
Fibrillatory Wave Amplitude Evolution during Persistent Atrial Fibrillation Ablation: Implications for Atrial Substrate and Fibrillation Complexity Assessment

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Electroanatomical Mapping and Ablation Procedure
2.3. Follow-Up
2.4. Signal Acquisition
2.5. Signal Processing
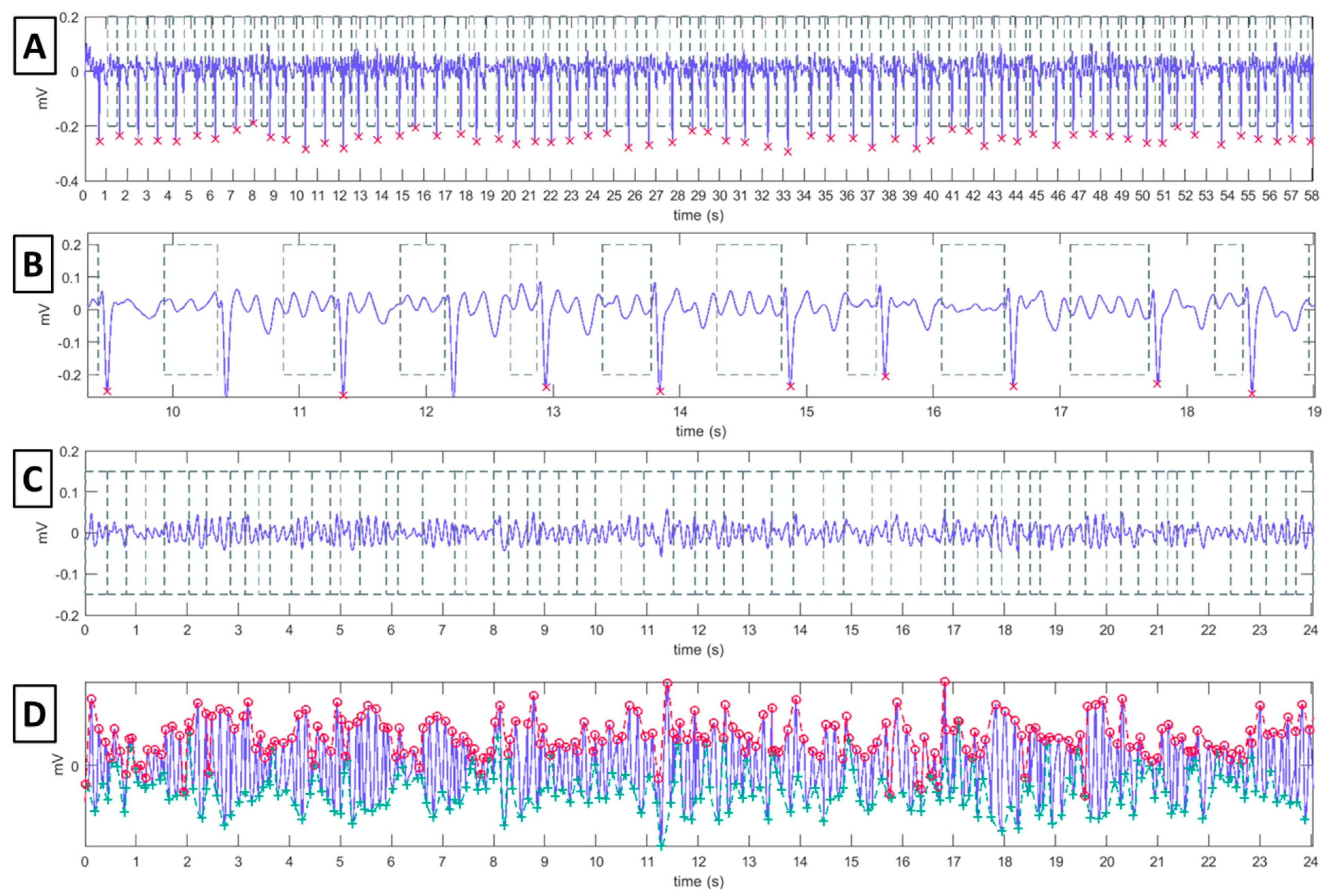
2.5.1. F-Wave and P-Wave Amplitude Computation
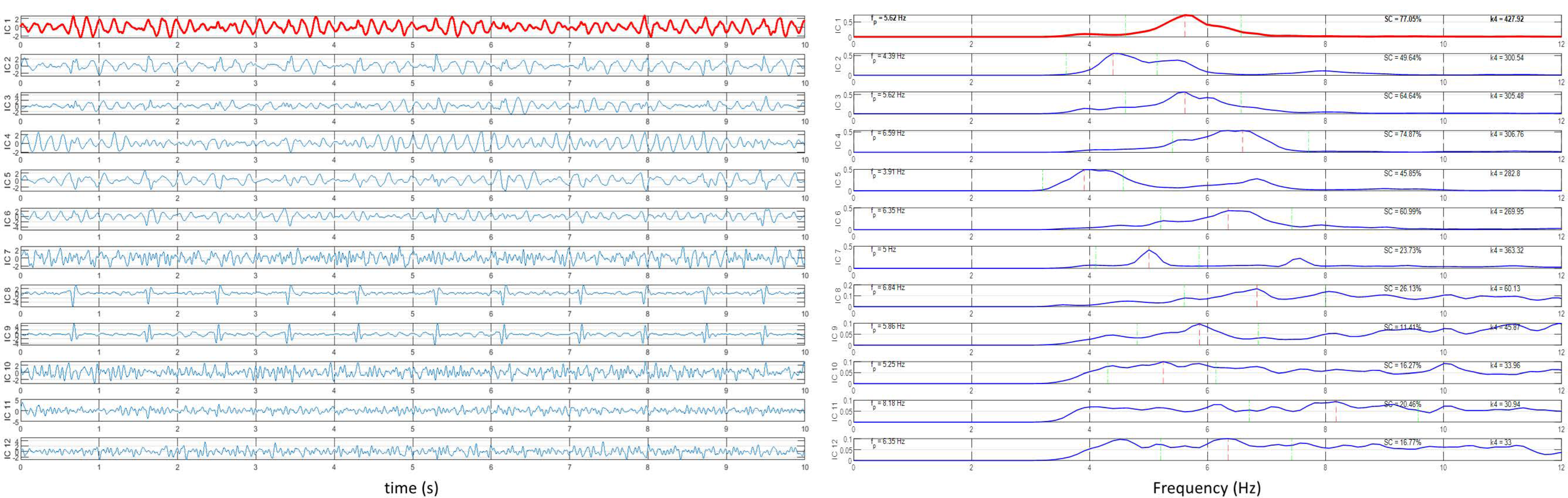
2.5.2. AF Dominant Frequency Assessment
2.6. Statistical Analysis
3. Results
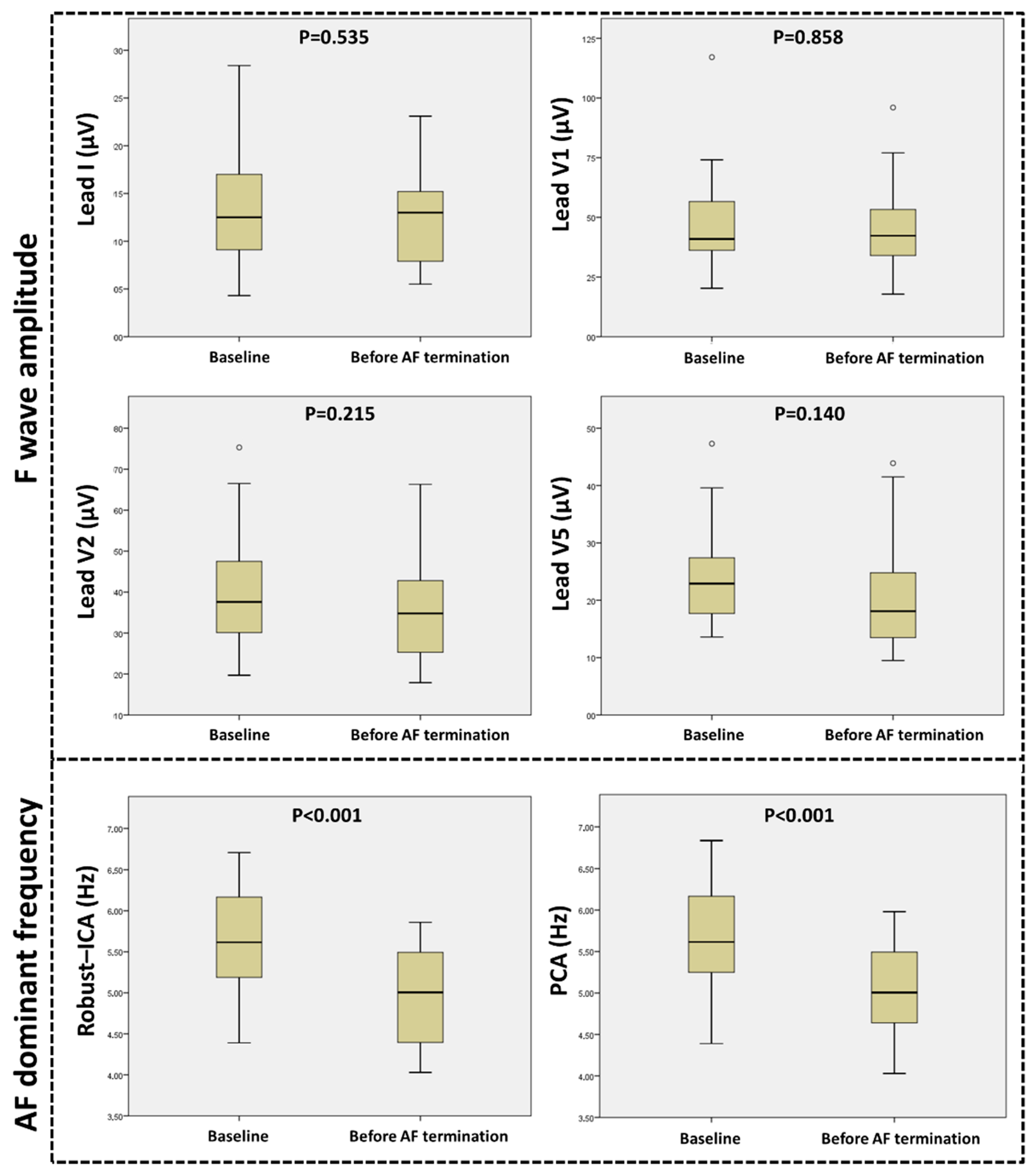
3.1. F-Wave Amplitude Evolution and Correlation with AF Complexity Parameters
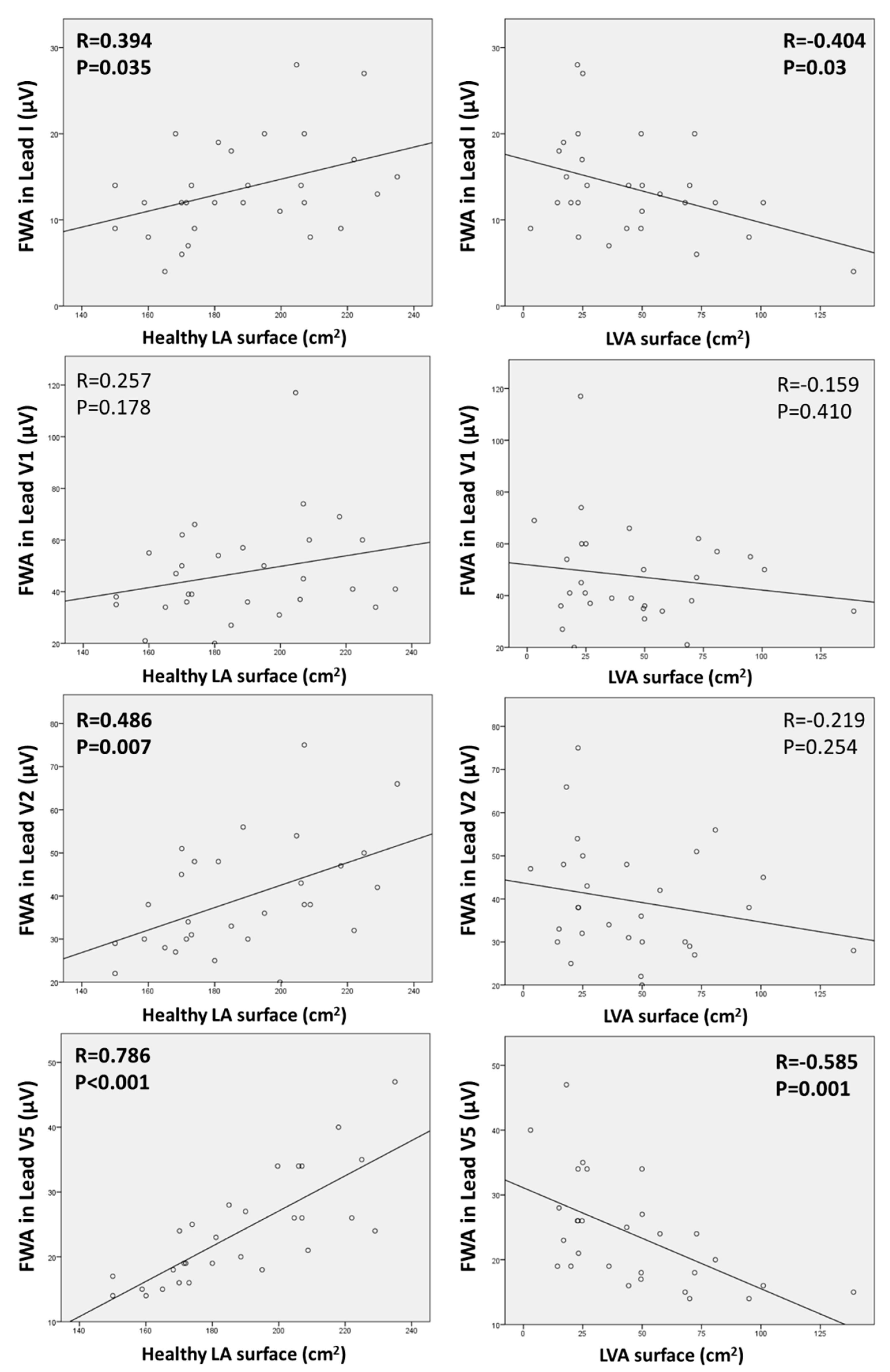
3.2. Relationship between ECG Parameters and the Extent of Anatomical LA Substrate
3.3. Relation between F-Wave Amplitude and P-Wave Amplitude
3.4. AF Termination and Follow-Up
4. Discussion
4.1. Main Results
4.2. Previous Studies and Purpose of FWA Assessment
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 esc guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the european association for cardio-thoracic surgery (eacts): The task force for the diagnosis and management of atrial fibrillation of the european society of cardiology (esc) developed with the special contribution of the european heart rhythm association (ehra) of the esc. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Lankveld, T.A.; Zeemering, S.; Crijns, H.J.; Schotten, U. The ecg as a tool to determine atrial fibrillation complexity. Heart 2014, 100, 1077–1084. [Google Scholar] [CrossRef]
- Cheng, Z.; Deng, H.; Cheng, K.; Chen, T.; Gao, P.; Yu, M.; Fang, Q. The amplitude of fibrillatory waves on leads avf and v1 predicting the recurrence of persistent atrial fibrillation patients who underwent catheter ablation. Ann. Noninvasive Electrocardiol. Off. J. Int. Soc. Holter Noninvasive Electrocardiol. Inc. 2013, 18, 352–358. [Google Scholar] [CrossRef]
- Lankveld, T.; Zeemering, S.; Scherr, D.; Kuklik, P.; Hoffmann, B.A.; Willems, S.; Pieske, B.; Haïssaguerre, M.; Jaïs, P.; Crijns, H.J.; et al. Atrial fibrillation complexity parameters derived from surface ecgs predict procedural outcome and long-term follow-up of stepwise catheter ablation for atrial fibrillation. Circ. Arrhythm. Electrophysiol. 2016, 9, e003354. [Google Scholar] [CrossRef] [Green Version]
- Nault, I.; Lellouche, N.; Matsuo, S.; Knecht, S.; Wright, M.; Lim, K.T.; Sacher, F.; Platonov, P.; Deplagne, A.; Bordachar, P.; et al. Clinical value of fibrillatory wave amplitude on surface ecg in patients with persistent atrial fibrillation. J. Interv. Card. Electrophysiol. 2009, 26, 11–19. [Google Scholar] [CrossRef]
- Zarzoso, V.; Latcu, D.G.; Hidalgo-Muñoz, A.R.; Meo, M.; Meste, O.; Popescu, I.; Saoudi, N. Non-invasive prediction of catheter ablation outcome in persistent atrial fibrillation by fibrillatory wave amplitude computation in multiple electrocardiogram leads. Arch. Cardiovasc. Dis. 2016, 109, 679–688. [Google Scholar] [CrossRef]
- de Groot, N.M.; Houben, R.P.; Smeets, J.L.; Boersma, E.; Schotten, U.; Schalij, M.J.; Crijns, H.; Allessie, M.A. Electropathological substrate of longstanding persistent atrial fibrillation in patients with structural heart disease: Epicardial breakthrough. Circulation 2010, 122, 1674–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seitz, J.; Bars, C.; Théodore, G.; Beurtheret, S.; Lellouche, N.; Bremondy, M.; Ferracci, A.; Faure, J.; Penaranda, G.; Yamazaki, M.; et al. Af ablation guided by spatiotemporal electrogram dispersion without pulmonary vein isolation: A wholly patient-tailored approach. J. Am. Coll. Cardiol. 2017, 69, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Nademanee, K.; McKenzie, J.; Kosar, E.; Schwab, M.; Sunsaneewitayakul, B.; Vasavakul, T.; Khunnawat, C.; Ngarmukos, T. A new approach for catheter ablation of atrial fibrillation: Mapping of the electrophysiologic substrate. J. Am. Coll. Cardiol. 2004, 43, 2044–2053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Mañero, M.; Valderrábano, M.; Baluja, A.; Kreidieh, O.; Martínez-Sande, J.L.; García-Seara, J.; Saenen, J.; Iglesias-Álvarez, D.; Bories, W.; Villamayor-Blanco, L.M.; et al. Validating left atrial low voltage areas during atrial fibrillation and atrial flutter using multielectrode automated electroanatomic mapping. JACC Clin. Electrophysiol. 2018, 4, 1541–1552. [Google Scholar] [CrossRef]
- Chelu, M.G.; King, J.B.; Kholmovski, E.G.; Ma, J.; Gal, P.; Marashly, Q.; AlJuaid, M.A.; Kaur, G.; Silver, M.A.; Johnson, K.A.; et al. Atrial fibrosis by late gadolinium enhancement magnetic resonance imaging and catheter ablation of atrial fibrillation: 5-year follow-up data. J. Am. Heart Assoc. 2018, 7, e006313. [Google Scholar] [CrossRef] [Green Version]
- Pokushalov, E.; Romanov, A.; Corbucci, G.; Artyomenko, S.; Turov, A.; Shirokova, N.; Karaskov, A. Use of an implantable monitor to detect arrhythmia recurrences and select patients for early repeat catheter ablation for atrial fibrillation: A pilot study. Circ. Arrhythm. Electrophysiol. 2011, 4, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Pokushalov, E.; Romanov, A.; Corbucci, G.; Bairamova, S.; Losik, D.; Turov, A.; Shirokova, N.; Karaskov, A.; Mittal, S.; Steinberg, J.S. Does atrial fibrillation burden measured by continuous monitoring during the blanking period predict the response to ablation at 12-month follow-up? Heart Rhythm 2012, 9, 1375–1379. [Google Scholar] [CrossRef]
- Andrade, J.G.; Khairy, P.; Macle, L.; Packer, D.L.; Lehmann, J.W.; Holcomb, R.G.; Ruskin, J.N.; Dubuc, M. Incidence and significance of early recurrences of atrial fibrillation after cryoballoon ablation: Insights from the multicenter stop af trial. Circ. Arrhythm. Electrophysiol. 2014, 7, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Meo, M.; Zarzoso, V.; Meste, O.; Latcu, D.G.; Saoudi, N. Spatial variability of the 12-lead surface ecg as a tool for noninvasive prediction of catheter ablation outcome in persistent atrial fibrillation. IEEE Trans. Biomed. Eng. 2013, 60, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Tompkins, W.J. A real-time qrs detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Cabasson, A.; Meste, O. Time delay estimation: A new insight into the woody’s method. IEEE Signal Processing Lett. 2008, 15, 573–576. [Google Scholar] [CrossRef]
- Bollmann, A.; Husser, D.; Mainardi, L.; Lombardi, F.; Langley, P.; Murray, A.; Rieta, J.J.; Millet, J.; Olsson, S.B.; Stridh, M.; et al. Analysis of surface electrocardiograms in atrial fibrillation: Techniques, research, and clinical applications. Europace 2006, 8, 911–926. [Google Scholar] [CrossRef]
- de Oliveira, P.M.R.; Goulart, J.D.M.; Fernandes, C.A.R.; Zarzoso, V. Blind source separation in persistent atrial fibrillation electrocardiograms using block-term tensor decomposition with lwner constraints. IEEE J. Biomed. Health Inform. 2021, 26, 1538–1548. [Google Scholar] [CrossRef]
- Rieta, J.J.; Castells, F.; Sánchez, C.; Zarzoso, V.; Millet, J. Atrial activity extraction for atrial fibrillation analysis using blind source separation. IEEE Trans. Biomed. Eng. 2004, 51, 1176–1186. [Google Scholar] [CrossRef] [Green Version]
- Zarzoso, V.; Comon, P. Robust independent component analysis by iterative maximization of the kurtosis contrast with algebraic optimal step size. IEEE Trans. Neural Netw. 2010, 21, 248–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castells, F.; Rieta, J.J.; Millet, J.; Zarzoso, V. Spatiotemporal blind source separation approach to atrial activity estimation in atrial tachyarrhythmias. IEEE Trans. Biomed. Eng. 2005, 52, 258–267. [Google Scholar] [CrossRef]
- Henriksson, M.; García-Alberola, A.; Goya, R.; Vadillo, A.; Melgarejo-Meseguer, F.M.; Sandberg, F.; Sörnmo, L. Changes in f-wave characteristics during cryoballoon catheter ablation. Physiol. Meas. 2018, 39, 105001. [Google Scholar] [CrossRef] [PubMed]
- McCann, A.; Vesin, J.M.; Pruvot, E.; Roten, L.; Sticherling, C.; Luca, A. Ecg-based indices to characterize persistent atrial fibrillation before and during stepwise catheter ablation. Front. Physiol. 2021, 12, 654053. [Google Scholar] [CrossRef]
- Haïssaguerre, M.; Sanders, P.; Hocini, M.; Takahashi, Y.; Rotter, M.; Sacher, F.; Rostock, T.; HSU, L.F.; Bordachar, P.; Reuter, S.; et al. Catheter ablation of long-lasting persistent atrial fibrillation: Critical structures for termination. J. Cardiovasc. Electrophysiol. 2005, 16, 1125–1137. [Google Scholar] [CrossRef]
- Yoshida, K.; Chugh, A.; Good, E.; Crawford, T.; Myles, J.; Veerareddy, S.; Billakanty, S.; Wong, W.S.; Ebinger, M.; Pelosi, F.; et al. A critical decrease in dominant frequency and clinical outcome after catheter ablation of persistent atrial fibrillation. Heart Rhythm 2010, 7, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, T.; Kähler, N.; Tscholl, V.; Nagel, P.; Blaschke, F.; Landmesser, U.; Attanasio, P.; Huemer, M. Correlation of p-wave properties with the size of left atrial low voltage areas in patients with atrial fibrillation. J. Electrocardiol. 2019, 56, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Morgan, R.; Colman, M.A.; Chubb, H.; Seemann, G.; Aslanidi, O.V. Slow conduction in the border zones of patchy fibrosis stabilizes the drivers for atrial fibrillation: Insights from multi-scale human atrial modeling. Front. Physiol. 2016, 7, 474. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 29 | |
|---|---|
| Age (y) | 67.9 ± 9.2 |
| Female gender (n; %) | 8/29; 27.6% |
| AF duration (months) | 21.7 ± 20.4 |
| Left atrial volume (mL) | 169.7 ± 37.1 |
| AF cycle length in LAA (ms) | 180.4 ± 24.3 |
| Number of LA dispersion-fragmentation zones per patient (n) | 5.5 ± 1.5 |
| Total LA surface of dispersion-fragmentation zones (cm2) | 21.3 ± 8.7 |
| Total LA surface of dispersion-fragmentation zones/Total LA surface (%) | 8.9 ± 3.6 |
| Right pulmonary vein ostium dispersion-fragmentation zone (n; %) | 26/29; 89.7% |
| Left pulmonary vein ostium dispersion-fragmentation zone (n; %) | 26/29; 89.7% |
| Anterior dispersion-fragmentation zone (n; %) | 21/29; 72.4% |
| Left atrial appendage ostium dispersion-fragmentation zone (n; %) | 13/29; 44.8% |
| Roof dispersion-fragmentation zone (n; %) | 19/29; 65.5% |
| Septal dispersion-fragmentation zone (n; %) | 19/29; 65.5% |
| Floor dispersion-fragmentation zone (n; %) | 6/29; 20.7% |
| Lateral mitral isthmus dispersion-fragmentation zone (n; %) | 8/29; 27.6% |
| Basal AF dominant frequency (Hz) | 5.31 ± 0.72 |
| Basal F-wave amplitude in lead I (µV) | 13.6 ± 5.7 |
| Basal F-wave amplitude in lead V1 (µV) | 47.4 ± 19.3 |
| Basal F-wave amplitude in lead V2 (µV) | 39.5 ± 13.0 |
| Basal F-wave amplitude in lead V5 (µV) | 23.9 ± 8.4 |
| AF termination during radiofrequency ablation procedure (n; %) | 19/29; 65.5% |
| Follow-up duration (months) | 23.3 ± 9.8 |
| AF recurrence (n; %) | 2/29; 6.9% |
| Recurrence of any atrial arrhythmia (n; %) | 13/29; 44.8% |
| Follow-up duration to any atrial arrhythmia recurrence (months) | 4.0 [3.0–6.2] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Squara, F.; Scarlatti, D.; Bun, S.-S.; Moceri, P.; Ferrari, E.; Meste, O.; Zarzoso, V. Fibrillatory Wave Amplitude Evolution during Persistent Atrial Fibrillation Ablation: Implications for Atrial Substrate and Fibrillation Complexity Assessment. J. Clin. Med. 2022, 11, 4519. https://doi.org/10.3390/jcm11154519
Squara F, Scarlatti D, Bun S-S, Moceri P, Ferrari E, Meste O, Zarzoso V. Fibrillatory Wave Amplitude Evolution during Persistent Atrial Fibrillation Ablation: Implications for Atrial Substrate and Fibrillation Complexity Assessment. Journal of Clinical Medicine. 2022; 11(15):4519. https://doi.org/10.3390/jcm11154519
Chicago/Turabian StyleSquara, Fabien, Didier Scarlatti, Sok-Sithikun Bun, Pamela Moceri, Emile Ferrari, Olivier Meste, and Vicente Zarzoso. 2022. "Fibrillatory Wave Amplitude Evolution during Persistent Atrial Fibrillation Ablation: Implications for Atrial Substrate and Fibrillation Complexity Assessment" Journal of Clinical Medicine 11, no. 15: 4519. https://doi.org/10.3390/jcm11154519