Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study



 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Bio-ADM Measurement
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Banerjee, A.; Pasea, L.; Harris, S.; Gonzalez-Izquierdo, A.; Torralbo, A.; Shallcross, L.; Noursadeghi, M.; Pillay, D.; Sebire, N.; Holmes, C.; et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: A population-based cohort study. Lancet 2020, 395, 1715–1725. [Google Scholar] [CrossRef]
- Dreher, M.; Kersten, A.; Bickenbach, J.; Balfanz, P.; Hartmann, B.; Cornelissen, C.; Daher, A.; Stöhr, R.; Kleines, M.; Lemmen, S.W.; et al. The Characteristics of 50 hospitalized COVID-19 patients with and without ARDS. Dtsch. Aerzteblatt Online 2020, 117, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Aboughdir, M.; Kirwin, T.; Khader, A.A.; Wang, B. Prognostic value of cardiovascular biomarkers in COVID-19: A review. Viruses 2020, 12, 527. [Google Scholar] [CrossRef] [PubMed]
- Guzik, T.J.; Mohiddin, S.A.; DiMarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- Kermali, M.; Khalsa, R.K.; Pillai, K.; Ismail, Z.; Harky, A. The role of biomarkers in diagnosis of COVID-19—A systematic review. Life Sci. 2020, 254, 117788. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair allocation of scarce medical resources in the time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Li, T. COVID-19: Towards understanding of pathogenesis. Cell Res. 2020, 30, 367–369. [Google Scholar] [CrossRef]
- Elke, G.; Bloos, F.; Wilson, D.C.; Brunkhorst, F.M.; Briegel, J.; Reinhart, K.; Loeffler, M.; Kluge, S.; Nierhaus, A.; Jaschinski, U.; et al. The use of mid-regional proadrenomedullin to identify disease severity and treatment response to sepsis—A secondary analysis of a large randomised controlled trial. Crit. Care 2018, 22, 79. [Google Scholar] [CrossRef]
- Wilson, D.C.; Schefold, J.C.; Baldirà, J.; Spinetti, T.; Saeed, K.; Elke, G. Adrenomedullin in COVID-19 induced endotheliitis. Crit. Care 2020, 24, 1–2. [Google Scholar] [CrossRef]
- Hinson, J.P.; Kapas, S.; Smith, D.M. Adrenomedullin, a multifunctional regulatory peptide. Endocr. Rev. 2000, 21, 138–167. [Google Scholar] [CrossRef]
- Schönauer, R.; Els-Heindl, S.; Beck-Sickinger, A.G. Adrenomedullin—New perspectives of a potent peptide hormone. J. Pept. Sci. 2017, 23, 472–485. [Google Scholar] [CrossRef]
- Kitamura, K.; Kangawa, K.; Kawamoto, M.; Ichiki, Y.; Nakamura, S.; Matsuo, H.; Eto, T. Adrenomedullin: A novel hypotensive peptide isolated from human pheochromocytoma. Biochem. Biophys. Res. Commun. 1993, 192, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Sakata, J.; Shimokubo, T.; Kitamura, K.; Nakamura, S.; Kangawa, K.; Matsuo, H.; Eto, T. Molecular cloning and biological activities of rat adrenomedullin, a hypotensive peptide. Biochem. Biophys. Res. Commun. 1993, 195, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Libby, P.; Lüscher, T. COVID-19 is, in the end, an endothelial disease. Eur. Heart J. 2020, 41, 3038–3044. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Weber, J.; Sachse, J.; Bergmann, S.; Sparwaßer, A.; Struck, J.; Bergmann, A. Sandwich immunoassay for bioactive plasma adrenomedullin. J. Appl. Lab. Med. 2017, 2, 222–233. [Google Scholar] [CrossRef]
- Van Lier, D.; Kox, M.; Pickkers, P. Promotion of vascular integrity in sepsis through modulation of bioactive adrenomedullin and dipeptidyl peptidase 3. J. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Karakas, M.; Jarczak, D.; Becker, M.; Roedl, K.; Addo, M.M.; Hein, F.; Bergmann, A.; Zimmermann, J.; Simon, T.-P.; Marx, G.; et al. Targeting endothelial dysfunction in eight extreme-critically ill patients with covid-19 using the anti-adrenomedullin antibody adrecizumab (ham8101). Biomolecules 2020, 10, 1171. [Google Scholar] [CrossRef]
- Geven, C.; Bergmann, A.; Kox, M.; Pickkers, P. Vascular effects of adrenomedullin and the anti-adrenomedullin antibody adrecizumab in sepsis. Shock 2018, 50, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Geven, C.; Hollinger, A.; Wittebole, X.; Chousterman, B.G.; Blet, A.; Gayat, E.; Hartmann, O.; Scigalla, P.; Struck, J.; et al. Circulating adrenomedullin estimates survival and reversibility of organ failure in sepsis: The prospective observational multinational adrenomedullin and outcome in sepsis and septic shock-1 (AdrenOSS-1) study. Crit. Care 2018, 22, 1–12. [Google Scholar] [CrossRef]
- Caironi, P.; Latini, R.; Struck, J.; Hartmann, O.; Bergmann, A.; Maggio, G.; Cavana, M.; Tognoni, G.; Pesenti, A.; Gattinoni, L.; et al. Circulating biologically active adrenomedullin (bio-ADM) predicts hemodynamic support requirement and mortality during sepsis. Chest 2017, 152, 312–320. [Google Scholar] [CrossRef]
- Spadaro, S.; Park, M.; Turrini, C.; Tunstall, T.; Thwaites, R.; Mauri, T.; Ragazzi, R.; Ruggeri, P.; Hansel, T.T.; Caramori, G.; et al. Biomarkers for acute respiratory distress syndrome and prospects for personalised medicine. J. Inflamm. 2019, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The berlin definition. JAMA 2012, 307, 2526–2533. [Google Scholar]
- Bartlett, R.H.; Ogino, M.T.; Brodie, D.; McMullan, D.M.; Lorusso, R.; MacLaren, G.; Stead, C.M.; Rycus, P.; Fraser, J.F.; Belohlavek, J.; et al. Initial ELSO guidance document: ECMO for COVID-19 patients with severe cardiopulmonary failure. ASAIO J. 2020, 66, 472–474. [Google Scholar] [CrossRef]
- Marino, R.; Struck, J.; Maisel, A.S.; Magrini, L.; Bergmann, A.; Di Somma, S. Plasma adrenomedullin is associated with short-term mortality and vasopressor requirement in patients admitted with sepsis. Crit. Care 2014, 18, R34. [Google Scholar] [CrossRef]
- Blet, A.; de Roquetaillade, C.; Hartmann, O.; Struck, J.; Mebazaa, A.; Chousterman, B.G. Added value of serial bio-adrenomedullin measurement in addition to lactate for the prognosis of septic patients admitted to ICU. Crit. Care 2020, 24, 1–6. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Murthy, S.; Gomersall, C.D.; Fowler, R.A. Care for critically Ill patients with COVID-19. JAMA 2020, 323, 1499. [Google Scholar] [CrossRef] [PubMed]
- Caron, K.M.; Smithies, O. Extreme Hydrops Fetalis and Cardiovascular Abnormalities in Mice Lacking a Functional Adrenomedullin Gene. Proc. Natl. Acad. Sci. USA 2001, 98, 615–619. [Google Scholar] [CrossRef]
- Lundberg, O.H.M.; Lengquist, M.; Spångfors, M.; Annborn, M.; Bergmann, D.; Schulte, J.; Levin, H.; Melander, O.; Frigyesi, A.; Friberg, H. Circulating bioactive adrenomedullin as a marker of sepsis, septic shock and critical illness. Crit. Care 2020, 24, 1–10. [Google Scholar] [CrossRef]
- Voors, A.A.; Kremer, D.; Geven, C.; Ter Maaten, J.M.; Struck, J.; Bergmann, A.; Pickkers, P.; Metra, M.; Mebazaa, A.; Düngen, H.-D.; et al. Adrenomedullin in heart failure: Pathophysiology and therapeutic application. Eur. J. Heart Fail. 2019, 21, 163–171. [Google Scholar] [CrossRef]
- Tolppanen, H.; Rivas-Lasarte, M.; Lassus, J.; Sans-Roselló, J.; Hartmann, O.; Lindholm, M.; Arrigo, M.; Tarvasmäki, T.; Köber, L.; Thiele, H.; et al. Adrenomedullin: A marker of impaired hemodynamics, organ dysfunction, and poor prognosis in cardiogenic shock. Ann. Intensiv. Care 2017, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ferrario, C.M.; Jessup, J.; Chappell, M.C.; Averill, D.B.; Brosnihan, K.B.; Tallant, E.A.; Diz, D.I.; Gallagher, P.E. Effect of angiotensin-converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin-converting enzyme 2. Circulation 2005, 111, 2605–2610. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Koczera, P.; Zechendorf, E.; Schuerholz, T. The endothelial glycocalyx: New diagnostic and therapeutic approaches in sepsis. BioMed Res. Int. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Joffre, J.; Hellman, J.; Ince, C.; Ait-Oufella, H. Endothelial responses in sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, Z.; Yu, M.; Tao, Y.; Xie, M. 15-day mortality and associated risk factors for hospitalized patients with COVID-19 in Wuhan, China: An ambispective observational cohort study. Intensiv. Care Med. 2020, 46, 1472–1474. [Google Scholar] [CrossRef]
- Paulus, P.; Jennewein, C.; Zacharowski, K. Biomarkers of Endothelial Dysfunction: Can They Help Us Deciphering Systemic Inflammation and Sepsis? Biomarkers 2011, 16, S11–S21. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Tu, L.; Zhu, P.; Mu, M.; Wang, R.; Yang, P.; Wang, X.; Hu, C.; Ping, R.; Hu, P.; et al. Clinical features of 85 fatal cases of covid-19 from Wuhan: A retrospective observational study. Am. J. Respir. Crit. Care Med. 2020. [Google Scholar] [CrossRef]
- Deng, Y.; Liu, W.; Liu, K.; Fang, Y.Y.; Shang, J.; Zhou, L.; Wang, K.; Leng, F.; Wei, S.; Chen, L.; et al. Clinical characteristics of fatal and recovered cases of coronavirus disease 2019 (covid-19) in Wuhan, China: A retrospective study. Chin. Med. J. 2020, 133, 1261–1267. [Google Scholar] [CrossRef]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M. Procalcitonin in patients with severe coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chim. Acta 2020, 505, 190–191. [Google Scholar] [CrossRef] [PubMed]
- Hodges, G.; Pallisgaard, J.; Olsen, A.-M.S.; Mcgettigan, P.; Andersen, M.; Krogager, M.; Kragholm, K.; Køber, L.; Gislason, G.H.; Torp-Pedersen, C.; et al. Association between biomarkers and COVID-19 severity and mortality: A nationwide Danish cohort study. BMJ Open 2020, 10, e041295. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 53) | None (n = 3) | Mild (n = 12) | Moderate (n = 13) | Severe (n = 25) | p-Value |
|---|---|---|---|---|---|---|
| Age (years, median (IQR)) | 62 {57–70} | 53 {49–65} | 61 {59–64} | 62 {54–67} | 66 {58–72} | 0.767 |
| Gender male, n (%) | 40 (75.5) | 3 (100) | 10 (83.3) | 6 (46.2) | 21 (84.0) | 0.039 |
| Body mass index (kg/m2, median (IQR)) | 29.3 {24.9–32.6} | 24.9 {24.7–28.2} | 29.2 {26.3–34.9} | 30.5 {6.7–35.2} | 29.3 {24.7–31.3} | 0.758 |
| Temperature, max (°C, median (IQR)) | 38.1 {37.4–38.5} | 38.1 {37.8–38.8} | 38.1 {37.8–38.6} | 38.2 {37.0–38.5} | 38.0 {37.3–38.5} | 0.934 |
| Heart rate (bpm, median (IQR)) | 106 {89–114} | 93 {86–107} | 105 {93–109} | 91 {72–103} | 112 {104–121} | 0.014 |
| Respiratory rate (bpm, median (IQR)) | 25 {23–28} | 24 {22–25} | 24 {23–26} | 25 {22–28} | 25 {23–29} | 0.678 |
| SOFA score at the day of enrollment (points, median (IQR)) | 9.0 {7.0–11.0} | 8.5 {7.8–9.3} | 7.0 {6.0–9.5} | 8.5 {7.8–10.0} | 11.0 {9.0–11.0} | 0.037 |
| Blood gas analysis (at the day of enrollment) | ||||||
| Arterial pH (median (IQR)) | 7.36 {7.30–7.42} | 7.47 {7.38–7.49} | 7.40 {7.37–7.44} | 7.38 {7.33–7.43} | 7.32 {7.28–7.36} | 0.011 |
| pCO2 (mmHg, median (IQR)) | 45.1 {39.3–52.0} | 48.0 {42.1–71.3} | 36.7 {33.8–41.2} | 45.5 {43.2–52.0} | 48.2 {42.1–55.4} | 0.001 |
| pO2 (mmHg, median (IQR)) | 79 {70–91} | 71 {64–80} | 92 {75–105} | 79 {70–92} | 79 {70–84} | 0.345 |
| SpO2 (%, median (IQR)) | 95 {94–98} | 94 {93–94} | 98 {96–99} | 98 {95–100} | 94 {93–97} | 0.031 |
| Horowitz index (mmHg/%, median (IQR)) | 114 {88–151} | 133 {89–276} | 224 {168–276} | 115 {100–150} | 94 {71–115} | 0.002 |
| Biomarker (at the day of enrollment, unless otherwise stated) | ||||||
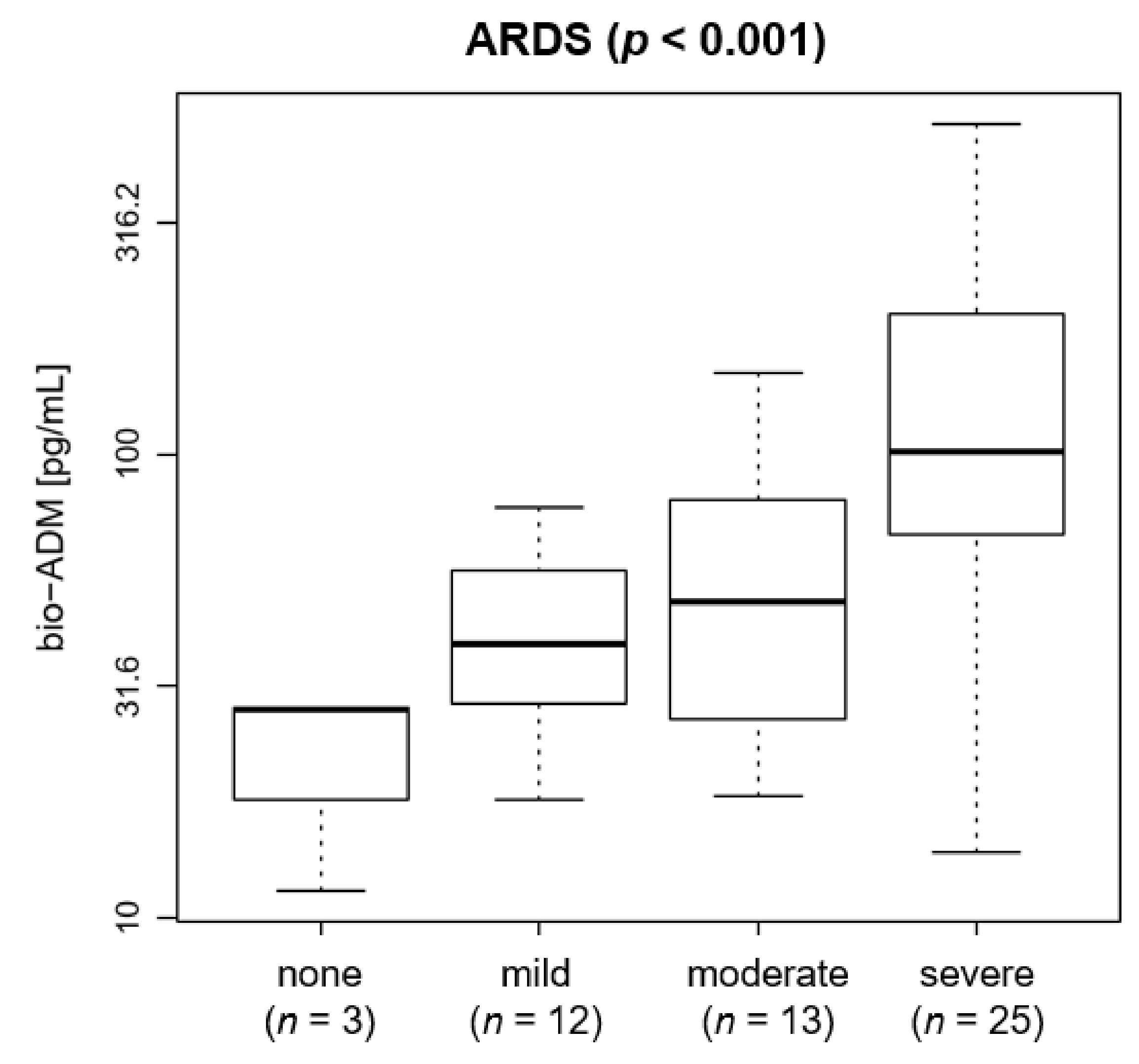
| bio-ADM (pg/mL, median (IQR)) | 59.9 {37.9–101.9} | 28.3 {19.9–28.4} | 39.0 {29.2–54.5} | 48.1 {26.9–79.8} | 101.9 {67.0–201.1} | <0.001 |
| bio-ADM > 70 pg/mL, n (%) | 22 (41.5) | 0 (0) | 1 (8.3) | 4 (30.8) | 17 (68.0) | 0.002 |
| Lactate (mmol/L, median (IQR)) | 1.0 {0.8–1.4} | 0.7 {0.5–1.0} | 0.8 {0.7–0.9} | 0.9 {0.7–1.5} | 1.3 {1–1.7} | 0.003 |
| IL-6 (pg/mL, median (IQR)) | 158.4 {97.4–337.4} | 51.9 {34.5–69.4} | 65.7 {46.9–93.5} | 211.2 {141.3–519.9} | 251.5 {151.2–475.2} | 0.001 |
| PCT (ng/mL, median (IQR)) | 0.53 {0.13–1.89} | 0.07 {0.06–0.08} | 0.14 {0.11–0.25} | 0.22 {0.11–0.69} | 1.46 {0.66–5.06} | <0.001 |
| CRP (nmol/L, median (IQR)) | 175 {117–326} | 182 {182–182} | 80 {34–142} | 256 {124–298} | 251 {158–350} | 0.002 |
| WBC (103/mm3, median (IQR)) | 9.3 {6.6–13.0} | 10.4 {9.3–11.9} | 6.2 {5.7–10.8} | 8.0 {7.4–9.4} | 10.1 {8.0–13.9} | 0.120 |
| Platelets (103/µL, median (IQR)) | 228 {198–329} | 202 {200–292} | 197 {140–236} | 237 {204–328} | 263 {204–338} | 0.242 |
| Creatinine (mg/dL, median (IQR)) | 1.1 {0.8–2.2} | 0.7 {0.6–0.7} | 1.0 {0.8–1.2} | 0.9 {0.6–1.1} | 1.8 {1.2–3.0} | 0.004 |
| Comorbidities | ||||||
| Arterial hypertension, n (%) | 27 (50.9) | 1 (33.3) | 5 (41.7) | 9 (69.2) | 12 (48.0) | 0.455 |
| Diabetes mellitus, n (%) | 13 (24.5) | 0 (0) | 1 (8.3) | 3 (23.1) | 9 (36.0) | 0.215 |
| Ischemic heart disease, n (%) | 10 (18.9) | 0 (0) | 2 (16.7) | 4 (30.8) | 4 (16.0) | 0.557 |
| Embolism/thrombosis, n (%) | 6 (11.3) | 1 (33.3) | 1 (8.3) | 3 (23.1) | 1 (4.0) | 0.197 |
| Cardiac arrhythmia, n (%) | 6 (11.3) | 0 (0) | 1 (8.3) | 0 (0) | 5 (20.0) | 0.259 |
| Cerebral vascular disease, n (%) | 5 (9.4) | 0 (0) | 2 (16.7) | 0 (0) | 3 (12.0) | 0.459 |
| COPD, n (%) | 6 (11.3) | 1 (33.3) | 2 (16.7) | 1 (7.7) | 2 (8.0) | 0.525 |
| Other lung diseases, n (%) | 2 (3.8) | 1 (33.3) | 1 (8.3) | 0 (0) | 0 (0) | 0.025 |
| Chronic kidney disease, n (%) | 8 (15.1) | 0 (0) | 2 (16.7) | 3 (23.1) | 3 (12.0) | 0.708 |
| Tumor disease, n (%) | 4 (7.5) | 0 (0) | 3 (25.0) | 1 (7.7) | 0 (0) | 0.057 |
| Smoker, n (%) | 3 (5.7) | 0 (0) | 1 (8.3) | 2 (15.4) | 0 (0) | 0.247 |
| Treatment in the ICU (first 14 days, unless otherwise stated) | ||||||
| ICU length of stay (days, median (IQR)) | 16 {7.5–20.0} | 6 {4.0–9.5} | 7.5 {3.0–10.5} | 19.5 {16.5–23.0} | 17.5 {15.0–21.0} | 0.004 |
| Highest dose of Norepinephrine during the first 7 days (µg/kg/min, median (IQR)) | 0.15 {0.06–0.29} | 0.07 {0.03–0.11} | 0 {0–0.09} | 0.15 {0.06–0.18} | 0.29 {0.13–0.35} | <0.001 |
| Anticoagulation, n (%) | 15 (28.3) | 1 (33.3) | 2 (16.7) | 3 (23.1) | 9 (36.0) | 0.627 |
| Antiplatelet, n (%) | 15 (28.3) | 0 (0) | 4 (33.3) | 6 (46.2) | 5 (20.0) | 0.238 |
| Antihypertensive, n (%) | 32 (60.4) | 1 (33.3) | 8 (66.7) | 10 (76.9) | 13 (52.0) | 0.343 |
| Immunosuppressant, n (%) | 9 (17) | 1 (33.3) | 2 (16.7) | 4 (30.8) | 2 (8.0) | 0.289 |
| Analgesics, n (%) | 8 (15.1) | 1 (33.3) | 4 (33.3) | 1 (7.7) | 2 (8.0) | 0.143 |
| Ventilation | ||||||
| Intubation during ICU stay, n (%) | 44 (83.0) | 1 (33.3) | 5 (41.7) | 13 (100) | 25 (100) | 0.006 |
| Intubation: | ||||||
| never, n (%) | 9 (17.0) | 2 (67.7) | 7 (58.3) | 0 (0) | 0 (0) | |
| at admission, n (%) | 38 (71.7) | 1 (33.3) | 3 (25.0) | 12 (92.3) | 22 (88.0) | 0.022 |
| later, n (%) | 6 (11.3) | 0 (0) | 2 (16.7) | 1 (7.7) | 3 (12.0) | |
| Outcome | ||||||
| Death 28 days, n (%) | 13 (24.5) | 1 (33.3) | 0 (0) | 1 (7.7) | 11 (44.0) | 0.011 |
| Status on day 28: | 0.001 | |||||
| discharged, n (%) | 32 (60.4) | 2 (66.7) | 12 (100) | 11 (84.6) | 7 (28.0) | |
| in ICU post day 28, n (%) | 8 (15.1) | 0 (0) | 0 (0) | 1 (7.7) | 7 (28.0) | |
| death 28 days, n (%) | 13 (24.5) | 1 (33.3) | 0 (0) | 1 (7.7) | 11 (44.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, T.-P.; Stoppe, C.; Breuer, T.; Stiehler, L.; Dreher, M.; Kersten, A.; Kluge, S.; Karakas, M.; Zechendorf, E.; Marx, G.; et al. Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study. J. Clin. Med. 2021, 10, 1667. https://doi.org/10.3390/jcm10081667
Simon T-P, Stoppe C, Breuer T, Stiehler L, Dreher M, Kersten A, Kluge S, Karakas M, Zechendorf E, Marx G, et al. Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study. Journal of Clinical Medicine. 2021; 10(8):1667. https://doi.org/10.3390/jcm10081667
Chicago/Turabian StyleSimon, Tim-Philipp, Christian Stoppe, Thomas Breuer, Lara Stiehler, Michael Dreher, Alexander Kersten, Stefan Kluge, Mahir Karakas, Elisabeth Zechendorf, Gernot Marx, and et al. 2021. "Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study" Journal of Clinical Medicine 10, no. 8: 1667. https://doi.org/10.3390/jcm10081667
APA StyleSimon, T.-P., Stoppe, C., Breuer, T., Stiehler, L., Dreher, M., Kersten, A., Kluge, S., Karakas, M., Zechendorf, E., Marx, G., & Martin, L. (2021). Prognostic Value of Bioactive Adrenomedullin in Critically Ill Patients with COVID-19 in Germany: An Observational Cohort Study. Journal of Clinical Medicine, 10(8), 1667. https://doi.org/10.3390/jcm10081667