
The Prognostic Value of Deleted in Colorectal Cancer (DCC) Receptor and Serum Netrin-1 in Severe Traumatic Brain Injury

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Variables
2.3. Immunohistochemistry
2.4. ELISA Analysis
2.5. Statistical Methods
3. Results
3.1. Baseline Patient Characteristics
3.2. The Relationship between Serum Netrin-1 Concentrations and Trauma Severity
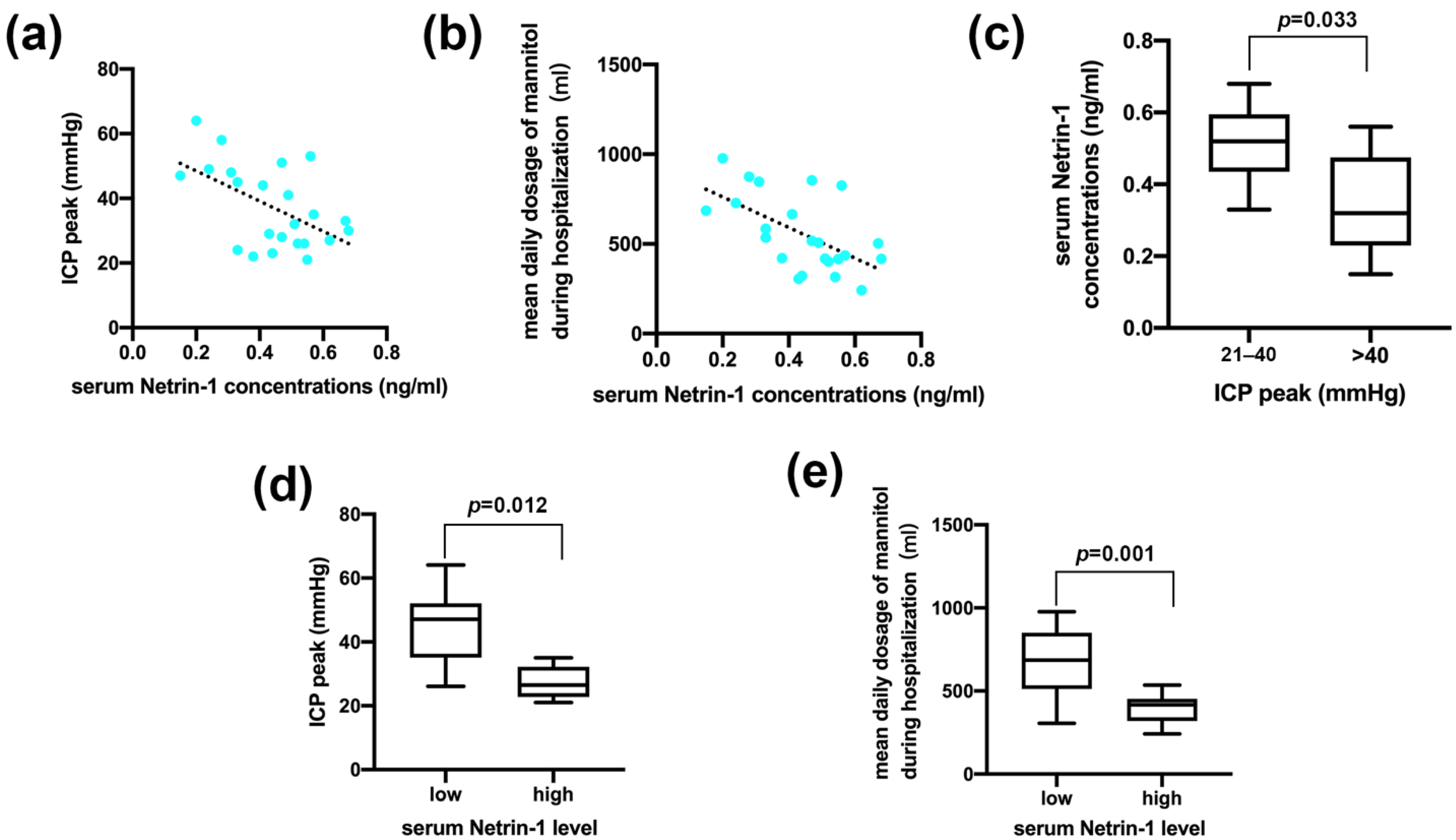
3.3. Serum Netrin-1 Level Indicated Postoperative Intracranial Pressure and Sensitivity to Dehydration Therapy
3.4. Positive DCC Receptors Indicated Postoperative Intracranial Pressure and Sensitivity to Dehydration Therapy
3.5. Serum Netrin-1 Levels Did Not Evaluate Prognosis, While the Expression of DCC Receptors Reflected the Prognosis of TBI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jiang, J.-Y.; Gao, G.-Y.; Feng, J.-F.; Mao, Q.; Chen, L.-G.; Yang, X.-F.; Liu, J.-F.; Wang, Y.-H.; Qiu, B.-H.; Huang, X.-J. Traumatic brain injury in China. Lancet Neurol. 2019, 18, 286–295. [Google Scholar] [CrossRef]
- Gao, G.; Wu, X.; Feng, J.; Hui, J.; Mao, Q.; Lecky, F.; Lingsma, H.; Maas, A.I.R.; Jiang, J. Clinical characteristics and outcomes in patients with traumatic brain injury in China: A prospective, multicentre, longitudinal, observational study. Lancet Neurol. 2020, 19, 670–677. [Google Scholar] [CrossRef]
- McGinn, M.J.; Povlishock, J.T. Pathophysiology of Traumatic Brain Injury. Neurosurg. Clin. North Am. 2016, 27, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Unterberg, A.W.; Stover, J.; Kress, B.; Kiening, K.L. Edema and brain trauma. Neuroscience 2004, 129, 1021–1029. [Google Scholar] [CrossRef]
- Pan, Y.; Xue, Y.; Zhao, P.; Ding, J.; Ren, Z.; Xu, J. Significance of ICP-related parameters for the treatment and outcome of severe traumatic brain injury. J. Int. Med. Res. 2020, 48, 300060520941291. [Google Scholar] [CrossRef]
- Berger, R.P.; Pierce, M.C.; Wisniewski, S.R.; Adelson, P.D.; Clark, R.S.B.; Ruppel, R.A.; Kochanek, P.M. Neuron-specific enolase and S100B in cerebrospinal fluid after severe traumatic brain injury in infants and children. Pediatrics 2002, 109, E31. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Akinyi, L.; Scharf, D.; Mo, J.; Larner, S.F.; Muller, U.; Oli, M.W.; Zheng, W.; Kobeissy, F.; Papa, L.; et al. Ubiquitin C-terminal hydrolase-L1 as a biomarker for ischemic and traumatic brain injury in rats. Eur. J. Neurosci. 2010, 31, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Nylén, K.; Ost, M.; Csajbok, L.Z.; Nilsson, I.; Blennow, K.; Nellgård, B.; Rosengren, L. Increased serum-GFAP in patients with severe traumatic brain injury is related to outcome. J. Neurol. Sci. 2006, 240, 85–91. [Google Scholar] [CrossRef]
- Schulte, S.; Podlog, L.W.; Hamson-Utley, J.J.; Strathmann, F.G.; Strüder, H.K. A systematic review of the biomarker S100B: Implications for sport-related concussion management. J. Athl. Train. 2014, 49, 830–850. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.J.; Scheff, S.W.; Miller, K.M.; Roberts, K.N.; Gilmer, L.K.; Yang, C.; Shaw, G. The phosphorylated axonal form of the neurofilament subunit NF-H (pNF-H) as a blood biomarker of traumatic brain injury. J. Neurotrauma 2008, 25, 1079–1085. [Google Scholar] [CrossRef]
- Ringger, N.C.; O’Steen, B.E.; Brabham, J.G.; Silver, X.; Pineda, J.; Wang, K.K.W.; Hayes, R.L.; Papa, L. A novel marker for traumatic brain injury: CSF alphaII-spectrin breakdown product levels. J. Neurotrauma 2004, 21, 1443–1456. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, E.; Dalmau, J. Neuronal autoantigens—Pathogenesis, associated disorders and antibody testing. Nat. Rev. Neurol. 2012, 8, 380–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.H.; Chen, X.H.; Nonaka, M.; Trojanowski, J.Q.; Lee, V.M.; Saatman, K.E.; Leoni, M.J.; Xu, B.N.; Wolf, J.A.; Meaney, D.F. Accumulation of amyloid beta and tau and the formation of neurofilament inclusions following diffuse brain injury in the pig. J. Neuropathol. Exp. Neurol. 1999, 58, 982–992. [Google Scholar] [CrossRef]
- Dun, X.-P.; Parkinson, D.B. Role of Netrin-1 Signaling in Nerve Regeneration. Int. J. Mol. Sci. 2017, 18, 491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegon, L.; Schlegel, M. Netrin-1: A Modulator of Macrophage Driven Acute and Chronic Inflammation. Int. J. Mol. Sci. 2021, 23, 275. [Google Scholar] [CrossRef]
- Liu, L.; Xie, S.; Liao, X.; Zhang, L.; Zhong, L. Netrin-1 pretreatment protects rat kidney against ischemia/reperfusion injury via suppression of oxidative stress and neuropeptide Y expression. J. Biochem. Mol. Toxicol. 2013, 27, 231–236. [Google Scholar] [CrossRef]
- Xie, Y.; Guo, Z.; Chen, F.; Xiao, C.; Xu, J.; Bo, D. Serum netrin-1 as a potential biomarker for functional outcome of traumatic brain injury. Clin. Chim. Acta; Int. J. Clin. Chem. 2021, 518, 22–27. [Google Scholar] [CrossRef]
- Ly, N.P.; Komatsuzaki, K.; Fraser, I.P.; Tseng, A.A.; Prodhan, P.; Moore, K.J.; Kinane, T.B. Netrin-1 inhibits leukocyte migration in vitro and in vivo. Proc. Natl. Acad. Sci. USA 2005, 102, 14729–14734. [Google Scholar] [CrossRef] [Green Version]
- Meijers, R.; Smock, R.G.; Zhang, Y.; Wang, J.-H. Netrin Synergizes Signaling and Adhesion through DCC. Trends Biochem. Sci. 2020, 45, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Huang, L.; Enkhjargal, B.; Reis, C.; Wan, W.; Tang, J.; Cheng, Y.; Zhang, J.H. Intranasal administration of recombinant Netrin-1 attenuates neuronal apoptosis by activating DCC/APPL-1/AKT signaling pathway after subarachnoid hemorrhage in rats. Neuropharmacology 2017, 119, 123–133. [Google Scholar] [CrossRef]
- Zang, Y.; Guo, D.; Chen, L.; Yang, P.; Zhu, Z.; Bu, X.; Xu, T.; Zhong, C.; Wang, A.; Peng, H.; et al. Association between serum netrin-1 and prognosis of ischemic stroke: The role of lipid component levels. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, S.; Li, B.; Wang, X.; Sun, C.; Qin, H.; Sun, H. Netrin-1 overexpression improves neurobehavioral outcomes and reduces infarct size via inhibition of the notch1 pathway following experimental stroke. J. Neurosci. Res. 2017, 95, 1850–1857. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Huang, L.; Enkhjargal, B.; Reis, C.; Wan, W.; Tang, J.; Cheng, Y.; Zhang, J.H. Recombinant Netrin-1 binding UNC5B receptor attenuates neuroinflammation and brain injury via PPARγ/NFκB signaling pathway after subarachnoid hemorrhage in rats. Brain Behav. Immun. 2018, 69, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Finci, L.; Zhang, Y.; Meijers, R.; Wang, J.H. Signaling mechanism of the netrin-1 receptor DCC in axon guidance. Prog. Biophys. Mol. Biol. 2015, 118, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Lin, F.; Jiang, J.; Chen, Y.; Mei, A.; Zhu, P. Effects of intra-arterial transplantation of adipose-derived stem cells on the expression of netrin-1 and its receptor DCC in the peri-infarct cortex after experimental stroke. Stem Cell Res. Ther. 2017, 8, 223. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.Q.; Hsieh, J.T.; Yao, F.; Fang, B.; Pong, R.C.; Cipriano, S.C.; Krepulat, F. Induction of apoptosis and G2/M cell cycle arrest by DCC. Oncogene 1999, 18, 2747–2754. [Google Scholar] [CrossRef] [Green Version]
- Webber, C.A.; Christie, K.J.; Cheng, C.; Martinez, J.A.; Singh, B.; Singh, V.; Thomas, D.; Zochodne, D.W. Schwann cells direct peripheral nerve regeneration through the Netrin-1 receptors, DCC and Unc5H2. Glia 2011, 59, 1503–1517. [Google Scholar] [CrossRef]
- Wang, X.; Xu, J.; Gong, J.; Shen, H.; Wang, X. Expression of netrin-1 and its receptors, deleted in colorectal cancer and uncoordinated locomotion-5 homolog B, in rat brain following focal cerebral ischemia reperfusion injury. Neural Regen. Res. 2013, 8, 64–69. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CT Findings | Score |
|---|---|
| Basal cisterns | |
| Normal | 0 |
| Compressed | 1 |
| Absent | 2 |
| Midline shift of the brain parenchyma | |
| ≤5 mm | 0 |
| ≥5 mm | 1 |
| Epidural hematoma, brain contusion or other occupying lesions | |
| Yes | 0 |
| No | 1 |
| Intraventricular hemorrhage or subarachnoid hemorrhage | |
| Yes | 0 |
| No | 1 |
| Total | +1 |
| All Patients (n = 23) | ICP Level | GOS Score | |||
|---|---|---|---|---|---|
| Moderate | Severe | Unfavorable | Favorable | ||
| (n = 13) | (n = 10) | (n = 15) | (n = 8) | ||
| Gender (male/female) | 11/12 | 6/7 | 5/5 | 7/8 | 4/4 |
| Age (y) | 49.48 ± 15.65 | 44.15 ± 12.79 | 56.40 ± 16.30 | 44.87 ± 13.38 | 58.13 ± 15.92 |
| Hypertension | 11 (47.83%) | 4 (30.77%) | 7 (70.00%) | 7 (46.67%) | 4 (50.00%) |
| Diabetes mellitus | 8 (34.78%) | 5 (38.46%) | 3 (30.00%) | 6 (40.00%) | 2 (25.00%) |
| Coronary heart disease | 4 (17.39%) | 2 (15.38%) | 2 (20.00%) | 2 (13.33%) | 2 (25.00%) |
| Mean temperature of mild hypothermia therapy (°C) | 33.54 ± 0.44 | 33.44 ± 0.39 | 33.65 ± 0.46 | 33.59 ± 0.54 | 33.52 ± 0.37 |
| Average dose of dexmedetomidine (μg/kg/d) | 15.18 ± 1.87 | 15.12 ± 1.94 | 15.24 ± 1.78 | 14.83 ± 1.77 | 15.36 ± 1.89 |
| ICP Level (mmHg) | Total | |||
|---|---|---|---|---|
| 21–40 | >40 | |||
| Low Netrin-1 | 3 | 10 | 13 | p = 0.001 |
| High Netrin-1 | 9 | 1 | 10 | |
| Total | 12 | 11 | 23 | |
| ICP Level (mmHg) | Total | ||||
|---|---|---|---|---|---|
| 21–40 | >40 | ||||
| High Netrin-1 (n = 10) | DCC (+) | 8 | 0 | 8 | p = 0.035 |
| DCC (−) | 1 | 1 | 2 | ||
| Total | 9 | 1 | 10 | ||
| UNC5B (+) | 6 | 1 | 7 | p = 0.490 | |
| UNC5B (−) | 3 | 0 | 3 | ||
| Total | 9 | 1 | 10 | ||
| Low Netrin-1 (n = 13) | DCC (+) | 2 | 0 | 2 | p = 0.005 |
| DCC (−) | 1 | 10 | 11 | ||
| Total | 3 | 10 | 13 | ||
| UNC5B (+) | 1 | 7 | 8 | p = 0.252 | |
| UNC5B (−) | 2 | 3 | 5 | ||
| Total | 3 | 10 | 13 | ||
| ICP Level (mmHg) | Total | |||
|---|---|---|---|---|
| 21–40 | >40 | |||
| DCC (+) | 10 | 0 | 10 | p = 0.000 |
| DCC (−) | 2 | 11 | 13 | |
| Total | 12 | 11 | 23 | |
| UNC5B (+) | 8 | 7 | 15 | p = 0.879 |
| UNC5B (−) | 4 | 4 | 8 | |
| Total | 12 | 11 | 23 | |
| GOS Score | Total | |||
|---|---|---|---|---|
| 1–3 | 4–5 | |||
| Low Netrin-1 | 7 | 6 | 13 | p = 0.192 |
| High Netrin-1 | 8 | 2 | 10 | |
| Total | 15 | 8 | 23 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zhang, Q.; Sun, L.; Zhao, D.; Ruan, C.; Zhou, J.; Tan, H.; Bao, Y. The Prognostic Value of Deleted in Colorectal Cancer (DCC) Receptor and Serum Netrin-1 in Severe Traumatic Brain Injury. J. Clin. Med. 2022, 11, 3700. https://doi.org/10.3390/jcm11133700
Zhang Y, Zhang Q, Sun L, Zhao D, Ruan C, Zhou J, Tan H, Bao Y. The Prognostic Value of Deleted in Colorectal Cancer (DCC) Receptor and Serum Netrin-1 in Severe Traumatic Brain Injury. Journal of Clinical Medicine. 2022; 11(13):3700. https://doi.org/10.3390/jcm11133700
Chicago/Turabian StyleZhang, Yuanda, Qiao Zhang, Lihua Sun, Dongxu Zhao, Cijie Ruan, Jue Zhou, Haoyuan Tan, and Yinghui Bao. 2022. "The Prognostic Value of Deleted in Colorectal Cancer (DCC) Receptor and Serum Netrin-1 in Severe Traumatic Brain Injury" Journal of Clinical Medicine 11, no. 13: 3700. https://doi.org/10.3390/jcm11133700
APA StyleZhang, Y., Zhang, Q., Sun, L., Zhao, D., Ruan, C., Zhou, J., Tan, H., & Bao, Y. (2022). The Prognostic Value of Deleted in Colorectal Cancer (DCC) Receptor and Serum Netrin-1 in Severe Traumatic Brain Injury. Journal of Clinical Medicine, 11(13), 3700. https://doi.org/10.3390/jcm11133700