
Reablation in Atrial Fibrillation Recurrence and Pulmonary Vein Reconnection: Cryoballoon versus Radiofrequency as Index Ablation Procedures

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. CB and RF Ablation Procedures for AF
2.3. Follow-Up
2.4. Variables and Endpoints
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Follow-up Period and Reablation
3.3. Need for Reablation in Patients with CB and RF Ablation
3.4. Need for Reablation in Patients with Paroxysmal and Persistent AF
3.5. Identification of Predictors of Reablation in Patients with CB and RF Ablation
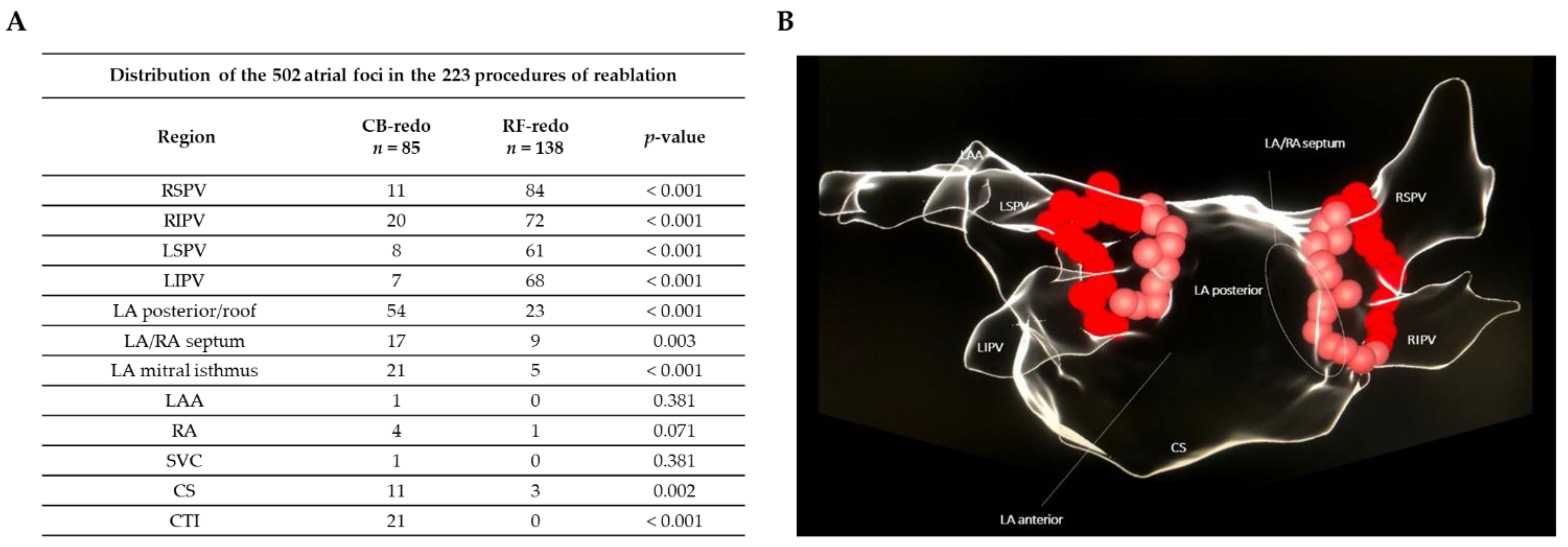
3.6. PV Reconnection in Patients with Reablation
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedural Complications and Duration | Total n = 1055 | CB- Group n = 557 | RF-Group n = 498 | p-Value |
|---|---|---|---|---|
| Major complications; n % | 38 (3.6%) | 15 (2.7%) | 23 (4.6%) | 0.099 |
| 7 (0.7%) | 7 (1.3%) | 0 (0.0%) | 0.011 |
| 7 (0.7%) | 1 (0.2%) | 6 (1.2%) | 0.010 |
| 11 (1.0%) | 4 (0.7%) | 7 (1.4%) | 0.086 |
| 3 (0.3%) | 0 (0.0%) | 3 (0.6%) | 0.194 |
| 4 (0.4%) | 1 (0.2%) | 3 (0.6%) | 0.269 |
| 6 (0.6%) | 2 (0.4%) | 4 (0.8%) | 0.290 |
| Minor complications; n % | 54 (5.1%) | 34 (6.1%) | 20 (4.0%) | 0.161 |
| 9 (0.9%) | 3 (0.6%) | 6 (1.2%) | 0.321 |
| 21 (1.9%) | 21 (3.7%) | 0 (0.0%) | <0.001 |
| 7 (0.7%) | 5 (0.9%) | 2 (0.4%) | 0.277 |
| 14 (1.3%) | 4 (0.7%) | 10 (2.0%) | 0.058 |
| 3 (0.3%) | 1 (0.2%) | 2 (0.4%) | 0.544 |
| ** Death from the procedure; n % | 1 (0.1%) | 0 (0.0%) | 1 (0.2%) | 0.222 |
| Total fluoroscopy time (min); mean ± SD | - | 17.4 ± 17.2 | 7.2 ± 5.7 | <0.001 |
| Total duration (min); mean ± SD | - | 46.1 ± 25.6 | 77.2 ± 30.5 | <0.001 |
| Characteristic | Total n = 223 | CB-Redo n = 85 | RF-Redo n = 138 | p-Value |
|---|---|---|---|---|
| Age (years); mean ± SD | 55.8 ± 11.0 | 56.8 ± 11.5 | 55.3 ± 10.6 | 0.346 |
| Sex, male; n % | 149 (66.8%) | 58 (68.2%) | 91 (65.6%) | 0.420 |
| Left atrial diameter (mm); mean ± SD | 40.3 ± 4.4 | 39.4 ± 4.8 | 40.9 ± 3.9 | 0.028 |
| Hypertension; n % | 131 (58.7%) | 56 (65.8%) | 75 (54.3%) | 0.094 |
| Diabetes mellitus; n % | 29 (13.0%) | 13 (15.3%) | 16 (11.6%) | 0.303 |
| Dyslipidemia; n % | 82 (36.7%) | 36 (42.4%) | 46 (33.3%) | 0.153 |
| Active smoking; n % | 32 (14.3%) | 12 (14.1%) | 20 (14.5%) | 0.342 |
| Severe OSA; n % | 59 (26.4%) | 26 (30.6%) | 33 (23.9%) | 0.298 |
| Body-mass index (kg/m2); mean ± SD | 27.9 ± 4.2 | 29.6± 5.5 | 27.2± 3.5 | 0.165 |
| Previous heart disease (s); n % | 39 (17.4%) | 21 (24.7%) | 18 (13.0%) | 0.015 |
| 4 (1.8%) | 1 (1.2%) | 3 (2.2%) | 0.507 |
| 14 (6.3%) | 10 (11.7%) | 4 (2.9%) | 0.011 |
| 4 (1.8%) | 2 (2.3%) | 2 (1.4%) | 0.493 |
| 12 (5.4%) | 0 (0.0%) | 3 (2.2%) | 0.235 |
| 6 (2.7%) | 5 (5.9%) | 1 (0.7%) | 0.031 |
| 8 (3.6%) | 3 (3.5%) | 5 (3.6%) | 0.639 |
| 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Previous PCI; n % | 11 (4.9%) | 8 (9.4%) | 3 (2.2%) | 0.019 |
| Previous CABG; n % | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | - |
| Left systolic ventricular function (%); mean ± SD | 58.6 ± 5.2% | 57.4 ± 7% | 59.4 ± 3.2% | 0.016 |
| Persistent AF; n % | 86 (39.6%) | 31 (36.4%) | 55 (39.8%) | 0.359 |
| Early recurrence; n % | 55 (24.6%) | 21 (24.7%) | 34 (24.6%) | 0.556 |
| Treatment after recurrence; n % | ||||
| 156 (70.0%) | 70 (82.4%) | 86 (62.3%) | 0.195 |
| 207 (92.8%) | 77 (90.6%) | 130 (94.2%) | 0.453 |
| Previous electrical cardioversion; n % | 42 (18.8%) | 18 (21.2%) | 24 (17.4%) | 0.637 |
References
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation 2014, 130, 199–267. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS) The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- Verma, A.; Jiang, C.Y.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. for the STAR AF II Investigators. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H.; Brugada, J.; Fürnkranz, A.; Metzner, A.; Ouyang, F.; Chun, K.J.; Elvan, A.; Arentz, T.; Bestehorn, K.; Pocock, S.J.; et al. for the FIRE AND ICE Investigators*. Cryoballoon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation. N. Engl. J. Med. 2016, 374, 2235–2245. [Google Scholar] [CrossRef] [PubMed]
- Luik, A.; Radzewitz, A.; Kieser, M.; Walter, M.; Bramlage, P.; Hörmann, P.; Schmidt, K.; Horn, N.; Brinkmeier-Theofanopoulou, M.; Kunzmann, K.; et al. Cryoballoon versus open irrigated radio frequency ablation in patients with paroxysmal atrial fibrillation: The prospective, randomized, controlled, noninferiority FreezeAF Study. Circulation 2015, 132, 1311–1319. [Google Scholar] [CrossRef] [PubMed]
- Wasserlauf, J.; Pelchovitz, D.J.; Rhyner, J.; Verma, N.; Bohn, M.; Li, Z.; Arora, R.; Chicos, A.B.; Goldberger, J.J.; Kim, S.S.; et al. Cryoballoon versus radiofrequency catheter ablation for paroxysmal atrial fibrillation. Pacing. Clin. Electrophysiol. 2015, 38, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Jourda, F.; Providencia, R.; Marijon, E.; Bouzeman, A.; Hireche, H.; Khoueiry, Z.; Cardin, C.; Combes, N.; Combes, S.; Boveda, S.; et al. Contact-force guided radiofrequency vs. second-generation balloon cryotherapy for pulmonary vein isolation in patients with paroxysmal atrial fibrillation-a prospective evaluation. Europace 2015, 17, 225–231. [Google Scholar] [CrossRef]
- Squara, F.; Zhao, A.; Marijon, E.; Latcu, D.G.; Providencia, R.; Di Giovanni, G.; Jauvert, G.; Jourda, F.; Chierchia, G.B.; De Asmundis, C.; et al. Comparison between radiofrequency with contact force-sensing and second-generation cryoballoon for paroxysmal atrial fibrillation catheter ablation: A multicentre European evaluation. Europace 2015, 17, 718–724. [Google Scholar] [CrossRef]
- Fitzgerald, J.L.; Middeldorp, M.E.; Gallagher, C.; Sanders, P. Lifestyle Modification and Atrial Fibrillation: Critical Care for Successful Ablation. J. Clin. Med. 2022, 11, 2660. [Google Scholar] [CrossRef]
- Matiello, M.; Nadal, M.; Tamborero, D.; Berruezo, A.; Montserrat, J.; Embid, C.; Rios, J.; Villacastín, J.; Brugada, J.; Mont, L. Low efficacy of atrial fibrillation ablation in severe obstructive sleep apnea patients. Europace 2010, 12, 1084–1089. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Blomström-Lundqvist, C.; Gizurarson, S.; Schwieler, J.; Jensen, S.M.; Bergfeldt, L.; Kennebäck, G.; Rubulis, A.; Malmborg, H.; Raatikainen, P.; Lönnerholm, S.; et al. Effect of catheter ablation vs antiarrhythmic medication on quality of life in patients with atrial fibrillation: The CAPTAF randomized clinical trial. JAMA 2019, 321, 1059–1068. [Google Scholar] [CrossRef] [PubMed]
- Mark, D.B.; Anstrom, K.J.; Sheng, S.; Piccini, J.P.; Baloch, K.N.; Monahan, K.H.; Daniels, M.R.; Bahnson, T.D.; Poole, J.E.; Rosenberg, Y.; et al. Effect of catheter ablation vs medical therapy on quality of life among patients with atrial fibrillation: The CABANA randomized clinical trial. JAMA 2019, 321, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.G.; Champagne, J.; Dubuc, M.; Deyell, M.W.; Verma, A.; Macle, L.; Leong-Sit, P.; Novak, P.; Badra-Verdu, M.; Sapp, J.; et al. For the CIRCA-DOSE Study Investigators. Cryoballoon or Radiofrequency Ablation for Atrial Fibrillation Assessed by Continuous Monitoring. Circulation 2019, 140, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Bergau, L.; Bengel, P.; Sciacca, V.; Fink, T.; Sohns, C.; Sommer, P. Atrial Fibrillation and Heart Failure. J. Clin. Med. 2022, 11, 2510. [Google Scholar] [CrossRef]
- Holmqvist, F.; Simon, D.; Steinberg, B.A.; Hong, S.J.; Kowey, P.R.; Reiffel, J.A.; Naccarelli, G.V.; Chang, P.; Gersh, B.J.; Peterson, E.D.; et al. ORBIT-investigators. Catheter Ablation of Atrial Fibrillation in U.S. Community Practice—Results from Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). J. Am. Heart Assoc. 2015, 4, e001901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.H.; Uhm, J.S.; Kim, J.Y.; Joung, B.; Lee, M.H.; Pak, H.N. Does Additional Electrogram-Guided Ablation After Linear Ablation Reduce Recurrence After Catheter Ablation for Longstanding Persistent Atrial Fibrillation? A Prospective Randomized Study. J. Am. Heart Assoc. 2017, 6, e004811. [Google Scholar] [CrossRef] [PubMed]
- Kuck, K.H.; Fürnkranz, A.; Chun, K.J.; Metzner, A.; Ouyang, F.; Schlüter, M.; Elvan, A.; Lim, H.W.; Kueffer, F.J.; Arentz, T.; et al. Cryoballoon or radiofrequency ablation for symptomatic paroxysmal atrial fibrillation: Reintervention, rehospitalization and quality-of-life outcomes in the FIRE AND ICE trial. Eur. Heart J. 2016, 37, 2858–2865. [Google Scholar] [CrossRef] [Green Version]
- Cheung, C.C.; Deyell, M.W.; Macle, L.; Verma, A.; Champagne, J.; Leong-Sit, P.; Novak, P.; Badra-Verdu, M.; Sapp, J.; Khairy, P.; et al. Repeat atrial fibrillation ablation procedure in the CIRCA-DOSE Study. Circ. Arrhythmia Electrophysiol. 2020, 13, e008480. [Google Scholar] [CrossRef]
- Kuck, K.H.; Albenque, J.P.; Chun, K.J.; Fürnkranz, A.; Busch, M.; Elvan, A.; Schlüter, M.; Braegelmann, K.M.; Kueffer, F.J.; Hemingway, L.; et al. Fire and Ice investigators. Repeat Ablation for Atrial Fibrillation Recurrence Post Cryoballoon or Radiofrequency Ablation in the FIRE AND ICE Trial Circ Arrhythm Electrophysiol. Circ. Arrhythmia Electrophysiol. 2019, 12, e007247. [Google Scholar] [CrossRef]
- Kany, S.; Brachmann, J.; Lewalter, T.; Kuck, K.H.; Andresen, D.; Willems, S.; Hoffmann, E.; Eckardt, L.; Thomas, D.; Hochadel, M.; et al. Safety and patient-reported outcomes in index ablation versus repeat ablation in atrial fibrillation: Insights from the German Ablation Registry. Clin. Res. Cardiol. 2021, 110, 841–850. [Google Scholar] [CrossRef]
- Chen, S.; Schmidt, B.; Bordignon, S.; Bologna, F.; Perrotta, L.; Nagase, T.; Chun, K.J. Atrial fibrillation ablation using cryoballoon technology: Recent advances and practical techniques. J. Cardiovasc. Electrophysiol. 2018, 29, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Nery, P.B.; Belliveau, D.; Nair, G.M.; Bernick, J.; Redpath, C.J.; Szczotka, A.; Sadek, M.M.; Green, M.S.; Wells, G.; Birnie, D.H. Relationship Between Pulmonary Vein Reconnection and Atrial Fibrillation Recurrence. J. Am. Coll. Cardiol. EP. 2016, 2, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, S.; Sekihara, T.; Hasegawa, K.; Mukai, M.; Aoyama, D.; Nodera, M.; Tada, H. The feasibility and safety of substrate modification on the left atrial roof area using a cryoballoon in atrial fibrillation ablation. Int. J. Cardiol. 2019, 350, 41–47. [Google Scholar] [CrossRef] [PubMed]




| Characteristic | Total n = 1055 | CB Group n = 557 | RF Group n = 498 | p-Value |
|---|---|---|---|---|
| Age (years); mean ± SD | 56.5 ± 11.0 | 57.0 ± 11.0 | 55.8 ± 11.0 | 0.103 |
| Sex, male; n % | 721 (68.3%) | 376 (67.5%) | 345 (69.3%) | 0.291 |
| Body mass index (kg/m2); mean ± SD | 28.9 ± 4.9 | 29.3 ± 5.0 | 28.4 ± 4.6 | 0.105 |
| Active smoking; n % | 133 (15.6%) | 72 (15.9%) | 61 (15.3%) | 0.276 |
| Hypertension; n % | 589 (56.9%) | 322 (57.9%) | 267 (55.7%) | 0.261 |
| Diabetes mellitus; n % | 123 (11.9%) | 60 (10.8%) | 63 (13.2%) | 0.141 |
| Dyslipidemia; n % | 370 (42.6%) | 199 (43.4%) | 171 (41.8%) | 0.348 |
| Severe OSA; n % | 233 (26.1%) | 140 (28.7%) | 93 (22.9%) | 0.027 |
| LA diameter (mm); mean ± SD | 39.2 ± 4.2 | 38.6 ± 3.8 | 39.8 ± 4.4 | 0.225 |
| Previous heart disease(s); n % | 156 (14.8%) | 86 (15.4%) | 70 (14%) | 0.374 |
| 13 (1.2%) | 9 (1.6%) | 4 (0.8%) | 0.181 |
| 65 (6.1%) | 42 (7.5%) | 23 (4.6%) | 0.032 |
| 17 (1.6%) | 5 (0.9%) | 12 (2.4%) | 0.044 |
| 12 (1.1%) | 4 (0.7%) | 8 (1.4%) | 0.143 |
| 18 (1.7%) | 12 (2.1%) | 6 (1.2%) | 0.171 |
| 26 (2.4%) | 13 (2.3%) | 13 (2.6%) | 0.463 |
| 1 (0.1%) | 1 (0.2%) | 0 (0.0%) | 0.528 |
| 4 (0.4%) | 0 (0.0%) | 4 (0.8%) | 0.049 |
| Previous PCI; n % | 43 (4.1%) | 27 (4.8%) | 16 (3.2%) | 0.164 |
| Previous CABG; n % | 2 (0.2%) | 2 (0.4%) | 0 (0.0%) | 0.110 |
| Left systolic ventricular function (%); mean ± SD | 59.0 ± 4.8 | 58.5 ± 5.9 | 59.4 ± 3.1 | 0.288 |
| Previous treatment; n % | ||||
| 870 (82.5%) | 444 (79.7%) | 426 (85.5%) | 0.113 |
| 892 (84.5%) | 469 (84.3%) | 423 (84.9%) | 0.521 |
| Persistent AF; n % | 295 (28.0%) | 146 (26.2%) | 149 (29.9%) | 0.102 |
| Cox Regression Model | Independent Variable | HR (95% CI) | p-Value |
|---|---|---|---|
| Model 1 | Age | 0.51 (0.39–0.67) | <0.001 |
| Sex | |||
| Model 2 | Age | 0.47 (0.36–0.60) | <0.001 |
| Sex | |||
| Active smoking | |||
| Hypertension | |||
| Diabetes mellitus | |||
| Dyslipidemia | |||
| Model 3 | Age | 0.45 (0.32–0.51) | <0.001 |
| Sex | |||
| Active smoking | |||
| Hypertension | |||
| Diabetes mellitus | |||
| Dyslipidemia | |||
| Severe OSA | |||
| Dilated LA | |||
| Persistent AF | |||
| Early recurrence |
| Independent Variable | Cox Regression Model for Reablation | ||
|---|---|---|---|
| HR | 95% CI | p-Value | |
| RF ablation | 2.25 | 1.63–3.10 | <0.001 |
| Age | 0.99 | 0.97–1.00 | 0.161 |
| Sex, male | 1.12 | 0.79–1.59 | 0.526 |
| Active smoking | 0.79 | 0.50–1.16 | 0.203 |
| Hypertension | 1.12 | 0.80–1.58 | 0.513 |
| Diabetes mellitus | 1.02 | 0.66–1.61 | 0.927 |
| Dyslipidemia | 1.07 | 0.80–1.41 | 0.659 |
| Severe OSA | 1.36 | 0.98–1.90 | 0.067 |
| Dilated LA | 1.42 | 1.03–1.96 | 0.032 |
| Persistent AF | 1.49 | 1.07–2.06 | 0.017 |
| Early recurrence | 5.85 | 3.94–8.67 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Ramos, A.I.; Ruiz-Salas, A.; Medina-Palomo, C.; Pavón-Morón, F.J.; Rodríguez-Capitán, J.; Gutiérrez-Bedmar, M.; Berteli-García, G.; Fernández-Lozano, I.; Gómez-Doblas, J.J.; Jiménez-Navarro, M.; et al. Reablation in Atrial Fibrillation Recurrence and Pulmonary Vein Reconnection: Cryoballoon versus Radiofrequency as Index Ablation Procedures. J. Clin. Med. 2022, 11, 5862. https://doi.org/10.3390/jcm11195862
Molina-Ramos AI, Ruiz-Salas A, Medina-Palomo C, Pavón-Morón FJ, Rodríguez-Capitán J, Gutiérrez-Bedmar M, Berteli-García G, Fernández-Lozano I, Gómez-Doblas JJ, Jiménez-Navarro M, et al. Reablation in Atrial Fibrillation Recurrence and Pulmonary Vein Reconnection: Cryoballoon versus Radiofrequency as Index Ablation Procedures. Journal of Clinical Medicine. 2022; 11(19):5862. https://doi.org/10.3390/jcm11195862
Chicago/Turabian StyleMolina-Ramos, Ana Isabel, Amalio Ruiz-Salas, Carmen Medina-Palomo, Francisco Javier Pavón-Morón, Jorge Rodríguez-Capitán, Mario Gutiérrez-Bedmar, Germán Berteli-García, Ignacio Fernández-Lozano, Juan José Gómez-Doblas, Manuel Jiménez-Navarro, and et al. 2022. "Reablation in Atrial Fibrillation Recurrence and Pulmonary Vein Reconnection: Cryoballoon versus Radiofrequency as Index Ablation Procedures" Journal of Clinical Medicine 11, no. 19: 5862. https://doi.org/10.3390/jcm11195862
APA StyleMolina-Ramos, A. I., Ruiz-Salas, A., Medina-Palomo, C., Pavón-Morón, F. J., Rodríguez-Capitán, J., Gutiérrez-Bedmar, M., Berteli-García, G., Fernández-Lozano, I., Gómez-Doblas, J. J., Jiménez-Navarro, M., Alzueta-Rodríguez, J., & Barrera-Cordero, A. (2022). Reablation in Atrial Fibrillation Recurrence and Pulmonary Vein Reconnection: Cryoballoon versus Radiofrequency as Index Ablation Procedures. Journal of Clinical Medicine, 11(19), 5862. https://doi.org/10.3390/jcm11195862