Abstract
Background: Literature regarding ergonomic protocols for surgery is lacking, and there is a paucity of information on how this impacts on gender differences with regards to the barriers faced by women in surgery. Methods: This article reviews current literature addressing women in surgery and ergonomics through a systematic search including the Web of Science, Scopus, and PubMed databases. Results: Searches retrieved 425 items, and after a thorough evaluation for inclusion, 15 studies were examined—predominantly surveys (n = 9) and originating from the USA (n = 9). Identified ergonomic challenges included the general shorter height and smaller glove size of women. Furthermore, women experienced more musculoskeletal pain than men, potentially because the size and design of theatre tools are designed for male and tall individuals, highlighting an unconscious gender bias still pervading the surgical field. Conclusions: As more women enter medicine and pursue surgical careers, it is essential to foster a culture of diversity and inclusion in theatre to develop more ergonomic environments.
1. Introduction
Surgery remains overwhelmingly a male field [1]. Despite the fact that efforts to attract and retain the female surgical workforce are growing daily, these focus mainly on promoting a change in the culture [2], which has fortunately already resulted in a significant reduction in much of the overt sexism that was apparent in previous years. However, there remains an overarching theme where unconscious bias identifies surgeons to a stereotype of male individuals [3].
Initiatives aiming at how to strategically tackle gender equity among professionals, through networking and mentoring supported by societies and organisations, are in place [4,5,6,7], but not much has been done to relieve the struggle commonly associated with long operations. There is evidence that female surgeons experience more discomfort in their bodies and their hands than their male colleagues [8,9,10].
It comes then as no surprise that the abovementioned issues add to the well-known surgical work–life imbalance, with a direct impact on women’s ability to work, to operate, and to acquire practical skills. Altogether, these factors are likely to affect the determination of prospective female trainees, and to negatively impact on the retention of the current female surgeons.
Why are diversity and inclusion (DEI)—i.e., the recognition that each individual requires different resources and opportunities to achieve an equal outcome—so important? In general, it is thought that people with different experiences, perspectives, and thinking styles combine and collaborate to create a stronger, more successful environment, so the inclusion of diverse surgical members ultimately builds better teams [3,4].
The aim of this review is to identify the principal barriers perceived by women according to the “ergonomics” principles, i.e., the scientific discipline concerned with the understanding of interactions between humans and other elements of a system, and the field that applies theory, principles, data, and methods to design, aiming to optimise human wellbeing and overall system performance [11].
2. Materials and Methods
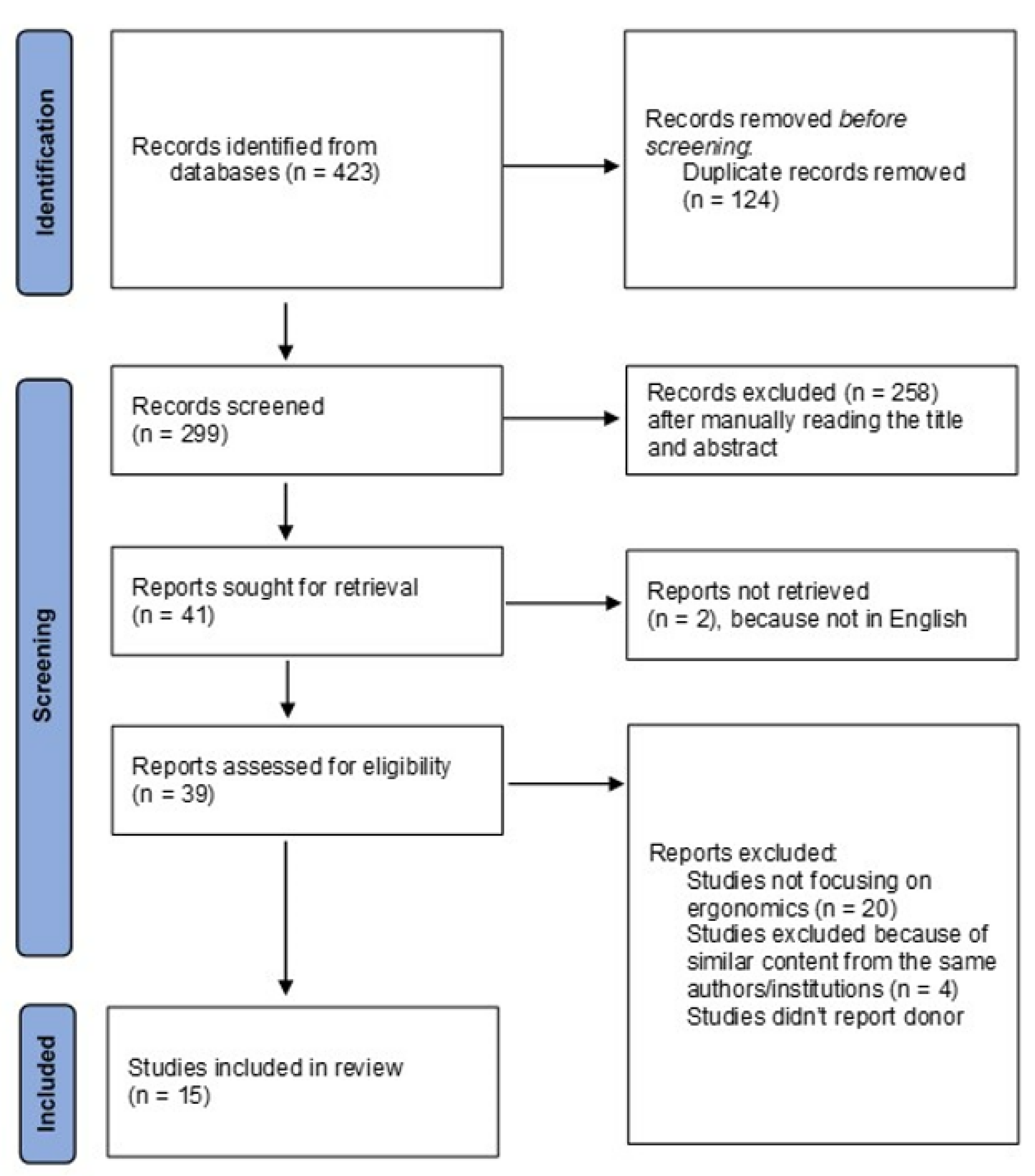
A systematic search was performed to identify studies focusing on ergonomics for women in surgery within the PubMed, Scopus, and Web of Science electronic databases. Only original articles in English, with no time restrictions, and reporting specifically on the principles of ergonomics—as previously identified [11]—were considered. Search terms included combinations of the keywords “ergonomics” and “women in surgery”. Studies that originated from the same centre were considered only if not overlapping in the reported cases. Two independent reviewers (M.I.B. and M.I.A.) performed the search and the screening, before producing a list of studies eligible for inclusion. In case of disagreement, a third reviewer (P.S.) was consulted. The included studies were evaluated according to the Newcastle–Ottawa Scale [12]. The complete evaluation is reported in Table 1. The PRISMA diagram for the search is reported in Figure 1.

Table 1.
Quality of evidence in the selected papers for the systematic review according to the Newcastle–Ottawa Scale.
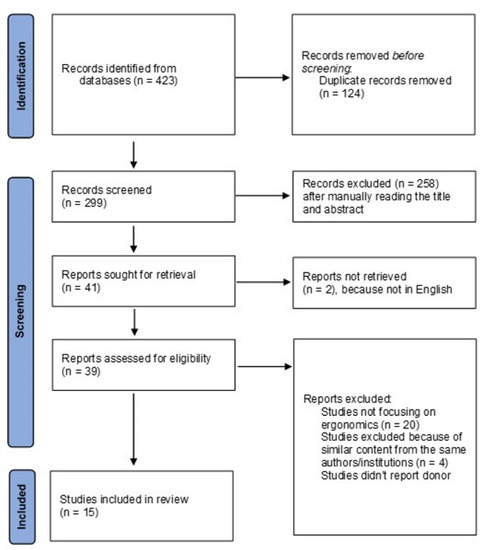
Figure 1.
PRISMA flow diagram.
3. Results
The systematic search identified the following results in each of the investigated databases: Web of Science (n = 73), PubMed (n = 273), and Scopus (n = 77). After duplicate removal (n = 124) and screening based on titles and abstracts, a total of 41 articles were analysed. Reading those articles in full then led to 15 studies meeting the inclusion criteria. Most studies (n = 9) were surveys, and with the USA as the country of origin (n = 9). The specialties represented were general surgery (n = 7), gynaecology (n = 4), dentistry (n = 1), endocrine surgery (n = 1), orthopaedics (n = 1), and otorhinolaryngology (n = 1). A full list of the studies included for review is summarised in Table 2; the main findings are described below.
Table 2.
Study characteristics, aims, and main findings.
3.1. Work-Related Physical Discomfort
The incidence of physical strain secondary to maintaining prolonged uncomfortable postures, or to remaining static holding retractors with high levels of manual force, has been reported frequently [15,19,22,23]. More specifically, we can distinguish between musculoskeletal symptoms and hand symptoms. The regions of interest are the cervical (58.1%), dorsal (40.5%), lumbar (52.7%), wrist (27.1%), and shoulder regions (24.3%) [19], although the frequency might vary according to the type of surgery performed.
Female sex per se is linked to a more severe progression of upper limb musculoskeletal disorders; in fact, the prevalence of rotator cuff syndrome is reported to be as high as 6.6% in men and 8.5% in women, on a general population basis [25]. In the literature, women reported experiencing pain or discomfort associated with their surgical practice [13,16,21], with an approximately twofold risk in comparison to their male colleagues [13]. Shortness is also associated with higher discomfort [14,24], particularly when performing minimally invasive surgery; shorter surgeons are in fact at greater risk of spinal torsion to watch the monitor, given their propensity to pose their shoulder flexed, thus leading to greater spinal rotation to the right. Interestingly, in the study by Stewart et al. [24], greater pain scores were related to short stature (p < 0.001), i.e., height ≤ 168 cm, and male gender (p < 0.001). The use of robotic system seems to reduce pain scores in comparison to both laparoscopy and open surgery [17,24], or to cancel any significant pain-related effects, although this is limited only to certain demographic subgroups [24], i.e., tall surgeons (p = 0.07) and female surgeons (p = 0.13).
3.2. Compliance of Surgical Devices with Female Requirements
In laparoscopy, the evaluation of wrist movements is also of utmost importance, given the need for long levers and pistol-grip handles, causing poor force transmission efficiency from the forearm to the hand. Three studies [9,10,21] examining surgeons with small glove sizes (i.e., <6.5) reported a low satisfaction level regarding the anastomotic staplers, as well as when using laparoscopic instruments in general. These findings suggest an unaccommodating environment, in which the usability of surgical tools is significantly compromised by different hand sizes and finger lengths. Furthermore, firing the stapler by gripping the proximal side of the lever was defined as “physically impossible” for most women with small glove sizes [9]. Kono et al. reported that the most appropriate stapler diameter for surgeons with a given hand size is not the same for male and female individuals, but needs to be established separately for each sex, ideally by developing smart instruments whose usability is not affected by the gender identity of the user [22]. This also applies to the ergonomics of handles for laparoscopic tools in general [16].
3.3. Impact on Training, Productivity, and Career Longevity
A positive correlation has been reported between higher pain scores and lower work satisfaction, burnout, and callousness toward others [23], meaning that poor ergonomics are not only an obstacle to progress in training and advancement in the surgical career, but also have a negative impact on leisure activities [13] and productivity [23], thus further decreasing the attractiveness of surgical specialties. However, self-selected settings were demonstrated to be improved by following objective surgeon postures, for both women and men [25], with low percentages of respondents reporting having received ergonomics education during surgical training [21].
4. Discussion
Among surgical specialties, a tacit acceptance of physical efforts in addition to the mental concentration required to perform complex operations has encouraged stoicism—particularly in the form of not reporting work-related injuries [13]. However, it is part of human nature to feel fatigue when operating for long periods without breaks, and it should not be labelled as a sign of weakness to seek alternatives, or to disclose the struggles that surgeons have been through. On the contrary, this review highlights the need to improve ergonomic challenges in operative settings so as to not discourage those who naturally have a different stature or muscular capacity in terms of their advancement or their feeling of belonging to the surgical field. This would really imply a true DEI environment in the operating theatre.
As already mentioned, women in general tend to have significantly less absolute and relative skeletal muscle mass [26], but nevertheless, they should not feel “unwelcome” to pursue a surgical career. Indeed, on the contrary, it is a sign of strength to recognise one’s own limitations; furthermore, for organisations to achieve true gender equity, important consideration must be given by providing women with the same opportunities to succeed, following the principles of DEI.
What could be the initial changes to adopt? Ergonomics education during training should be prioritised [27], as often younger colleagues might be at higher risk of muscular strain [28]. To assume the assistant role, in fact, often entails adapting to contorted body positions for holding instruments with prolonged retraction or, for shorter surgeons, reaching the table height might require them to use a step stool, which contributes to awkward postures to keep the surgical field in view.
It would be recommendable, therefore, to adjust the height of the monitor to a common level of suitability for the whole operating staff; eventually, the use of a second screen appears essential in considerations of different surgeons’ heights, aiming to place the screen at the centre, just below the eye level.
With regards to the instruments, as noted in the present review [9,10,18,22], there is evidence that an adjustment according to hand size—especially for those with smaller glove sizes, mainly female—is a priority so as to not discriminate in surgical practice. Unsurprisingly, two studies were from Japan, where the 2018 exposé of Tokyo Medical University [29]—which had reduced the scores of its female applicants over a period of at least 12 years to cap female entrants at 30%—revealed the regressive thinking unfortunately hindering medical practice in that country. Luckily, a more legal framework is now in place to prevent discrimination. Importantly, a more diverse staff also helps patients from minority backgrounds to feel better valued during their hospital stay. In fact, it is not uncommon to observe—because of religious and sociocultural beliefs—challenges for women to be assisted by male doctors or associated staff; therefore, to have an impact on patient health outcomes and quality of life, the care the same patients experience and how they perceive their representation is essential [30,31].
Additionally, a relatively low number of females generally participated in most of the analysed studies, highlighting the need for gender-focused research—especially in surgery, where the field is still male-dominated. Interestingly, according to a large Canadian registry analysis, patients treated by female surgeons had a decrease in 30-day mortality, length of stay, complications, and readmission, in comparison to those treated by male surgeons. These important findings could be the result of a higher level achieved by women who successfully completed their training, in view of a more uncomfortable environment that may have significantly impacted on the development of their performance and skills [32].
To overcome physical-related challenges, several solutions have been proposed, such as the use of chairs providing chest support and adjustable armrests, as well as footrests mounted with a bipolar control pedal. Those chairs, motor-driven and adjustable according to the patient’s and surgeon’s size, could be personalised, with the result of ergonomic improvement during excision and suturing, allowing the operation to be safely transferred to second generation of surgeons for training purposes [33]. The combination of standing with sitting would be also beneficial to lower down the risk of developing chronic venous disorders, known to be higher in professionals working in prolonged sitting or standing postures [34]. Operating surgeons should also be encouraged to take minibreaks during long operations, or to eventually perform stretching as a relief from the musculoskeletal grief accumulated. It is therefore highly recommendable to raise awareness of ergonomics for all theatre staff, aiming to optimise human wellbeing and overall system performance [11]. From the present review, educational interventions such as the one reported by Hokenstad et al. [20] improved objective surgeon posture at the console, when compared to the previous surgeons’ self-selected settings, demonstrating room for improvement towards higher surgeon awareness.
Another valuable solution could be the use of automated and personalised theatre tools, such as regulable laparoscopic instruments or smart technology able to read and translate tissue characteristics, thus alerting surgeons when and where to clip or to staple. The artificial intelligence applied in this way would allow, for instance, that staplers or clip applicators could be fired and handled by anyone, independently from the force a particular individual could provide.
The relatively low number of studies focusing on ergonomics for women in surgery limited the level of evidence we were able to achieve, based mainly on survey data and small sample size studies.
In conclusion, future research should focus on the mitigation of surgeons’ physical-related barriers and seek to understand the ergonomic gender differences that could act as an impediment during training and progression in the surgical career. This is of utmost importance in a context of full inclusivity, so as to acknowledge diverse medical device design and integrate technology and innovation to optimise human wellbeing and the overall system performance.
Author Contributions
Conceptualization, M.I.B. and V.D.; methodology, M.I.B., M.I.A. and P.S.; validation, M.I.B., M.I.A., P.S., N.Z. and R.C.; formal analysis, M.I.B. and M.I.A.; data curation, M.I.B., N.Z. and M.T.; writing—original draft preparation, M.I.B.; writing—review and editing, M.I.B., M.I.A., M.T., R.C. and V.D.; supervision, M.T., R.C. and V.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study, performed in accordance to the Declaration of Helsinki principles, is a retrospective analysis. The data used were anonymised; the study did not require patient or public involvement nor affected patient care. The study fell under the category of research through the use of anonymised data of existing databases which, based on the Health Research Authority criteria, does not require proportional or full ethics review and approval.
Informed Consent Statement
This is a review of published data, no informed consent was required.
Data Availability Statement
The data used to support the findings of this study are included within the article and are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stephens, E.H.; Heisler, C.A.; Temkin, S.M.; Miller, P. The Current Status of Women in Surgery: How to Affect the Future. JAMA Surg. 2020, 155, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Adair, A.; Fotopoulou, C.; Graham, Y.; Hutson, A.; McNally, S.; Mohan, H.; Vig, S.; Parks, R.; Papalois, V. Changing the norm towards gender equity in surgery: The women in surgery working group of the Association of Surgeons of Great Britain and Ireland’s perspective. J. R. Soc. Med. 2019, 112, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Dossa, F.; Zeltzer, D.; Sutradhar, R.; Simpson, A.N.; Baxter, N.N. Sex Differences in the Pattern of Patient Referrals to Male and Female Surgeons. JAMA Surg. 2022, 157, 95. [Google Scholar] [CrossRef] [PubMed]
- Bellini, M.I.; Graham, Y.; Hayes, C.; Zakeri, R.; Parks, R.; Papalois, V. A woman’s place is in theatre: Women’s perceptions and experiences of working in surgery from the Association of Surgeons of Great Britain and Ireland women in surgery working group. BMJ Open 2019, 9, e024349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenup, R.A.; Pitt, S.C. Women in Academic Surgery: A Double-Edged Scalpel. Acad. Med. 2020, 95, 1483–1484. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Jacob-Brassard, J.; Dossa, F.; Salata, K.; Kishibe, T.; Greco, E.; Baxter, N.N.; Al-Omran, M. Gender differences in faculty rank among academic physicians: A systematic review and meta-analysis. BMJ Open 2021, 11, e050322. [Google Scholar] [CrossRef]
- Murphy, M.; Record, H.; Callander, J.K.; Dohan, D.; Grandis, J.R. Mentoring Relationships and Gender Inequities in Academic Medicine: Findings from a Multi-Institutional Qualitative Study. Acad. Med. 2022, 97, 136–142. [Google Scholar] [CrossRef]
- Sutton, E.; Irvin, M.; Zeigler, C.; Lee, G.; Park, A. The ergonomics of women in surgery. Surg. Endosc. Other Interv. Tech. 2014, 28, 1051–1055. [Google Scholar] [CrossRef]
- Kono, E.; Tada, M.; Kouchi, M.; Endo, Y.; Tomizawa, Y.; Matsuo, T.; Nomura, S. Ergonomic evaluation of a mechanical anastomotic stapler used by Japanese surgeons. Surg. Today 2014, 44, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Berguer, R.; Hreljac, A. The relationship between hand size and difficulty using surgical instruments: A survey of 726 laparoscopic surgeons. Surg. Endosc. 2004, 18, 508–512. [Google Scholar] [CrossRef]
- Karwowski, W.; Rizzo, F.; Rodrick, D. Ergonomics. In Encyclopedia of Information Systems; Bidgoli, H., Ed.; Elsevier: New York, NY, USA, 2003; pp. 185–201. [Google Scholar]
- The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 December 2019).
- Adams, S.R.; Hacker, M.R.; McKinney, J.L.; Elkadry, E.A.; Rosenblatt, P.L. Musculoskeletal Pain in Gynecologic Surgeons. J. Minim. Invasive Gynecol. 2013, 20, 656–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aitchison, L.P.; Cui, C.K.; Arnold, A.; Nesbitt-Hawes, E.; Abbott, J. The ergonomics of laparoscopic surgery: A quantitative study of the time and motion of laparoscopic surgeons in live surgical environments. Surg. Endosc. Other Interv. Tech. 2016, 30, 5068–5076. [Google Scholar] [CrossRef] [PubMed]
- Armijo, P.R.; Flores, L.; Pokala, B.; Huang, C.K.; Siu, K.C.; Oleynikov, D. Gender equity in ergonomics: Does muscle effort in laparoscopic surgery differ between men and women? Surg. Endosc. Other Interv. Tech. 2022, 36, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Cavanagh, J.; Brake, M.; Kearns, D.; Hong, P. Work environment discomfort and injury: An ergonomic survey study of the American Society of Pediatric Otolaryngology members. Am. J. Otolaryngol. 2012, 33, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Dalsgaard, T.; Jensen, M.D.; Hartwell, D.; Mosgaard, B.J.; Jorgensen, A.; Jensen, B.R. Robotic Surgery Is Less Physically Demanding Than Laparoscopic Surgery Paired Cross Sectional Study. Ann. Surg. 2020, 271, 106–113. [Google Scholar] [CrossRef]
- Gonzalez, A.G.; Salgado, D.R.; García-Moruno, L. Optimisation of a laparoscopic tool handle dimension based on ergonomic analysis. Int. J. Ind. Ergon. 2015, 48, 16–24. [Google Scholar] [CrossRef]
- Harutunian, K.; Gargallo-Albiol, J.; Figueiredo, R.; Escoda, C.G. Ergonomics and musculoskeletal pain among postgraduate students and faculty members of the School of Dentistry of the University of Barcelona (Spain). A cross-sectional study. Med. Oral Patol. Oral Y Cir. Bucal. 2011, 16, e425–e429. [Google Scholar] [CrossRef] [Green Version]
- Hokenstad, E.D.; Hallbeck, M.S.; Lowndes, B.R.; Morrow, M.M.; Weaver, A.L.; McGree, M.; Glaser, G.E.; Occhino, J.A. Ergonomic Robotic Console Configuration in Gynecologic Surgery: An Interventional Study. J. Minim. Invasive Gynecol. 2021, 28, 850–859. [Google Scholar] [CrossRef]
- Jensen, M.J.; Pagedar, N.A.; Sugg, S.L.; Lal, G. Endocrine surgeons have high rates of work-related musculoskeletal (MSK) injury and symptoms. Am. J. Surg. 2021. [Google Scholar] [CrossRef]
- Kono, E.; Tomizawa, Y.; Matsuo, T.; Nomura, S. Rating and issues of mechanical anastomotic staplers in surgical practice: A survey of 241 Japanese gastroenterological surgeons. Surg. Today 2012, 42, 962–972. [Google Scholar] [CrossRef]
- McQuivey, K.S.; Deckey, D.G.; Christopher, Z.K.; Rosenow, C.S.; Mi, L.; Spangehl, M.J.; Bingham, J.S. Surgical Ergonomics and Musculoskeletal Pain in Orthopaedic Surgery Residents: A Multicenter Survey Study. JAAOS Glob. Res. Rev. 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.; Raoof, M.; Fong, Y.; Dellinger, T.; Warner, S. Who is hurting? A prospective study of surgeon ergonomics. Surg. Endosc. 2022, 36, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Bodin, J.; Ha, C.; Chastang, J.-F.; Descatha, A.; Leclerc, A.; Goldberg, M.; Imbernon, E.; Roquelaure, Y. Comparison of risk factors for shoulder pain and rotator cuff syndrome in the working population. Am. J. Ind. Med. 2012, 55, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Dopsaj, M.; Kukić, F.; Đorđević-Nikić, M.; Koropanovski, N.; Radovanović, D.; Miljuš, D.; Subošić, D.; Tomanić, M.; Dopsaj, V. Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing. Int. J. Environ. Res. Public Health 2020, 17, 5977. [Google Scholar] [CrossRef] [PubMed]
- Surma-Aho, A.; Hölttä-Otto, K.; Nelskylä, K.; Lindfors, N.C. Usability issues in the operating room—Towards contextual design guidelines for medical device design. Appl. Ergon. 2020, 90, 103221. [Google Scholar] [CrossRef] [PubMed]
- Barnard, E.; Sheaffer, K.; Hampton, S.; Measel, M.L.; Farag, A.; Shaw, C. Ergonomics and Work-Related Musculoskeletal Disorders: Characteristics Among Female Interventionists. Cureus 2021, 13, e18226. [Google Scholar] [CrossRef] [PubMed]
- Tokyo Medical University ‘Changed Female Exam Scores’. Available online: https://www.bbc.com/news/world-asia-45043818 (accessed on 30 May 2022).
- Wallis, C.J.D.; Jerath, A.; Coburn, N.; Klaassen, Z.; Luckenbaugh, A.N.; Magee, D.E.; Hird, A.E.; Armstrong, K.; Ravi, B.; Esnaola, N.F.; et al. Association of Surgeon-Patient Sex Concordance with Postoperative Outcomes. JAMA Surg. 2022, 157, 146. [Google Scholar] [CrossRef]
- Tong, A.; Oberbauer, R.; Bellini, M.I.; Budde, K.; Caskey, F.J.; Dobbels, F.; Pengel, L.; Rostaing, L.; Schneeberger, S.; Naesens, M. Patient-Reported Outcomes as Endpoints in Clinical Trials of Kidney Transplantation Interventions. Transpl. Int. 2022, 35, 10134. [Google Scholar] [CrossRef]
- Wallis, C.J.; Ravi, B.; Coburn, N.; Nam, R.K.; Detsky, A.S.; Satkunasivam, R. Comparison of postoperative outcomes among patients treated by male and female surgeons: A population based matched cohort study. BMJ 2017, 359, j4366. [Google Scholar] [CrossRef] [Green Version]
- Rassweiler, J.J.; Klein, J.; Tschada, A.; Gözen, A.S. Laparoscopic retroperitoneal partial nephrectomy using an ergonomic chair -demonstration of technique and matched-pair analysis. Br. J. Urol. 2016, 119, 349–357. [Google Scholar] [CrossRef]
- Sudoł-Szopińska, I.; Bogdan, A.; Szopinski, T.; Panorska, A.K.; Kołodziejczak, M. Prevalence of Chronic Venous Disorders Among Employees Working in Prolonged Sitting and Standing Postures. Int. J. Occup. Saf. Ergon. 2011, 17, 165–173. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).