
Biomarker-Guided Assessment of Acute Kidney Injury Phenotypes E among ST-Segment Elevation Myocardial Infarction Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shacham, Y.; Leshem-Rubinow, E.; Steinvil, A.; Assa, E.B.; Keren, G.; Roth, A.; Arbel, Y. Renal impairment according to acute kidney injury network criteria among st elevation myocardial infarction patients undergoing primary percutaneous intervention: A retrospective observational study. Clin. Res. Cardiol. 2014, 103, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Assanelli, E.; Campodonico, J.; De Metrio, M.; Lauri, G.; Marana, I.; Moltrasio, M.; Rubino, M.; Veglia, F.; Montorsi, P.; et al. Acute kidney injury in st-segment elevation acute myocardial infarction complicated by cardiogenic shock at admission. Crit. Care Med. 2010, 38, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Kellum, J.A.; Lameire, N.; Group, K.A.G.W. Diagnosis, evaluation, and management of acute kidney injury: A kdigo summary (part 1). Crit. Care 2013, 17, 204. [Google Scholar] [CrossRef]
- Haase-Fielitz, A.; Haase, M.; Devarajan, P. Neutrophil gelatinase-associated lipocalin as a biomarker of acute kidney injury: A critical evaluation of current status. Ann. Clin. Biochem. 2014, 51, 335–351. [Google Scholar] [CrossRef]
- Helanova, K.; Spinar, J.; Parenica, J. Diagnostic and prognostic utility of neutrophil gelatinase-associated lipocalin (ngal) in patients with cardiovascular diseases—Review. Kidney Blood Press. Res. 2014, 39, 623–629. [Google Scholar] [CrossRef]
- Kafkas, N.; Demponeras, C.; Zoubouloglou, F.; Spanou, L.; Babalis, D.; Makris, K. Serum levels of gelatinase associated lipocalin as indicator of the inflammatory status in coronary artery disease. Int. J. Inflam. 2012, 2012, 189797. [Google Scholar] [CrossRef]
- Khatami, M.R.; Sabbagh, M.R.; Nikravan, N.; Khazaeipour, Z.; Boroumand, M.A.; Sadeghian, S.; Davoudi, B. The role of neutrophil-gelatinase-associated lipocalin in early diagnosis of contrast nephropathy. Indian J. Nephrol. 2015, 25, 292–296. [Google Scholar] [CrossRef]
- Shang, W.; Wang, Z. The update of ngal in acute kidney injury. Curr. Protein Pept. Sci. 2017, 18, 1211–1217. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A. Group NM-aI: Accuracy of neutrophil gelatinase-associated lipocalin (ngal) in diagnosis and prognosis in acute kidney injury: A systematic review and meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef]
- Corbacioglu, S.K.; Cevik, Y.; Akinci, E.; Uzunosmanoglu, H.; Dagar, S.; Safak, T.; Oncul, V.; Guvendi, M. Value of plasma neutrophil gelatinase-associated lipocalin (ngal) in distinguishing between acute kidney injury (aki) and chronic kidney disease (ckd). Turk. J. Emerg. Med. 2017, 17, 85–88. [Google Scholar] [CrossRef]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers from the Acute Disease Quality Initiative Consensus Conference: A Consensus Statement. JAMA Netw. Open. 2020, 3, e2019209. [Google Scholar] [CrossRef] [PubMed]
- Moledina, D.G.; Parikh, C.R. Phenotyping of Acute Kidney Injury: Beyond Serum Creatinine. Semin. Nephrol. 2018, 38, 3–11. [Google Scholar] [CrossRef] [PubMed]
- de Geus, H.R.; Ronco, C.; Haase, M.; Jacob, L.; Lewington, A.; Vincent, J.L. The cardiac surgery-associated neutrophil gelatinase-associated lipocalin (csa-ngal) score: A potential tool to monitor acute tubular damage. J. Thorac. Cardiovasc. Surg. 2016, 151, 1476–1481. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury N: Acute kidney injury network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Nickolas, T.L.; Schmidt-Ott, K.M.; Canetta, P.; Forster, C.; Singer, E.; Sise, M.; Elger, A.; Maarouf, O.; Valle, D.A.S.-D.; O’Rourke, M.; et al. Diagnostic and prognostic stratification in the emergency department using urinary biomarkers of nephron damage: A multicenter prospective cohort study. J. Am. Coll. Cardiol. 2012, 59, 246–255. [Google Scholar] [CrossRef]
- Rozenfeld, K.L.; Zahler, D.; Shtark, M.; Goldiner, I.; Keren, G.; Banai, S.; Shacham, Y. Elevated Neutrophil Gelatinase-Associated Lipocalin for the Assessment of Structural versus Functional Renal Damage among ST-Segment Elevation Myocardial Infarction Patients. Blood Purif. 2020, 49, 560–566. [Google Scholar] [CrossRef]
- Au, V.; Feit, J.; Barasch, J.; Sladen, R.N.; Wagener, G. Urinary neutrophil gelatinase-associated lipocalin (NGAL) distinguishes sustained from transient acute kidney injury after general surgery. Kidney Int. Rep. 2016, 1, 3–9. [Google Scholar] [CrossRef]
- Damman, K.; Valente, M.A.E.; Voors, A.A.; O’Connor, C.M.; van Veldhuisen, D.J.; Hillege, H.L. Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur. Heart J. 2014, 35, 455–469. [Google Scholar] [CrossRef]
- Heywood, J.T.; Fonarow, G.C.; Costanzo, M.R.; Mathur, V.S.; Wigneswaran, J.R.; Wynne, J. High prevalence of renal dysfunction and its impact on outcome in 118,465 patients hospitalized with acute decompensated heart failure: A report from the ADHERE database. J. Card Fail. 2007, 13, 422–430. [Google Scholar] [CrossRef]
- Albert, C.; Albert, A.; Kube, J.; Bellomo, R.; Wettersten, N.; Kuppe, H.; Westphal, S.; Haase, M.; Haase-Fielitz, A. Urinary biomarkers may provide prognostic information for subclinical acute kidney injury after cardiac surgery. J. Thorac. Cardiovasc. Surg. 2018, 155, 2441–2445. [Google Scholar] [CrossRef] [PubMed]
- Joannidis, M.; Forni, L.G.; Haase, M.; Koyner, J.; Shi, J.; Kashani, K.; Chawla, L.; Kellum, J.A. Use of cell cycle arrest biomarkers in conjunction with classical markers of acute kidney injury. Crit. Care Med. 2019, 47, e820-6. [Google Scholar] [CrossRef] [PubMed]
- Coca, S.G.; Garg, A.X.; Thiessen-Philbrook, H.; Koyner, J.L.; Patel, U.D.; Krumholz, H.M.; Shlipak, M.G.; Parikh, C.R. Urinary biomarkers of AKI and mortality 3 years after cardiac surgery. J. Am. Soc. Nephrol. 2014, 25, 1063–1071. [Google Scholar] [CrossRef]
- Koyner, J.L.; Shaw, A.D.; Chawla, L.S.; Hoste, E.A.J.; Bihorac, A.; Kashani, K.; Haase, M.; Shi, J.; Kellum, J.A. Tissue Inhibitor Metalloproteinase-2 (TIMP-2)•IGF-Binding Protein-7 (IGFBP-7) levels are associated with adverse long-term outcomes in patients with AKI. J. Am. Soc. Nephrol. 2015, 26, 1747–1754. [Google Scholar] [CrossRef]
- Kellum, J.A.; Sileanu, F.E.; Murugan, R.; Lucko, N.; Shaw, A.D.; Clermont, G. Classifying AKI by Urine Output versus Serum Creatinine Level. J. Am. Soc. Nephrol. JASN 2015, 26, 2231–2238. [Google Scholar] [CrossRef] [PubMed]
- Kofman, N.; Margolis, G.; Gal-Oz, A.; Letourneau-Shesaf, S.; Keren, G.; Rozenbaum, Z.; Shacham, Y. Long-term renal outcomes and mortality following renal injury among myocardial infarction patients treated by primary percutaneous intervention. Coron. Artery Dis. 2019, 30, 87–92. [Google Scholar] [CrossRef]
- Margolis, G.; Gal-Oz, A.; Letourneau-Shesaf, S.; Khoury, S.; Keren, G.; Shacham, Y. Acute kidney injury based on the KDIGO criteria among ST elevation myocardial infarction patients treated by primary percutaneous intervention. J. Nephrol. 2018, 31, 423–428. [Google Scholar] [CrossRef]
- Barbarash, O.L.; Bykova, I.S.; Kashtalap, V.V.; Zykov, M.V.; Hryachkova, O.N.; Kalaeva, V.V.; Shafranskaya, K.S.; Karetnikova, V.N.; Kutikhin, A.G. Serum neutrophil gelatinase-associated lipocalin has an advantage over serum cystatin C and glomerular filtration rate in prediction of adverse cardiovascular outcome in patients with ST-segment elevation myocardial infarction. BMC Cardiovasc. Disord. 2017, 17, 81. [Google Scholar] [CrossRef]
- Akcay, A.B.; Ozlu, M.F.; Sen, N.; Cay, S.; Ozturk, O.H.; Yalcn, F.; Bilen, P.; Kanat, S.; Karakas, M.F.; Isleyen, A.; et al. Prognostic significance of neutrophil gelatinase associated lipocalin in St-segment elevation myocardial infarction. J. Investig. Med. 2012, 60, 508–513. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | No AKI n = 176 | Subclinical AKI n = 46 | Hemodynamic AKI n = 17 | Severe AKI n = 42 | p Value |
|---|---|---|---|---|---|
| Age, years, mean ± SD | 63.35 ± 13.4 | 72.4 ± 13.3 | 69.4 ± 9.4 | 74.3 ± 11. | <0.001 |
| Male gender, n (%) | 30(17) | 13(28.3) | 3(17.6) | 11(26.2) | 0.269 |
| BMI, median [IQR] | 27.4 [24.7–30.3] | 27.9 [25.6–31.3] | 27.7 [25.3–29] | 25.3 [23.2–28.1] | 0.047 |
| Diabetes mellitus, n (%) | 57 (32.4) | 16 (34.8) | 5 (29.4) | 17 (40.5) | 0.763 |
| Hypertension, n (%) | 92 (521.3) | 32 (69.6) | 16 (94.1) | 33 (78.6) | <0.001 |
| Hyperlipidemia, n (%) | 103 (58.5) | 29 (63) | 10 (58.8) | 27 (64.3) | 0.881 |
| Obesity, n (%) | 47 (26.7) | 15 (32.6) | 2 (11.8) | 7 (16.7) | 0.188 |
| Past MI, n (%) | 40 (22.7) | 19 (41.3) | 4 (23.5) | 17 (40.5) | 0.021 |
| Smoker, n (%) | 82 (46.6) | 22 (47.8) | 9 (52.9) | 11 (26.2) | 0.082 |
| Family history of IHD, n (%) | 38 (21.6) | 3 (6.5) | 0 (0) | 4 (9.5) | 0.008 |
| Heart rate (beats per minute), mean ± SD | 77.9 ± 18.6 | 78.7 ± 16.4 | 80.8 ± 22.6 | 89.2 ± 20.3 | 0.007 |
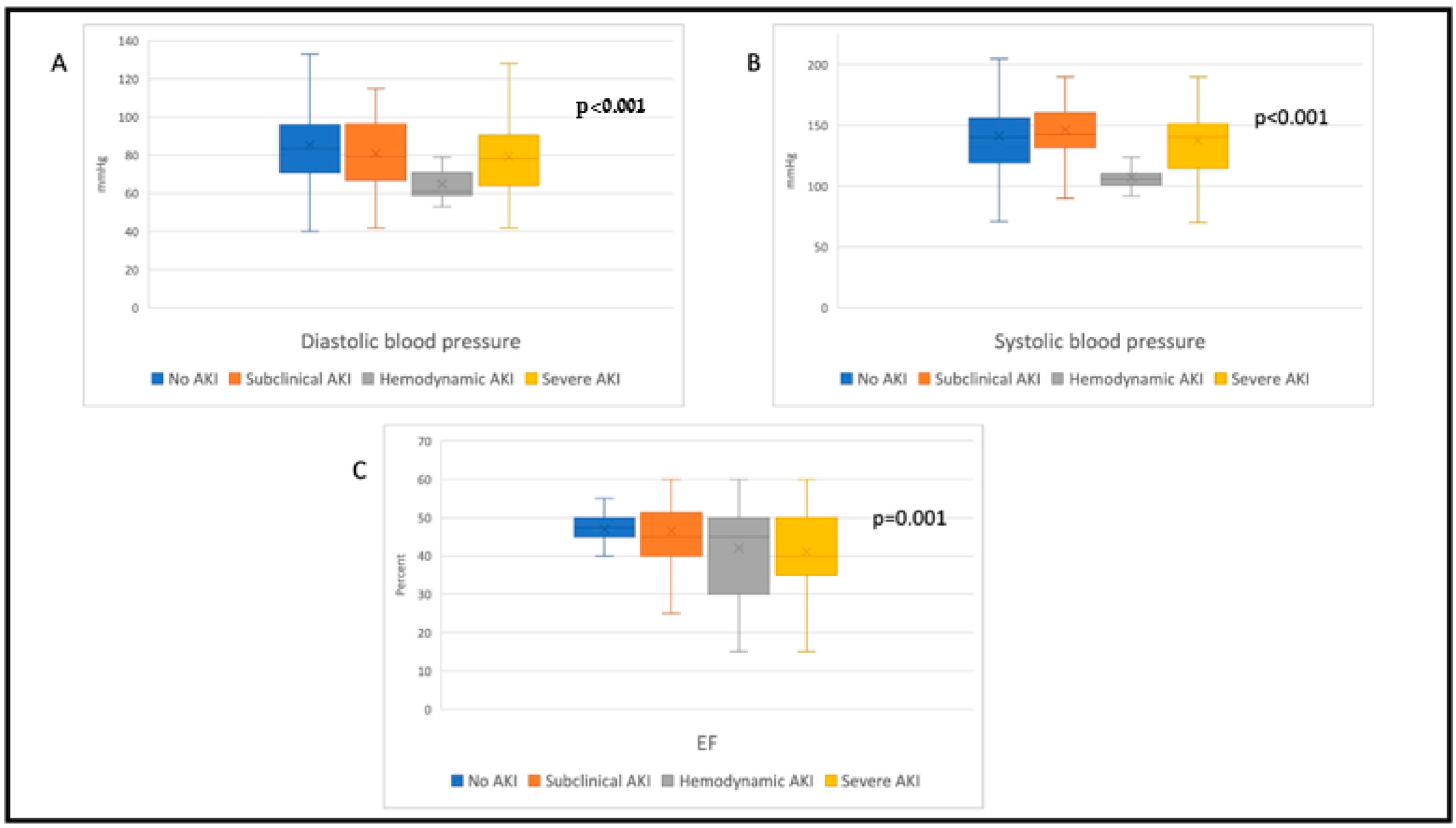
| Systolic blood pressure (mmHg), mean ± SD | 140.9 ± 29.7 | 145.4 ± 30.7 | 107.5 ± 8.5 | 137.6 ± 32.1 | <0.001 |
| Diastolic blood pressure (mmHg), mean ± SD | 85.6 ± 18.5 | 82.3 ± 16.9 | 64.9 ± 7.8 | 79.4 ± 2.9 | <0.001 |
| EF%, mean ± SD | 47 ± 8.3 | 46.5 ± 8.6 | 42 ± 12.9 | 41.1 ± 9.1 | <0.001 |
| Hemoglobin (g/dL), median [IQR] | 14.5 [13.4–15.5] | 13.7 [12.8–16.2] | 13.6 [12.8–14.5] | 12.7 [11.1–15.2] | <0.001 |
| White blood cells (10 × 103/µL), mean ± SD | 11 ± 3.9 | 10.3 ± 3.5 | 10.5 ± 4.1 | 12.3 ± 4.2 | 0.099 |
| Troponin I (ng/L), median [IQR] | 23,154 [10,575,72,401] | 15,179 [3394–58,105] | 17,385 [8471–94,224] | 12,707 [738,197,861] | 0.683 |
| HR for MACE | 95% Confidence Interval | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| No AKI | Reference for baseline hazard | |||
| Subclinical AKI | 4.151 | 2.068 | 8.331 | <0.001 |
| Hemodynamic AKI | 4.517 | 1.608 | 12.691 | 0.004 |
| Severe AKI | 12.964 | 5.597 | 30.028 | <0.001 |
| Past MI | 0.574 | 0.308 | 1.069 | 0.080 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banai, A.; Frydman, S.; Abu Katash, H.; Stark, M.; Goldiner, I.; Banai, S.; Shacham, Y. Biomarker-Guided Assessment of Acute Kidney Injury Phenotypes E among ST-Segment Elevation Myocardial Infarction Patients. J. Clin. Med. 2022, 11, 5402. https://doi.org/10.3390/jcm11185402
Banai A, Frydman S, Abu Katash H, Stark M, Goldiner I, Banai S, Shacham Y. Biomarker-Guided Assessment of Acute Kidney Injury Phenotypes E among ST-Segment Elevation Myocardial Infarction Patients. Journal of Clinical Medicine. 2022; 11(18):5402. https://doi.org/10.3390/jcm11185402
Chicago/Turabian StyleBanai, Ariel, Shir Frydman, Hytham Abu Katash, Moshe Stark, Ilana Goldiner, Shmuel Banai, and Yacov Shacham. 2022. "Biomarker-Guided Assessment of Acute Kidney Injury Phenotypes E among ST-Segment Elevation Myocardial Infarction Patients" Journal of Clinical Medicine 11, no. 18: 5402. https://doi.org/10.3390/jcm11185402