Abstract
Dehydroepiandrosterone (DHEA) is an adrenal steroid converted to potent androgens. This study aimed to discover the association between serum DHEA levels and immunologic response in people with HIV/AIDS (PLWHA). We enrolled patients aged ≥ 18 years who were treated with combination antiretroviral therapy (cART). We measured CD4+ and CD8+ T-cell counts, HIV-RNA titres, and serum DHEA levels. We assigned each patient to a good- or poor-responder group depending on their CD4+ T-cell counts at study enrolment. Participants with CD4+ T-cell counts > 200/µL were assigned to the good-responder group, whilst those with CD4+ T-cell counts < 200/µL were assigned to the poor-responder group. The participants were followed up for 2 years. The poor-responder group showed lower CD4+ T-cell counts and higher HIV PCR titres at their initial HIV diagnosis and in their 2-year follow-up data. Serum DHEA level was lower in the poor-responder group. Multivariable logistic analysis showed that BMI, initial CD4+ T-cell counts, and serum DHEA level were clinical factors associated with poor immunologic responsiveness to cART in PLWHA. Therefore, DHEA may be used as an indicator of the immunological recovery of PLWHA.
1. Introduction
Advances in combination antiretroviral therapy (cART) have enhanced the therapeutic success and prognosis of people with HIV/AIDS (PLWHA). The morbidity and mortality of PLWHA are significantly reduced, making their life expectancy comparable to that of the average population [1]. However, even with appropriate treatment with cART, some PLWHA fail to recover their CD4+ T-cell counts. Despite successful virologic suppression, approximately 15–18% of patients fail to achieve immune recovery, and such patients are referred to as “immune non-responders” or patients with “immune–virologic discordance” [1,2].
The important predisposing factors to poor response to cART are baseline immunosuppression levels and old age [3]. An initial CD4+ T-cell count < 200 is associated with blunted CD4+ T-cell recovery [4,5]. Previous studies have attempted to find supplements, such as zinc or vitamin D, to enhance the immunologic response and prognosis of PLWHA [6,7].
Dehydroepiandrosterone (DHEA) is a naturally occurring steroid mainly produced by the adrenal glands and is converted into potent androgens [8]. Previous studies have indicated that DHEA may have immunomodulatory properties by regulating the cytokine and complement cascades of inflammatory pathways [9]. Preliminary results showed that DHEA might act as an inhibitor of HIV replication [10]. This study hypothesises that serum DHEA is reduced in the poor-immune-responder group compared to PLWHA who successfully recovered CD4+ T-cell counts with cART. We performed a comparative analysis by dividing the good and poor responders and analysed the serum DHEA levels and other clinical factors associated with immune responsiveness.
2. Materials and Methods
2.1. Study Population
All participants were Koreans with HIV infection and were treated with cART at Severance Hospital (Seoul, Korea), a 2000-bed tertiary teaching hospital with an HIV research institution. We prospectively enrolled HIV-infected patients aged ≥ 18 years who were currently receiving cART. Written informed consent was obtained from all the participants. PLWHA without written consent were excluded from the study. From October 2016 to November 2019, serum blood samples were collected from each participant during their regular HIV clinic visits. This study was approved by the institutional review board of Severance Hospital (4-2016-0596).
2.2. Study Design and Definitions
CD4+ and CD8+ T-cell counts and HIV-RNA titres were collected at enrolment and on follow-up visits two years after enrolment in the study. Serum DHEA levels were measured once, at the study enrolment. The data of the initial HIV profile, including CD4+ and CD8+ T-cell counts and HIV-RNA titre at first diagnosis of HIV, were collected by reviewing electronic medical records. According to their CD4+ T-cell counts at the enrolment, the participants were assigned to good- and poor-responder groups. Since PLWHA with CD4+ T-cell counts below 200 have a higher chance of acquiring opportunistic infections, we assigned patients to the good-responder group who showed CD4+ T-cell counts above 200/mm3 whilst assigning participants with CD4+ T-cell counts below 200/mm3 in the poor-responder group [11]. There is no consensus on an acceptable CD4+ T-cell count recovery range for those on cART [12]. The good- and poor-responder groups were compared using various clinical factors, such as baseline characteristics of patients, underlying medical conditions, and HIV-related profiles such as CD4+ and CD8+ T-cell counts and HIV-RNA viral titres.
2.3. Measurement of Plasma DHEA
Each 0.5 cc blood sample was collected in an EDTA tube, centrifuged, and stored at −70 °C until testing. Serum DHEA levels were measured using an enzyme-linked immunosorbent assay (ELISA) kit (LDN GmbH & Co., KG, Nordhorn, Germany). Readings were measured using an ELISA plate reader SpectraMax190 (Molecular Devices, Sunnyvale, CA, USA) at Seoul Clinical Laboratories, Yongin, Korea.
2.4. Data Collection
Information on age, sex, weight, waist circumference, body mass index (BMI), underlying medical conditions, type of cART administered at study enrolment, CD4+ and CD8+ T-cell counts, HIV-RNA titres, date of HIV diagnosis, and date of cART initiation were obtained from electronic medical records and laboratory results.
2.5. Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Sciences ver. 26 (SPSS, Chicago, IL, USA). Statistical significance was set at p < 0.05. All values are expressed as the mean ± standard deviation or median with 25% and 75% values, respectively. Univariate and multivariate logistic regression analyses were performed to evaluate the clinical factors associated with responsiveness to HIV treatment. The receiver operating characteristic (ROC) curve was used to assess DHEA as a predictive marker for a poor immunological response. We used the Youden index to analyse the specific cut-off point of the serum DHEA level to predict poor clinical outcomes. The Biostatics Collaboration Unit of Yonsei University College of Medicine reviewed and certified statistical analysis and data of the study.
3. Results
A total of 198 participants were enrolled in this study. Thirty-five patients were excluded from the analysis due to follow-up loss or due to their missing initial HIV profile at first diagnosis (Figure 1).
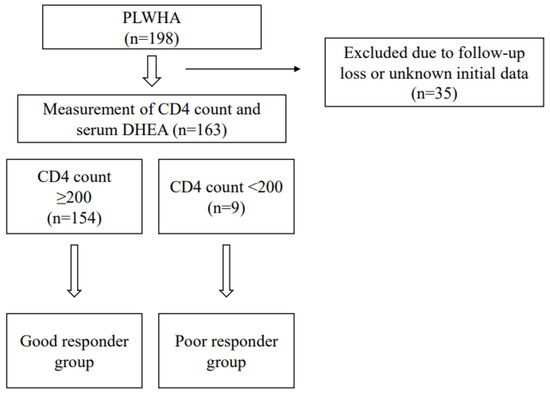
Figure 1.
Study flow. PLWHA: people living with HIV/AIDS.
Table 1 shows the baseline characteristics of the participants. The average age of the participants was 44.1 years, and 155 (95.1%) were men. The number of participants assigned to the good- and poor-responder groups was 154 and 9, respectively.

Table 1.
Baseline Characteristics of the Study Population.
Table 2 compares the differences between the two groups. The poor-responder group had a lower BMI, weight, and waist circumference than the good-responder group. Additionally, the poor-responder group showed lower initial CD4+ T-cell count (282.7 vs. 92.4/µL, p = 0.001) and CD8+ T-cell count (966.7 vs. 497.3/µL, p = 0.025) and higher initial log10 HIV-RNA titre (4.7 vs. 5.6 copies/mm3, p = 0.001) at the first HIV diagnosis. At the two-year follow-up after study enrolment, the HIV profile remained similar to the initial HIV profile at diagnosis. The poor-responder group had a lower CD4+ T-cell count (726.6 vs. 187.4/µL, p < 0.0001) and CD8+ T-cell count (821.4 vs. 569.0/µL, p = 0.034) than the good-responder group. None of the poor responders had underlying chronic medical conditions such as diabetes mellitus, hypertension, chronic kidney disease, dyslipidaemia, or fatty liver. Whilst the good-responder group showed a fully suppressed HIV-RNA titre, the poor-responder group showed an elevated HIV-RNA titre compared to the good-responder group. Serum DHEA levels were lower in the poor-responder group than in the good-responder group (4.3 vs. 2.9 ng/mL, p = 0.013). Both groups showed no significant differences in the duration or treatment of HIV infection. The poor-responder group had a shorter time from diagnosis to treatment (488.6 vs. 83.2 days, p = 0.006).
Table 2.
Comparison of the good and poor responders.
Table 3 compares antiretroviral regimens of the good and poor responders. The poor-responder group tended to take the cART regimen with a greater number of different classes (3.1 vs. 3.0, p < 0.001), while a higher percentage of poor-responder participants added protease inhibitors in the regimen than the good-responder group (21.4% vs. 55.6%, p = 0.033).
Table 3.
Comparison of Antiretroviral Therapy in the Good and Poor Responders.
The clinical characteristics of the poor responders are listed in Table 4 to provide individual information for the poor responders. All of the patients received a cART regimen including integrase inhibitor with or without protease inhibitor.
Table 4.
Characteristics of the Poor Responders.
Univariable and multivariable logistic regression analyses were performed to analyse the clinical factors associated with poor immunologic response to cART. The univariable logistic regression results in Table 5 demonstrate that factors such as BMI, weight, and waist circumference, which indicate the severity of HIV-related cachexia, are associated with poor immunologic response. The initial CD4+ T-cell count, initial CD8+ T-cell count, and serum DHEA level were also associated with poor immunological responses. In the multivariable analysis, BMI, initial CD4+ T-cell counts, and serum DHEA remained significant clinical factors associated with poor immunological responsiveness.
Table 5.
Factors associated with CD4+ T-cell count in PLWHA on cART.
To assess the usefulness of serum DHEA levels in predicting an immunologic recovery in PLWHA receiving cART, the ROC curve is displayed in Figure 2. The area under the ROC curve was 0.079 (95% CI = 0.593–0.901, p = 0.013). According to the Youden index of the ROC curve, a serum DHEA level of 4.19 ng/mL is the cut-off value for predicting a poor immune recovery in response to cART.
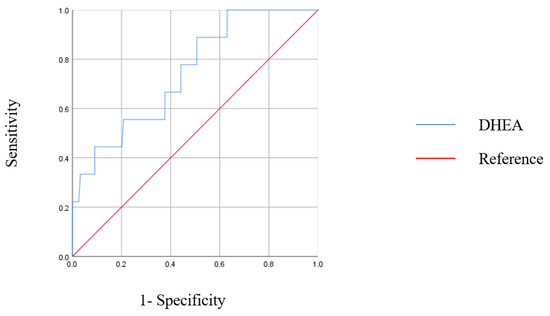
Figure 2.
Receiver operating characteristic (ROC) curve for DHEA level in predicting poor immunologic responsiveness. The area under the ROC curve for DHEA was 0.079 (95% CI 0.593–0.901, p = 0.013).
4. Discussion
A low initial CD4+ T-cell count and high viraemia are well-known factors related to the poor prognosis of HIV treatment [13,14]. Our study results also confirm that the poor responders had a low baseline CD4+ T-cell count and higher HIV-RNA viraemia state compared to the good responders at HIV diagnosis. Poor responders also presented lower body-mass index, weight, and waist circumference, which supports the previous notion that cachexia is also an important poor prognostic factor in PLWHA [15,16]. Interestingly, the poor responders did not have any chronic medical conditions, but this may be due to the small sample size of a relatively young group (average age 44.9).
Treatment with cART protects numerous PLWHA from progressing to terminal AIDS and reduces the risk of opportunistic infections by improving immune function [13]. However, some PLWHA experienced treatment failure, showing no CD4+ T-cell count recovery even with appropriate treatment with cART and achievement of full viral suppression, also referred to as “immune–virologic discordance” or in many other similar terms by previous research journals [17]. CD4+ T-cell count recovery is essential for the immune function of PLWHA, which is related to the risk of acquiring opportunistic infections and mortality. The previously known risk factors for immune–virologic discordance are low CD4+ T-cell count and high HIV-RNA at diagnosis of HIV, which are indicators of poor treatment response to cART. Among the nine participants who displayed CD4+ T-cell counts below 200/µL, only three participants were able to recover higher CD4+ T-cell counts at the two-year follow-up.
Many adjunctive therapies have been proposed to improve the immune–virologic discordance of PLWHA, and oral DHEA replacement is one of the suggested therapies [10]. We evaluated the significance of serum DHEA level in PLWHA with poor immune recovery to assess the possibility of the replacement of DHEA as a supplemental method to enhance CD4+ T-cell count as an adjunctive to cART.
DHEA was first isolated from humans in 1954 [18]. The adrenal cortex is the main organ responsible for DHEA production, but the testes and ovaries also produce DHEA [18,19,20]. Serum DHEA levels are decreased in older patients and those with advanced stages of HIV infection [21,22,23]. Randomised controlled trials have been conducted to improve sexual function, well-being sensation, bone mass density, and cognitive performance by replacing DHEA orally [24]. In a placebo–controlled trial by Rabkin et al., the DHEA replacement was proven useful in treating non-major but persistent depression in PLWHA [25]. Piketty et al. performed a double-blind placebo–controlled trial of oral DHEA (50 mg/day for four months) in patients with advanced HIV stage between June 1995 and November 1996 [26]. The study results confirmed the improvement in physiological and psychological well-being but were unable to show improvements in CD4+ T-cell counts. Additionally, there is an expert opinion that using a higher dose of DHEA (300–600 mg twice daily) may be necessary to improve CD4+ T-cell counts [27].
Currently, there are no guidelines for replacing DHEA with PLWHA. According to our results, oral replacement of DHEA may be considered for patients who satisfy both of the following criteria: (1) serum DHEA level < 4.19 ng/mL and (2) no recovery of CD4+ T-cell count > 200/mm3 after treatment with appropriate cART without drug resistance or compliance issues. Since the normal range of DHEA varies according to age and sex, subgroup analysis should be performed in the future to verify the appropriate cut-off serum DHEA values for different age and sex groups. In our study, groups of people displayed low serum DHEA levels but showed good immunologic recovery of CD4+ T-cell counts. Therefore, this finding suggests that low serum DHEA level is not an absolute indication of DHEA replacement.
Furthermore, serum DHEA level can predict poor immune recovery in PLWHA patients treated with cART. Our journal is the first to use serum DHEA level as a tool to assess therapeutic outcomes. According to the ROC curve, serum DHEA level can be used to predict unfavourable responses to immune recovery. As optimal serum DHEA level varies by age and sex, such clinical factors should be considered when assessing PLWHA for DHEA replacement.
The limitation of this study is in the small sample size of the poor responders and the absence of clinical results for oral replacement of DHEA. A prospective, case–controlled study comparing the effects of DHEA replacement will help assess the clinical usefulness of DHEA replacement in the poor-responder group.
Thus far, the previous studies did not report any major side effects due to replacement of DHEA for various purposes [28]. Therefore, therapeutic replacement of DHEA can be incorporated into augmentation of immunologic function in PLWHA.
5. Conclusions
The serum DHEA level can be used to predict poor immunologic recovery in PLWHA treated with cART. Replacement of DHEA in poor responders might be a valuable treatment option for enhancing the immunologic function of PLWHA.
Author Contributions
Conceptualisation, S.J.J.; Methodology, S.J.J.; Software, E.H.L.; Validation, J.K., J.Y.A., N.S.K., S.J.L. and K.H.L.; Formal Analysis, E.H.L.; Investigation, S.J.J.; Resources, S.J.J.; Data Curation, S.J.J.; Writing—Original Draft Preparation, E.H.L.; Writing—Review and Editing, E.H.L.; Visualisation, E.H.L.; Supervision, J.H.K., J.Y.C. and J.-S.Y.; Project Administration, S.J.J.; Funding Acquisition, S.J.J. All authors have read and agreed to the published version of the manuscript.
Funding
Sponsorship for this study was funded by the Handok Inc., Seoul, Korea (HANDOK 2014-158). The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Severance Hospital (4-2016-0596) and followed the Helsinki Declaration (164, amended most recently in 2008) of the World Medical Association.
Informed Consent Statement
Informed consent was obtained from each patient.
Data Availability Statement
All data are available on request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Younes, S.A.; Talla, A.; Pereira Ribeiro, S.; Saidakova, E.V.; Korolevskaya, L.B.; Shmagel, K.V.; Shive, C.L.; Freeman, M.L.; Panigrahi, S.; Zweig, S.; et al. Cycling CD4+ T Cells in HIV-Infected Immune Nonresponders Have Mitochondrial Dysfunction. J. Clin. Investig. 2018, 128, 5083–5094. [Google Scholar] [CrossRef] [PubMed]
- Zoufaly, A.; Cozzi-Lepri, A.; Reekie, J.; Kirk, O.; Lundgren, J.; Reiss, P.; Jevtovic, D.; Machala, L.; Zangerle, R.; Mocroft, A.; et al. Immuno-Virological Discordance and the Risk of Non-AIDS and AIDS Events in a Large Observational Cohort of HIV-Patients in Europe. PLoS ONE 2014, 9, e87160. [Google Scholar] [CrossRef] [PubMed]
- Engsig, F.N.; Zangerle, R.; Katsarou, O.; Dabis, F.; Reiss, P.; Gill, J.; Porter, K.; Sabin, C.; Riordan, A.; Fätkenheuer, G.; et al. Long-Term Mortality in HIV-Positive Individuals Virally Suppressed for >3 Years With Incomplete CD4 Recovery. Clin. Infect. Dis. 2014, 58, 1312–1321. [Google Scholar] [CrossRef] [PubMed]
- Kelley, C.F.; Kitchen, C.M.R.; Hunt, P.W.; Rodriguez, B.; Hecht, F.M.; Kitahata, M.; Crane, H.M.; Willig, J.; Mugavero, M.; Saag, M.; et al. Incomplete Peripheral CD4+ Cell Count Restoration in HIV-Infected Patients Receiving Long-Term Antiretroviral Treatment. Clin. Infect. Dis. 2009, 48, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Robbins, G.K.; Spritzler, J.G.; Chan, E.S.; Asmuth, D.M.; Gandhi, R.T.; Rodriguez, B.A.; Skowron, G.; Skolnik, P.R.; Shafer, R.W.; Pollard, R.B.; et al. Incomplete Reconstitution of T Cell Subsets on Combination Antiretroviral Therapy in the AIDS Clinical Trials Group Protocol 384. Clin. Infect. Dis. 2009, 48, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.; Montes, C.G.; Canals, A.; Mackenna, M.J.; Wolff, M. Role and Effects of Zinc Supplementation in HIV-Infected Patients with Immunovirological Discordance: A Randomized, Double Blind, Case Control Study. PLoS ONE 2021, 16, e0244823. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, N.; Aguilar-Jimenez, W.; Rugeles, M.T. The Potential Protective Role of Vitamin D Supplementation on HIV-1 Infection. Front. Immunol. 2019, 10, 2291. [Google Scholar] [CrossRef] [PubMed]
- Van Vollenhoven, R.F. Dehydroepiandrosterone: Uses and Abuses. In Textbook of Rheumatology; Kelley, W.N., Harris, J., Ruddy, S., Sledge, C.B., Eds.; W. B. Saunders Co.: Philadelphia, PA, USA, 1997; pp. 1–25. [Google Scholar]
- Prall, S.P.; Muehlenbein, M.P. DHEA Modulates Immune Function: A Review of Evidence. Vitam. Horm. 2018, 108, 125–144. [Google Scholar]
- Abrams, D.I.; Shade, S.B.; Couey, P.; McCune, J.M.; Lo, J.; Bacchetti, P.; Chang, B.; Epling, L.; Liegler, T.; Grant, R.M. Dehydroepiandrosterone (DHEA) Effects on HIV Replication and Host Immunity: A Randomized Placebo-Controlled Study. AIDS Res. Hum. Retrovir. 2007, 23, 77–85. [Google Scholar] [CrossRef]
- Damtie, D.; Yismaw, G.; Woldeyohannes, D.; Anagaw, B. Common Opportunistic Infections and Their CD4 Cell Correlates Among HIV-Infected Patients Attending at Antiretroviral Therapy Clinic of Gondar University Hospital, Northwest Ethiopia. BMC. Res. Notes 2013, 6, 534. [Google Scholar] [CrossRef]
- Rb-Silva, R.; Goios, A.; Kelly, C.; Teixeira, P.; João, C.; Horta, A.; Correia-Neves, M. Definition of Immunological Nonresponse to Antireviral Therapy: A systemic Review. J. Acquir. Immune Defic. Syndr. 2019, 82, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Wolbers, M.; Bucher, H.C.; Furrer, H.; Rickenbach, M.; Cavassini, M.; Weber, R.; Schmid, P.; Bernasconi, E.; Hirschel, B.; Battegay, M.; et al. Delayed Diagnosis of HIV Infection and Late Initiation of Antiretroviral Therapy in the Swiss HIV Cohort Study. HIV Med. 2008, 9, 397–405. [Google Scholar] [CrossRef]
- Egger, M.; May, M.; Chêne, G.; Phillips, A.N.; Ledergerber, B.; Dabis, F.; Costagliola, D.; D’Arminio Monforte, A.; de Wolf, F.; Reiss, P.; et al. Prognosis of HIV-1-Infected Patients Starting Highly Active Antiretroviral Therapy: A Collaborative Analysis of Prospective Studies. Lancet 2002, 360, 119–129. [Google Scholar] [CrossRef]
- Hoffman, J.; van Griensven, J.; Colebunders, R.; McKellar, M. Role of the CD4 Count in HIV Management. HIV Ther. 2010, 4, 27–39. [Google Scholar] [CrossRef]
- Massanella, M.; Negredo, E.; Pérez-Alvarez, N.; Puig, J.; Ruiz-Hernández, R.; Bofill, M.; Clotet, B.; Blanco, J. CD4 T-Cell Hyperactivation and Susceptibility to Cell Death Determine Poor CD4 T-Cell Recovery During Suppressive HAART. AIDS 2010, 24, 959–968. [Google Scholar] [CrossRef]
- Von Roenn, J.H.; Armstrong, D.; Kotler, D.P.; Cohn, D.L.; Klimas, N.G.; Tchekmedyian, N.S.; Cone, L.; Brennan, P.J.; Weitzman, S.A. Megestrol Acetate in Patients With AIDS-Related Cachexia. Ann. Intern. Med. 1994, 121, 393–399. [Google Scholar] [CrossRef]
- Von Roenn, J.H.; Roth, E.L.; Craig, R. HIV-Related Cachexia: Potential Mechanisms and Treatment. Oncology 1992, 49 (Suppl. 2), 50–54. [Google Scholar] [CrossRef] [PubMed]
- Tan, R.; Westfall, A.O.; Willig, J.H.; Mugavero, M.J.; Saag, M.S.; Kaslow, R.A.; Kempf, M.C. Clinical Outcome of HIV-Infected Antiretroviral-Naive Patients With Discordant Immunologic and Virologic Responses to Highly Active Antiretroviral Therapy. J. Acquir. Immune Defic. Syndr. 2008, 47, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Migeon, C.J.; Plager, J.E. Identification and Isolation of Dehydroisoandrosterone from Peripheral Human Plasma. J. Biol. Chem. 1954, 209, 767–772. [Google Scholar] [CrossRef]
- Hall, P.F.; Sozer, C.C.; Eik-Nes, K.B. Formation of Dehydroepiandrosterone during In Vivo and In Vitro Biosynthesis of Testosterone by Testicular Tissue. Endocrinology 1964, 74, 35–43. [Google Scholar] [CrossRef]
- Aakvaag, A.; Hagen, A.A.; Eik-Nes, K.B. Biosynthesis In Vivo of Testosterone and Δ4-Androstenedione From Dehydroepiandrosterone-Sodium Sulfate by the Canine Testis and Ovary. Biochim. Biophys. Acta (BBA) Gen. Subj. 1964, 86, 622–627. [Google Scholar] [CrossRef]
- Christeff, N.; Gherbi, N.; Mammes, O.; Dalle, M.T.; Gharakhanian, S.; Lortholary, O.; Melchior, J.C.; Nunez, E.A. Serum Cortisol and DHEA Concentrations During HIV Infection. Psychoneuroendocrinology 1997, 22 (Suppl. 1), S11–S18. [Google Scholar] [CrossRef]
- Simpson, E.R.; Davis, S.R. Minireview: Aromatase and the Regulation of Estrogen Biosynthesis—Some New Perspectives. Endocrinology 2001, 142, 4589–4594. [Google Scholar] [CrossRef]
- Rabkin, J.G.; McElhiney, M.C.; Rabkin, R.; McGrath, P.J.; Ferrando, S.J. Placebo-Controlled Trial of Dehydroepiandrosterone (DHEA) for Treatment of Nonmajor Depression in Patients with HIV/AIDS. Am. J. Psychiatry 2006, 163, 59–66. [Google Scholar] [CrossRef]
- Piketty, C.; Jayle, D.; Leplege, A.; Castiel, P.; Ecosse, E.; Gonzalez-Canali, G.; Sabatier, B.; Boulle, N.; Debuire, B.; Le Bouc, Y.; et al. Double-Blind Placebo-Controlled Trial of Oral Dehydroepiandrosterone in Patients With Advanced HIV Disease. Clin. Endocrinol. (Oxf.) 2001, 55, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Hasheeve, D.; Salvato, P.; Thompson, C. DHEA: A Potential Treatment for HIV Disease. In Proceedings of the International Conference on AIDS, Yokohama, Japan, 7–12 August 1994; Volume 10, p. 223. [Google Scholar]
- Wang, F.; He, Y.; Santos, H.O.; Sathian, B.; Price, J.C.; Diao, J. The effects of dehydroepiandrosterone (DHEA) supplementation on body composition and blood pressure: A meta-analysis of randomized clinical trials. Steroids 2020, 163, 108710. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).