
Demarcation Line Depth in Epithelium-Off Corneal Cross-Linking Performed at the Slit Lamp
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CXL Procedure
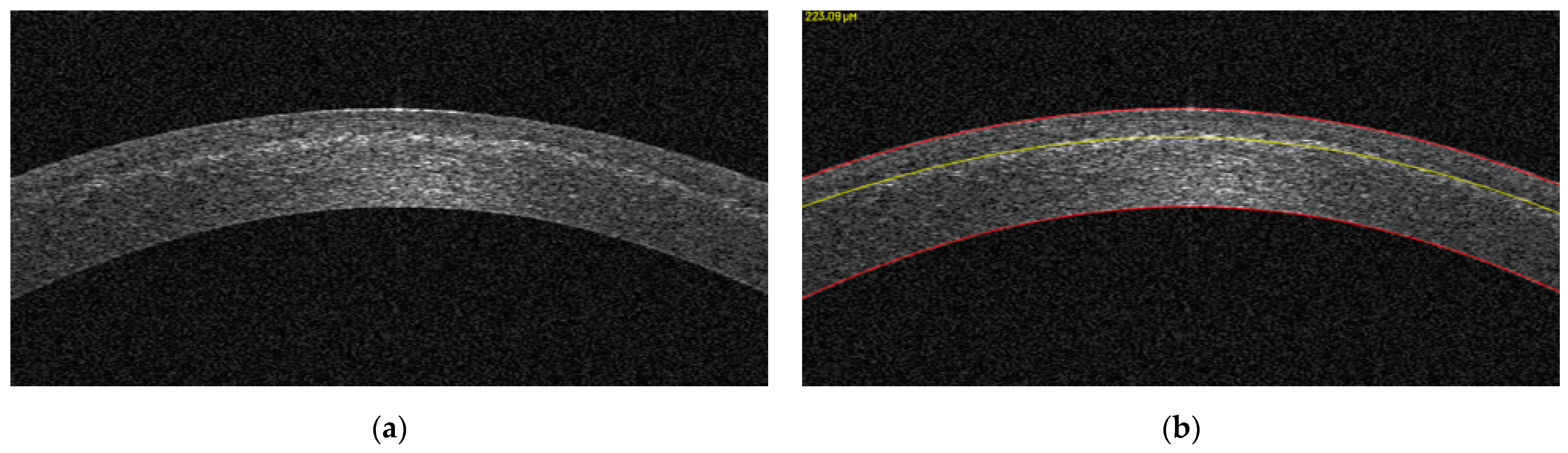
2.3. Analysis of Demarcation Line Depth
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wollensak, G.; Spoerl, E.; Seiler, T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am. J. Ophthalmol. 2003, 135, 620–627. [Google Scholar] [CrossRef]
- Raiskup, F.; Spoerl, E. Corneal crosslinking with riboflavin and ultraviolet A. Part II. Clinical indications and results. Ocul. Surf. 2013, 11, 93–108. [Google Scholar] [CrossRef]
- Seiler, T.; Hafezi, F. Corneal cross-linking-induced stromal demarcation line. Cornea 2006, 25, 1057–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres-Netto, E.A.; Randleman, J.B.; Hafezi, N.L.; Hafezi, F. Corneal stromal demarcation line after 4 protocols of corneal crosslinking in keratoconus determined with anterior segment optical coherence tomography. J. Cataract. Refract. Surg. 2006, 44, 1535. [Google Scholar] [CrossRef] [PubMed]
- Vinciguerra, R.; Tzamalis, A.; Romano, V.; Arbabi, E.M.; Batterbury, M.; Kaye, S.B. Assessment of the Association between In Vivo Corneal Biomechanical Changes after Corneal Cross-linking and Depth of Demarcation Line. J. Refract. Surg. 2019, 35, 202–206. [Google Scholar] [CrossRef]
- Hafezi, F.; Richoz, O.; Torres-Netto, E.A.; Hillen, M.; Hafezi, N.L. Corneal Cross-linking at the Slit Lamp. J. Refract. Surg. 2021, 37, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Dhaini, A.R.; Chokr, M.; El-Oud, S.M.; Fattah, M.A.; Awwad, S. Automated Detection and Measurement of Corneal Haze and Demarcation Line in Spectral-Domain Optical Coherence Tomography Images. IEEE Access 2018, 6, 3977–3991. [Google Scholar] [CrossRef]
- Dhaini, A.R.; Fattah, M.; El Oud, S.M.; Awwad, S. Automated Detection and Classification of Corneal Haze using Optical Coherence Tomography in Patients with Keratoconus after Cross-Linking. Cornea 2018, 37, 863–869. [Google Scholar] [CrossRef]
- Ng, A.L.; Chan, T.C.; Lai, J.S.; Cheng, A.C. Comparison of the Central and Peripheral Corneal Stromal Demarcation Line Depth in Conventional versus Accelerated Collagen Cross-Linking. Cornea 2015, 34, 1432–1436. [Google Scholar] [CrossRef]
- Pircher, N.; Lammer, J.; Holzer, S.; Gschliesser, A.; Donner, R.; Pieh, S.; Schmidinger, G. Correlation between central stromal demarcation line depth and changes in K values after corneal cross-linking (CXL). Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 759–764. [Google Scholar] [CrossRef]
- Toker, E.; Cerman, E.; Ozcan, D.O.; Seferoglu, O.B. Efficacy of different accelerated corneal crosslinking protocols for progressive keratoconus. J. Cataract. Refract. Surg. 2017, 43, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Kymionis, G.D.; Tsoulnaras, K.I.; Grentzelos, M.A.; Plaka, A.D.; Mikropoulos, D.G.; Liakopoulos, D.A.; Tsakalis, N.G.; Pallikaris, I.G. Corneal stroma demarcation line after standard and high-intensity collagen crosslinking determined with anterior segment optical coherence tomography. J. Cataract. Refract. Surg. 2014, 40, 736–740. [Google Scholar] [CrossRef]
- Spadea, L.; Di Genova, L.; Tonti, E. Corneal stromal demarcation line after 4 protocols of corneal crosslinking in keratoconus determined with anterior segment optical coherence tomography. J. Cataract. Refract. Surg. 2018, 44, 596–602. [Google Scholar] [CrossRef]
- Mazzotta, C.; Raiskup, F.; Hafezi, F.; Torres-Netto, E.A.; Balamoun, A.A.; Giannaccare, G.; Bagaglia, S.A. Long term results of accelerated 9 mW corneal crosslinking for early progressive keratoconus: The Siena Eye-Cross Study 2. Eye Vis. 2021, 8, 16. [Google Scholar] [CrossRef]
- Salmon, B.; Richoz, O.; Tabibian, D.; Kling, S.; Wuarin, R.; Hafezi, F. CXL at the Slit Lamp: No Clinically Relevant Changes in Corneal Riboflavin Distribution during Upright UV Irradiation. J. Refract. Surg. 2017, 33, 281. [Google Scholar] [CrossRef] [Green Version]
- Thorsrud, A.; Hagem, A.M.; Sandvik, G.F.; Drolsum, L. Superior outcome of corneal collagen cross-linking using riboflavin with methylcellulose than riboflavin with dextran as the main supplement. Acta Ophthalmol. 2019, 97, 415–421. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Parameter | Experimental Groups |
|---|---|
| Treatment target | Ectasia treatment |
| Fluence (total; J/cm²) | 5.4 |
| Soak Time (min) | 10 |
| Intensity (mW/cm²) | 9 |
| Treatment time (min) | 10 |
| Epithelium status | Off |
| Chromophore | 0.1% riboflavin (RiboKER, EMAGine AG) |
| Light source | C-eye |
| Irradiation mode | Continuous |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hafezi, F.; Lu, N.-J.; Assaf, J.F.; Hafezi, N.L.; Koppen, C.; Vinciguerra, R.; Vinciguerra, P.; Hillen, M.; Awwad, S.T. Demarcation Line Depth in Epithelium-Off Corneal Cross-Linking Performed at the Slit Lamp. J. Clin. Med. 2022, 11, 5873. https://doi.org/10.3390/jcm11195873
Hafezi F, Lu N-J, Assaf JF, Hafezi NL, Koppen C, Vinciguerra R, Vinciguerra P, Hillen M, Awwad ST. Demarcation Line Depth in Epithelium-Off Corneal Cross-Linking Performed at the Slit Lamp. Journal of Clinical Medicine. 2022; 11(19):5873. https://doi.org/10.3390/jcm11195873
Chicago/Turabian StyleHafezi, Farhad, Nan-Ji Lu, Jad F. Assaf, Nikki L. Hafezi, Carina Koppen, Riccardo Vinciguerra, Paolo Vinciguerra, Mark Hillen, and Shady T. Awwad. 2022. "Demarcation Line Depth in Epithelium-Off Corneal Cross-Linking Performed at the Slit Lamp" Journal of Clinical Medicine 11, no. 19: 5873. https://doi.org/10.3390/jcm11195873