
The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vivo Sepsis Model Induction
2.2. Colony Forming Unit (CFU) Assay
2.3. Bacterial Isolation
2.4. Lactate Assay
2.5. ALT and Creatinine
2.6. Cytokine Measurements
2.7. Assessment of Plasma Levels of Reactive Oxygen Species (ROS)
2.8. Ex vivo Peripheral Blood Mononuclear Cell (PBMC) Stimulation with LPS
2.9. Statistical Analysis
3. Results
3.1. Effects of Different Antibiotics in the Rat Intra-abdominal Infection (IAI) Model
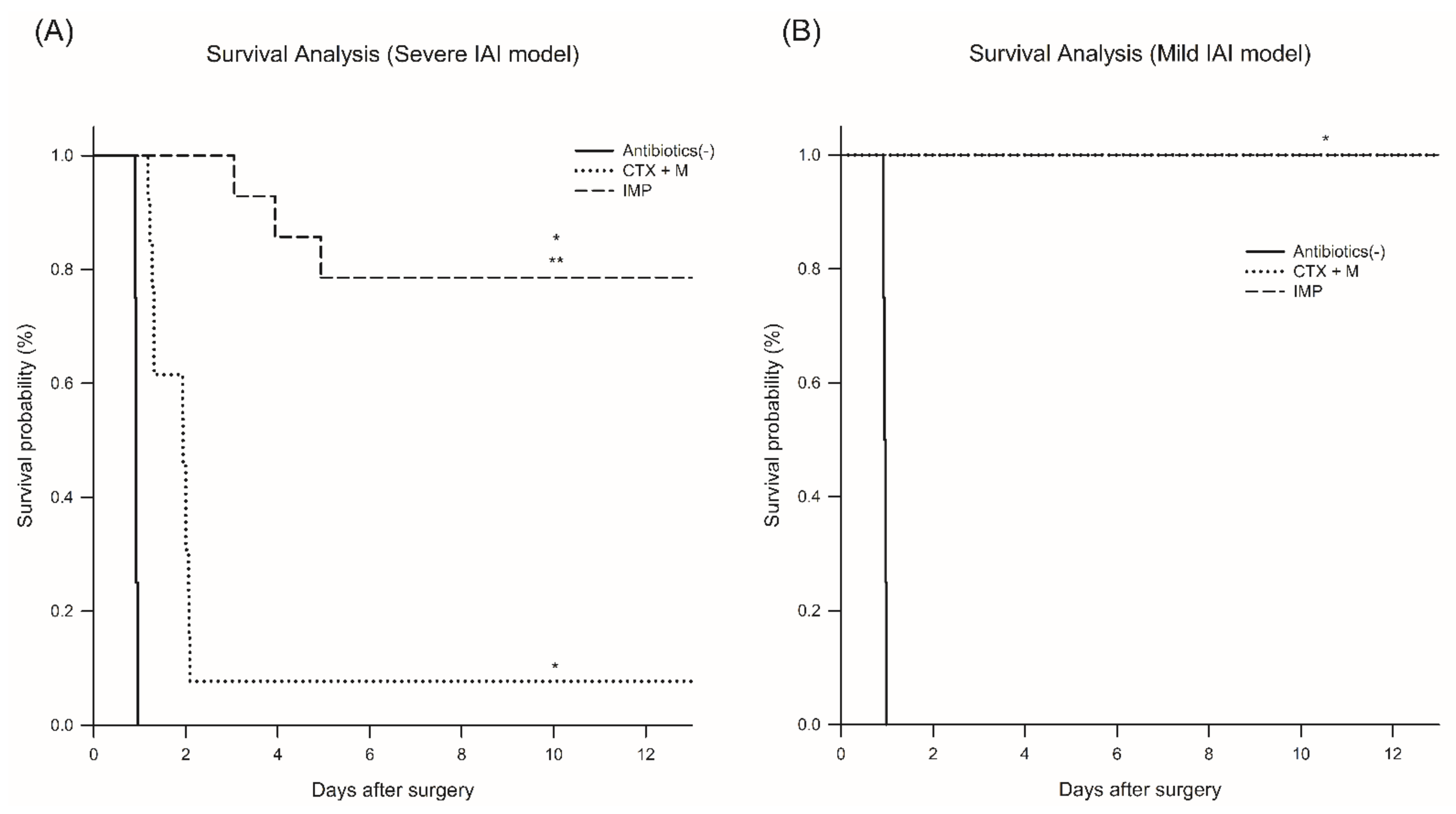
3.1.1. Survival Rate and Plasma Lactate Levels
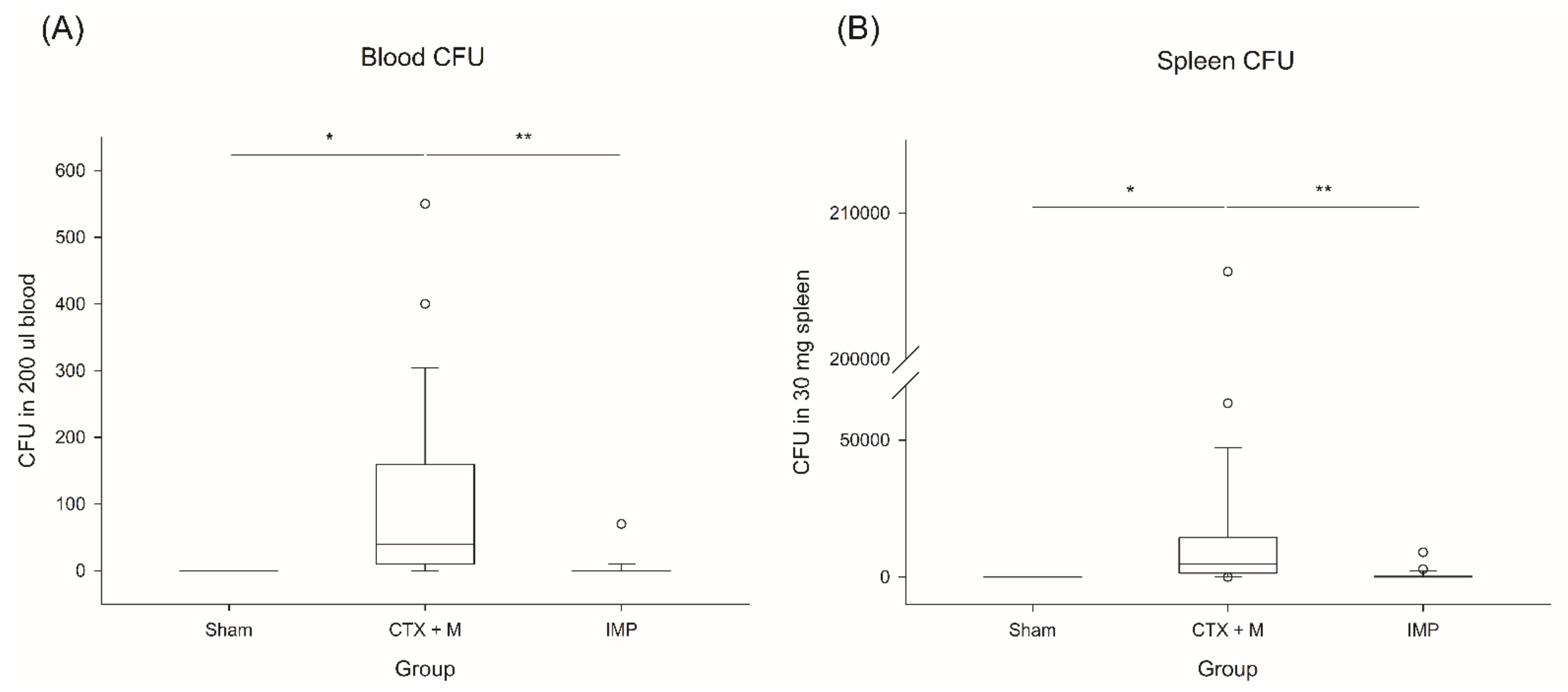
3.1.2. Bacterial Isolation and CFU
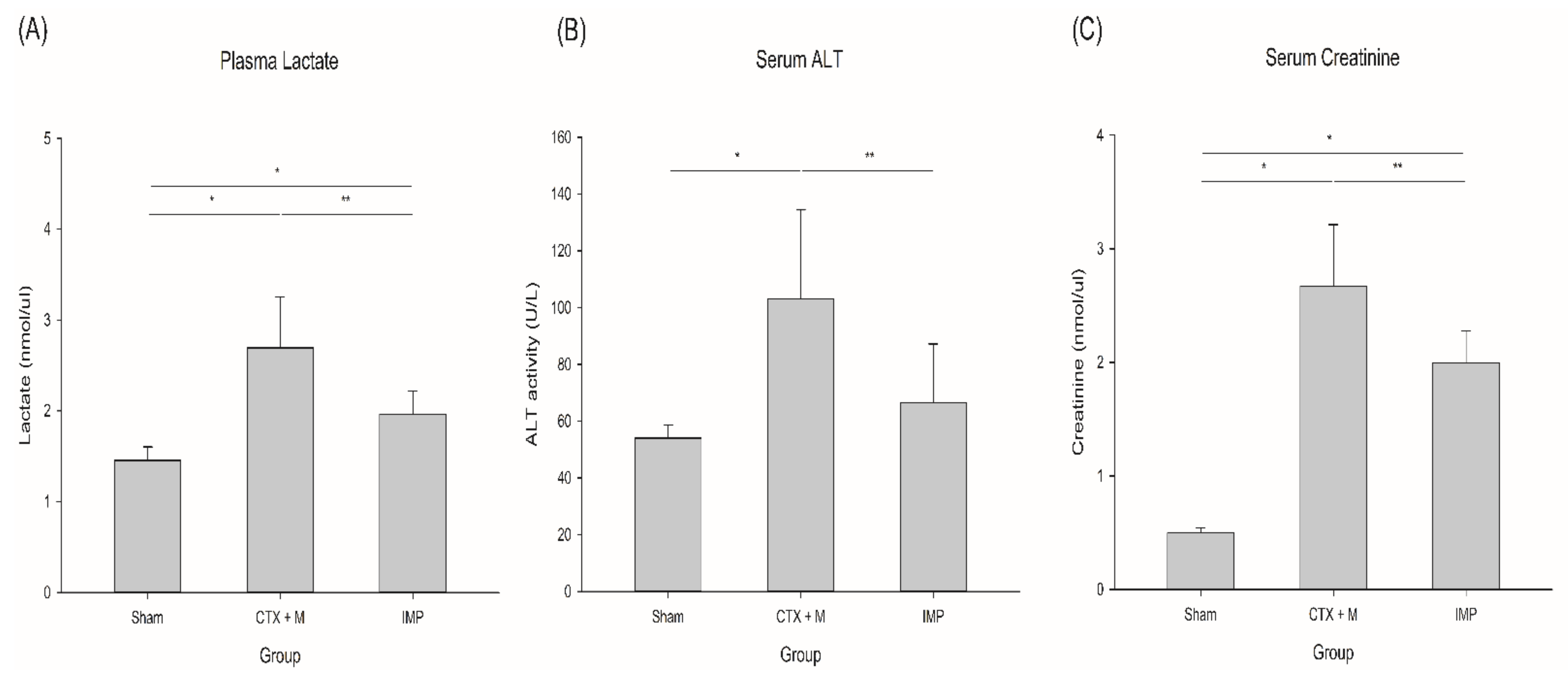
3.1.3. Lactate, Alanine Aminotransferase (ALT), and Creatinine
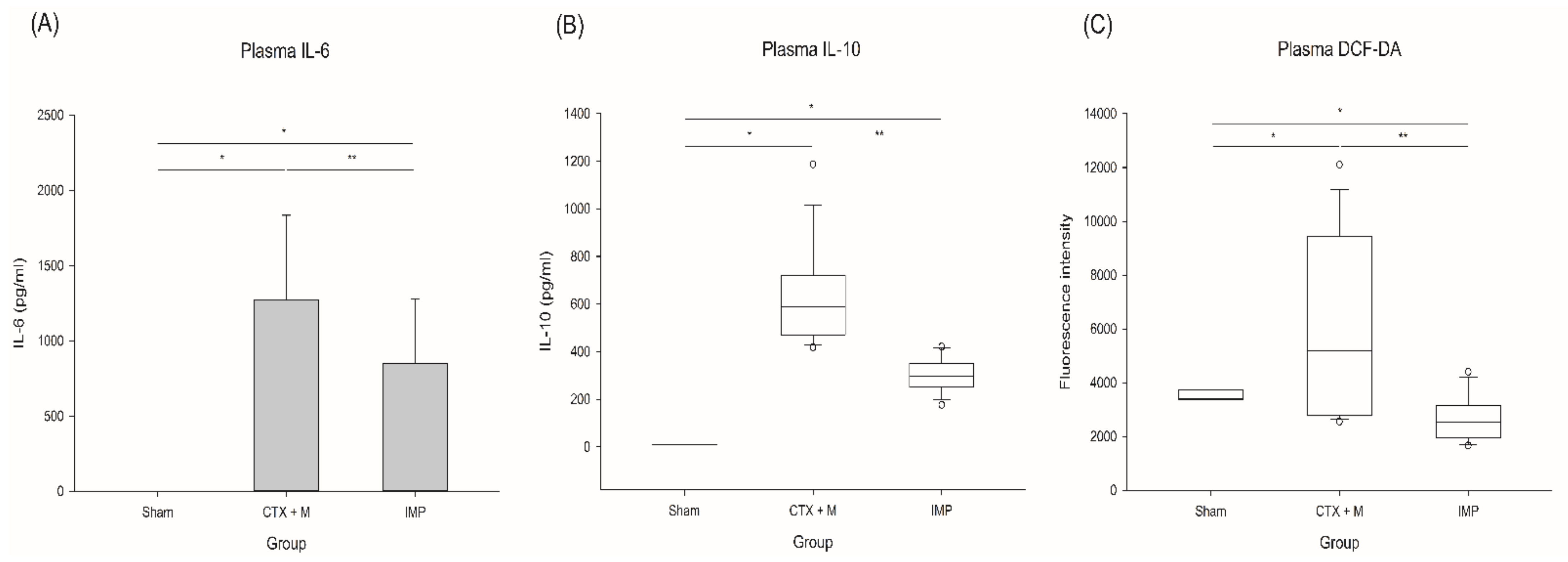
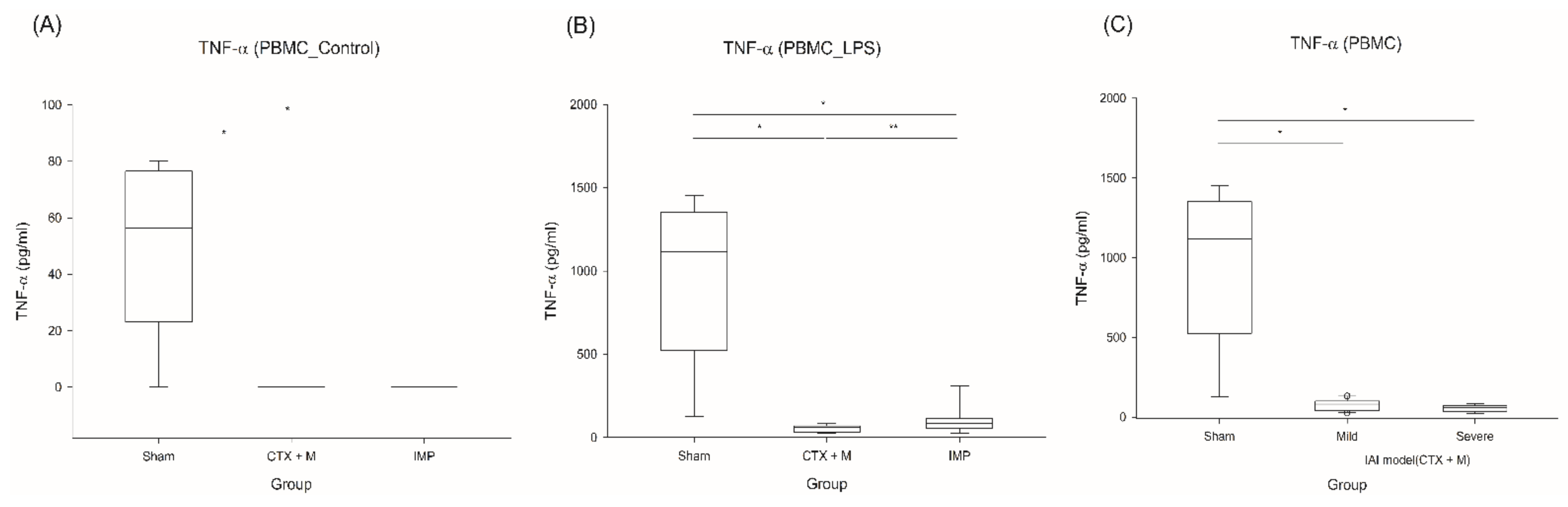
3.1.4. Cytokines
3.1.5. Reactive Oxygen Species (ROS)
3.2. Immune Suppression Effect of IAI Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Brun-Buisson, C.; Doyon, F.; Carlet, J.; Dellamonica, P.; Gouin, F.; Lepoutre, A.; Mercier, J.C.; Offenstadt, G.; Regnier, B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA 1995, 274, 968–974. [Google Scholar] [CrossRef]
- DeFrances, C.J.; Cullen, K.A.; Kozak, L.J. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat. 2007, 13, 1–209. [Google Scholar]
- Solomkin, J.S.; Mazuski, J.E.; Bradley, J.S.; Rodvold, K.A.; Goldstein, E.J.; Baron, E.J.; O’Neill, P.J.; Chow, A.W.; Dellinger, E.P.; Eachempati, S.R.; et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 133–164. [Google Scholar] [CrossRef] [Green Version]
- Mazuski, J.E.; Tessier, J.M.; May, A.K.; Sawyer, R.G.; Nadler, E.P.; Rosengart, M.R.; Chang, P.K.; O’Neill, P.J.; Mollen, K.P.; Huston, J.M.; et al. The Surgical Infection Society Revised Guidelines on the Management of Intra-Abdominal Infection. Surg. Infect. 2017, 18, 1–76. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Kim, K.; Jo, Y.H.; Lee, J.H.; Hwang, J.E. Dose-dependent mortality and organ injury in a cecal slurry peritonitis model. J. Surg. Res. 2016, 206, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, K.; Jo, Y.H.; Hwang, J.E.; Chung, H.J.; Yang, C. Reoxygenation speed and its implication for cellular injury responses in hypoxic RAW 264.7 cells. J. Surg. Res. 2018, 227, 88–94. [Google Scholar] [CrossRef]
- Posel, C.; Moller, K.; Frohlich, W.; Schulz, I.; Boltze, J.; Wagner, D.C. Density gradient centrifugation compromises bone marrow mononuclear cell yield. PLoS ONE 2012, 7, e50293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomkin, J.S.; Reinhart, H.H.; Dellinger, E.P.; Bohnen, J.M.; Rotstein, O.D.; Vogel, S.B.; Simms, H.H.; Hill, C.S.; Bjornson, H.S.; Haverstock, D.C.; et al. Results of a randomized trial comparing sequential intravenous/oral treatment with ciprofloxacin plus metronidazole to imipenem/cilastatin for intra-abdominal infections. The Intra-Abdominal Infection Study Group. Ann. Surg. 1996, 223, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.S.; Wilson, S.E.; Christou, N.V.; Rotstein, O.D.; Dellinger, E.P.; Bennion, R.S.; Pak, R.; Tack, K. Results of a clinical trial of clinafloxacin versus imipenem/cilastatin for intraabdominal infections. Ann. Surg. 2001, 233, 79–87. [Google Scholar] [CrossRef]
- Solomkin, J.S.; Yellin, A.E.; Rotstein, O.D.; Christou, N.V.; Dellinger, E.P.; Tellado, J.M.; Malafaia, O.; Fernandez, A.; Choe, K.A.; Carides, A.; et al. Protocol 017 Study, Ertapenem versus piperacillin/tazobactam in the treatment of complicated intraabdominal infections: Results of a double-blind, randomized comparative phase III trial. Ann. Surg. 2003, 237, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Goh, H.M.S.; Yong, M.H.A.; Chong, K.K.L.; Kline, K.A. Model systems for the study of Enterococcal colonization and infection. Virulence 2017, 8, 1525–1562. [Google Scholar] [CrossRef] [Green Version]
- Sava, I.G.; Heikens, E.; Huebner, J. Pathogenesis and immunity in enterococcal infections. Clin. Microbiol. Infect. 2010, 16, 533–540. [Google Scholar] [CrossRef]
- Eshaghi, A.; Shahinas, D.; Li, A.; Kariyawasam, R.; Banh, P.; Desjardins, M.; Melano, R.G.; Patel, S.N. Characterization of an Enterococcus gallinarum Isolate Carrying a Dual vanA and vanB Cassette. J. Clin. Microbiol. 2015, 53, 2225–2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dargere, S.; Vergnaud, M.; Verdon, R.; Saloux, E.; le Page, O.; Leclercq, R.; Bazin, C. Enterococcus gallinarum endocarditis occurring on native heart valves. J. Clin. Microbiol. 2002, 40, 2308–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corso, A.; Faccone, D.; Gagetti, P.; Togneri, A.; Lopardo, H.; Melano, R.; Rodriguez, V.; Rodriguez, M.; Galas, M. First report of VanA Enterococcus gallinarum dissemination within an intensive care unit in Argentina. Int. J. Antimicrob. Agents 2005, 25, 51–56. [Google Scholar] [CrossRef]
- Reid, K.C.; Cockerill, I.F.; Patel, R. Clinical and epidemiological features of Enterococcus casseliflavus/flavescens and Enterococcus gallinarum bacteremia: A report of 20 cases. Clin. Infect. Dis. 2001, 32, 1540–1546. [Google Scholar] [CrossRef]
- Contreras, G.A.; DiazGranados, C.A.; Cortes, L.; Reyes, J.; Vanegas, S.; Panesso, D.; Rincon, S.; Diaz, L.; Prada, G.; Murray, B.E.; et al. Nosocomial outbreak of Enteroccocus gallinarum: Untaming of rare species of enterococci. J. Hosp. Infect. 2008, 70, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.K.; Lai, C.C.; Wang, J.Y.; Lin, S.H.; Liao, C.H.; Huang, Y.T.; Wang, C.Y.; Lin, H.I.; Hsueh, P.R. Bacteremia caused by non-faecalis and non-faecium enterococcus species at a Medical center in Taiwan, 2000 to 2008. J. Infect. 2010, 61, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Fattahi, F.; Ward, P.A. Understanding Immunosuppression after Sepsis. Immunity 2017, 47, 3–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-induced immunosuppression: From cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef]
- Calvano, S.E.; Xiao, W.; Richards, D.R.; Felciano, R.M.; Baker, H.V.; Cho, R.J.; Chen, R.O.; Brownstein, B.H.; Cobb, J.P.; Tschoeke, S.K.; et al. Host Response to Injury Large Scale Collab. Res, A network-based analysis of systemic inflammation in humans. Nature 2005, 437, 1032–1037. [Google Scholar] [CrossRef]
- Otto, G.P.; Sossdorf, M.; Claus, R.A.; Rodel, J.; Menge, K.; Reinhart, K.; Bauer, M.; Riedemann, N.C. The late phase of sepsis is characterized by an increased microbiological burden and death rate. Crit. Care 2011, 15, R183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pena, O.M.; Hancock, D.G.; Lyle, N.H.; Linder, A.; Russell, J.A.; Xia, J.; Fjell, C.D.; Boyd, J.H.; Hancock, R.E. An Endotoxin Tolerance Signature Predicts Sepsis and Organ Dysfunction at Initial Clinical Presentation. EBioMedicine 2014, 1, 64–71. [Google Scholar]
- Schefold, J.C.; Hasper, D.; Volk, H.D.; Reinke, P. Sepsis: Time has come to focus on the later stages. Med. Hypotheses 2008, 71, 203–208. [Google Scholar] [CrossRef]
- Osuchowski, M.F.; Welch, K.; Siddiqui, J.; Remick, D.G. Circulating cytokine/inhibitor profiles reshape the understanding of the SIRS/CARS continuum in sepsis and predict mortality. J. Immunol. 2006, 177, 1967–1974. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.P.; Chen, C.K.; Chung, K.; Tseng, J.C.; Hua, C.C.; Liu, Y.C.; Chuang, D.Y.; Yang, C.H. Serial cytokine levels in patients with severe sepsis. Inflamm. Res. 2009, 58, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, R.S.; Moldawer, L.L.; Opal, S.M.; Reinhart, K.; Turnbull, I.R.; Vincent, J.L. Sepsis and septic shock. Nat. Rev. Dis. Primers 2016, 2, 16045. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2.5 CTX + M | 2.5 IMP | 5.5 CTX + M | 5.5 IMP | p-value | |
|---|---|---|---|---|---|
| Enterococcus (-) | 2 | 6 | 0 | 3 | 0.00482 |
| Enterococcus (+) | 4 | 0 | 6 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, M.J.; Chung, T.N.; B., Y.J.P.; Lee, H.A.R.; Lee, J.H.; Yune, C.J.; Bae, J.; Mun, S.; Park, J.S.; Kim, K. The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study. J. Clin. Med. 2021, 10, 1027. https://doi.org/10.3390/jcm10051027
Lee MJ, Chung TN, B. YJP, Lee HAR, Lee JH, Yune CJ, Bae J, Mun S, Park JS, Kim K. The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study. Journal of Clinical Medicine. 2021; 10(5):1027. https://doi.org/10.3390/jcm10051027
Chicago/Turabian StyleLee, Min Ji, Tae Nyoung Chung, Ye Jin Park B., Han A. Reum Lee, Jung Ho Lee, Chang June Yune, Jinkun Bae, Sehwan Mun, Jeong Su Park, and Kyuseok Kim. 2021. "The Need of Enterococcal Coverage in Severe Intra-Abdominal Infection: Evidence from Animal Study" Journal of Clinical Medicine 10, no. 5: 1027. https://doi.org/10.3390/jcm10051027