


A Novel Method to Combine Maxilla-Based Coordinate System and Mandibular Voxel-Based Superimposition with Cone-Bean Computed Tomography

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Object and Data Collection
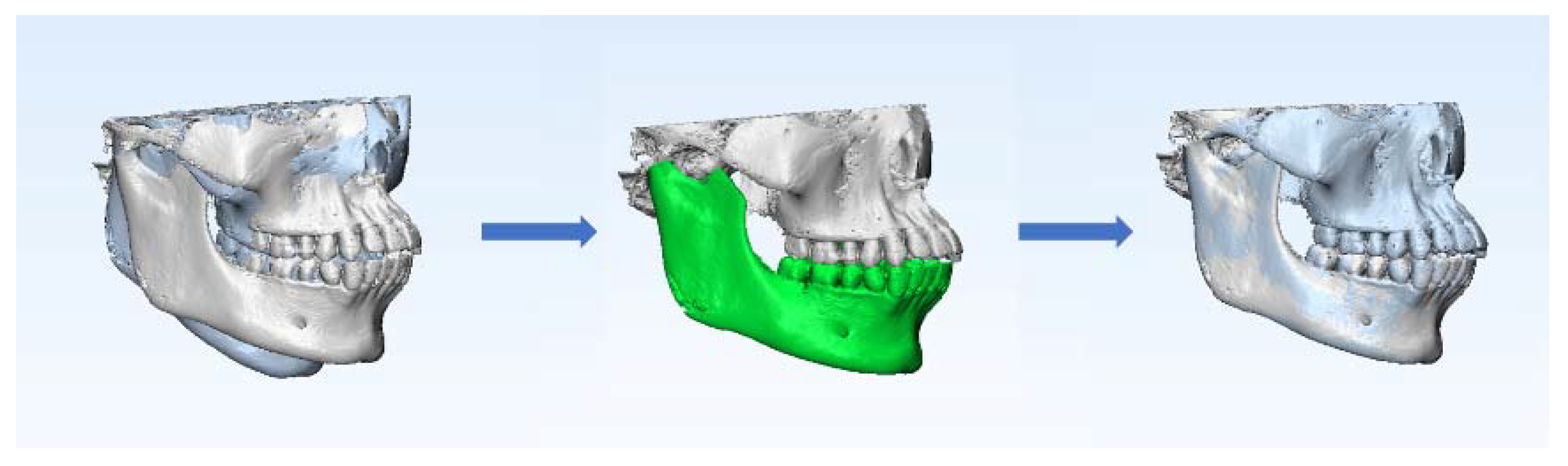
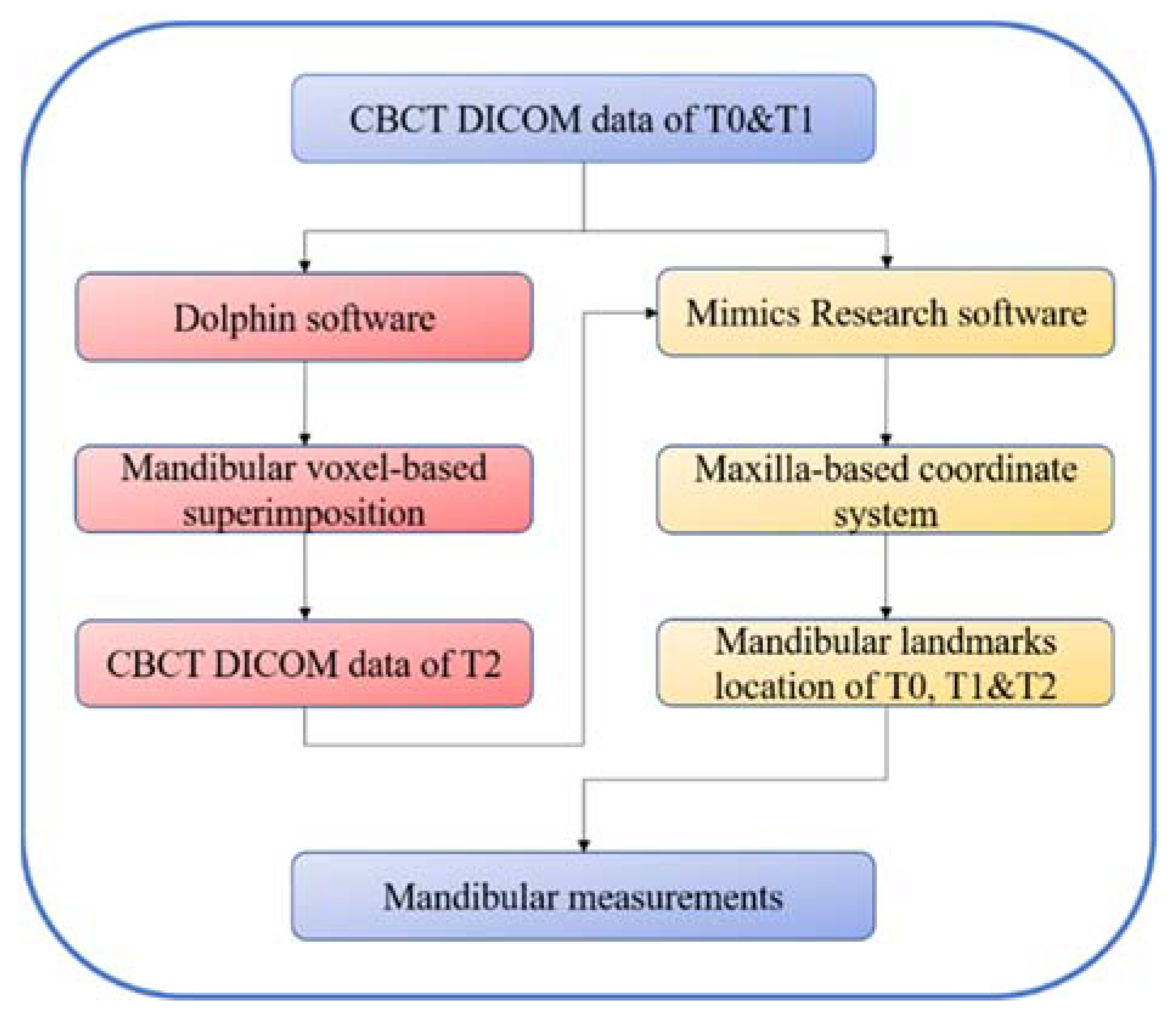
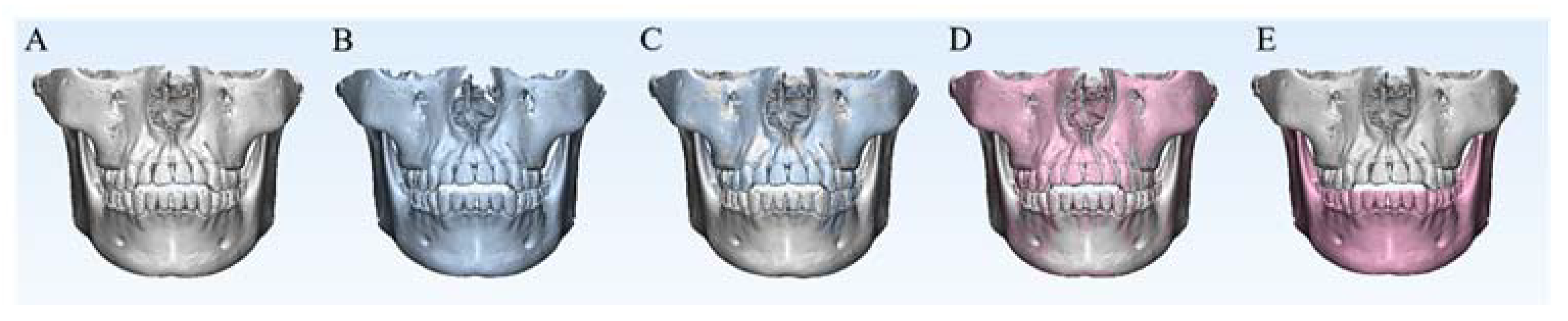
2.2. Mandibular Voxel-Based Superimposition
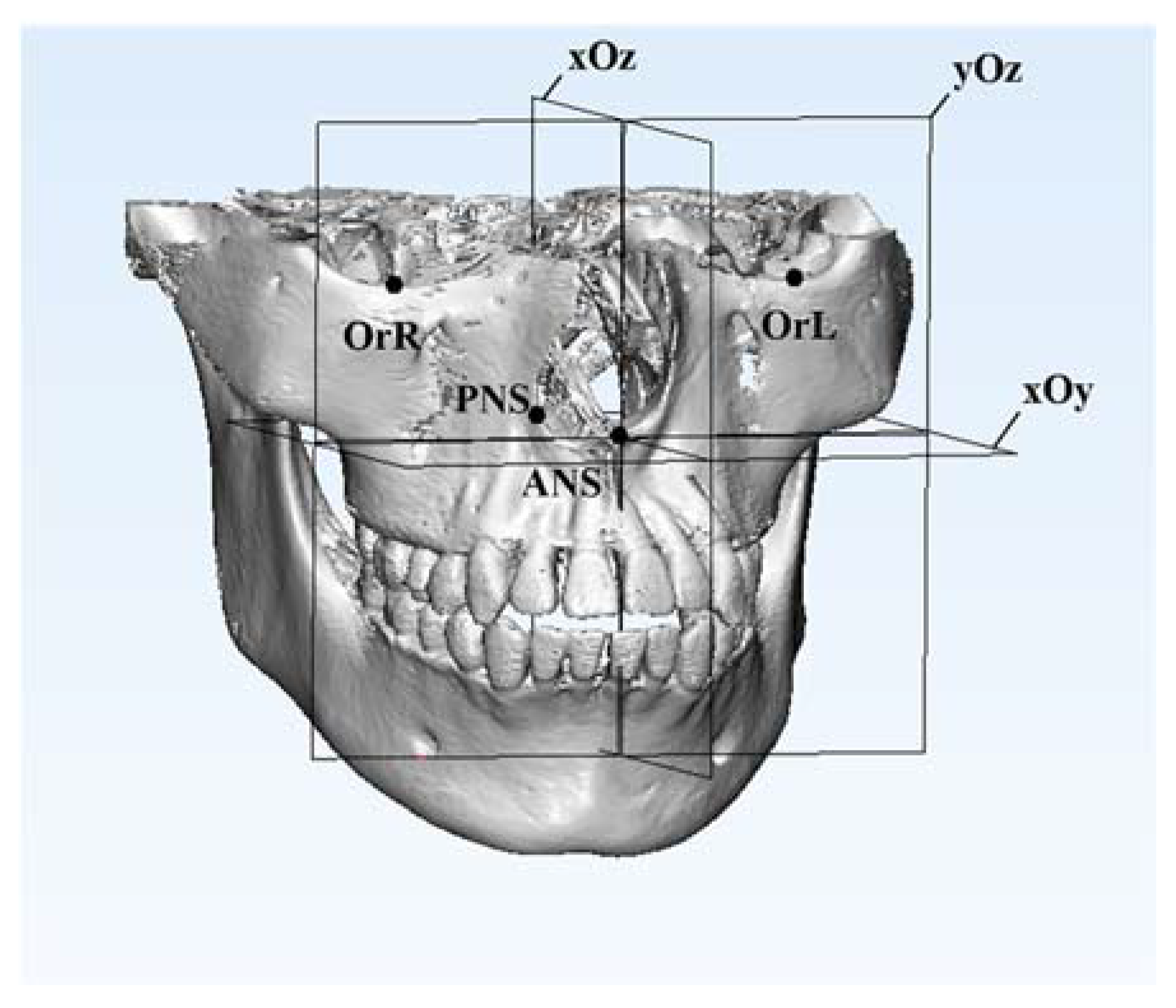
2.3. Construction of Maxilla-Based Coordinate System and Location of Mandibular Measurement Landmarks
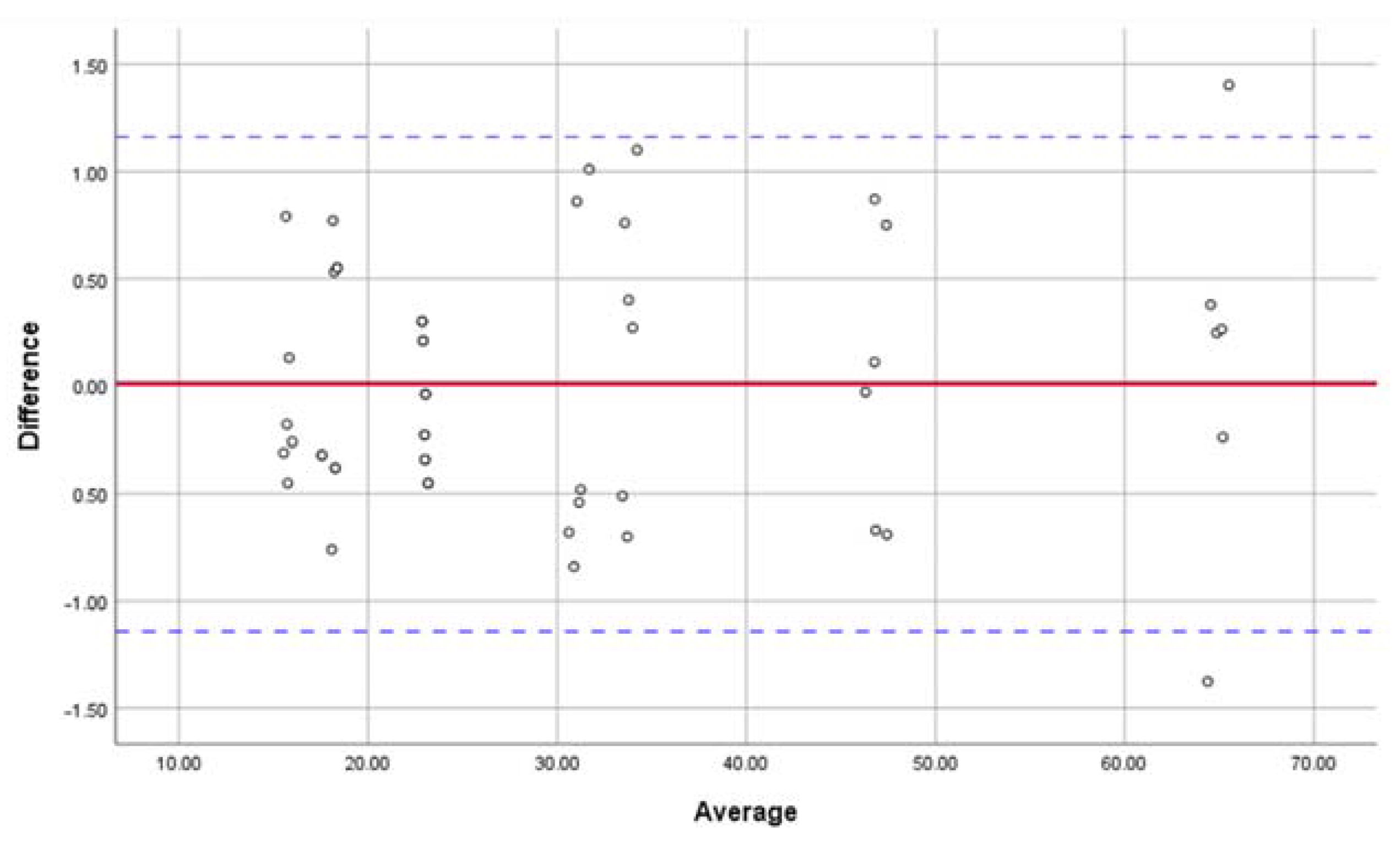
2.4. Data Analysis and Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Venkatesh, E.; Elluru, S.V. Cone beam computed tomography: Basics and applications in dentistry. J. Istanb. Univ. Fac. Dent. 2017, 51, S102–S121. [Google Scholar] [CrossRef] [PubMed]
- Takei, Y.; Monzen, H.; Matsumoto, K.; Hanaoka, K.; Tamura, M.; Nishimura, Y. Registration accuracy with the low dose kilovoltage cone-beam CT: A phantom study. BJR Open 2019, 1, 20190028. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Wang, Y.; Ouyang, W.; Yu, M.; Wang, H. Construction and validity of a midsagittal plane based on the symmetry of a 3-dimensional model of the relevant cranial base. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e49–e58. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Kook, Y.A.; Park, J.H.; Park, J.; Bayome, M.; Vaid, N.R.; Kim, Y. Short-term cone-beam computed tomography evaluation of maxillary third molar changes after total arch distalization in adolescents. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Kheir, N.A.; Kau, C.H. Measuring mandibular asymmetry in Class I normal subjects using 3D novel coordinate system. Ann. Maxillofac. Surg. 2014, 4, 34–38. [Google Scholar]
- Kim, N.K.; Lee, C.; Kang, S.H.; Park, J.W.; Kim, M.J.; Chang, Y.I. A three-dimensional analysis of soft and hard tissue changes after a mandibular setback surgery. Comput. Methods Programs Biomed. 2006, 83, 178–187. [Google Scholar] [CrossRef]
- Pan, F.; Yang, Z.; Wang, J.; Cai, R.; Liu, J.; Zhang, C.; Liao, W. Influence of orthodontic treatment with premolar extraction on the spatial position of maxillary third molars in adult patients: A retrospective cohort cone-bean computed tomography study. BMC Oral Health 2020, 20, 321. [Google Scholar] [CrossRef]
- Guichet, N.F. Biologic laws governing functions of muscles that move the mandible. Part III. Speed of closure--manipulation of the mandible. J. Prosthet. Dent. 1977, 38, 174–179. [Google Scholar] [CrossRef]
- Griffin, C.J.; Hawthorn, R.; Harris, R. Anatomy and histology of the human temporomandibular joint. Monogr. Oral Sci. 1975, 4, 1–26. [Google Scholar]
- Freitas, K.M.; Janson, G.; Tompson, B.; de Freitas, M.R.; Simão, T.M.; Valarelli, F.P.; Cançado, R.H. Posttreatment and physiologic occlusal changes comparison. Angle Orthod. 2013, 83, 239–245. [Google Scholar] [CrossRef]
- Bombonatti, R.; Aliaga-Del Castillo, A.; Bombonatti, J.F.S.; Garib, D.; Tompson, B.; Janson, G. Cephalometric and occlusal changes of Class III malocclusion treated with or without extractions. Dent. Press. J. Orthod. 2020, 25, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, A.P.; Aras, I.; Othman, E.; Aras, A. Comparison of 2 treatment protocols using fixed functional appliances in Class II malocclusion: Treatment results and stability. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Moshiri, S.; Araújo, E.A.; McCray, J.F.; Thiesen, G.; Kim, K.B. Cephalometric evaluation of adult anterior open bite non-extraction treatment with Invisalign. Dent. Press. J. Orthod. 2017, 22, 30–38. [Google Scholar] [CrossRef]
- Pittayapat, P.; Jacobs, R.; Bornstein, M.M.; Odri, G.A.; Kwon, M.S.; Lambrichts, I.; Willems, G.; Politis, C.; Olszewski, R. A new mandible-specific landmark reference system for three-dimensional cephalometry using cone-beam computed tomography. Eur. J. Orthod. 2016, 38, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Almukhtar, A.; Ju, X.; Khambay, B.; McDonald, J.; Ayoub, A. Comparison of the accuracy of voxel based registration and surface based registration for 3D assessment of surgical change following orthognathic surgery. PLoS ONE 2014, 9, e93402. [Google Scholar]
- Äner, S.T.; Kanavakis, G.; Matthey, F.; Gkantidis, N. Voxel-based superimposition of serial craniofacial CBCTs: Reliability, reproducibility and segmentation effect on hard-tissue outcomes. Orthod. Craniofac. Res. 2020, 23, 92–101. [Google Scholar]
- Ghoneima, A.; Cho, H.; Farouk, K.; Kula, K. Accuracy and reliability of landmark-based, surface-based and voxel-based 3D cone-beam computed tomography superimposition methods. Orthod. Craniofac. Res. 2017, 20, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.Y.; Atresh, A.; Ruellas, A.; Cevidanes, L.H.S.; Nguyen, T.; Larson, B.E.; Mangum, J.E.; Manton, D.J.; Schneider, P.M. Three-dimensional condylar changes from Herbst appliance and multibracket treatment: A comparison with matched Class II elastics. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 505–517.e6. [Google Scholar] [CrossRef]
- Haas Junior, O.L.; Guijarro-Martínez, R.; Sousa Gil, A.P.; Méndez-Manjón, I.; Valls-Otañón, A.; de Oliveira, R.B.; Hernández-Alfaro, F. Cranial Base Superimposition of Cone-Beam Computed Tomography Images: A Voxel-Based Protocol Validation. J. Craniofac. Surg. 2019, 30, 1809–1814. [Google Scholar] [CrossRef]
- Ruellas, A.C.; Yatabe, M.S.; Souki, B.Q.; Benavides, E.; Nguyen, T.; Luiz, R.R.; Franchi, L.; Cevidanes, L.H. 3D Mandibular Superimposition: Comparison of Regions of Reference for Voxel-Based Registration. PLoS ONE 2016, 11, e0157625. [Google Scholar] [CrossRef]
- Nguyen, T.; Cevidanes, L.; Franchi, L.; Ruellas, A.; Jackson, T. Three-dimensional mandibular regional superimposition in growing patients. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Song, K.T.; Park, J.H.; Moon, W.; Chae, J.M.; Kang, K.H. Three-dimensional changes of the zygomaticomaxillary complex after mini-implant assisted rapid maxillary expansion. Am. J. Orthod. Dentofacial. Orthop. 2019, 156, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Al Awadi, M.; Chambers, D.W.; Lagravère-Vich, M.O.; Xu, T.; Oh, H. The three-dimensional stable mandibular landmarks in patients between the ages of 12.5 and 17.1 years. BMC Oral Health 2020, 20, 153. [Google Scholar] [CrossRef]
- Noh, H.K.; Park, H.S. Does maxillary yaw exist in patients with skeletal Class III facial asymmetry? Am. J. Orthod. Dentofac. Orthop. 2021, 160, 573–587. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Byun, I.Y.; Kim, J.H.; Park, H.K.; Kim, M.K. Three-dimensional anatomic analysis of mandibular foramen with mandibular anatomic landmarks for inferior alveolar nerve block anesthesia. Oral Surg Oral Med Oral Pathol Oral Radiol 2013, 115, e17–e23. [Google Scholar] [CrossRef] [PubMed]
- Ishaq, R.A.; AlHammadi, M.S.; Fayed, M.M.; El-Ezz, A.A.; Mostafa, Y. Fixed functional appliances with multibracket appliances have no skeletal effect on the mandible: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 612–624. [Google Scholar] [CrossRef]
- Lee, G.H.; Park, J.H.; Moon, D.N.; Lee, S.M. Protocols for orthodontic treatment of patients with temporomandibular joint disorders. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 373–388. [Google Scholar] [CrossRef]
- Han, J.J.; Jung, S.; Park, H.J.; Oh, H.K.; Kook, M.S. Evaluation of Postoperative Mandibular Positional Changes After Mandibular Setback Surgery in a Surgery-First Approach: Isolated Mandibular Surgery Versus Bimaxillary Surgery. J. Oral Maxillofac. Surg. 2019, 77, 181.e1–181.e12. [Google Scholar] [CrossRef]
- Sreelal, T.; Janardanan, K.; Nair, A.S.; Nair, A.S. Age changes in horizontal condylar angle: A clinical and cephalometric study. J. Indian Prosthodont. Soc. 2013, 13, 108–112. [Google Scholar] [CrossRef]
- Kattiney de Oliveira, L.; Fernandes Neto, A.J.; Moraes Mundim Prado, I.; Guimarães Henriques, J.C.; Beom Kim, K.; de Araújo Almeida, G. Evaluation of the condylar position in younger and older adults with or without temporomandibular symptoms by using cone beam computed tomography. J. Prosthet. Dent. 2022, 127, 445–452. [Google Scholar] [CrossRef]
- Ikeda, K.; Kawamura, A. Disc displacement and changes in condylar position. Dentomaxillofac. Radiol. 2013, 42, 84227642. [Google Scholar] [CrossRef] [PubMed]
- Alhammadi, M.S.; Fayed, M.S.; Labib, A. Three-dimensional assessment of condylar position and joint spaces after maxillary first premolar extraction in skeletal Class II malocclusion. Orthod. Craniofac. Res. 2017, 20, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Weissheimer, A.; Menezes, L.M.; Koerich, L.; Pham, J.; Cevidanes, L.H. Fast three-dimensional superimposition of cone beam computed tomography for orthopaedics and orthognathic surgery evaluation. Int. J. Oral Maxillofac. Surg. 2015, 44, 1188–1196. [Google Scholar] [CrossRef]
- Cevidanes, L.H.; Motta, A.; Proffit, W.R.; Ackerman, J.L.; Styner, M. Cranial base superimposition for 3-dimensional evaluation of soft-tissue changes. Am. J. Orthod. Dentofac. Orthop. 2010, 137, S120–S129. [Google Scholar] [CrossRef] [Green Version]
- Scarfe, W.C.; Azevedo, B.; Toghyani, S.; Farman, A.G. Cone Beam Computed Tomographic imaging in orthodontics. Aust. Dent. J. 2017, 62, 33–50. [Google Scholar] [CrossRef]
- Anderson, P.J.; Yong, R.; Surman, T.L.; Rajion, Z.A.; Ranjitkar, S. Application of three-dimensional computed tomography in craniofacial clinical practice and research. Aust. Dent. J. 2014, 59, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, A.K.; Papageorgiou, S.N.; Hatzopoulos, S.A.; Tsirlis, A.; Athanasiou, A.E. Alveolar ridge alterations in the maxillary anterior region after tooth extraction through orthodontic forced eruption for implant site development: A clinical CBCT study. Eur. J. Orthod. 2020, 42, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Yuan, L.; Wang, B.; Zhang, L.; Shen, G.; Fang, B. Changes of alveolar bone dehiscence and fenestration after augmented corticotomy-assisted orthodontic treatment: A CBCT evaluation. Prog. Orthod. 2019, 20, 7. [Google Scholar] [CrossRef]
- Becker, K.; Unland, J.; Wilmes, B.; Tarraf, N.E.; Drescher, D. Is there an ideal insertion angle and position for orthodontic mini-implants in the anterior palate? A CBCT study in humans. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 345–354. [Google Scholar] [CrossRef]
- Shibata, M.; Nawa, H.; Kise, Y.; Fuyamada, M.; Yoshida, K.; Katsumata, A.; Ariji, E.; Goto, S. Reproducibility of three-dimensional coordinate systems based on craniofacial landmarks: A tentative evaluation of four systems created on images obtained by cone-beam computed tomography with a large field of view. Angle Orthod. 2012, 82, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J.; Wang, R.F.; Na, H.J.; Palomo, J.M. Normal range of facial asymmetry in spherical coordinates: A CBCT study. Imaging Sci. Dent. 2013, 43, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Park, K.R.; Park, H.S.; Piao, Z.; Kim, M.K.; Yu, H.S.; Seo, J.K.; Lee, S.H. Three-dimensional vector analysis of mandibular structural asymmetry. J. Craniomaxillofac. Surg. 2013, 41, 338–344. [Google Scholar] [CrossRef]
- Leonardi, R.M.; Aboulazm, K.; Giudice, A.L.; Ronsivalle, V.; D’Antò, V.; Lagravère, M.; Isola, G. Evaluation of mandibular changes after rapid maxillary expansion: A CBCT study in youngsters with unilateral posterior crossbite using a surface-to-surface matching technique. Clin. Oral Investig. 2021, 25, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Claus, J.D.P.; Koerich, L.; Weissheimer, A.; Almeida, M.S.; Belle de Oliveira, R. Assessment of condylar changes after orthognathic surgery using computed tomography regional superimposition. Int. J. Oral Maxillofac. Surg. 2019, 48, 1201–1208. [Google Scholar] [CrossRef]
- Muraglie, S.; Leonardi, R.; Aboulazm, K.; Stumpo, C.; Loreto, C.; Grippaudo, C. Evaluation of structural skeletal asymmetry of the glenoid fossa in adult patients with unilateral posterior crossbite using surface-to-surface matching on CBCT images. Angle Orthod. 2020, 90, 376–382. [Google Scholar] [CrossRef]
- Ruellas, A.C.; Tonello, C.; Gomes, L.R.; Yatabe, M.S.; Macron, L.; Lopinto, J.; Goncalves, J.R.; Garib Carreira, D.G.; Alonso, N.; Souki, B.Q.; et al. Common 3-dimensional coordinate system for assessment of directional changes. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 645–656. [Google Scholar] [CrossRef]
- Elshenawy, H.; Aly, W.; Salah, N.; Nasry, S.; Anter, E.; Ekram, K. Influence of Small, Midi, Medium and Large Fields of View on Accuracy of Linear Measurements in CBCT Imaging: Diagnostic Accuracy Study. Open Access Maced. J. Med. Sci. 2019, 7, 1037–1041. [Google Scholar] [CrossRef]
- Little, D.P. Image quality improvement for medium and large field of view Elekta XVI scans. Australas. Phys. Eng. Sci. Med. 2019, 42, 1153–1164. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Maxillary Basic Landmarks and Basic Planes | |
|---|---|
| OrL | The most inferior point of the left bony orbit |
| OrR | The most inferior point of the left bony orbit |
| ANS | The tip of the anterior nasal spine |
| PNS | The tip of the posterior nasal spine |
| xOy | The horizontal plane, passing through ANS and PNS while parallel to the line OrL-OrR |
| yOz | The sagittal plane, passing through ANS and PNS while perpendicular to the horizontal plane |
| xOz | The frontal plane, passing through ANS while perpendicular to both horizontal plane and sagittal plane |
| Mandibular Measurement Landmarks and Planes | |
|---|---|
| MfL | The most anterior point of the left mental foramen |
| MfR | The most anterior point of the right mental foramen |
| GoL | The midpoint of the bony border of the left mandibular angle |
| GoR | The midpoint of the bony border of the right mandibular angle |
| Gn | The intersection between the mid-sagittal plane and the most anteroinferior point of |
| the mandibular symphysis | |
| R1 | The midpoint of the incisor edge of the mandibular right incisor |
| R7 | The mesial–buccal cusp tip of the mandibular right second molar |
| L7 | The mesial–buccal cusp tip of the mandibular left second molar |
| OP | Occlusal plane, constructed by R1, L7 and R7 |
| MP | Mandibular plane, constructed by Gn, GoL and GoR |
| T0 | T1 | p-Value | |||
|---|---|---|---|---|---|
| Mean (mm) | SD | Mean (mm) | SD | ||
| ANS-PNS | 46.8 | 0.35 | 47.04 | 0.66 | 0.4496 |
| OrL-OrR | 64.96 | 0.64 | 64.9 | 0.6 | 0.8645 |
| OrL to horiz | 22.98 | 0.12 | 23.02 | 0.25 | 0.7375 |
| OrL to sagit | 33.6 | 0.35 | 33.97 | 0.48 | 0.1549 |
| OrL to front | 15.73 | 0.27 | 15.76 | 0.28 | 0.854 |
| OrR to horiz | 22.98 | 0.12 | 23.02 | 0.25 | 0.7375 |
| OrR to sagit | 31.32 | 0.53 | 30.89 | 0.45 | 0.1591 |
| OrR to front | 18.15 | 0.39 | 18.07 | 0.46 | 0.7452 |
| T0 | T1 | T2 | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (mm) | SD | Mean (mm) | SD | Mean (mm) | SD | T0 vs. T1 | T1 vs. T2 | T0 vs. T2 | |
| L7 to horiz | 22.09 | 0.23 | 22.27 | 0.16 | 22.17 | 0.18 | 0.291 | 0.664 | 0.774 |
| L7 to sagit | 26.93 | 0.32 | 28.35 | 0.29 | 27 | 0.2 | 0.000 *** | 0.000 *** | 0.888 |
| L7 to front | 36.62 | 0.43 | 38.4 | 0.26 | 36.57 | 0.24 | 0.000 *** | 0.000 *** | 0.956 |
| R7 to horiz | 21.83 | 0.3 | 21.81 | 0.33 | 21.8 | 0.31 | 0.996 | 0.997 | 0.987 |
| R7 to sagit | 25.24 | 0.4 | 23.61 | 0.46 | 24.81 | 0.55 | 0.000 *** | 0.002 ** | 0.293 |
| R7 to front | 41.36 | 0.25 | 42 | 0.34 | 41.25 | 0.34 | 0.008 ** | 0.002 ** | 0.803 |
| R1 to horiz | 30.54 | 0.19 | 31.08 | 0.15 | 30.63 | 0.23 | 0.001 *** | 0.003 ** | 0.747 |
| R1 to sagit | 2.74 | 0.48 | 0.71 | 0.39 | 2.76 | 0.34 | 0.000 *** | 0.000 *** | 0.995 |
| R1 to front | 0.71 | 0.17 | 0.86 | 0.13 | 0.89 | 0.24 | 0.394 | 0.962 | 0.273 |
| T0 | T1 | T2 | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (mm) | SD | Mean (mm) | SD | Mean (mm) | SD | T0 vs. T1 | T1 vs. T2 | T0 vs. T2 | |
| MfL to horiz | 53.15 | 0.33 | 53.06 | 0.41 | 53.03 | 0.2 | 0.888 | 0.987 | 0.812 |
| MfL to sagit | 22.35 | 0.28 | 24.1 | 0.48 | 22.36 | 0.43 | 0.000 *** | 0.000 *** | 0.999 |
| MfL to front | 24.75 | 0.4 | 27.12 | 0.16 | 24.76 | 0.37 | 0.000 *** | 0.000 *** | 0.999 |
| MfR to horiz | 51.32 | 0.4 | 51.84 | 0.4 | 51.42 | 0.24 | 0.054 | 0.136 | 0.867 |
| MfR to sagit | 21.68 | 0.34 | 20.37 | 0.15 | 21.69 | 0.37 | 0.000 *** | 0.000 *** | 0.999 |
| MfR to front | 28.96 | 0.19 | 30.13 | 0.28 | 29.08 | 0.36 | 0.000 *** | 0.000 *** | 0.76 |
| GoL to horiz | 35.31 | 0.76 | 35.42 | 0.26 | 35.6 | 0.35 | 0.932 | 0.818 | 0.608 |
| GoL to sagit | 48.99 | 0.45 | 49.88 | 0.25 | 49.19 | 0.31 | 0.001 ** | 0.010 ** | 0.604 |
| GoL to front | 74.91 | 0.73 | 76.57 | 0.4 | 74.46 | 0.33 | 0.000 *** | 0.000 *** | 0.315 |
| GoR to horiz | 35.04 | 0.55 | 34.74 | 0.48 | 35.26 | 0.72 | 0.651 | 0.296 | 0.792 |
| GoR to sagit | 39.48 | 0.55 | 39.12 | 0.51 | 39.24 | 0.6 | 0.519 | 0.924 | 0.746 |
| GoR to front | 83.8 | 0.3 | 84.2 | 0.9 | 83.47 | 0.58 | 0.539 | 0.15 | 0.647 |
| Gn to horiz | 66.09 | 0.41 | 66.71 | 0.27 | 66.23 | 0.4 | 0.027 * | 0.087 | 0.805 |
| Gn to sagit | 0.61 | 0.28 | 0.91 | 0.44 | 0.74 | 0.44 | 0.426 | 0.748 | 0.848 |
| Gn to front | 18.26 | 0.38 | 20.77 | 0.5 | 18.65 | 0.55 | 0.000 *** | 0.000 *** | 0.362 |
| T0 | T1 | T2 | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (°) | SD | Mean (°) | SD | Mean (°) | SD | T0 vs. T1 | T1 vs. T2 | T0 vs. T2 | |
| OP with horiz | 12.16 | 0.24 | 12.91 | 0.19 | 12.24 | 0.33 | 0.000 *** | 0.001 ** | 0.851 |
| OP with sagit | 89.19 | 0.26 | 89.61 | 0.43 | 89.24 | 0.21 | 0.079 | 0.127 | 0.961 |
| OP with front | 77.88 | 0.24 | 77.1 | 0.19 | 77.79 | 0.33 | 0.000 *** | 0.001 ** | 0.83 |
| MP with horiz | 26.75 | 0.44 | 27.89 | 0.47 | 26.95 | 0.71 | 0.008 ** | 0.026 * | 0.811 |
| MP with sagit | 87.58 | 0.41 | 88.1 | 0.22 | 87.56 | 0.41 | 0.064 | 0.051 | 0.992 |
| MP with front | 63.38 | 0.43 | 62.19 | 0.49 | 63.18 | 0.74 | 0.007 ** | 0.022 * | 0.823 |
| OP with horiz | 12.16 | 0.24 | 12.91 | 0.19 | 12.24 | 0.33 | 0.000 *** | 0.001 ** | 0.851 |
| OP with sagit | 89.19 | 0.26 | 89.61 | 0.43 | 89.24 | 0.21 | 0.079 | 0.127 | 0.961 |
| OP with front | 77.88 | 0.24 | 77.1 | 0.19 | 77.79 | 0.33 | 0.000 *** | 0.001 ** | 0.83 |
| MP with horiz | 26.75 | 0.44 | 27.89 | 0.47 | 26.95 | 0.71 | 0.008 ** | 0.026 * | 0.811 |
| MP with sagit | 87.58 | 0.41 | 88.1 | 0.22 | 87.56 | 0.41 | 0.064 | 0.051 | 0.992 |
| MP with front | 63.38 | 0.43 | 62.19 | 0.49 | 63.18 | 0.74 | 0.007 ** | 0.022 * | 0.823 |
| OP with horiz | 12.16 | 0.24 | 12.91 | 0.19 | 12.24 | 0.33 | 0.000 *** | 0.001 ** | 0.851 |
| OP with sagit | 89.19 | 0.26 | 89.61 | 0.43 | 89.24 | 0.21 | 0.079 | 0.127 | 0.961 |
| OP with front | 77.88 | 0.24 | 77.1 | 0.19 | 77.79 | 0.33 | 0.000 *** | 0.001 ** | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Ji, L.; Li, Y.; Pan, F.; Liao, W.; Zhao, Z. A Novel Method to Combine Maxilla-Based Coordinate System and Mandibular Voxel-Based Superimposition with Cone-Bean Computed Tomography. J. Clin. Med. 2022, 11, 5229. https://doi.org/10.3390/jcm11175229
Zhang C, Ji L, Li Y, Pan F, Liao W, Zhao Z. A Novel Method to Combine Maxilla-Based Coordinate System and Mandibular Voxel-Based Superimposition with Cone-Bean Computed Tomography. Journal of Clinical Medicine. 2022; 11(17):5229. https://doi.org/10.3390/jcm11175229
Chicago/Turabian StyleZhang, Chenghao, Ling Ji, Yijun Li, Fangwei Pan, Wen Liao, and Zhihe Zhao. 2022. "A Novel Method to Combine Maxilla-Based Coordinate System and Mandibular Voxel-Based Superimposition with Cone-Bean Computed Tomography" Journal of Clinical Medicine 11, no. 17: 5229. https://doi.org/10.3390/jcm11175229
APA StyleZhang, C., Ji, L., Li, Y., Pan, F., Liao, W., & Zhao, Z. (2022). A Novel Method to Combine Maxilla-Based Coordinate System and Mandibular Voxel-Based Superimposition with Cone-Bean Computed Tomography. Journal of Clinical Medicine, 11(17), 5229. https://doi.org/10.3390/jcm11175229