
Efficacy and Safety of Empagliflozin in Type 2 Diabetes Mellitus Saudi Patients as Add-On to Antidiabetic Therapy: A Prospective, Open-Label, Observational Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Patient Demographics at Baseline
2.3. Data Analysis
3. Results
3.1. Efficacy
3.2. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes-Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef]
- Meo, S.A. Prevalence and future prediction of type 2 diabetes mellitus in the Kingdom of Saudi Arabia: A systematic review of published studies. JPMA. J. Pak. Med. Assoc. 2017, 66, 722–725. [Google Scholar]
- Al Dawish, A.A.; Robert, A.; Braham, M.; Musallam, R.A.; Al Hayek, M.A.; Nasser, A.H. Type 2 Diabetes Mellitus in Saudi Arabia: Major Challenges and Possible Solutions. Curr. Diabetes Rev. 2017, 133, 59–64. [Google Scholar]
- Alotaibi, A.; Perry, L.; Gholizadeh, L.; Al-Ganmi, A. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: An overview. J. Epidemiol. Glob. Health 2017, 7, 211–218. [Google Scholar] [CrossRef]
- Robert, A.A.; Al Awad, A.D.; Al Dawish, M.A. Current Status of Knowledge and Awareness of Diabetes Mellitus in Saudi Arabia. Curr. Diabetes Rev. 2021, 15, e101220186818. [Google Scholar] [CrossRef]
- FDA. US Food and Drug Adminstration: FDA Approves Jardiance (empagliflozin) to Treat Type 2 Diabetes. Available online: https://www.fda-approves-jardiance-empagliflozin-type-2-diabetes-4064.html (accessed on 1 August 2014).
- Pan, D.; Xu, L.; Chen, P.; Jiang, H.; Shi, D.; Guo, M. Empagliflozin in Patients With Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Cardiovasc. Med. 2021, 8, 683281. [Google Scholar] [CrossRef]
- Frampton, J.E. Empagliflozin: A Review in Type 2 Diabetes. Drugs 2018, 78, 1037–1048. [Google Scholar] [CrossRef]
- Ridgefield, C. Jardiance (Empagliflozin) Tablets [Prescribing Information]; Boehringer Ingelheim Pharmaceuticals: Ingelheim am Rhein, Germany, 2014. [Google Scholar]
- Fala, L. Jardiance (Empagliflozin), an SGLT2 Inhibitor, Receives FDA Approval for the Treatment of Patients with Type 2 Diabetes. Am. Health Drug Benefits 2015, 8, 92–95. [Google Scholar]
- Patorno, E.; Pawar, A.; Wexler, J.; Glynn, J.; Bessette, G.; Paik, J.M.; Najafzadeh, M.; Brodovicz, K.G.; Deruaz-Luyet, A.; Schneeweiss, S. Effectiveness and safety of empagliflozin in routine care patients: Results from the EMPagliflozin compaRative effectIveness and SafEty (EMPRISE) study. Diabetes Obes. Metab. 2021, 24, 442–454. [Google Scholar] [CrossRef]
- Liakos, A.; Karagiannis, T.; Athanasiadou, E.; Sarigianni, M.; Mainou, M.; Papatheodorou, K.; Bekiari, E.; Tsapas, A. Efficacy and safety of empagliflozin for type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 984–993. [Google Scholar] [CrossRef]
- Neeland, I.J.; McGuire, D.K.; Chilton, R.; Crowe, S.; Lund, S.S.; Woerle, H.J.; Broedl, U.C.; Johansen, O.E. Empagliflozin reduces body weight and indices of adipose distribution in patients with type 2 diabetes mellitus. Diab. Vasc. Dis. Res. 2016, 13, 119–126. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Cooper, M.E.; Tikkanen, I.; Pfarr, E.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Lund, S.S. Pooled analysis of Phase III trials indicate contrasting influences of renal function on blood pressure, body weight, and HbA1c reductions with empagliflozin. Kidney Int. 2018, 93, 231–244. [Google Scholar] [CrossRef]
- Fitchett, D.; Inzucchi, S.E.; Cannon, C.P.; McGuire, D.K.; Scirica, B.M.; Johansen, O.E.; Sambevski, S.; Kaspers, S.; Pfarr, E.; George, J.T.; et al. Empagliflozin Reduced Mortality and Hospitalization for Heart Failure Across the Spectrum of Cardiovascular Risk in the EMPA-REG OUTCOME Trial. Circulation 2019, 139, 1384–1395. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Khan, M.S.; Marx, N.; Lam, C.S.P.; Schnaidt, S.; Ofstad, A.P.; Brueckmann, M.; Jamal, W.; et al. Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients With Heart Failure by Baseline Diabetes Status: Results From the EMPEROR-Reduced Trial. Circulation 2021, 143, 337–349. [Google Scholar] [CrossRef]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Patorno, E.; Pawar, A.; Franklin, J.M.; Najafzadeh, M.; Deruaz-Luyet, A.; Brodovicz, K.G.; Sambevski, S.; Bessette, L.G.; Santiago Ortiz, A.J.; Kulldorff, M.; et al. Empagliflozin and the Risk of Heart Failure Hospitalization in Routine Clinical Care. Circulation 2019, 139, 2822–2830. [Google Scholar] [CrossRef]
- Griffin, M.; Rao, V.S.; Ivey-Miranda, J.; Fleming, J.; Mahoney, D.; Maulion, C.; Suda, N.; Siwakoti, K.; Ahmad, T.; Jacoby, D.; et al. Empagliflozin in Heart Failure: Diuretic and Cardiorenal Effects. Circulation 2020, 142, 1028–1039. [Google Scholar] [CrossRef]
- Lee, M.M.Y.; Brooksbank, K.J.M.; Wetherall, K.; Mangion, K.; Roditi, G.; Campbell, R.T.; Berry, C.; Chong, V.; Coyle, L.; Docherty, K.F.; et al. Effect of Empagliflozin on Left Ventricular Volumes in Patients With Type 2 Diabetes, or Prediabetes, and Heart Failure With Reduced Ejection Fraction (SUGAR-DM-HF). Circulation 2021, 143, 516–525. [Google Scholar] [CrossRef]
- Abraham, W.T.; Lindenfeld, J.; Ponikowski, P.; Agostoni, P.; Butler, J.; Desai, A.S.; Filippatos, G.; Gniot, J.; Fu, M.; Gullestad, L.; et al. Effect of empagliflozin on exercise ability and symptoms in heart failure patients with reduced and preserved ejection fraction, with and without type 2 diabetes. Eur. Heart J. 2021, 42, 700–710. [Google Scholar] [CrossRef]
- Wanner, C.; Lachin, J.M.; Inzucchi, S.E.; Fitchett, D.; Mattheus, M.; George, J.; Woerle, H.J.; Broedl, U.C.; von Eynatten, M.; Zinman, B.; et al. Empagliflozin and Clinical Outcomes in Patients With Type 2 Diabetes Mellitus, Established Cardiovascular Disease, and Chronic Kidney Disease. Circulation 2018, 137, 119–129. [Google Scholar] [CrossRef]
- Mazer, C.D.; Hare, G.M.T.; Connelly, P.W.; Gilbert, R.E.; Shehata, N.; Quan, A.; Teoh, H.; Leiter, L.A.; Zinman, B.; Juni, P.; et al. Effect of Empagliflozin on Erythropoietin Levels, Iron Stores, and Red Blood Cell Morphology in Patients With Type 2 Diabetes Mellitus and Coronary Artery Disease. Circulation 2020, 141, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Hoshika, Y.; Kubota, Y.; Mozawa, K.; Tara, S.; Tokita, Y.; Yodogawa, K.; Iwasaki, Y.K.; Yamamoto, T.; Takano, H.; Tsukada, Y.; et al. Effect of Empagliflozin Versus Placebo on Body Fluid Balance in Patients With Acute Myocardial Infarction and Type 2 Diabetes Mellitus: Subgroup Analysis of the EMBODY Trial. J. Card. Fail. 2022, 28, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Zannad, F.; Ferreira, J.P.; Pocock, S.J.; Zeller, C.; Anker, S.D.; Butler, J.; Filippatos, G.; Hauske, S.J.; Brueckmann, M.; Pfarr, E.; et al. Cardiac and Kidney Benefits of Empagliflozin in Heart Failure Across the Spectrum of Kidney Function: Insights From EMPEROR-Reduced. Circulation 2021, 143, 310–321. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B.; et al. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Cherney, D.Z.I.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; von Eynatten, M.; Wanner, C. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: An exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 610–621. [Google Scholar] [CrossRef]
- Wanner, C.; Heerspink, H.J.L.; Zinman, B.; Inzucchi, S.E.; Koitka-Weber, A.; Mattheus, M.; Hantel, S.; Woerle, H.J.; Broedl, U.C.; von Eynatten, M.; et al. Empagliflozin and Kidney Function Decline in Patients with Type 2 Diabetes: A Slope Analysis from the EMPA-REG OUTCOME Trial. J. Am. Soc. Nephrol. 2018, 29, 2755–2769. [Google Scholar] [CrossRef] [PubMed]
- Halden, T.A.S.; Kvitne, K.E.; Midtvedt, K.; Rajakumar, L.; Robertsen, I.; Brox, J.; Bollerslev, J.; Hartmann, A.; Asberg, A.; Jenssen, T. Efficacy and Safety of Empagliflozin in Renal Transplant Recipients With Posttransplant Diabetes Mellitus. Diabetes Care 2019, 42, 1067–1074. [Google Scholar] [CrossRef]
- Sattar, N.; Fitchett, D.; Hantel, S.; George, J.T.; Zinman, B. Empagliflozin is associated with improvements in liver enzymes potentially consistent with reductions in liver fat: Results from randomised trials including the EMPA-REG OUTCOME(R) trial. Diabetologia 2018, 61, 2155–2163. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801–1808. [Google Scholar] [CrossRef]
- Taheri, H.; Malek, M.; Ismail-Beigi, F.; Zamani, F.; Sohrabi, M.; Reza Babaei, M.; Khamseh, M.E. Effect of Empagliflozin on Liver Steatosis and Fibrosis in Patients With Non-Alcoholic Fatty Liver Disease Without Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. Adv. Ther. 2020, 37, 4697–4708. [Google Scholar] [CrossRef]
- Sone, H.; Kaneko, T.; Shiki, K.; Tachibana, Y.; Pfarr, E.; Lee, J.; Tajima, N. Efficacy and safety of empagliflozin as add-on to insulin in Japanese patients with type 2 diabetes: A randomized, double-blind, placebo-controlled trial. Diabetes Obes. Metab. 2020, 22, 417–426. [Google Scholar] [CrossRef]
- Kaku, K.; Chin, R.; Naito, Y.; Iliev, H.; Ikeda, R.; Ochiai, K.; Yasui, A. Safety and effectiveness of empagliflozin in Japanese patients with type 2 diabetes: Interim analysis from a post-marketing surveillance study. Expert Opin. Drug Saf. 2020, 19, 211–221. [Google Scholar] [CrossRef]
- Monteiro, P.; Bergenstal, R.M.; Toural, E.; Inzucchi, S.E.; Zinman, B.; Hantel, S.; Kis, S.G.; Kaspers, S.; George, J.T.; Fitchett, D. Efficacy and safety of empagliflozin in older patients in the EMPA-REG OUTCOME(R) trial. Age Ageing 2019, 48, 859–866. [Google Scholar] [CrossRef]
- Herat, L.Y.; Matthews, V.B.; Magno, A.L.; Kiuchi, M.G.; Carnagarin, R.; Schlaich, M.P. An evaluation of empagliflozin and it’s applicability to hypertension as a therapeutic option. Expert Opin. Pharmacother. 2020, 21, 1157–1166. [Google Scholar] [CrossRef]
- Devi, R.; Mali, G.; Chakraborty, I.; Unnikrishnan, M.K.; Abdulsalim, S. Efficacy and safety of empagliflozin in type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. Postgrad. Med. 2017, 129, 382–392. [Google Scholar] [CrossRef]
- SFDA. Saudi vigilance, Saudi Food & Drug Authority (SFDA): The Risk of Rare but Serious Infection in the Genital Area with Sodium Glucose Cotransporter-2 (SGLT2) Inhibitors. 2018. Available online: https://www.sfda.gov.sa/sites/default/files/2021-02/Jardiance%C2%AE%20SAFTEY%20COMM.pdf (accessed on 1 June 2018).
- Kadowaki, T.; Haneda, M.; Inagaki, N.; Terauchi, Y.; Taniguchi, A.; Koiwai, K.; Rattunde, H.; Woerle, H.J.; Broedl, U.C. Empagliflozin monotherapy in Japanese patients with type 2 diabetes mellitus: A randomized, 12-week, double-blind, placebo-controlled, phase II trial. Adv. Ther. 2014, 31, 621–638. [Google Scholar] [CrossRef]
- Ferrannini, E.; Berk, A.; Hantel, S.; Pinnetti, S.; Hach, T.; Woerle, H.J.; Broedl, U.C. Long-term safety and efficacy of empagliflozin, sitagliptin, and metformin: An active-controlled, parallel-group, randomized, 78-week open-label extension study in patients with type 2 diabetes. Diabetes Care 2013, 36, 4015–4021. [Google Scholar] [CrossRef]
- Rosenstock, J.; Aggarwal, N.; Polidori, D.; Zhao, Y.; Arbit, D.; Usiskin, K.; Capuano, G.; Canovatchel, W.; Canagliflozin, D.I.A.S.G. Dose-ranging effects of canagliflozin, a sodium-glucose cotransporter 2 inhibitor, as add-on to metformin in subjects with type 2 diabetes. Diabetes Care 2012, 35, 1232–1238. [Google Scholar] [CrossRef]
- Rosenstock, J.; Seman, L.J.; Jelaska, A.; Hantel, S.; Pinnetti, S.; Hach, T.; Woerle, H.J. Efficacy and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, as add-on to metformin in type 2 diabetes with mild hyperglycaemia. Diabetes Obes. Metab. 2013, 15, 1154–1160. [Google Scholar] [CrossRef]
- Kishimoto, M.; Yamaoki, K.; Adachi, M. Combination Therapy with Empagliflozin and Insulin Results in Successful Glycemic Control: A Case Report of Uncontrolled Diabetes Caused by Autoimmune Pancreatitis and Subsequent Steroid Treatment. Case Rep. Endocrinol. 2019, 2019, 9415347. [Google Scholar] [CrossRef]
- Al-Goblan, A.S.; Al-Alfi, M.A.; Khan, M.Z. Mechanism linking diabetes mellitus and obesity. Diabetes Metab. Syndr. Obes. 2014, 7, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, J.; Jelaska, A.; Frappin, G.; Salsali, A.; Kim, G.; Woerle, H.J.; Broedl, U.C.; Investigators, E.-R.M.T. Improved glucose control with weight loss, lower insulin doses, and no increased hypoglycemia with empagliflozin added to titrated multiple daily injections of insulin in obese inadequately controlled type 2 diabetes. Diabetes Care 2014, 37, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Bolinder, J.; Ljunggren, O.; Kullberg, J.; Johansson, L.; Wilding, J.; Langkilde, A.M.; Sugg, J.; Parikh, S. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J. Clin. Endocrinol. Metab. 2012, 97, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Liu, H.; Dong, P. Empagliflozin reduces blood pressure and uric acid in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. J. Hum. Hypertens. 2019, 33, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Boorsma, E.M.; Beusekamp, J.C.; Ter Maaten, J.M.; Figarska, S.M.; Danser, A.H.J.; van Veldhuisen, D.J.; van der Meer, P.; Heerspink, H.J.L.; Damman, K.; Voors, A.A. Effects of empagliflozin on renal sodium and glucose handling in patients with acute heart failure. Eur. J. Heart Fail. 2021, 23, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Schork, A.; Saynisch, J.; Vosseler, A.; Jaghutriz, B.A.; Heyne, N.; Peter, A.; Haring, H.U.; Stefan, N.; Fritsche, A.; Artunc, F. Effect of SGLT2 inhibitors on body composition, fluid status and renin-angiotensin-aldosterone system in type 2 diabetes: A prospective study using bioimpedance spectroscopy. Cardiovasc. Diabetol. 2019, 18, 46. [Google Scholar] [CrossRef] [PubMed]
- Ferdinand, K.C.; Izzo, J.L.; Lee, J.; Meng, L.; George, J.; Salsali, A.; Seman, L. Antihyperglycemic and Blood Pressure Effects of Empagliflozin in Black Patients With Type 2 Diabetes Mellitus and Hypertension. Circulation 2019, 139, 2098–2109. [Google Scholar] [CrossRef]
- Palmiero, G.; Cesaro, A.; Vetrano, E.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Moscarella, E.; Gragnano, F.; Salvatore, T.; Rinaldi, L.; et al. Impact of SGLT2 Inhibitors on Heart Failure: From Pathophysiology to Clinical Effects. Int. J. Mol. Sci. 2021, 22, 5863. [Google Scholar] [CrossRef]
- Salvatore, T.; Caturano, A.; Galiero, R.; Di Martino, A.; Albanese, G.; Vetrano, E.; Sardu, C.; Marfella, R.; Rinaldi, L.; Sasso, F.C. Cardiovascular Benefits from Gliflozins: Effects on Endothelial Function. Biomedicines 2021, 9, 1356. [Google Scholar] [CrossRef]
- Perrone-Filardi, P.; Avogaro, A.; Bonora, E.; Colivicchi, F.; Fioretto, P.; Maggioni, A.P.; Sesti, G.; Ferrannini, E. Mechanisms linking empagliflozin to cardiovascular and renal protection. Int. J. Cardiol. 2017, 241, 450–456. [Google Scholar] [CrossRef]
- Pabel, S.; Wagner, S.; Bollenberg, H.; Bengel, P.; Kovacs, A.; Schach, C.; Tirilomis, P.; Mustroph, J.; Renner, A.; Gummert, J.; et al. Empagliflozin directly improves diastolic function in human heart failure. Eur. J. Heart Fail. 2018, 20, 1690–1700. [Google Scholar] [CrossRef]
- Cherney, D.; Lund, S.S.; Perkins, B.A.; Groop, P.H.; Cooper, M.E.; Kaspers, S.; Pfarr, E.; Woerle, H.J.; von Eynatten, M. The effect of sodium glucose cotransporter 2 inhibition with empagliflozin on microalbuminuria and macroalbuminuria in patients with type 2 diabetes. Diabetologia 2016, 59, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Perry, R.J.; Samuel, V.T.; Petersen, K.F.; Shulman, G.I. The role of hepatic lipids in hepatic insulin resistance and type 2 diabetes. Nature 2014, 510, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kern, M.; Kloting, N.; Mark, M.; Mayoux, E.; Klein, T.; Bluher, M. The SGLT2 inhibitor empagliflozin improves insulin sensitivity in db/db mice both as monotherapy and in combination with linagliptin. Metabolism 2016, 65, 114–123. [Google Scholar] [CrossRef]
- Hattori, S. Empagliflozin decreases remnant-like particle cholesterol in type 2 diabetes patients with insulin resistance. J Diabetes Investig. 2018, 9, 870–874. [Google Scholar] [CrossRef]
- Jojima, T.; Sakurai, S.; Wakamatsu, S.; Iijima, T.; Saito, M.; Tomaru, T.; Kogai, T.; Usui, I.; Aso, Y. Empagliflozin increases plasma levels of campesterol, a marker of cholesterol absorption, in patients with type 2 diabetes: Association with a slight increase in high-density lipoprotein cholesterol. Int. J. Cardiol. 2021, 331, 243–248. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographics | |
|---|---|
| Sample volume, n | 256 |
| Age (years), mean (SD) | 58.9 (10.75) |
| Sex Males, n | 113 |
| Females, n | 143 |
| Male age, mean (SD) | 58.2 (11.88) |
| Female age, mean (SD) | 59.4 (9.76) |
| Duration since Diagnosis of T2DM, (years) | |
| Mean (SD) | 16.7 (8.47) |
| <1, n (%) | 0 |
| 1 to 5 | 22 (9%) |
| > 5 | 234 (91%) |
| DM Treatment before Empagliflozin | |
| Insulin + OHA (metformin) | 156 (64%) |
| OHA (metformin) | 93 (36%) |
| Baseline Group | Empagliflozin Group | Change Amount | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| Efficacy: | |||
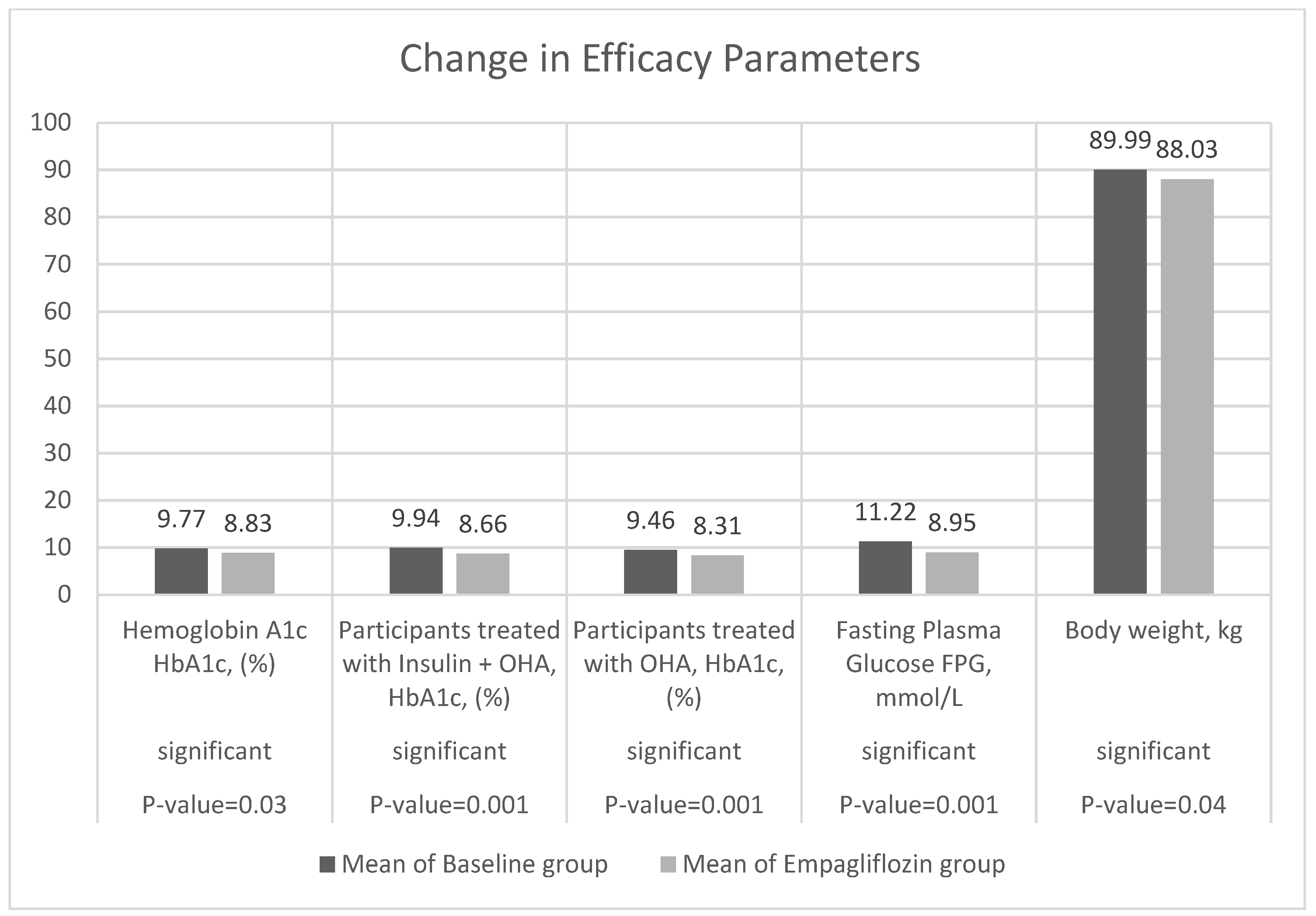
| Haemoglobin A1c HbA1c, (%) | 9.77 ± 1.76 | 8.85 ± 4.83 | −0.92 |
| Participants treated with Insulin + OHA, HbA1c, (%) | 9.94 ± 1.84 | 8.66 ± 1.47 | −1.27 |
| Participants treated with | 9.46 ± 1.56 | 8.31 ± 1.26 | −1.15 |
| OHA, HbA1c, (%) | |||
| Fasting Plasma Glucose FPG, mmol/L | 11.27 ± 4.79 | 8.95 ± 3.37 | −2.32 |
| Body weight, kg | 89.99 ± 18.09 | 88.03 ± 18.47 | −1.96 |
| Safety: | |||
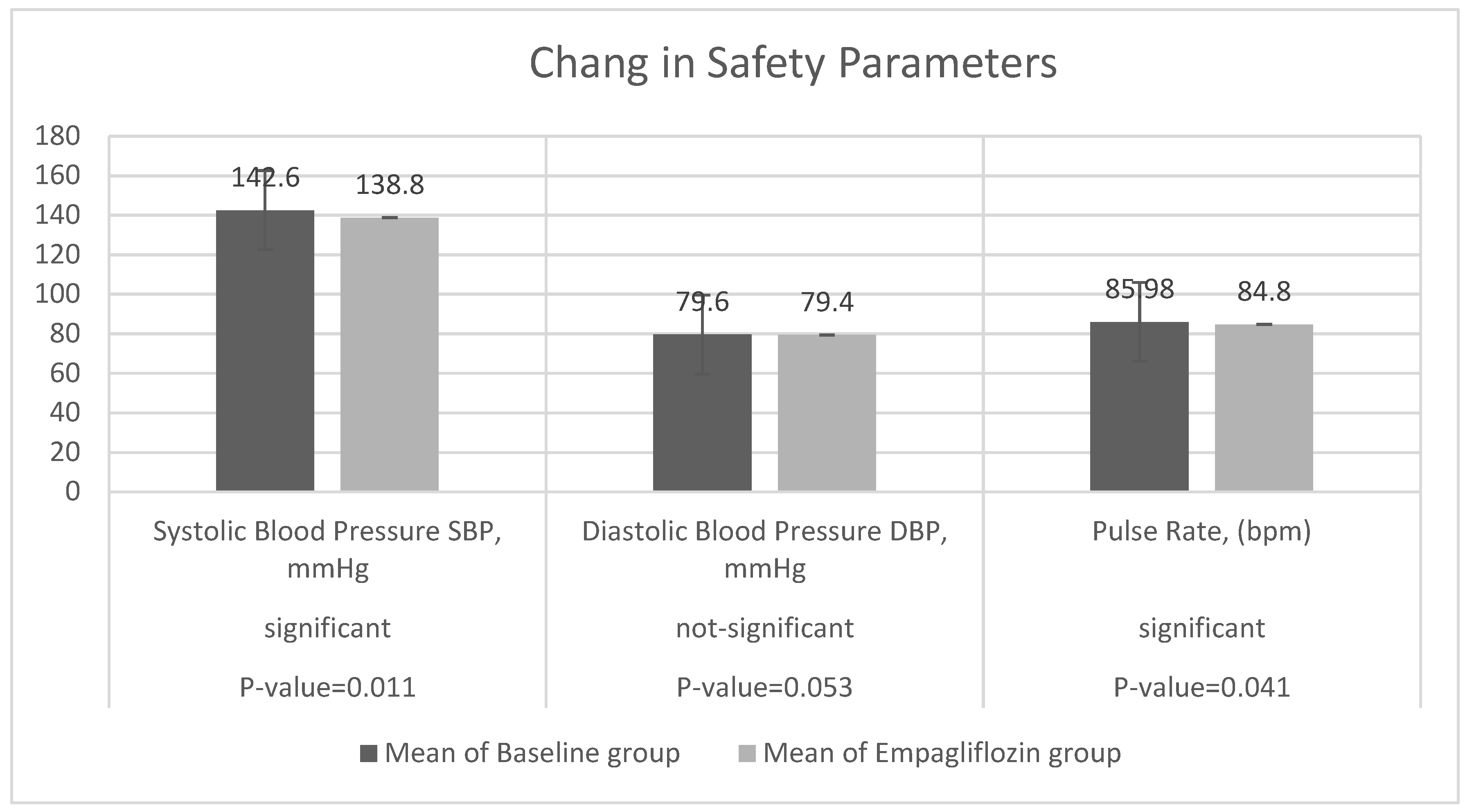
| Systolic Blood Pressure SBP, mmHg | 142.6 ± 19.45 | 138.8 ± 20.23 | −3.8 |
| Diastolic Blood Pressure DBP, mmHg | 79.6 ± 20.32 | 79.4 ± 21.14 | −0.2 |
| Pulse Rate, (bpm) | 85.98 ± 11.33 | 84.80 ± 13.52 | −1.18 |
| Kidney Function Status | |||
| Urine Albumin/Creatinine Ratio UACR (mg/g) | 20.39 ± 43.72 | 17.12 ± 40.05 | −3.27 |
| eGFR, mL/min/1.73 m2 | 51.12 ± 120.45 | 72.51 ± 22.80 | 21.39 |
| Liver Function Status | |||
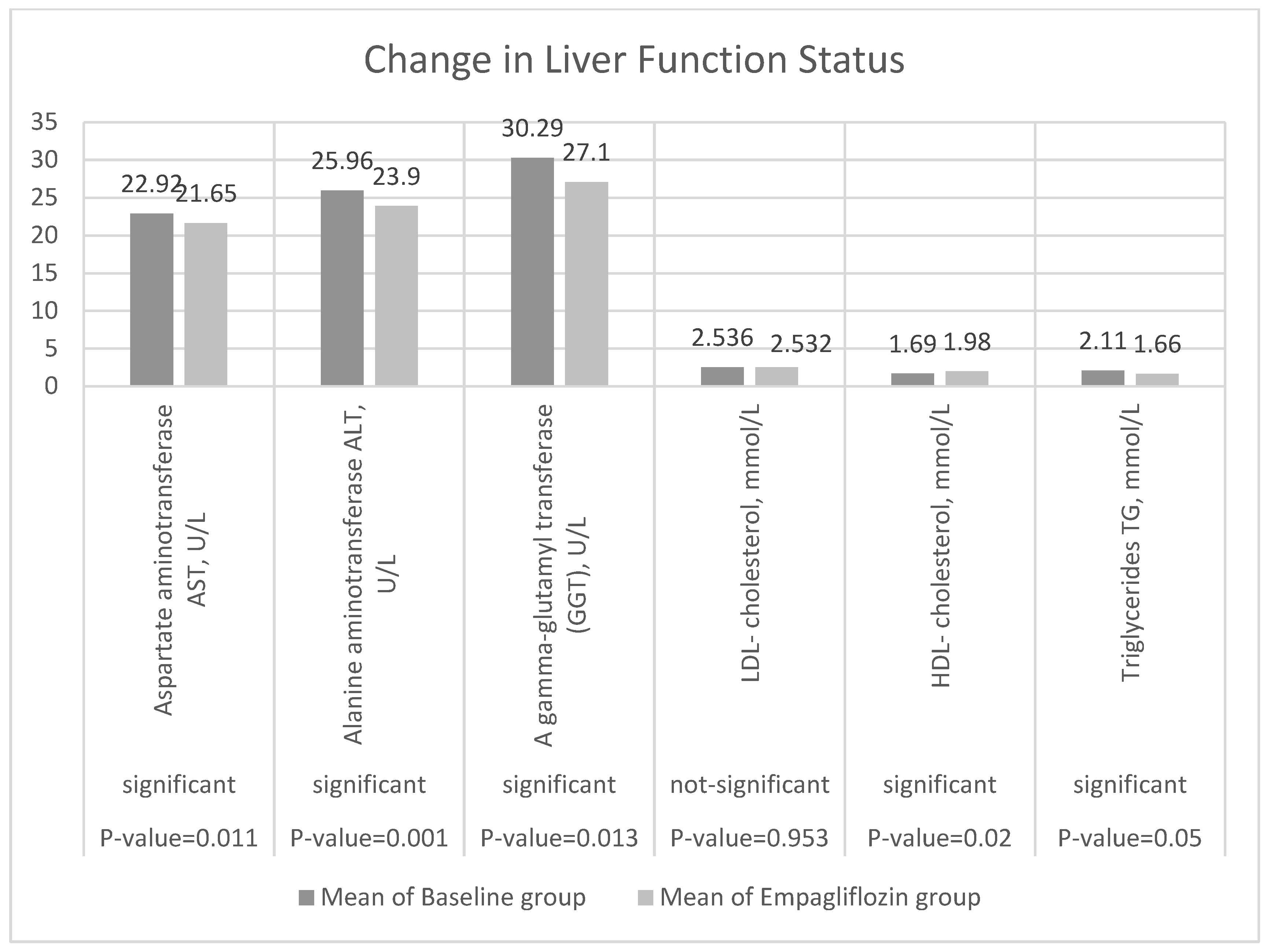
| Aspartate aminotransferase AST, U/L | 22.92 ± 8.10 | 21.65 ± 6.38 | −1.26 |
| Alanine aminotransferase ALT, U/L | 25.96 ± 8.09 | 23.91 ± 11.71 | −0.70 |
| A gamma-glutamyl transferase (GGT), U/L | 30.29 ± 25.15 | 27.12 ± 18.32 | −4.31 |
| LDL- cholesterol, mmol/L | 2.543 ± 0.93 | 2.544 ± 1.50 | 0.0009 |
| HDL- cholesterol, mmol/L | 1.69 ± 3.59 | 1.98 ± 0.22 | 0.29 |
| Triglycerides TG, mmol/L | 2.11 ± 5.90 | 1.66 ± 0.20 | −0.45 |
| Baseline Start Treatment Empagliflozin | Change from Baseline at Week 12 | Rate of Change | |
|---|---|---|---|
| Efficacy variables | |||
| Mean change in HbA1c | −0.93 (−0.32, −1.54) | −0.106 | |
| from baseline, % (95% CI) | |||
| Mean ± SD | −0.93 ± 4.93 | ||
| <7.0% | 5 (0.02) | 21 (0.08) | 0.76 |
| ≥7% to <8% | 4 (0.016) | 76 (0.30) | 0.95 |
| ≥8% to <9% | 80 (0.31) | 82 (0.32) | 0.02 |
| ≥9% | 167 (0.65) | 77 (0.30) | −0.54 |
| Decrease in HbA1c (%) in participants: ≥ 0.5%, n, (%) | 181(0.71) | ||
| Treated with insulin + OHA, HbA1c, (%) | −1.28(−1.03, −1.53) | −0.147 | |
| Treated with OHA, HbA1c (%) | −1.11(−0.799, −1.42) | −0.139 | |
| Decrease in insulin units in participants treated with insulin + OHA | 9.94 ± 1.84 | 8.67 ± 1.47 | −1.27 |
| Mean change in FPG | −2.28 (−2.81, −1.75) | −0.25 | |
| from baseline (95% CI) | |||
| Mean ± SD | −2.27 ± 4.22 | ||
| <7.8, n, (%) | 63 (0.25) | 115 (0.45) | 0.83 |
| 7.8 to <11.0 | 80 (0.32) | 86 (0.34) | 0.08 |
| ≥11 | 113 (0.44) | 55 (0.21) | −0.51 |
| Mean change in body weight | −0.874 (−4.36, −6.10) | −0.02 | |
| from baseline (95% CI) | |||
| Mean ± SD | −1.96 ± 11.98 | ||
| Safety variables | |||
| Mean change in SBP | −3.85 (−6.81, −0.88) | −0.03 | |
| from baseline, % (95% CI) | |||
| Mean ± SD | −3.82 ± 23.4 | ||
| Mean change in DBP | −0.06 (−0.81, −0.88) | −0.001 | |
| from baseline, % (95% CI) | |||
| Mean ± SD | −0.05 ± 0.28 | ||
| Mean change in pulse rate | −1.18 (−0.79, −3.15) | −0.01 | |
| from baseline (95% CI) | |||
| Mean ± SD | −1.18 ± 15.46 | ||
| Kidney Function Status | |||
| Mean change in Urine Albumin/ | −0.067 | ||
| Creatinine Ratio UACR (mg/g) | −1.76 (−1.07, −34.25) | ||
| Mean ± SD | −1.76 ± 103.5 | ||
| <30, n, (%) | 126 (0.50) | 177(0.70) | 0.4 |
| 30 to <300 n, (%) | 51(0.21) | 67 (0.27) | 0.31 |
| ≥300, n, (%) | 75 (0.29) | 8 (0.03) | −0.89 |
| Mean change in body eGFR | 3.54 (2.78, 9.87) | −0.418 | |
| from baseline, kg (95% CI) | |||
| Mean ± SD | 3.54 ± 45.98 | ||
| ≥90, n, (%) | 49 (0.19) | 55 (0.21) | 0.02 |
| 60 to < 90 | 120 (0.47) | 116 (0.45) | −0.018 |
| 30 to < 60 | 87 (0.34) | 84 (0.33) | −0.016 |
| Liver Function Status | |||
| Mean change in AST | −1.26 (−0.3011, −2.227) | −0.058 | |
| from baseline (95% CI) | |||
| Mean ± SD | −1.263 ± 7.72 | ||
| Mean change in ALT | −2.36 (−1.031, −3.69) | −0.029 | |
| from baseline (95% CI) | |||
| Mean ± SD | −2.36 ± 10.75 | ||
| Mean change in GGT | −4.31 (−2.33, −6.28) | −0.159 | |
| from baseline (95% CI) | |||
| Mean ± SD | −4.31 ± 15.66 | ||
| Mean change in LDL | 0.005 (0.192, 0.18) | 0.0004 | |
| from baseline (95% CI) | |||
| Mean ± SD | 0.005 ± 1.46 | ||
| Mean change in HDL | 0.29 (0.74, 0.15) | 0.171 | |
| from baseline, kg (95% CI) | |||
| Mean ± SD | 0.293 ± 3.61 | ||
| Mean change in TG | −0.43 (−0.31, −1.17) | −0.271 | |
| from baseline (95% CI) | |||
| Mean ± SD | −0.45 ± 5.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Althobaiti, F.M.; Alsanosi, S.M.; Falemban, A.H.; Alzahrani, A.R.; Fataha, S.A.; Salih, S.O.; Alrumaih, A.M.; Alotaibi, K.N.; Althobaiti, H.M.; Al-Ghamdi, S.S.; et al. Efficacy and Safety of Empagliflozin in Type 2 Diabetes Mellitus Saudi Patients as Add-On to Antidiabetic Therapy: A Prospective, Open-Label, Observational Study. J. Clin. Med. 2022, 11, 4769. https://doi.org/10.3390/jcm11164769
Althobaiti FM, Alsanosi SM, Falemban AH, Alzahrani AR, Fataha SA, Salih SO, Alrumaih AM, Alotaibi KN, Althobaiti HM, Al-Ghamdi SS, et al. Efficacy and Safety of Empagliflozin in Type 2 Diabetes Mellitus Saudi Patients as Add-On to Antidiabetic Therapy: A Prospective, Open-Label, Observational Study. Journal of Clinical Medicine. 2022; 11(16):4769. https://doi.org/10.3390/jcm11164769
Chicago/Turabian StyleAlthobaiti, Fahad M., Safaa M. Alsanosi, Alaa H. Falemban, Abdullah R. Alzahrani, Salma A. Fataha, Sara O. Salih, Ali M. Alrumaih, Khalid N. Alotaibi, Hazim M. Althobaiti, Saeed S. Al-Ghamdi, and et al. 2022. "Efficacy and Safety of Empagliflozin in Type 2 Diabetes Mellitus Saudi Patients as Add-On to Antidiabetic Therapy: A Prospective, Open-Label, Observational Study" Journal of Clinical Medicine 11, no. 16: 4769. https://doi.org/10.3390/jcm11164769