
Effectiveness of Clinical Pharmacist Service on Drug-Related Problems and Patient Outcomes for Hospitalized Patients with Chronic Kidney Disease: A Randomized Controlled Trial

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
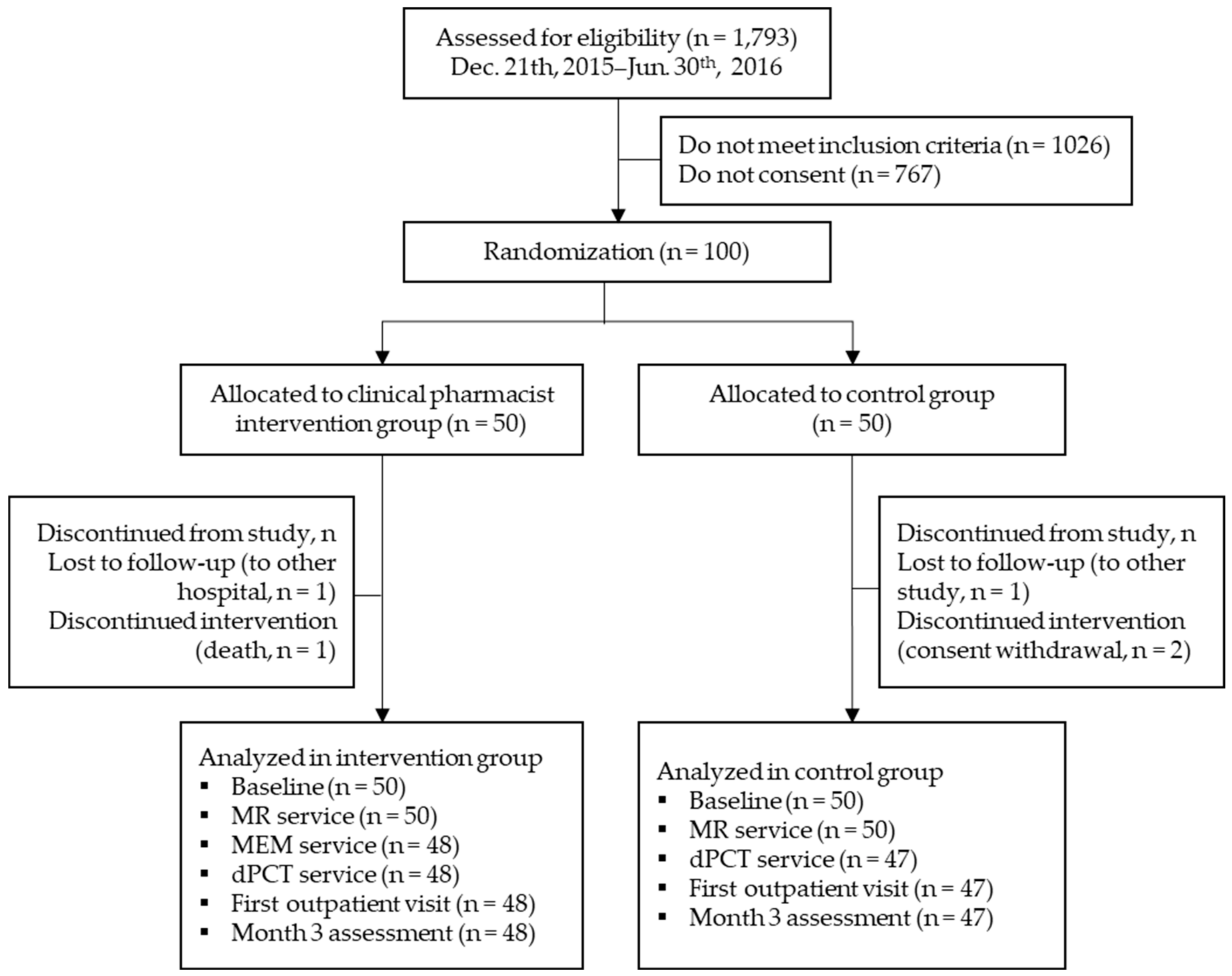
2.1. Study Design
2.2. Participants
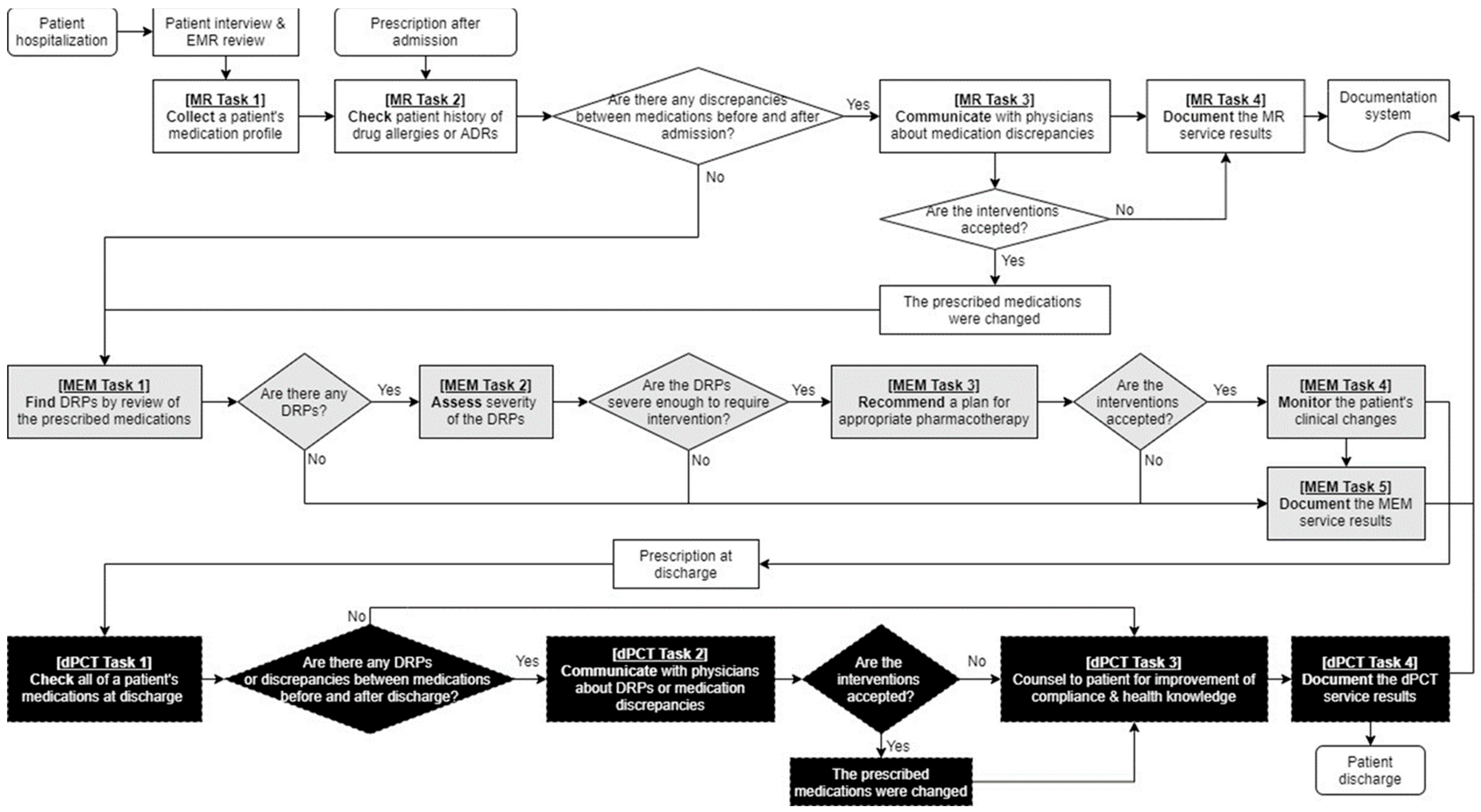
2.3. Intervention
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Drug-Related Problems by the DrugTEAM Service
3.3. Adherence and Acute Care Utilization after Discharge by the DrugTEAM Service
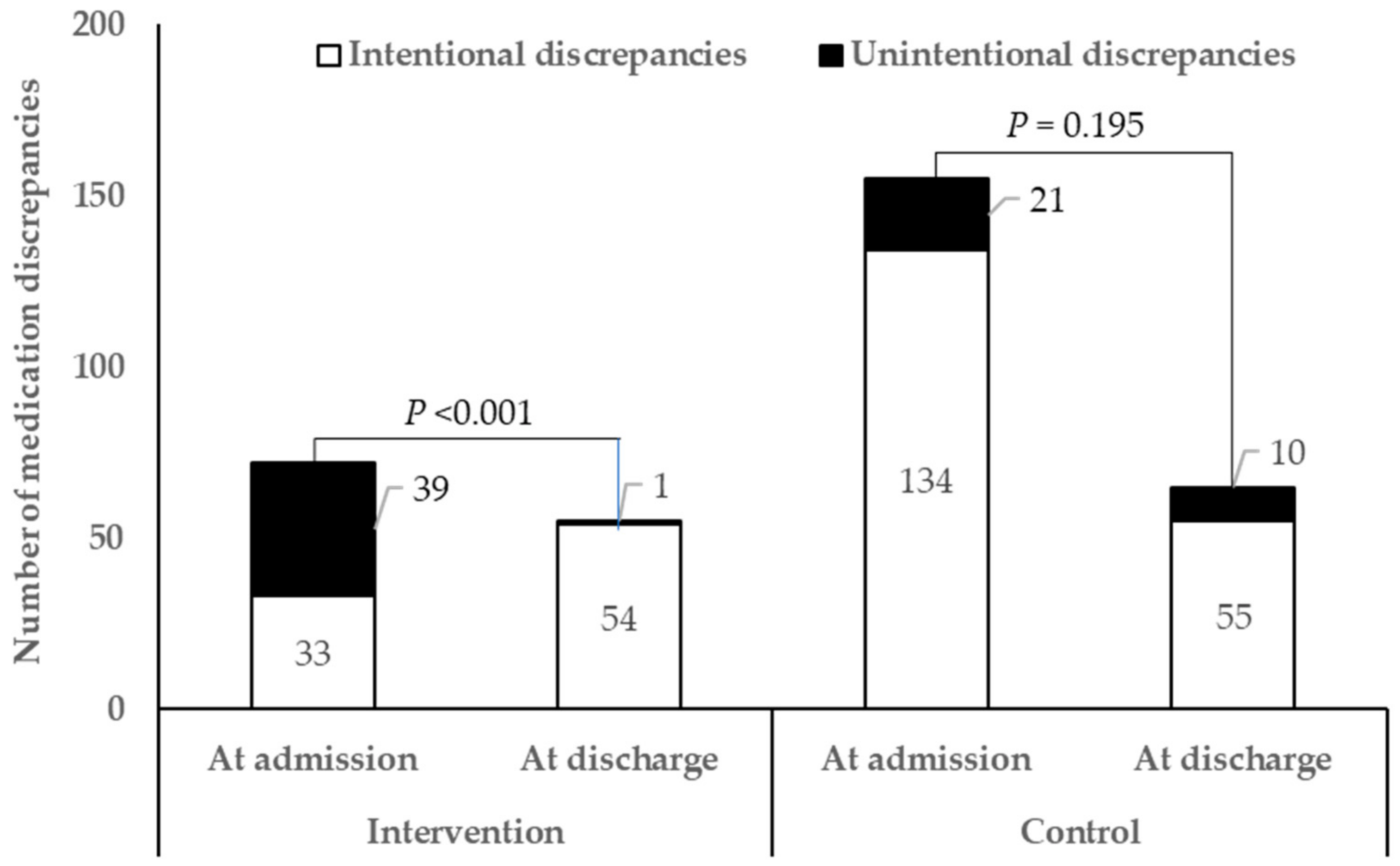
3.4. Unintentional Medication Discrepancies by the DrugTEAM Service
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Xie, Y.; Bowe, B.; Mokdad, A.H.; Xian, H.; Yan, Y.; Li, T.; Maddukuri, G.; Tsai, C.-Y.; Floyd, T.; Al-Aly, Z. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney Int. 2018, 94, 567–581. [Google Scholar] [CrossRef]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Chronic Kidney Disease (CKD) in Korea by Numbers. KSN NEWS Factsheet. 2019. Available online: http://www.ksn.or.kr/rang_board/list.html?num=1570&code=factsheet (accessed on 28 December 2020).
- United States Renal Data System. End Stage Renal Disease: Chapter 11. Iternational Comparisons. In 2020 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020. [Google Scholar]
- Tonelli, M.; Wiebe, N.; Guthrie, B.; James, M.T.; Quan, H.; Fortin, M.; Klarenbach, S.W.; Sargious, P.; Straus, S.; Lewanczuk, R.; et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int. 2015, 88, 859–866. [Google Scholar] [CrossRef]
- St. Peter, W.L.; Schoolwerth, A.C.; McGowan, T.; McClellan, W.M. Chronic kidney disease: Issues and establishing programs and clinics for improved patient outcomes. Am. J. Kidney Dis. 2003, 41, 903–924. [Google Scholar] [CrossRef]
- Lalonde, L.; Quintana-Bárcena, P.; Lord, A.; Bell, R.; Clément, V.; Daigneault, A.M.; Legris, M.; Letendre, S.; Mouchbahani, M.; Jouini, G.; et al. Community Pharmacist Training-and-Communication Network and Drug-Related Problems in Patients With CKD: A Multicenter, Cluster-Randomized, Controlled Trial. Am. J. Kidney Dis. 2017, 70, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Belaiche, S.; Romanet, T.; Allenet, B.; Calop, J.; Zaoui, P. Identification of drug-related problems in ambulatory chronic kidney disease patients: A 6-month prospective study. J. Nephrol. 2012, 25, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Al Raiisi, F.; Stewart, D.; Fernandez-Llimos, F.; Salgado, T.M.; Mohamed, M.F.; Cunningham, S. Clinical pharmacy practice in the care of Chronic Kidney Disease patients: A systematic review. Int. J. Clin. Pharm. 2019, 41, 630–666. [Google Scholar] [CrossRef] [PubMed]
- Mechta Nielsen, T.; Frøjk Juhl, M.; Feldt-Rasmussen, B.; Thomsen, T. Adherence to medication in patients with chronic kidney disease: A systematic review of qualitative research. Clin. Kidney J. 2018, 11, 513–527. [Google Scholar] [CrossRef]
- Cohen, E.A.; McKimmy, D.; Cerilli, A.; Kulkarni, S. A Pharmacist-Driven Intervention Designed to Improve Medication Accuracy in the Outpatient Kidney Transplant Setting. Drug Health Patient Saf. 2020, 12, 229–235. [Google Scholar] [CrossRef]
- Wang, S.M.; Hsiao, L.C.; Ting, I.W.; Yu, T.M.; Liang, C.C.; Kuo, H.L.; Chang, C.T.; Liu, J.H.; Chou, C.Y.; Huang, C.C. Multidisciplinary care in patients with chronic kidney disease: A systematic review and meta-analysis. Eur. J. Intern. Med. 2015, 26, 640–645. [Google Scholar] [CrossRef]
- Joy, M.S.; DeHart, R.M.; Gilmartin, C.; Hachey, D.M.; Hudson, J.Q.; Pruchnicki, M.; Dumo, P.; Grabe, D.W.; Saseen, J.; Zillich, A.J. Clinical pharmacists as multidisciplinary health care providers in the management of CKD: A joint opinion by the Nephrology and Ambulatory Care Practice and Research Networks of the American College of Clinical Pharmacy. Am. J. Kidney Dis. 2005, 45, 1105–1118. [Google Scholar] [CrossRef] [PubMed]
- Al Hamarneh, Y.N.; Tsuyuki, R.T.; Jones, C.A.; Manns, B.; Tonelli, M.; Scott-Douglass, N.; Jindal, K.; Tink, W.; Hemmelgarn, B.R. Effectiveness of Pharmacist Interventions on Cardiovascular Risk in Patients With CKD: A Subgroup Analysis of the Randomized Controlled R(x)EACH Trial. Am. J. Kidney Dis. 2018, 71, 42–51. [Google Scholar] [CrossRef]
- Lee, I.-H.; Rhie, S.J.; Je, N.K.; Rhew, K.Y.; Ji, E.; Oh, J.M.; Lee, E.; Yoon, J.-H. Perceived needs of pharmaceutical care services among healthcare professionals in South Korea: A qualitative study. Int. J. Clin. Pharm. 2016, 38, 1219–1229. [Google Scholar] [CrossRef]
- Create a Blocked Randomization List. Available online: http://www.sealedenvelope.com/simple-randomiser/v1/lists (accessed on 19 December 2015).
- Han, N.; Han, S.H.; Chu, H.; Kim, J.; Rhew, K.Y.; Yoon, J.H.; Je, N.K.; Rhie, S.J.; Ji, E.; Lee, E.; et al. Service design oriented multidisciplinary collaborative team care service model development for resolving drug related problems. PLoS ONE 2018, 13, e0201705. [Google Scholar] [CrossRef]
- Domingues, D.; Carneiro, R.; Costa, I.; Monteiro, C.; Shvetz, Y.; Barbosa, A.C.; Azevedo, P. Therapeutic futility in cancer patients at the time of palliative care transition: An analysis with a modified version of the Medication Appropriateness Index. Palliat Med. 2015, 29, 643–651. [Google Scholar] [CrossRef]
- Medical Fee Schedule Department. Health Insurance Medical Care Benefit Expenses; Health Insurance Review and Assessment Service: Gangwon-do, Korea, 2019; pp. 633–637. [Google Scholar]
- Cipolle, R.J.; Strand, L.M.; Morley, P.C. Drug Therapy Problems. In Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management Services, 3rd ed.; McGraw-Hill: New York, NY, USA, 2012. [Google Scholar]
- Pharmaceutical Care Network Europe Foundation. PCNE Classification scheme for Drug-Related Problems V6.2. 2010. Available online: https://www.pcne.org/upload/files/11_PCNE_classification_V6-2.pdf (accessed on 19 December 2015).
- Case Management Society of America. Modified Morisky Scale. In Case Management Adherence Guidelines Version 2.0; Case Management Society of America: Little Rock, AR, USA, 2006; pp. 69–75. [Google Scholar]
- Hias, J.; Van der Linden, L.; Spriet, I.; Vanbrabant, P.; Willems, L.; Tournoy, J.; De Winter, S. Predictors for unintentional medication reconciliation discrepancies in preadmission medication: A systematic review. Eur. J. Clin. Pharmacol. 2017, 73, 1355–1377. [Google Scholar] [CrossRef]
- Lenander, C.; Elfsson, B.; Danielsson, B.; Midlöv, P.; Hasselström, J. Effects of a pharmacist-led structured medication review in primary care on drug-related problems and hospital admission rates: A randomized controlled trial. Scand. J. Prim. Health Care 2014, 32, 180–186. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Alicic, R.Z.; Short, R.A.; Neumiller, J.J.; Gates, B.J.; Daratha, K.B.; Barbosa-Leiker, C.; McPherson, S.M.; Chaytor, N.S.; Dieter, B.P.; et al. Medication Therapy Management after Hospitalization in CKD: A Randomized Clinical Trial. Clin. J. Am. Soc. Nephrol. 2018, 13, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, P.F.; Huang, J.; Fukagawa, M.; Hoy, W.; Jha, V.; Oh, K.-H.; Sola, L.; Cockwell, P.; Levin, A.; Feldman, H.I.; et al. A collaborative, individual-level analysis compared longitudinal outcomes across the International Network of Chronic Kidney Disease (iNETCKD) cohorts. Kidney Int. 2019, 96, 1217–1233. [Google Scholar] [CrossRef] [PubMed]
- Burnier, M.; Pruijm, M.; Wuerzner, G.; Santschi, V. Drug adherence in chronic kidney diseases and dialysis. Nephrol. Dial. Transplant. 2014, 30, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Nakayama, I.; Kawakatsu, Y.; Yamamoto, T.; Ishigami, N.; Watanuki, K.; Okabe, T.; Yokoyama, H. Effects of pharmacist participation in chronic kidney disease (CKD) network and CKD manual distribution on drug-related kidney injury. Pharmacoepidemiol. Drug Saf. 2019, 28, 887–896. [Google Scholar] [CrossRef]
- Alqenae, F.A.; Steinke, D.; Keers, R.N. Prevalence and Nature of Medication Errors and Medication-Related Harm Following Discharge from Hospital to Community Settings: A Systematic Review. Drug Saf. 2020, 43, 517–537. [Google Scholar] [CrossRef] [PubMed]
- Quintana-Bárcena, P.; Lord, A.; Lizotte, A.; Berbiche, D.; Lalonde, L. Prevalence and Management of Drug-Related Problems in Chronic Kidney Disease Patients by Severity Level: A Subanalysis of a Cluster Randomized Controlled Trial in Community Pharmacies. J. Manag. Care Spec. Pharm. 2018, 24, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Garin, N.; Sole, N.; Lucas, B.; Matas, L.; Moras, D.; Rodrigo-Troyano, A.; Gras-Martin, L.; Fonts, N. Drug related problems in clinical practice: A cross-sectional study on their prevalence, risk factors and associated pharmaceutical interventions. Sci. Rep. 2021, 11, 883. [Google Scholar] [CrossRef]
- Saldanha, V.; Araujo, I.B.; Lima, S.; Martins, R.R.; Oliveira, A.G. Risk factors for drug-related problems in a general hospital: A large prospective cohort. PLoS ONE 2020, 15, e0230215. [Google Scholar] [CrossRef]
- Cossette, B.; Éthier, J.F.; Joly-Mischlich, T.; Bergeron, J.; Ricard, G.; Brazeau, S.; Caron, M.; Germain, O.; Payette, H.; Kaczorowski, J.; et al. Reduction in targeted potentially inappropriate medication use in elderly inpatients: A pragmatic randomized controlled trial. Eur. J. Clin. Pharmacol. 2017, 73, 1237–1245. [Google Scholar] [CrossRef]
- Joost, R.; Dörje, F.; Schwitulla, J.; Eckardt, K.U.; Hugo, C. Intensified pharmaceutical care is improving immunosuppressive medication adherence in kidney transplant recipients during the first post-transplant year: A quasi-experimental study. Nephrol. Dial. Transplant. 2014, 29, 1597–1607. [Google Scholar] [CrossRef]
- Moon, S.J.; Lee, W.Y.; Hwang, J.S.; Hong, Y.P.; Morisky, D.E. Accuracy of a screening tool for medication adherence: A systematic review and meta-analysis of the Morisky Medication Adherence Scale-8. PLoS ONE 2017, 12, e0187139. [Google Scholar] [CrossRef]
- Lee, Y.M.; Kim, R.B.; Lee, H.J.; Kim, K.; Shin, M.H.; Park, H.K.; Ahn, S.K.; Kim, S.Y.; Lee, Y.H.; Kim, B.G.; et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: A cross-sectional study. Health Qual. Life Outcomes 2018, 16, 100. [Google Scholar] [CrossRef]
- Ravn-Nielsen, L.V.; Duckert, M.L.; Lund, M.L.; Henriksen, J.P.; Nielsen, M.L.; Eriksen, C.S.; Buck, T.C.; Pottegård, A.; Hansen, M.R.; Hallas, J. Effect of an In-Hospital Multifaceted Clinical Pharmacist Intervention on the Risk of Readmission: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Frament, J.; Hall, R.K.; Manley, H.J. Medication Reconciliation: The Foundation of Medication Safety for Patients Requiring Dialysis. Am. J. Kidney Dis. 2020, 76, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Chisholm, M.A.; Vollenweider, L.J.; Mulloy, L.L.; Wynn, J.J.; Wade, W.E.; DiPiro, J.T. Cost-benefit analysis of a clinical pharmacist-managed medication assistance program in a renal transplant clinic. Clin. Transplant. 2000, 14, 304–307. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 100) | Intervention Group (n = 50) | Control Group (n = 50) | p Value |
|---|---|---|---|---|
| Age, mean ± SD, years | 52.5 ± 16.9 | 51.0 ± 16.6 | 54.0 ± 17.4 | 0.381 |
| Age, median (IQR), years | 55 (37–67) | 51 (36.3–64) | 57.5 (38–67) | |
| Male, n (%) | 60 (60) | 31 (62) | 29 (58) | 0.683 |
| eGFR, median (IQR), mL/min/1.73 m2 | 9.2 (5.7–20.8) | 8.9 (5.9–20.6) | 9.2 (5.4–20.9) | 0.834 |
| CKD stage, n (%) | ||||
| Stage 2 (eGFR 60–89 mL/min/1.73 m2) | 3 (3) | 2 (2) | 1 (2) | 1.000 |
| Stage 3 (eGFR 30–59 mL/min/1.73 m2) | 12 (12) | 7 (14) | 5 (10) | 0.538 |
| Stage 4 (eGFR 15–29 mL/min/1.73 m2) | 20 (20) | 7 (14) | 13 (26) | 0.134 |
| Stage 5 (eGFR < 15 mL/min/1.73 m2) | 65 (65) | 34 (68) | 31 (62) | 0.529 |
| Renal replacement therapy, n (%) | ||||
| Dialysis | 33 (33) | 13 (26) | 20 (40) | 0.137 |
| Kidney transplantation | 17 (17) | 7 (14) | 10 (20) | 0.425 |
| None | 50 (50) | 30 (60) | 20 (40) | 0.046 |
| CKD etiology, n (%) | ||||
| Diabetes mellitus | 28 (28) | 12 (24) | 16 (32) | 0.373 |
| Hypertension | 8 (8) | 5 (10) | 3 (6) | 0.715 |
| Glomerulonephritis | 40 (40) | 23 (46) | 17 (34) | 0.221 |
| Others | 9 (9) | 5 (10) | 4 (8) | 1.000 |
| Unknown | 15 (15) | 5 (10) | 10 (20) | 0.161 |
| Diagnosis at admission, n (%) | ||||
| Uremia | 33 (33) | 17 (34) | 16 (32) | 0.832 |
| Renal replacement therapy | 26 (26) | 11 (22) | 15 (30) | 0.362 |
| Infection | 16 (16) | 9 (18) | 7 (14) | 0.585 |
| Graft rejection | 8 (8) | 3 (6) | 5 (10) | 0.715 |
| Cardiovascular diseases | 7 (7) | 5 (10) | 2 (4) | 0.436 |
| Others | 10 (10) | 5 (10) | 5 (10) | 1.000 |
| Number of comorbid diseases, median (IQR) | 5 (4–6) | 5 (2–9) | 5 (5–7) | 0.009 |
| Adherence at admission measured by MMS, mean ± SD | 4.5 ± 1.3 | 4.1 ± 1.5 | 4.5 ± 1.5 | 0.226 |
| Number of medicines per patient at admission, median (IQR) | 9 (7–12) | 8 (5.8–12) | 9 (8–12) | 0.241 |
| Outcomes | DRPs, n (%) | Resolved DRPs, n (%) |
|---|---|---|
| Patients with any DRPs during hospitalization, n (%) | 48 (100.0) | NA |
| Total number of DRPs during hospitalization | 182 (100.0) | 149 (81.9) |
| Number of DRPs per patient during hospitalization, mean ± SD | 3.8 ± 1.8 | NA |
| DRP classification a, n (%) | ||
| Prescription without indication | 20 (11.0) | 20 (100.0) |
| Indication without prescription | 65 (35.7) | 53 (81.5) |
| Duplicated prescription | 2 (1.1) | 2 (100.0) |
| Inappropriate drug selection | 12 (6.6) | 9 (75.0) |
| Inappropriate dosage/administration | 58 (31.9) | 49 (84.5) |
| Allergy | 2 (1.1) | 2 (100.0) |
| Adverse drug reaction | 11 (6.0) | 7 (63.6) |
| Cost issue | 4 (2.2) | 3 (75.0) |
| Others | 8 (4.4) | 4 (50.0) |
| Planned Interventions | MEM Service, n (%) | dPCT Service, n (%) |
|---|---|---|
| Drug started | 73 (37.1) | 20 (37.0) |
| Drug paused or stopped | 58 (29.4) | 16 (29.6) |
| Dosage increased | 19 (9.6) | 0 |
| Dosage decreased | 26 (13.2) | 8 (14.8) |
| Instructions for use changed | 9 (4.6) | 1 (1.9) |
| Administration time changed | 2 (1.0) | 3 (5.6) |
| Information of insurance coverage provided | 4 (2.0) | 2 (3.7) |
| Laboratory test recommended for drug efficacy monitoring | 6 (3.0) | 3 (5.6) |
| Others | 0 | 1 (1.9) |
| Total | 197 (100.0) | 54 (100.0) |
| Factors | Prevalence Ratio (95% CI) | p Value |
|---|---|---|
| Age | 0.989 (0.973–1.006) | 0.223 |
| Gender (male) | 1.248 (0.742–2.009) | 0.404 |
| Estimated glomerular filtration rate | 0.970 (0.951–0.989) | 0.002 |
| Renal replacement therapy | ||
| None | Reference | |
| Dialysis | 0.839 (0.469–1.502) | 0.555 |
| Kidney transplantation | 0.979 (0.444–2.160) | 0.958 |
| Number of comorbid diseases | 0.924 (0.778–1.097) | 0.368 |
| Adherence measured by MMS at admission | 0.979 (0.809–1.183) | 0.823 |
| Number of medicines per patients at admission | 0.936 (0.864–1.014) | 0.105 |
| Number of medicines per patients during hospitalization | 0.976 (0.904–1.054) | 0.534 |
| Number of unintentional medication discrepancies at admission | 1.294 (1.034–1.620) | 0.025 |
| Outcomes | Intervention (n = 48) | Control (n = 47) | p Value | |
|---|---|---|---|---|
| DRPs | Patients with any DRPs at discharge, n (%) | 29 (60.4) | 43 (91.5) | <0.001 |
| Total number of DRPs at discharge | 45 | 92 | <0.001 | |
| Number of DRPs per patient at discharge, mean ± SD | 0.9 ± 1.0 | 2.0 ± 1.3 | <0.001 | |
| DRP classification a, n (%) | ||||
| Prescription without indication | 1 (2.2) | 8 (8.7) | 0.271 | |
| Indication without prescription | 14 (31.1) | 36 (39.1) | 0.360 | |
| Inappropriate drug selection | 5 (11.1) | 4 (4.3) | 0.154 | |
| Inappropriate dosage/administration | 15 (33.3) | 19 (20.7) | 0.107 | |
| Adverse drug reaction | 3 (6.7) | 10 (10.9) | 0.545 | |
| Drug interaction | 0 | 8 (8.7) | 0.053 | |
| Cost issue | 2 (4.4) | 4 (4.3) | 1.000 | |
| Others | 5 (11.1) | 3 (3.3) | 0.114 | |
| Adherence | MMS at first visit after discharge, mean ± SD | 5.2 ± 1.0 | 4.9 ± 1.3 | 0.205 |
| Patients with increased MMS score, n (%) | 39 (81.3) | 30 (63.8) | 0.057 | |
| Acute care utilization | Patients readmitted or visiting emergency center within 3 months of discharge, n (%) | 16 (33.3) | 12 (25.5) | 0.404 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.-K.; Jeong, S.; Han, N.; Na, H.; Jang, H.Y.; Sohn, M.; Kim, Y.S.; Joo, K.-W.; Oh, K.-H.; Kim, D.K.; et al. Effectiveness of Clinical Pharmacist Service on Drug-Related Problems and Patient Outcomes for Hospitalized Patients with Chronic Kidney Disease: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 1788. https://doi.org/10.3390/jcm10081788
Song Y-K, Jeong S, Han N, Na H, Jang HY, Sohn M, Kim YS, Joo K-W, Oh K-H, Kim DK, et al. Effectiveness of Clinical Pharmacist Service on Drug-Related Problems and Patient Outcomes for Hospitalized Patients with Chronic Kidney Disease: A Randomized Controlled Trial. Journal of Clinical Medicine. 2021; 10(8):1788. https://doi.org/10.3390/jcm10081788
Chicago/Turabian StyleSong, Yun-Kyoung, Sohyun Jeong, Nayoung Han, Heejin Na, Ha Young Jang, Minji Sohn, Yon Su Kim, Kwon-Wook Joo, Kook-Hwan Oh, Dong Ki Kim, and et al. 2021. "Effectiveness of Clinical Pharmacist Service on Drug-Related Problems and Patient Outcomes for Hospitalized Patients with Chronic Kidney Disease: A Randomized Controlled Trial" Journal of Clinical Medicine 10, no. 8: 1788. https://doi.org/10.3390/jcm10081788
APA StyleSong, Y.-K., Jeong, S., Han, N., Na, H., Jang, H. Y., Sohn, M., Kim, Y. S., Joo, K.-W., Oh, K.-H., Kim, D. K., Lee, H., Oh, J. M., & DrugTEAM Study Group. (2021). Effectiveness of Clinical Pharmacist Service on Drug-Related Problems and Patient Outcomes for Hospitalized Patients with Chronic Kidney Disease: A Randomized Controlled Trial. Journal of Clinical Medicine, 10(8), 1788. https://doi.org/10.3390/jcm10081788