
Clinical Characteristics of Actinic Keratosis Associated with the Risk of Progression to Invasive Squamous Cell Carcinoma: A Systematic Review
 , , and
, , and
Abstract
:1. Introduction
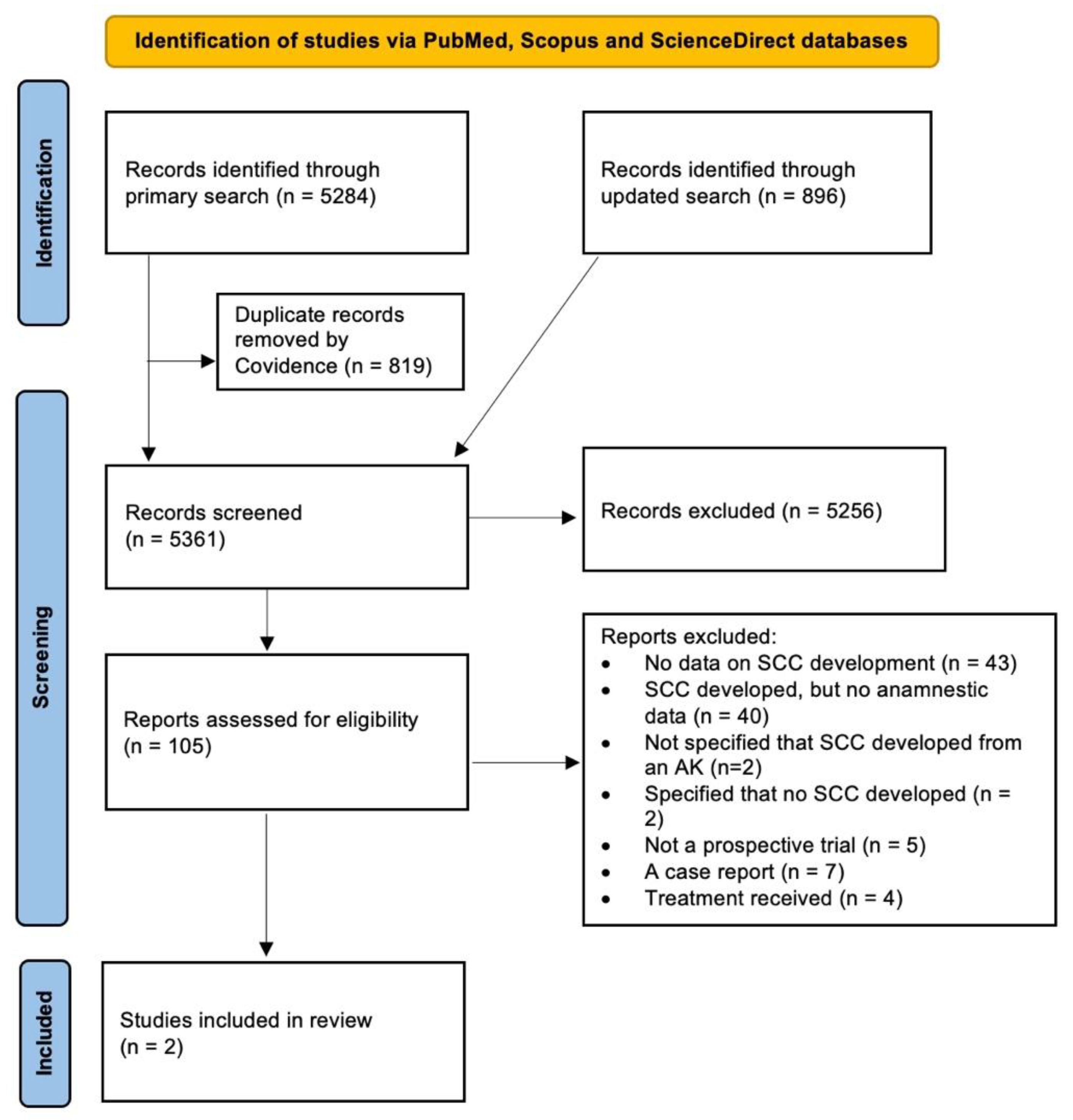
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dessinioti, C.; Stratigos, A.J. Overview of Guideline Recommendations for the Management of High-Risk and Advanced Cutaneous Squamous Cell Carcinoma. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Eisen, D.B.; Asgari, M.M.; Bennett, D.D.; Connolly, S.M.; Dellavalle, R.P.; Freeman, E.E.; Goldenberg, G.; Leffell, D.J.; Peschin, S.; Sligh, J.E.; et al. Guidelines of Care for the Management of Actinic Keratosis. J. Am. Acad. Derm. 2021, 85, e209–e233. [Google Scholar] [CrossRef] [PubMed]
- Grada, A.; Feldman, S.R.; Bragazzi, N.L.; Damiani, G. Patient-Reported Outcomes of Topical Therapies in Actinic Keratosis: A Systematic Review. Dermatol. Ther. 2021, 34, e14833. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Figueras, M.T.; Carrato, C.; Sáenz, X.; Puig, L.; Musulen, E.; Ferrándiz, C.; Ariza, A. Actinic Keratosis with Atypical Basal Cells (AK I) Is the Most Common Lesion Associated with Invasive Squamous Cell Carcinoma of the Skin. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Fernandez Figueras, M.T. From Actinic Keratosis to Squamous Cell Carcinoma: Pathophysiology Revisited. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 5–7. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, A.; Marmur, E. The Kinetics of Skin Cancer: Progression of Actinic Keratosis to Squamous Cell Carcinoma. Dermatol. Surg. 2007, 33, 1099–1101. [Google Scholar] [CrossRef]
- Ratushny, V.; Gober, M.D.; Hick, R.; Ridky, T.W.; Seykora, J.T. Review Series From Keratinocyte to Cancer: The Pathogenesis and Modeling of Cutaneous Squamous Cell Carcinoma. J. Clin. Investig. 2012, 122, 464–472. [Google Scholar] [CrossRef] [Green Version]
- Stockfleth, E.; Zwingers, T.; Willers, C. Recurrence Rates and Patient Assessed Outcomes of 0.5% 5-Fluorouracil in Combination with Salicylic Acid Treating Actinic Keratoses. Eur. J. Dermatol. 2012, 22, 370–374. [Google Scholar] [CrossRef]
- Stratigos, A.J.; Garbe, C.; Dessinioti, C.; Lebbe, C.; Bataille, V.; Bastholt, L.; Dreno, B.; Concetta Fargnoli, M.; Forsea, A.M.; Frenard, C.; et al. European Interdisciplinary Guideline on Invasive Squamous Cell Carcinoma of the Skin: Part 2. Treatment. Eur. J. Cancer 2020, 128, 83–102. [Google Scholar] [CrossRef] [Green Version]
- Quaedvlieg, P.J.F.; Tirsi, E.; Thissen, M.R.T.M.; Krekels, G.A. Actinic Keratosis: How to Differentiate the Good from the Bad Ones? Eur. J. Dermatol. 2006, 16, 335–339. [Google Scholar]
- Balcere, A.; Konrāde Jilmaza, L.; Rone Kupfere, M.; Čēma, I.; Krūmiņa, A. Which Actinic Keratosis Will Progress to Invasive Squamous Cell Carcinoma? A Systematic Review. PROSPERO 2020, 2020, CRD42020200429. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Criscione, V.D.; Weinstock, M.A.; Naylor, M.F.; Luque, C.; Eide, M.J.; Bingham, S.F. Actinic Keratoses: Natural History and Risk of Malignant Transformation in the Veterans Affairs Topical Tretinoin Chemoprevention Trial. Cancer 2009, 115, 2523–2530. [Google Scholar] [CrossRef] [PubMed]
- Wallingford, S.C.; Russell, S.A.; Vail, A.; Proby, C.M.; Lear, J.T.; Green, A.C. Actinic Keratoses, Actinic Field Change and Associations with Squamous Cell Carcinoma in Renal Transplant Recipients in Manchester, UK. Acta Derm. Venereol. 2015, 95, 830–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harwood, C.A.; Mesher, D.; McGregor, J.M.; Mitchell, L.; Leedham-Green, M.; Raftery, M.; Cerio, R.; Leigh, I.M.; Sasieni, P.; Proby, C.M. A Surveillance Model for Skin Cancer in Organ Transplant Recipients: A 22-Year Prospective Study in an Ethnically Diverse Population. Am. J. Transplant. 2013, 13, 119–129. [Google Scholar] [CrossRef]
- Jiyad, Z.; O’Rourke, P.; Soyer, H.P.; Green, A.C. Clinical Comparison of Actinic Changes Preceding Squamous Cell Carcinoma vs. Intraepidermal Carcinoma in Renal Transplant Recipients. Clin. Exp. Derm. 2017, 42, 895–897. [Google Scholar] [CrossRef]
- Jiyad, Z.; O’Rourke, P.; Soyer, H.P.; Green, A.C. Actinic Keratosis-Related Signs Predictive of Squamous Cell Carcinoma in Renal Transplant Recipients: A Nested Case–Control Study. Br. J. Dermatol. 2017, 176, 965–970. [Google Scholar] [CrossRef] [Green Version]
- Lang, P.G.; Braun, M.A.; Kwatra, R. Aggressive Squamous Carcinomas of the Scalp. Dermatol. Surg. 2006, 32, 1163–1170. [Google Scholar]
- Reinehr, C.P.H.; Bakos, R.M. Actinic Keratoses: Review of Clinical, Dermoscopic, and Therapeutic Aspects. Bras. Derm. 2019, 94, 637–657. [Google Scholar] [CrossRef]
- Suchniak, J.M.; Baer, S.; Goldberg, L.H. High Rate of Malignant Transformation in Hyperkeratotic Actinic Keratoses. J. Am. Acad. Derm. 1997, 37, 392–394. [Google Scholar] [CrossRef]
- Schmitz, L.; Kahl, P.; Majores, M.; Bierhoff, E.; Stockfleth, E.; Dirschka, T. Actinic Keratosis: Correlation between Clinical and Histological Classification Systems. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1303–1307. [Google Scholar] [CrossRef] [PubMed]
- Bridges, M.N.; Doval, M. Cutaneous Squamous Cell Carcinoma of the External Auditory Canal. Derm. Online J. 2009, 15, 13. [Google Scholar] [CrossRef]
- Jung, J.H.; Jeon, Y.R.; Kim, H.I.; Lee, M.K.; Chung, S. Verrucous Carcinoma Arising from Actinic Keratosis: A Case Report. Arch. Craniofac. Surg. 2021, 22, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Yamazato, S.; Nakai, N.; Katoh, N. A Case of Cutaneous Squamous Cell Carcinoma Arising in an Actinic Keratosis on the Face in a Centenarian Woman Successfully Treated with Surgery. Indian J. Derm. 2014, 59, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Ruini, C.; Witkowski, A.M.; Cesinaro, A.; Teixeira De Carvalho, N.; Pellacani, G. From Actinic Keratosis to Squamous Cell Carcinoma: Evidence of Morphologic and Biologic Progression. J. Am. Acad. Derm. 2015, 72, S8–S10. [Google Scholar] [CrossRef]
- Tokuriki, A.; Kiyohara, T.; Kouraba, S.; Kumakiri, M. Spindle Cell Squamous Cell Carcinoma Not Expressing Stratified but Simple Epithelial Cytokeratin: Efficacy of Simple Epithelial Cytokeratin Immunoreactivity. J. Dermatol. 2012, 39, 72–75. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balcere, A.; Konrāde-Jilmaza, L.; Pauliņa, L.A.; Čēma, I.; Krūmiņa, A. Clinical Characteristics of Actinic Keratosis Associated with the Risk of Progression to Invasive Squamous Cell Carcinoma: A Systematic Review. J. Clin. Med. 2022, 11, 5899. https://doi.org/10.3390/jcm11195899
Balcere A, Konrāde-Jilmaza L, Pauliņa LA, Čēma I, Krūmiņa A. Clinical Characteristics of Actinic Keratosis Associated with the Risk of Progression to Invasive Squamous Cell Carcinoma: A Systematic Review. Journal of Clinical Medicine. 2022; 11(19):5899. https://doi.org/10.3390/jcm11195899
Chicago/Turabian StyleBalcere, Alise, Laura Konrāde-Jilmaza, Laura Agnese Pauliņa, Ingrīda Čēma, and Angelika Krūmiņa. 2022. "Clinical Characteristics of Actinic Keratosis Associated with the Risk of Progression to Invasive Squamous Cell Carcinoma: A Systematic Review" Journal of Clinical Medicine 11, no. 19: 5899. https://doi.org/10.3390/jcm11195899