.; Rowan, K.; et al. Extracorporeal life support for adults with acute respiratory distress syndrome. Intensive Care Med. 2020, 46, 2464–2476. [Google Scholar]
- Chiu, L.C.; Chuang, L.P.; Leu, S.W.; Lin, Y.J.; Chang, C.J.; Li, H.H.; Tsai, F.C.; Chang, C.H.; Hung, C.Y.; Lin, S.W.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome: Propensity Score Matching. Membranes 2021, 11, 393. [Google Scholar]
- Akoumianaki, E.; Jonkman, A.; Sklar, M.C.; Georgopoulos, D.; Brochard, L. A rational approach on the use of extracorporeal membrane oxygenation in severe hypoxemia: Advanced technology is not a panacea. Annu. Intensive Care 2021, 11, 107. [Google Scholar]
- Ramanathan, K.; Shekar, K.; Ling, R.R.; Barbaro, R.P.; Wong, S.N.; Tan, C.S.; Rochwerg, B.; Fernando, S.M.; Takeda, S.; MacLaren, G.; et al. Extracorporeal membrane oxygenation for COVID-19: A systematic review and meta-analysis. Crit. Care 2021, 25, 211. [Google Scholar]
- Peek, G.J.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar]
- Combes, A.; Peek, G.J.; Hajage, D.; Hardy, P.; Abrams, D.; Schmidt, M.; Dechartres, A.; Elbourne, D. ECMO for severe ARDS: Systematic review and individual patient data meta-analysis. Intensive Care Med. 2020, 46, 2048–2057. [Google Scholar]
- Schmidt, M.; Pellegrino, V.; Combes, A.; Scheinkestel, C.; Cooper, D.J.; Hodgson, C. Mechanical ventilation during extracorporeal membrane oxygenation. Crit Care. 2014, 18, 203. [Google Scholar]
- Marhong, J.D.; Munshi, L.; Detsky, M.; Telesnicki, T.; Fan, E. Mechanical ventilation during extracorporeal life support (ECLS): A systematic review. Intensive Care Med. 2015, 41, 994–1003. [Google Scholar]
- Chiu, L.C.; Lin, S.W.; Chuang, L.P.; Li, H.H.; Liu, P.H.; Tsai, F.C.; Chang, C.H.; Hung, C.Y.; Lee, C.S.; Leu, S.W.; et al. Mechanical power during extracorporeal membrane oxygenation and hospital mortality in patients with acute respiratory distress syndrome. Crit. Care 2021, 25, 13. [Google Scholar]
- Pham, T.; Combes, A.; Rozé, H.; Chevret, S.; Mercat, A.; Roch, A.; Mourvillier, B.; Ara-Somohano, C.; Bastien, O.; Zogheib, E.; et al. REVA Research Network. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: A cohort study and propensity-matched analysis. Am. J. Respir. Crit. Care Med. 2013, 187, 276–285. [Google Scholar]
- Modrykamien, A.M.; Hernandez, O.O.; Im, Y.; Walters, R.W.; Schrader, C.L.; Smith, L.E.; Lima, B. Mechanical Ventilation in Patients with the Acute Respiratory Distress Syndrome and Treated with Extracorporeal Membrane Oxygenation: Impact on Hospital and 30 Day Postdischarge Survival. ASAIO J. 2016, 62, 607–612. [Google Scholar]
- Schmidt, M.; Stewart, C.; Bailey, M.; Nieszkowska, A.; Kelly, J.; Murphy, L.; Pilcher, D.; Cooper, D.J.; Scheinkestel, C.; Pellegrino, V.; et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: A retrospective international multicenter study. Crit. Care Med. 2015, 43, 654–664. [Google Scholar]
- Neto, A.S.; Schmidt, M.; Azevedo, L.C.; Bein, T.; Brochard, L.; Beutel, G.; Combes, A.; Costa, E.L.; Hodgson, C.; Lindskov, C.; et al. ReVA Research Network and the PROVE Network Investigators. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: A pooled individual patient data analysis: Mechanical ventilation during ECMO. Intensive Care Med. 2016, 42, 1672–1684. [Google Scholar]
- Chiu, L.C.; Hu, H.C.; Hung, C.Y.; Chang, C.H.; Tsai, F.C.; Yang, C.T.; Huang, C.C.; Wu, H.P.; Kao, K.C. Dynamic driving pressure associated mortality in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann. Intensive Care 2017, 7, 12. [Google Scholar]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar]
- Maiolo, G.; Collino, F.; Vasques, F.; Rapetti, F.; Tonetti, T.; Romitti, F.; Cressoni, M.; Chiumello, D.; Moerer, O.; Herrmann, P.; et al. Reclassifying Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2018, 197, 1586–1595. [Google Scholar]
- Rozencwajg, S.; Guihot, A.; Franchineau, G.; Lescroat, M.; Bréchot, N.; Hékimian, G.; Lebreton, G.; Autran, B.; Luyt, C.E.; Combes, A.; et al. Ultra-Protective Ventilation Reduces Biotrauma in Patients on Venovenous Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. Crit. Care Med. 2019, 47, 1505–1512. [Google Scholar]
- Schmidt, M.; Pham, T.; Arcadipane, A.; Agerstrand, C.; Ohshimo, S.; Pellegrino, V.; Vuylsteke, A.; Guervilly, C.; McGuinness, S.; Pierard, S.; et al. Mechanical Ventilation Management during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. An International Multicenter Prospective Cohort. Am. J. Respir. Crit. Care Med. 2019, 200, 1002–1012. [Google Scholar]
- Abrams, D.; Schmidt, M.; Pham, T.; Beitler, J.R.; Fan, E.; Goligher, E.C.; McNamee, J.J.; Patroniti, N.; Wilcox, M.E.; Combes, A.; et al. Mechanical Ventilation for Acute Respiratory Distress Syndrome during Extracorporeal Life Support. Research and Practice. Am. J. Respir. Crit. Care Med. 2020, 201, 514–525. [Google Scholar]
- Chiu, L.C.; Tsai, F.C.; Hu, H.C.; Chang, C.H.; Hung, C.Y.; Lee, C.S.; Li, S.H.; Lin, S.W.; Li, L.F.; Huang, C.C.; et al. Survival predictors in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2015, 99, 243–250. [Google Scholar]
- Kim, H.S.; Kim, J.H.; Chung, C.R.; Hong, S.B.; Cho, W.H.; Cho, Y.J.; Sim, Y.S.; Kim, W.Y.; Kang, B.J.; Park, S.H.; et al. Lung Compliance and Outcomes in Patients with Acute Respiratory Distress Syndrome Receiving ECMO. Ann. Thorac. Surg. 2019, 108, 176–182. [Google Scholar]
- Extracorporeal Life Support Organization. Available online: https://www.elso.org/Resources/Guidelines.aspx (accessed on 22 July 2021).
- Narendra, D.K.; Hess, D.R.; Sessler, C.N.; Belete, H.M.; Guntupalli, K.K.; Khusid, F.; Carpati, C.M.; Astiz, M.E.; Raoof, S. Update in Management of Severe Hypoxemic Respiratory Failure. Chest 2017, 152, 867–879. [Google Scholar]
- Cressoni, M.; Gotti, M.; Chiurazzi, C.; Massari, D.; Algieri, I.; Amini, M.; Cammaroto, A.; Brioni, M.; Montaruli, C.; Nikolla, K.; et al. Mechanical Power and Development of Ventilator-induced Lung Injury. Anesthesiology 2016, 124, 1100–1118. [Google Scholar]
- Serpa, N.A.; Deliberato, R.O.; Johnson, A.E.W.; Bos, L.D.; Amorim, P.; Pereira, S.M.; Cazati, D.C.; Cordioli, R.L.; Correa, T.D.; Pollard, T.J.; et al. Mechanical power of ventilation is associated with mortality in critically ill patients: An analysis of patients in two observational cohorts. Intensive Care Med. 2018, 44, 1914–1922. [Google Scholar]
- Parhar, K.K.S.; Zjadewicz, K.; Soo, A.; Sutton, A.; Zjadewicz, M.; Doig, L.; Lam, C.; Ferland, A.; Niven, D.J.; Fiest, K.M.; et al. Epidemiology, Mechanical Power, and 3-Year Outcomes in Acute Respiratory Distress Syndrome Patients Using Standardized Screening. An Observational Cohort Study. Ann. Am. Thorac. Soc. 2019, 16, 1263–1272. [Google Scholar]
- Cressoni, M.; Cadringher, P.; Chiurazzi, C.; Amini, M.; Gallazzi, E.; Marino, A.; Brioni, M.; Carlesso, E.; Chiumello, D.; Quintel, M.; et al. Lung inhomogeneity in patients with acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2014, 189, 149–158. [Google Scholar]
- Marini, J.J.; Rocco, P.R.M.; Gattinoni, L. Static and Dynamic Contributors to Ventilator-induced Lung Injury in Clinical Practice. Pressure, Energy, and Power. Am. J. Respir. Crit. Care Med. 2020, 201, 767–774. [Google Scholar]
- Marini, J.J.; Gattinoni, L. Time Course of Evolving Ventilator-Induced Lung Injury: The “Shrinking Baby Lung”. Crit. Care Med. 2020, 48, 1203–1209. [Google Scholar]
- Fan, E.; del Sorbo, L.; Goligher, E.C.; Hodgson, C.L.; Munshi, L.; Walkey, A.J.; Adhikari, N.K.J.; Amato, M.B.P.; Branson, R.; Brower, R.G.; et al. American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1253–1263. [Google Scholar]
- Sahetya, S.K.; Goligher, E.C.; Brower, R.G. Fifty Years of Research in ARDS. Setting Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1429–1438. [Google Scholar]
- Beitler, J.R.; Sarge, T.; Banner-Goodspeed, V.M.; Gong, M.N.; Cook, D.; Novack, V.; Loring, S.H.; Talmor, D. EPVent-2 Study Group. Effect of Titrating Positive End-Expiratory Pressure (PEEP) with an Esophageal Pressure-Guided Strategy vs an Empirical High PEEP-Fio2 Strategy on Death and Days Free from Mechanical Ventilation Among Patients with Acute Respiratory Distress Syndrome: A Randomized Clinical Trial. JAMA 2019, 321, 846–857. [Google Scholar]
- Hsu, H.J.; Chang, H.T.; Zhao, Z.; Wang, P.H.; Zhang, J.H.; Chen, Y.S.; Frerichs, I.; Möller, K.; Fu, F.; Hsu, H.S.; et al. Positive end-expiratory pressure titration with electrical impedance tomography and pressure-volume curve: A randomized trial in moderate to severe ARDS. Physiol. Meas. 2021, 42, 014002. [Google Scholar]
- Henderson, W.R.; Chen, L.; Amato, M.B.P.; Brochard, L.J. Fifty Years of Research in ARDS. Respiratory Mechanics in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 196, 822–833. [Google Scholar]
- Amato, M.B.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.; Mercat, A.; et al. Driving pressure and survival in the acute respiratory distress syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar]
- Del Sorbo, L.; Goffi, A.; Tomlinson, G.; Pettenuzzo, T.; Facchin, F.; Vendramin, A.; Goligher, E.C.; Cypel, M.; Slutsky, A.S.; Keshavjee, S.; et al. International ECMO Network (ECMONet). Effect of Driving Pressure Change During Extracorporeal Membrane Oxygenation in Adults with Acute Respiratory Distress Syndrome: A Randomized Crossover Physiologic Study. Crit. Care Med. 2020, 48, 1771–1778. [Google Scholar]
- Mauri, T.; Yoshida, T.; Bellani, G.; Goligher, E.C.; Carteaux, G.; Rittayamai, N.; Mojoli, F.; Chiumello, D.; Piquilloud, L.; Grasso, S.; et al. PLeUral pressure working Group (PLUG—Acute Respiratory Failure section of the European Society of Intensive Care Medicine). Esophageal and transpulmonary pressure in the clinical setting: Meaning, usefulness and perspectives. Intensive Care Med. 2016, 42, 1360–1373. [Google Scholar]
- Yoshida, T.; Amato, M.B.P.; Grieco, D.L.; Chen, L.; Lima, C.A.S.; Roldan, R.; Morais, C.C.A.; Gomes, S.; Costa, E.L.V.; Cardoso, P.F.G.; et al. Esophageal Manometry and Regional Transpulmonary Pressure in Lung Injury. Am. J. Respir. Crit. Care Med. 2018, 197, 1018–1026. [Google Scholar]
- Gattinoni, L.; Giosa, L.; Bonifazi, M.; Pasticci, I.; Busana, M.; Macri, M.; Romitti, F.; Vassalli, F.; Quintel, M. Targeting transpulmonary pressure to prevent ventilator-induced lung injury. Expert Rev. Respir. Med. 2019, 13, 737–746. [Google Scholar]
- Florio, G.; Ferrari, M.; Bittner, E.A.; de Santis, S.R.; Pirrone, M.; Fumagalli, J.; Teggia, D.M.; Mietto, C.; Pinciroli, R.; Berg, S.; et al. Investigators of the lung rescue team. A lung rescue team improves survival in obesity with acute respiratory distress syndrome. Crit. Care 2020, 24, 4. [Google Scholar]
- Grasso, S.; Terragni, P.; Birocco, A.; Urbino, R.; del Sorbo, L.; Filippini, C.; Mascia, L.; Pesenti, A.; Zangrillo, A.; Gattinoni, L.; et al. ECMO criteria for influenza A (H1N1)-associated ARDS: Role of transpulmonary pressure. Intensive Care Med. 2012, 38, 395–403. [Google Scholar]
- Wang, R.; Sun, B.; Li, X.; Tang, X.; He, H.; Li, Y.; Yuan, X.; Li, H.; Chu, H.; Tong, Z. Mechanical Ventilation Strategy Guided by Transpulmonary Pressure in Severe Acute Respiratory Distress Syndrome Treated with Venovenous Extracorporeal Membrane Oxygenation. Crit Care Med. 2020, 48, 1280–1288. [Google Scholar]
- Laffey, J.G.; Bellani, G.; Pham, T.; Fan, E.; Madotto, F.; Bajwa, E.K.; Brochard, L.; Clarkson, K.; Esteban, A.; Gattinoni, L.; et al. Potentially modifiable factors contributing to outcome from acute respiratory distress syndrome: The LUNG SAFE study. Intensive Care Med. 2016, 42, 1865–1876. [Google Scholar]
- Quintel, M.; Busana, M.; Gattinoni, L. Breathing and Ventilation during Extracorporeal Membrane Oxygenation: How to Find the Balance between Rest and Load. Am. J. Respir. Crit. Care Med. 2019, 200, 954–956. [Google Scholar]
- McNamee, J.J.; Gillies, M.A.; Barrett, N.A.; Perkins, G.D.; Tunnicliffe, W.; Young, D.; Bentley, A.; Harrison, D.A.; Brodie, D.; Boyle, A.J.; et al. REST Investigators. Effect of Lower Tidal Volume Ventilation Facilitated by Extracorporeal Carbon Dioxide Removal vs Standard Care Ventilation on 90-Day Mortality in Patients with Acute Hypoxemic Respiratory Failure: The REST Randomized Clinical Trial. JAMA 2021, 326, 1013–1023. [Google Scholar]
- Yoshida, T.; Fujino, Y.; Amato, M.B.; Kavanagh, B.P. Fifty Years of Research in ARDS. Spontaneous Breathing during Mechanical Ventilation. Risks, Mechanisms, and Management. Am. J. Respir. Crit. Care Med. 2017, 195, 985–992. [Google Scholar]
- Crotti, S.; Bottino, N.; Ruggeri, G.M.; Spinelli, E.; Tubiolo, D.; Lissoni, A.; Protti, A.; Gattinoni, L. Spontaneous Breathing during Extracorporeal Membrane Oxygenation in Acute Respiratory Failure. Anesthesiology 2017, 126, 678–687. [Google Scholar]
- Brochard, L.; Slutsky, A.; Pesenti, A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am. J. Respir. Crit. Care Med. 2017, 195, 438–442. [Google Scholar]
- Mauri, T.; Grasselli, G.; Suriano, G.; Eronia, N.; Spadaro, S.; Turrini, C.; Patroniti, N.; Bellani, G.; Pesenti, A. Control of Respiratory Drive and Effort in Extracorporeal Membrane Oxygenation Patients Recovering from Severe Acute Respiratory Distress Syndrome. Anesthesiology 2016, 125, 159–167. [Google Scholar]
- Araos, J.; Alegria, L.; Garcia, P.; Cruces, P.; Soto, D.; Erranz, B.; Amthauer, M.; Salomon, T.; Medina, T.; Rodriguez, F.; et al. Near-Apneic Ventilation Decreases Lung Injury and Fibroproliferation in an Acute Respiratory Distress Syndrome Model with Extracorporeal Membrane Oxygenation. Am. J. Respir. Crit. Care Med. 2019, 199, 603–612. [Google Scholar]
- Shekar, K.; McAuley, D.F.; Brodie, D. Will Not Breathing on Extracorporeal Membrane Oxygenation Help One Survive Acute Respiratory Distress Syndrome? Crit. Care Med. 2020, 48, 1901–1904. [Google Scholar]
- Boyle, A.J.; Sklar, M.C.; McNamee, J.J.; Brodie, D.; Slutsky, A.S.; Brochard, L.; McAuley, D.F. International ECMO Network (ECMONet). Extracorporeal carbon dioxide removal for lowering the risk of mechanical ventilation: Research questions and clinical potential for the future. Lancet Respir. Med. 2018, 6, 874–884. [Google Scholar]
- Combes, A.; Pesenti, A.; Ranieri, V.M. Fifty Years of Research in ARDS. Is Extracorporeal Circulation the Future of Acute Respiratory Distress Syndrome Management? Am. J. Respir. Crit. Care Med. 2017, 195, 1161–1170. [Google Scholar]
- Ficial, B.; Vasques, F.; Zhang, J.; Whebell, S.; Slattery, M.; Lamas, T.; Daly, K.; Agnew, N.; Camporota, L. Physiological Basis of Extracorporeal Membrane Oxygenation and Extracorporeal Carbon Dioxide Removal in Respiratory Failure. Membranes 2021, 11, 225. [Google Scholar]
- Giani, M.; Redaelli, S.; Siragusa, A.; Fumagalli, B.; Rona, R.; Foti, G. Extracorporeal Gas Exchange for Acute Respiratory Distress Syndrome: Open Questions, Controversies and Future Directions. Membranes 2021, 11, 172. [Google Scholar]
- Grasso, S.; Stripoli, T.; Mazzone, P.; Pezzuto, M.; Lacitignola, L.; Centonze, P.; Guarracino, A.; Esposito, C.; Herrmann, P.; Quintel, M.; et al. Low respiratory rate plus minimally invasive extracorporeal CO2 removal decreases systemic and pulmonary inflammatory mediators in experimental acute respiratory distress syndrome. Crit. Care Med. 2014, 42, e451–e460. [Google Scholar]
- Combes, A.; Fanelli, V.; Pham, T.; Ranieri, V.M. European Society of Intensive Care Medicine Trials Group and the “Strategy of Ultra-Protective lung ventilation with Extracorporeal CO2 Removal for New-Onset moderate to severe ARDS” (SUPERNOVA) investigators. Feasibility and safety of extracorporeal CO2 removal to enhance protective ventilation in acute respiratory distress syndrome: The SUPERNOVA study. Intensive Care Med. 2019, 45, 592–600. [Google Scholar]
- Goligher, E.C.; Combes, A.; Brodie, D.; Ferguson, N.D.; Pesenti, A.M.; Ranieri, V.M.; Slutsky, A.S. SUPERNOVA investigators (European Society of Intensive Care Medicine trials group) and for the International ECMO Network (ECMONet). Determinants of the effect of extracorporeal carbon dioxide removal in the SUPERNOVA trial: Implications for trial design. Intensive Care Med. 2019, 45, 1219–1230. [Google Scholar]
- Giraud, R.; Banfi, C.; Assouline, B.; de Charrière, A.; Cecconi, M.; Bendjelid, K. The use of extracorporeal CO2 removal in acute respiratory failure. Ann. Intensive Care 2021, 11, 43. [Google Scholar]
- Fitzgerald, M.; Millar, J.; Blackwood, B.; Davies, A.; Brett, S.J.; McAuley, D.F.; McNamee, J.J. Extracorporeal carbon dioxide removal for patients with acute respiratory failure secondary to the acute respiratory distress syndrome: A systematic review. Crit. Care 2014, 18, 222. [Google Scholar]
- Barbaro, R.P.; Odetola, F.O.; Kidwell, K.M.; Paden, M.L.; Bartlett, R.H.; Davis, M.M.; Annich, G.M. Association of hospital-level volume of extracorporeal membrane oxygenation cases and mortality. Analysis of the extracorporeal life support organization registry. Am. J. Respir. Crit. Care Med. 2015, 191, 894–901. [Google Scholar]



{kind=link}
{kind=link}
| Studies | Study Design | Main Results |
|---|---|---|
| Pham et al., 2013 [18] (n = 123) | Retrospective observational study | ICU mortality: 35.8% Higher plateau pressure on the first day under ECMO was independently associated with ICU mortality (OR 1.33, p < 0.01) |
| Schmidt et al., 2015 [20] (n = 168) | Retrospective study | ICU mortality: 29% Higher PEEP during the first 3 days of ECMO was independently associated with lower mortality (OR 0.75, p = 0.0006) |
| Marhong et al., 2015 [16] (n = 2042) | Systematic review | Median (IQR) overall mortality: 41% (31–51%) Mortality was lower in patients receiving lower intensity of applied ventilation during ECMO. Combined tidal volume ≤ 4 mL/kg PBW and plateau pressure ≤ 26 cmH2O during ECMO had lowest mortality |
| Modrykamien et al., 2016 [19] (n = 64) | Retrospective observational study | Hospital mortality: 46.9% Increased plateau pressure was independently associated with decreased odds of hospital survival (OR 0.79, p = 0.007) |
| Neto et al., 2016 [21] (n = 545) | Individual patient data meta-analysis of observational studies | In-hospital mortality: 35.2% Driving pressure was the only ventilatory parameter during ECMO that was independently associated with in-hospital mortality (adjusted HR 1.06, p < 0.001) |
| Kim et al., 2019 [29] (n = 56) | Retrospective study | Hospital mortality: 48.1% Lung compliance during ECMO was significantly associated with 6-month mortality (HR 0.943, p = 0.009) |
| Schmidt et al., 2019 [26] (n = 350) | International prospective cohort study | Six-month mortality: 39% MV settings during the first 2 days of ECMO did not impact the prognosis |
| Chiu et al., 2021 [17] (n = 152) | Retrospective study | Hospital mortality: 53.3% MP during the first 3 days of ECMO was the only ventilatory variable independently associated with 90-day hospital mortality, and MP referenced to compliance had the greatest predictive value for mortality compared to MP alone (adjusted HR 2.289, p = 0.010) |
| Trials/Organization/Consensus | Mechanical Ventilator Settings |
|---|---|
| CESAR trial, 2009 [12] | Pressure-controlled ventilation Peak inspiratory pressure 20–25 cmH2O PEEP 10–15 cmH2O RR 10 breaths per minute FiO2 0.3 |
| ELSO guideline, 2017 [30] | First 24 h: moderate to heavy sedation Pressure-controlled ventilation 25 cmH2O, PEEP 15 cmH2O (PEEP can be as high as tolerated and avoid inhibition of venous return), plateau pressure < 25 cmH2O, inspiratory/expiratory ratio 2:1, RR 5 breaths per minute, FiO2 0.5 After 24–48 h: moderate to minimal sedation Pressure-controlled ventilation 20 cmH2O, PEEP 10 cmH2O, Inspiratory/expiratory ratio 2:1, RR 5 breaths per minute plus spontaneous breaths, FiO2 0.2–0.4 After 48 h: minimal to no sedation Pressure-controlled ventilation as above or CPAP 20 cmH2O plus spontaneous breathing Tracheostomy or extubation within 3–5 days |
| EOLIA trial, 2018 [13] | Volume-assist control mode: Plateau pressure ≤ 24 cmH2O Tidal volume lowered to obtain plateau pressure ≤ 24 cmH2O PEEP ≥ 10 cmH2O RR 10–30 breaths per minute FiO2 0.3–0.5 Airway pressure release ventilation: High pressure ≤ 24 cmH2O PEEP ≥ 10 cmH2O RR 10–30 breaths per minute FiO2: 0.3–0.5 |
| ECMONet expert opinions’ consensus conference, 2018 [27] * | Plateau pressure ≤ 24 cmH2O and may be lower if feasible Tidal volume: typically ≤4 mL/kg PBW, often much lower and adjusted for the goal of plateau pressure PEEP ≥ 10 cmH2O Driving pressure ≤ 14 cmH2O RR ≤ 10 breaths per minute FiO2: 0.3–0.5 |
| Mechanical Ventilator Settings | Target |
|---|---|
| Plateau pressure | ≤24 cmH2O and may be lower if feasible |
| PEEP | ≥10 cmH2O |
| Driving pressure | ≤14 cmH2O |
| Tidal volume | Typically ≤4 mL/kg PBW and adjusted for the goal of plateau pressure (≤24 cmH2O) |
| Respiratory rate | ≤10 breaths per minute |
| FiO2 | 0.3–0.5 |
| Trial Names (Identifier, Status) | Inclusion Criteria | Interventional Group | Control Group | Primary Outcomes |
|---|---|---|---|---|
| New Lung Ventilation Strategies Guided by Transpulmonary Pressure in VV-ECMO for Severe ARDS (NCT02439151, published [50]) | ARDS with reversible cause (PaO2/FiO2 < 80) | Transpulmonary pressure guide new lung ventilation strategy in ECMO for severe ARDS patients | Conventional ventilation strategy (ELSO guide ventilation strategy) in ECMO for severe ARDS patients | Proportion weaned from VV-ECMO |
| pRotective vEntilation With Veno-venouS Lung assisT in Respiratory Failure (REST) (NCT02654327, published [53]) | Invasive MV within 48 h of acute potentially reversible hypoxemic respiratory failure (PaO2/FiO2 ≤ 150 mmHg) receiving PEEP ≥ 5 cmH2O | VV-ECCO2R: Plateau pressure ≤ 25 cmH2O Target tidal volume ≤ 3 mL/kg PBW | Standard care: Conventional lung protective mechanical ventilation | All causes of mortality at day 90 |
| Low frequency, ultra-low tidal volume ventilation in patients with ARDS and ECMO (NCT03764319, recruiting) | Moderate to severe ARDS ECMO < 24 h in situ | Ultra-protective ventilator settings: Plateau pressure 23–25 cmH2O, tidal volume < 4 mL/kg PBW, PEEP 14–16 cmH2O, RR 4–5 bpm | Standard ventilator settings: Plateau pressure ≤ 35 cmH2O PEEP 8–12 cmH2O, RR 12–15 bpm | Ventilator-free days at day 28 |
| Biomarkers, Genomics, Physiology in Critically Ill and ECMO Patients (IGNITE) (NCT04669444, enrolling by invitation) | Patient with ARDS supported with ECMO or a potential ECMO candidate A single interventional group | Low Driving Pressure Protocol: Initial driving pressure of 10–15 cmH2O and then decreased as tolerated for 2 h to evaluate the effects on pulmonary, cardiac, and inflammatory biomarkers | None | Change in plasma interleukin-6 level from baseline to low driving pressure ventilation |
| Ultra-Low Tidal Volume Mechanical Ventilation in ARDS Through ECMO (ULTIMATE) (NCT04832789, not yet recruiting) | Age ≥ 18 years Endotracheal mechanical ventilation ≤ 5 days Early moderate-severe ARDS | Ultra-protective ventilation with VV ECMO | Best conventional ventilation | Proportion of patients adhering to the study protocol and crossing over to VV ECMO Number of patients recruited for the study |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiu, L.-C.; Kao, K.-C. Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review. J. Clin. Med. 2021, 10, 4953. https://doi.org/10.3390/jcm10214953
Chiu L-C, Kao K-C. Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review. Journal of Clinical Medicine. 2021; 10(21):4953. https://doi.org/10.3390/jcm10214953
Chicago/Turabian StyleChiu, Li-Chung, and Kuo-Chin Kao. 2021. "Mechanical Ventilation during Extracorporeal Membrane Oxygenation in Acute Respiratory Distress Syndrome: A Narrative Review" Journal of Clinical Medicine 10, no. 21: 4953. https://doi.org/10.3390/jcm10214953