

Effects of Different Pressure Levels in Topical Negative Pressure Application—Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Blood Flow Measurement Devices
2.2. Topical Negative Pressure Application
3. Results
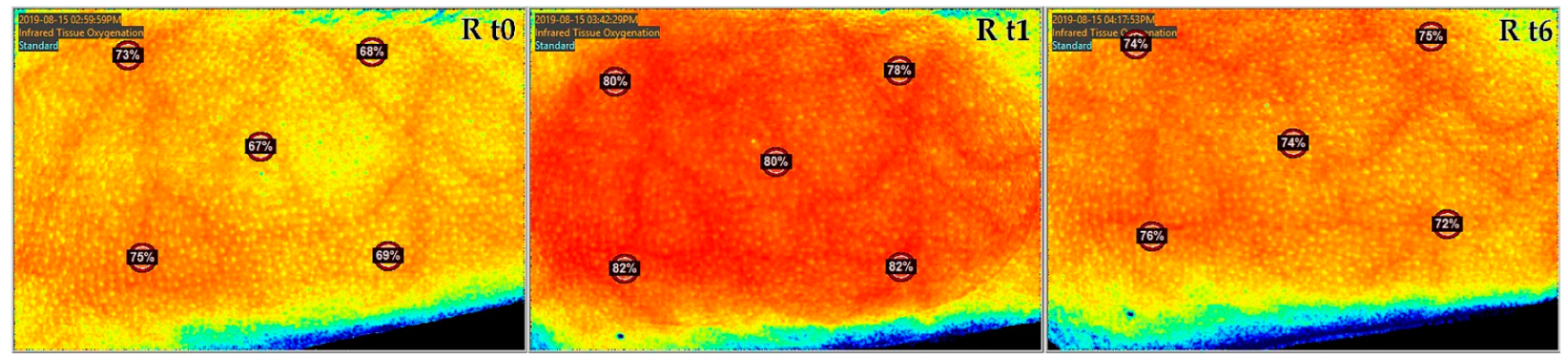
3.1. Tissue Oxygen Saturation by NIS
3.2. Skin Temperature
3.3. Vein Illuminator
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horch, R.E.; Gerngross, H.; Lang, W.; Mauckner, P.; Nord, D.; Peter, R.U.; Vogt, P.M.; Wetzel-Roth, W.; Willy, C. Indications and safety aspects of vacuum-assisted wound closure. MMW Fortschr. Med. 2005, 147 (Suppl. S1), 1–5. [Google Scholar] [PubMed]
- Hunter, J.E.; Teot, L.; Horch, R.E.; Banwell, P.E. Evidence-based medicine: Vacuum-assisted closure in wound care management. Int. Wound J. 2007, 4, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Labanaris, A.P.; Polykandriotis, E.; Horch, R.E. The effect of vacuum-assisted closure on lymph vessels in chronic wounds. J. Plast. Reconstr. Aesthet. Surg. 2009, 62, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Ludolph, I.; Müller-Seubert, W.; Zetzmann, K.; Hauck, T.; Arkudas, A.; Geierlehner, A. Topical negative-pressure wound therapy: Emerging devices and techniques. Expert. Rev. Med. Devices 2020, 17, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Horch, R.E.; Braumann, C.; Dissemond, J.; Lehner, B.; Hirche, C.; Woeste, G.; Wetzel-Roth, W.; Willy, C. Use of Negative Pressure Wound Therapy with Instillation and Dwell Time for Wound Treatment—Results of an Expert Consensus Conference. Zentralblatt Chir. 2018, 143, 609–616. [Google Scholar] [CrossRef]
- Renno, I.; Boos, A.M.; Horch, R.E.; Ludolph, I. Changes of perfusion patterns of surgical wounds under application of closed incision negative pressure wound therapy in postbariatric patients1. Clin. Hemorheol. Microcirc. 2019, 72, 139–150. [Google Scholar] [CrossRef]
- Horch, R.E. Incisional negative pressure wound therapy for high-risk wounds. J. Wound Care 2015, 24 (Suppl. S4), 21–28. [Google Scholar] [CrossRef]
- Muenchow, S.; Horch, R.E.; Dragu, A. Effects of topical negative pressure therapy on perfusion and microcirculation of human skin. Clin. Hemorheol. Microcirc. 2019, 72, 365–374. [Google Scholar] [CrossRef]
- Malmsjö, M.; Ingemansson, R.; Martin, R.; Huddleston, E. Wound edge microvascular blood flow: Effects of negative pressure wound therapy using gauze or polyurethane foam. Ann. Plast Surg. 2009, 63, 676–681. [Google Scholar] [CrossRef]
- Petzina, R.; Gustafsson, L.; Mokhtari, A.; Ingemansson, R.; Malmsjö, M. Effect of vacuum-assisted closure on blood flow in the peristernal thoracic wall after internal mammary artery harvesting. Eur. J. Cardiothorac. Surg. 2006, 30, 85–89. [Google Scholar] [CrossRef] [Green Version]
- Wackenfors, A.; Sjögren, J.; Gustafsson, R.; Algotsson, L.; Ingemansson, R.; Malmsjö, M. Effects of vacuum-assisted closure therapy on inguinal wound edge microvascular blood flow. Wound Repair. Regen. 2004, 12, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Lou, D.; Pang, Q.; Pei, X.; Dong, S.; Li, S.; Tan, W.-Q.; Ma, L. Flexible wound healing system for pro-regeneration, temperature monitoring and infection early warning. Biosens. Bioelectron. 2020, 162, 112275. [Google Scholar] [CrossRef] [PubMed]
- Power, G.; Moore, Z.; O’Connor, T. Measurement of pH, exudate composition and temperature in wound healing: A systematic review. J. Wound Care 2017, 26, 381–397. [Google Scholar] [CrossRef] [PubMed]
- Castilla, D.M.; Liu, Z.J.; Velazquez, O.C. Oxygen: Implications for Wound Healing. Adv. Wound Care 2012, 1, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.L. Influence of oxygen on wound healing. Int. Wound J. 2015, 12, 620–624. [Google Scholar] [CrossRef]
- Muller-Seubert, W.; Roth, S.; Hauck, T.; Arkudas, A.; Horch, R.E.; Ludolph, I. Novel imaging methods reveal positive impact of topical negative pressure application on tissue perfusion in an in vivo skin model. Int. Wound J. 2021, 18, 932–939. [Google Scholar] [CrossRef]
- Müller-Seubert, W.; Ostermaier, P.; Horch, R.E.; Distel, L.; Frey, B.; Cai, A.; Arkudas, A. Intra- and Early Postoperative Evaluation of Malperfused Areas in an Irradiated Random Pattern Skin Flap Model Using Indocyanine Green Angiography and Near-Infrared Reflectance-Based Imaging and Infrared Thermography. J. Pers. Med. 2022, 12, 237. [Google Scholar] [CrossRef]
- Geierlehner, A.; Horch, R.E.; Muller-Seubert, W.; Arkudas, A.; Ludolph, I. Limb salvage procedure in immunocompromised patients with therapy-resistant leg ulcers—The value of ultra-radical debridement and instillation negative-pressure wound therapy. Int. Wound J. 2020, 17, 1496–1507. [Google Scholar] [CrossRef]
- Morykwas, M.J.; Argenta, L.C.; Shelton-Brown, E.I.; McGuirt, W. Vacuum-assisted closure: A new method for wound control and treatment: Animal studies and basic foundation. Ann. Plast. Surg. 1997, 38, 553–562. [Google Scholar] [CrossRef]
- Timmers, M.S.; Le Cessie, S.; Banwell, P.; Jukema, G.N. The effects of varying degrees of pressure delivered by negative-pressure wound therapy on skin perfusion. Ann. Plast. Surg. 2005, 55, 665–671. [Google Scholar] [CrossRef]
- Sogorski, A.; Lehnhardt, M.; Goertz, O.; Harati, K.; Kapalschinski, N.; Hirsch, T.; Daigeler, A.; Kolbenschlag, J. Improvement of local microcirculation through intermittent negative pressure wound therapy (NPWT). J. Tissue Viability 2018, 27, 267–273. [Google Scholar] [CrossRef]
- Ichioka, S.; Watanabe, H.; Sekiya, N.; Shibata, M.; Nakatsuka, T. A technique to visualize wound bed microcirculation and the acute effect of negative pressure. Wound Repair. Regen. 2008, 16, 460–465. [Google Scholar] [CrossRef]
- Kairinos, N.; Solomons, M.; Hudson, D.A. Negative-pressure wound therapy I: The paradox of negative-pressure wound therapy. Plast. Reconstr. Surg. 2009, 123, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Kairinos, N.; Voogd, A.M.; Botha, P.H.; Kotze, T.; Kahn, D.; Hudson, D.A.; Solomons, M. Negative-pressure wound therapy II: Negative-pressure wound therapy and increased perfusion. Just an illusion? Plast. Reconstr. Surg. 2009, 123, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Morykwas, M.J.; Faler, B.J.; Pearce, D.J.; Argenta, L.C. Effects of varying levels of subatmospheric pressure on the rate of granulation tissue formation in experimental wounds in swine. Ann. Plast. Surg. 2001, 47, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Malmsjö, M.; Ingemansson, R.; Martin, R.; Huddleston, E. Negative-pressure wound therapy using gauze or open-cell polyurethane foam: Similar early effects on pressure transduction and tissue contraction in an experimental porcine wound model. Wound Repair. Regen. 2009, 17, 200–205. [Google Scholar] [CrossRef]
- Andres, T.; von Lübken, F.; Friemert, B.; Achatz, G. Vacuum-Assisted Closure in the Management of Degloving Soft Tissue Injury: A Case Report. J. Foot Ankle Surg. 2016, 55, 852–856. [Google Scholar] [CrossRef]
- Linkov, G.; Cracchiolo, J.; Fielding, A.F.; Liu, J.C. Facial nerve function preservation with vacuum-assisted closure. J. Craniofac. Surg. 2014, 25, 1560–1561. [Google Scholar] [CrossRef]
- Lindstedt, S.; Malmsjö, M.; Hansson, J.; Hlebowicz, J.; Ingemansson, R. Microvascular blood flow changes in the small intestinal wall during conventional negative pressure wound therapy and negative pressure wound therapy using a protective disc over the intestines in laparostomy. Ann. Surg. 2012, 255, 171–175. [Google Scholar] [CrossRef]
- Stiegler, P.; Matzi, V.; Pierer, E.; Hauser, O.; Schaffellner, S.; Renner, H.; Greilberger, J.; Aigner, R.; Maier, A.; Lackner, C.; et al. Creation of a prevascularized site for cell transplantation in rats. Xenotransplantation 2010, 17, 379–390. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Participant No (n) | (n) Male | (n) Female | TNPA Pressure |
|---|---|---|---|---|
| Control | 24 | 16 | 8 | −125 mmHg |
| Group 1 | 9 | 6 | 3 | 0 mmHg |
| Group 2 | 7 | 5 | 2 | −25 mmHg |
| Group 3 | 8 | 5 | 3 | −175 mmHg |
| Group | n | t0 Average | t1 Average | t2 Average | t6 Average | Δ t0−t1 | Δ t0−t6 | Δ t1−t6 | t0–t1 Relative Increase | t0–t1 Relative Increase |
|---|---|---|---|---|---|---|---|---|---|---|
| control | 24 | 63.75% | 71.82% | 72.24% | 66.50% | 8.07% | 2.75% | −5.32% | 12.65% | 65.92% |
| 1 | 9 | 65.22% | 67.77% | 68.26% | 68.77% | 2.55% | 3.55% | 1.00% | 2.55% | 39.21% |
| 2 | 7 | 64.40% | 68.40% | 69.22% | 65.62% | 4.00% | 1.12% | −2.78% | 6.21% | 69.50% |
| 3 | 8 | 61.45% | 69.90% | 70.30% | 65.82% | 8.45% | 4.37% | −4.08% | 13.75% | 48.28% |
| Group | n | t0 Average | t1 Average | t6 Average | Δ t0−t1 | Δ t0−t6 | Δ t1−t6 |
|---|---|---|---|---|---|---|---|
| control | 24 | 30.60 | 32.27 | 31.23 | 1.67 | 0.63 | −1.04 |
| 1 | 9 | 30.04 | 32.75 | 31.22 | 2.71 | 1.18 | −1.53 |
| 2 | 7 | 31.82 | 33.40 | 31.84 | 1.58 | 0.02 | −1.56 |
| 3 | 8 | 31.55 | 33.23 | 32.75 | 1.68 | 1.20 | −0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslan-Horch, E.C.; Horch, R.E.; Arkudas, A.; Müller-Seubert, W.; Ludolph, I. Effects of Different Pressure Levels in Topical Negative Pressure Application—Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques. J. Clin. Med. 2022, 11, 5133. https://doi.org/10.3390/jcm11175133
Aslan-Horch EC, Horch RE, Arkudas A, Müller-Seubert W, Ludolph I. Effects of Different Pressure Levels in Topical Negative Pressure Application—Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques. Journal of Clinical Medicine. 2022; 11(17):5133. https://doi.org/10.3390/jcm11175133
Chicago/Turabian StyleAslan-Horch, Emine Ceylan, Raymund E. Horch, Andreas Arkudas, Wibke Müller-Seubert, and Ingo Ludolph. 2022. "Effects of Different Pressure Levels in Topical Negative Pressure Application—Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques" Journal of Clinical Medicine 11, no. 17: 5133. https://doi.org/10.3390/jcm11175133
APA StyleAslan-Horch, E. C., Horch, R. E., Arkudas, A., Müller-Seubert, W., & Ludolph, I. (2022). Effects of Different Pressure Levels in Topical Negative Pressure Application—Analysis of Perfusion Parameters in a Clinical Skin Model Using Multimodal Imaging Techniques. Journal of Clinical Medicine, 11(17), 5133. https://doi.org/10.3390/jcm11175133