


Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction and Quality Assessment
2.5. Synthesis of Results
3. Results
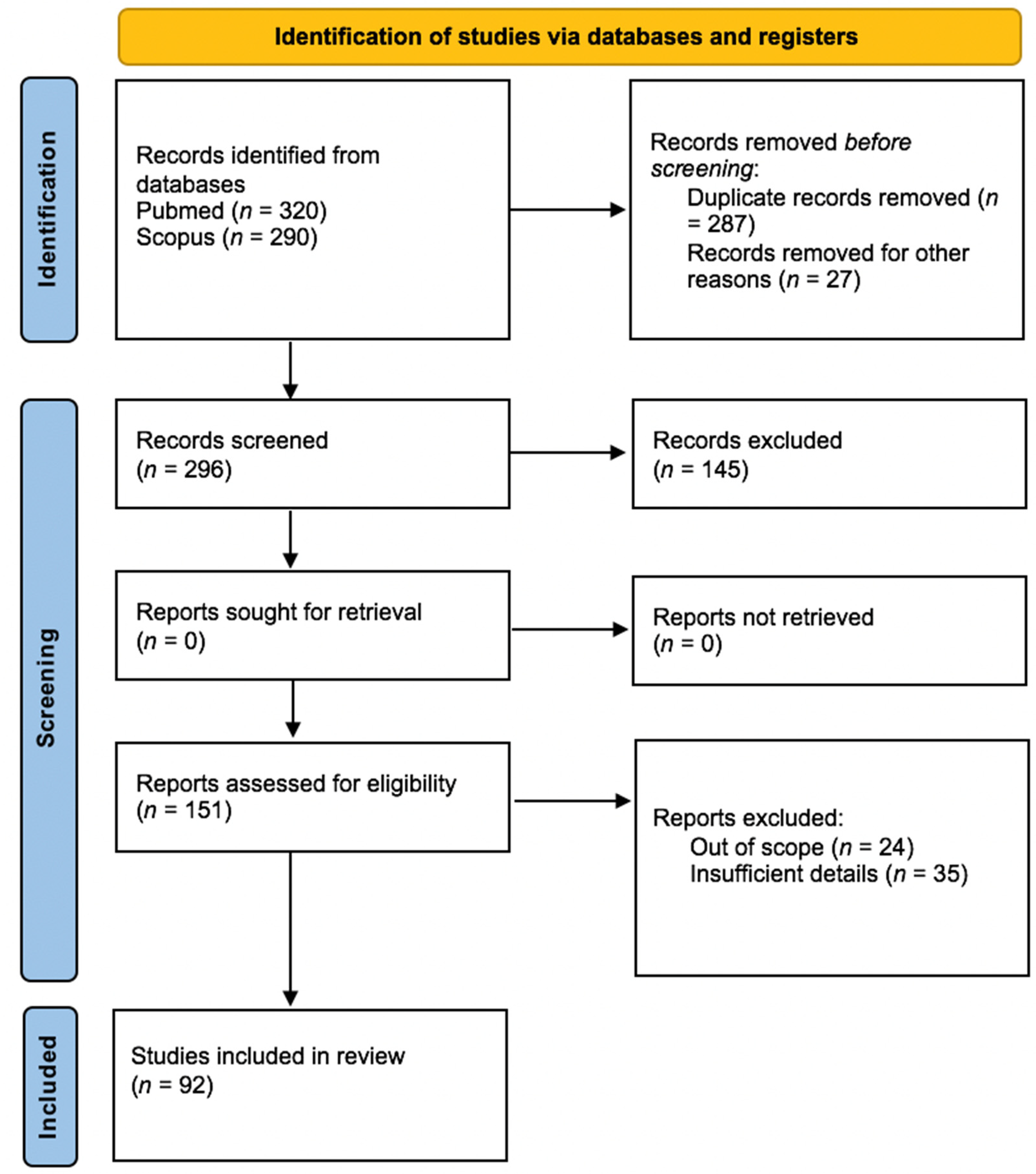
3.1. Study Selection
3.2. Study Characteristics and Results of Data Synthesis
3.3. Clinical Manifestations
3.4. Histopathological Findings
3.5. Treatment Regimens
- 1.
- Irritant removal
- 2.
- Topical and systemic corticosteroids
- 3.
- Topical and systemic immunosuppressants/immunomodulators
- 4.
- Surgery and similar treatments
- 5.
- Radiotherapy
- 6.
- Other therapies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antonelli, A.; Averta, F.; Diodati, F.; Muraca, D.; Brancaccio, Y.; Mignogna, C.; Giudice, A. An Uncommon Case of Plasma Cell Mucositis of the Tongue in a Young Man. Case Rep. Dent. 2020, 2020, 3429632. [Google Scholar] [CrossRef] [PubMed]
- Zoon, J.J. Balanoposthite chronique circonscrite bénigne à plasmocytes [Chronic benign circumscript plasmocytic balanoposthitis]. Dermatologica 1952, 105, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tailor, A.; Pemberton, M.N.; Murphy, R.; Hegarty, A.M. Plasma cell mucositis related to qat chewing: A report of 2 cases and review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, e65–e70. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.R.; Gupta, R.; Saran, R.K.; Krishnan, S. Plasma cell mucositis with gingival enlargement and severe periodontitis. J. Indian Soc. Periodontol. 2014, 18, 379–384. [Google Scholar] [CrossRef]
- Arun, K.; Ambooken, M.; Varghese, S.S.; Varghese, T.; Mathew, J.J. A rare case of plasma cell mucositis in a young patient. J. Indian Soc. Periodontol. 2017, 21, 63–65. [Google Scholar] [CrossRef]
- Shanahan, D.; Shipley, D.; Staines, K. Plasma Cell Mucositis. Ear Nose Throat J. 2020, 99, NP64–NP65. [Google Scholar] [CrossRef]
- Leuci, S.; Coppola, N.; Adamo, N.; Bizzoca, M.E.; Russo, D.; Spagnuolo, G.; Lo Muzio, L.; Mignogna, M.D. Clinico-Pathological Profile and Outcomes of 45 Cases of Plasma Cell Gingivitis. J. Clin. Med. 2021, 10, 830. [Google Scholar] [CrossRef]
- Galvin, S.; Bowe, C.; O Regan, E.M.; Conlon, N.; Flint, S.R.; Healy, C.M. Circumorificial plasmacytosis/plasma cell orificial mucositis: A case series and a review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, e77–e81. [Google Scholar] [CrossRef]
- Smith, M.E.; Crighton, A.J.; Chisholm, D.M.; Mountain, R.E. Plasma cell mucositis: A review and case report. J. Oral Pathol. Med. 1999, 28, 183–186. [Google Scholar] [CrossRef]
- Lightstone, A.C.; Cohen, H.J. Plasmocytic mucosal infiltrates in multiple myeloma. Arch. Dermatol. 1960, 82, 921–923. [Google Scholar] [CrossRef]
- Nosratzehi, T. Oral Lichen Planus: An Overview of Potential Risk Factors, Biomarkers and Treatments. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 1161–1167. [Google Scholar] [PubMed]
- Palmer, R.M.; Eveson, J.W. Plasma-cell gingivitis. Oral Surg. Oral Med. Oral Pathol. 1981, 51, 187–189. [Google Scholar] [CrossRef]
- White, J.W., Jr.; Olsen, K.D.; Banks, P.M. Plasma cell orificial mucositis. Report of a case and review of the literature. Arch. Dermatol. 1986, 122, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, K.H.; Hahm, J.E.; Ha, J.W.; Kwon, W.J.; Kim, C.W.; Kim, S.S. Plasma Cell Cheilitis: A Clinicopathological and Immunohistochemical Study of 13 Cases. Ann. Dermatol. 2017, 29, 536–542. [Google Scholar] [CrossRef]
- Senol, M.; Ozcan, A.; Aydin, N.E.; Hazneci, E.; Turan, N. Intertriginous plasmacytosis with plasmoacanthoma: Report of a typical case and review of the literature. Int. J. Dermatol. 2008, 47, 265–268. [Google Scholar] [CrossRef]
- Jayaraman, A.G.; Cesca, C.; Kohler, S. Cutaneous plasmacytosis: A report of five cases with immunohistochemical evaluation for HHV-8 expression. Am. J. Dermatopathol. 2006, 28, 93–98. [Google Scholar] [CrossRef]
- Silverman, S., Jr.; Lozada, F. An epilogue to plasma-cell gingivostomatitis (allergic gingivostamtitis). Oral Surg. Oral Med. Oral Pathol. 1977, 43, 211–217. [Google Scholar] [CrossRef]
- Kerr, D.A.; McClatchey, K.D.; Regezi, J.A. Allergic gingivostomatitis (due to gum chewing). J. Periodontol. 1971, 42, 709–712. [Google Scholar] [CrossRef]
- Grattan, C.E.; Gentle, T.A.; Basu, M.K. Oral papillary plasmacytosis resembling candidosis without demonstrable fungus in lesional tissue. Clin. Exp. Dermatol. 1992, 17, 112–116. [Google Scholar] [CrossRef]
- Marker, P.; Krogdahl, A. Plasma cell gingivitis apparently related to the use of khat: Report of a case. Br. Dent. J. 2002, 192, 311–313. [Google Scholar] [CrossRef]
- Kumar, V.; Tripathi, A.K.; Saimbi, C.S.; Sinha, J. Plasma cell gingivitis with severe alveolar bone loss. BMJ Case Rep. 2015, 2015, bcr2014207013. [Google Scholar] [CrossRef] [PubMed]
- Janam, P.; Nayar, B.R.; Mohan, R.; Suchitra, A. Plasma cell gingivitis associated with cheilitis: A diagnostic dilemma! J. Indian Soc. Periodontol. 2012, 16, 115–119. [Google Scholar] [PubMed]
- Saruya, K.; Fukuda, H.; Saito, R.; Urushibata, O.; Mukai, H. Plasmocytosis circumorificialis successfully treated with topical fusidic acid ointment. J. Dermatol. 2009, 36, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Bendtzen, K.; Diamant, M.; Faber, V. Fusidic acid, an immunosuppressive drug with functions similar to cyclosporin A. Cytokine 1990, 2, 423–429. [Google Scholar] [CrossRef]
- Baughman, R.D.; Berger, P.; Pringle, W.M. Plasma cell cheilitis. Arch. Dermatol. 1974, 110, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Moutsopoulos, N.M.; Konkel, J.E. Tissue-Specific Immunity at the Oral Mucosal Barrier. Trends Immunol. 2018, 39, 276–287. [Google Scholar] [CrossRef] [PubMed]
- Dutzan, N.; Konkel, J.E.; Greenwell-Wild, T.; Moutsopoulos, N.M. Characterization of the human immune cell network at the gingival barrier. Mucosal Immunol. 2016, 9, 1163–1172. [Google Scholar] [CrossRef]
- Vinay, K.; Abhijit, C.; Dogra, S. Unusual manifestation of mucosal plasmacytosis mimicking erythema multiforme. Dermatol. Online J. 2016, 22, 15. [Google Scholar] [CrossRef]
- Kaur, C.; Thami, G.P.; Sarkar, R.; Kanwar, A.J. Plasma cell mucositis. J. Eur. Acad. Dermatol. Venereol. JEADV 2001, 15, 566–567. [Google Scholar] [CrossRef]
- van de Kerkhof, P.C.; van Baar, H.M. Co-occurrence of plasma cell orificial mucositis and plasmoacanthoma. Report of a case and review of the literature. Dermatology 1995, 191, 53–55. [Google Scholar] [CrossRef]
- Timms, M.S.; Sloan, P.; Balzan, A.P. Idiopathic plasmacytosis of the oral and supraglottic mucosa. J. Laryngol. Otol. 1988, 102, 646–648. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, A.T.; Chandran, C.R.; Prabhakar, P.; Lakshmiganthan, M.; Parthasaradhi, T. Plasma cell gingivitis: Treatment with chlorpheniramine maleate. Int. J. Periodontics Restor. Dent. 2015, 35, 411–413. [Google Scholar] [CrossRef] [PubMed]
- Makkar, A.; Tewari, S.; Kishor, K.; Kataria, S. An unusual clinical presentation of plasma cell gingivitis related to “Acacia” containing herbal toothpaste. J. Indian Soc. Periodontol. 2013, 17, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Román, C.C.; Yuste, C.M.; González, M.A.; González, A.P.; López, G. Plasma cell gingivitis. Cutis 2002, 69, 41–45. [Google Scholar] [PubMed]
- Ahsanuddin, A.N.; Brynes, R.K.; Li, S. Peripheral blood polyclonal plasmacytosis mimicking plasma cell leukemia in patients with angioimmunoblastic T-cell lymphoma: Report of 3 cases and review of the literature. Int. J. Clin. Exp. Pathol. 2011, 4, 416–420. [Google Scholar]
- Błażewicz, I.; Barańska-Rybak, W.; Stawczyk-Macieja, M.; Petranyuk, A.; Nowicki, R. Plasma cell mucositis—A rare differential diagnosis for ulceration of oral mucosa. Dermatol. Rev. Przegląd Dermatol. 2015, 102, 520–523. [Google Scholar] [CrossRef]
- Tseng, J.T.; Cheng, C.J.; Lee, W.R.; Wang, K.H. Plasma-cell cheilitis: Successful treatment with intralesional injections of corticosteroids. Clin. Exp. Dermatol. 2009, 34, 174–177. [Google Scholar] [CrossRef]
- de Mendonça, R.M.; de Araújo, M.; Levy, C.E.; Morari, J.; Silva, R.A.; Yunes, J.A.; Brandalise, S.R. Prospective evaluation of HSV, Candida spp., and oral bacteria on the severity of oral mucositis in pediatric acute lymphoblastic leukemia. Support. Care Cancer 2012, 20, 1101–1107. [Google Scholar] [CrossRef]
- Osakabe, L.; Utsumi, A.; Saito, B.; Okamatsu, Y.; Kinouchi, H.; Nakamaki, T.; Hironaka, S. Influence of Oral Anaerobic Bacteria on Hematopoietic Stem Cell Transplantation Patients: Oral Mucositis and General Condition. Transplant. Proc. 2017, 49, 2176–2182. [Google Scholar] [CrossRef]
- Castillo, J.J. Plasma Cell Disorders. Prim. Care 2016, 43, 677–691. [Google Scholar] [CrossRef]
- Adamo, D.; Calabria, E.; Coppola, N.; Lo Muzio, L.; Giuliani, M.; Bizzoca, M.E.; Azzi, L.; Croveri, F.; Colella, G.; Boschetti, C.E.; et al. Psychological profile and unexpected pain in oral lichen planus: A case-control multicenter SIPMO study. Oral Dis. 2022, 28, 398–414. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Language | English | All other languages |
| Sample (S) | Patients affected by o-PCM | Patients who do not possess the inclusion criteria for this study |
| Phenomenon of interest (PI) | Histopathological features of o-PCM | |
| Design of study (D) | Case series, case reports, reviews, letter to editor | Opinion-based studies |
| Evaluation (E) | Clinical features, symptoms, histopathological characteristics, treatment of o-PCM | Studies that do not report even just a component between clinical, symptomatological, histopathological and/or DIF and/or immunohistochemical characteristics, therapy |
| Research type (R) | Qualitative, quantitative, and mixed-method studies | - |
| Frequency N (%) | |
|---|---|
| Chewing-gum | 18 (41.86%) |
| Toothpaste | 15 (34.88%)
|
| Khat | 7 (16.28%) |
| Foods | 4 (9.30%)
|
| Other | 1 (2.33%)
|
| Clinical Features | Palate N° (%) | Gingiva N° (%) | Tongue N° (%) | Buccal Mucosa N° (%) | Lip N° (%) | Oropharynx N° (%) | Larynx N° (%) | Floor of the Mouth N° (%) | Total Patients N° (%) |
|---|---|---|---|---|---|---|---|---|---|
| Erythema | 11 (7.01) | 79 (50.32) | 20 (12.74) | 15 (9.55) | 23 (14.65) | 5 (3.19) | 3 (1.91) | 1 (0.64) | 157 (99.37) |
| Swelling | 21 (42) | 2 (4) | 1 (2) | 25 (50) | 1 (2) | 50 (31.65) | |||
| Edema | 3 (6.12) | 38 (77.55) | 1 (20.04) | 2 (4.08) | 1 (2.04) | 4 (8.16) | 49 (31.01) | ||
| Erosion | 2 (5.13) | 2 (5.13) | 2 (5.13) | 5 (12.82) | 27 (69.23) | 1 (2.56) | 39 (24.68) | ||
| Ulceration | 2 (5.88) | 6 (17.65) | 3 (8.82) | 7 (20.59) | 15 (44.12) | 1 (2.94) | 34 (21.52) | ||
| Angular cheilitis | 30 (18.99) | ||||||||
| Secondary impetigo | 20 (100) | 20 (12.66) | |||||||
| Gingival hypertrophy | 17 (10.76) | ||||||||
| Fissuration | 7 (41.18) | 10 (58.82) | 17 (10.76) | ||||||
| Erythematous plaques | 1 (8.33) | 1 (8.33) | 1 (8.33) | 8 (66.67) | 1 (8.33) | 12 (7.60) | |||
| Bone loss | 11 (6.96) | ||||||||
| Pseudo-pockets | 11 (6.96) | ||||||||
| Desquamative gingivitis | 7 (4.43) | ||||||||
| Cobblestone appearance | 3 (42.86) | 1 (14.29) | 2 (28.57) | 1 (14.29) | 7 (4.43) | ||||
| Warty lesion | 1 (16.67) | 1 (16.67) | 1 (16.67) | 3 (50) | 6 (3.80) | ||||
| Keratotic plaques | 5 (100) | 5 (3.16) | |||||||
| Hyperplasia | 4 (80) | 1 (20) | 5 (3.16) | ||||||
| Papillary hyperplasia | 3 (60) | 2 (40) | 5 (3.16) | ||||||
| Tongue Atrophy | 2 (1.27) | ||||||||
| Exophytic sessile lesion | 1 (100) | 1 (0.63) | |||||||
| Exophytic pedunculated lesion | 1 (100) | 1 (0.63) | |||||||
| Small pink papules | 1 (100) | 1 (0.63) |
| Histopatological Features | Frequency N (%) |
|---|---|
| Sub-epithelial features | |
| Dense plasma cell-rich infiltrate | 158 (100) |
| Lymphocytes | 29 (18.35) |
| Dilated capillaries | 21 (13.29) |
| Neutrophils | 16 (10.13) |
| Eosinophils | 15 (9.49) |
| IgG | 10 (6.33) |
| Mast cells | 9 (5.70) |
| Russel bodies | 9 (5.70) |
| Micro-abscess | 8 (5.06) |
| Macrophages | 4 (2.53) |
| Fibrosis | 1 (0.63) |
| Epithelial features | |
| Epithelial hyperplasia * | 42 (26.58) |
| Parakeratosis | 22 (13.92) |
| Edema | 20 (12.66) |
| Acanthosis | 19 (12.02) |
| Atrophy | 12 (7.60) |
| Spongiosis | 11 (6.96) |
| Exocytosis | 10 (6.33) |
| Elongated rete pegs | 10 (6.33) |
| Vacuolar degeneration | 8 (5.06) |
| Acantholysis | 1 (0.63) |
| Efficacy (N) | Efficacy in Association with Other Therapy (N) | Partial or Null Effect (N) | Total | |
|---|---|---|---|---|
| Corticosteroids | ||||
| Prednisone | 9 | 3 | 3 | 15 |
| Triamcinolone Acetonide | 8 | 3 | 7 | 18 |
| Prednisolone | 4 | 4 | 8 | 16 |
| Betametasone | 4 | 1 | 4 | 9 |
| Clobetasol | 6 | 0 | 2 | 8 |
| Fluocinolone | 1 | 1 | 5 | 7 |
| Methylprednisolone | 1 | 0 | 7 | 8 |
| Hydrocortisone | 0 | 0 | 3 | 3 |
| Unspecified | 0 | 7 | 24 | 31 |
| Total | 33 (28.70%) | 19 (16.52%) | 63 (54.78%) | |
| Immunosuppressants/Immunomodulators | ||||
| Tacrolimus | 8 | 5 | 12 | 25 |
| Pimecrolimus | 1 | 0 | 2 | 3 |
| Mycophenolate Mofetil | 0 | 1 | 2 | 3 |
| Methotrexate | 0 | 0 | 2 | 2 |
| Colchicine | 0 | 0 | 2 | 2 |
| Azathioprine | 0 | 0 | 2 | 2 |
| Cyclosporine | 1 | 0 | 0 | 1 |
| Levamisolone | 0 | 2 | 0 | 2 |
| Etretinato | 0 | 0 | 1 | 1 |
| Hydroxychloroquine | 0 | 0 | 1 | 1 |
| Total | 10 (23.81%) | 8 (19.05%) | 24 (57.14%) | |
| Surgery and similar treatments | ||||
| Traditional surgery | 9 | 5 | 6 | 20 |
| Laser surgery | 2 | 0 | 0 | 2 |
| Cryotherapy | 1 | 0 | 2 | 3 |
| Electrocoagulation | 1 | 0 | 0 | 1 |
| Phototherapy | 1 | 0 | 0 | 1 |
| Total | 14 (51.85%) | 5 (18.51%) | 8 (29.63%) | |
| Other therapies | ||||
| Antifungals | 3 | 2 | 10 | 15 |
| Fusidic acid | 2 | 0 | 3 | 5 |
| Chlorphenamine maleate | 1 | 0 | 0 | 1 |
| Antibiotics, unspecified | 0 | 2 | 13 | 15 |
| Antivirals, unspecified | 0 | 0 | 1 | 1 |
| Acyclovir | 0 | 0 | 2 | 2 |
| Valacyclovir | 0 | 0 | 1 | 1 |
| Unspecified antihistamines | 0 | 0 | 1 | 1 |
| Diphenhydramine | 0 | 0 | 1 | 1 |
| Promethazine | 0 | 1 | 2 | 3 |
| Dapsone | 0 | 1 | 3 | 4 |
| Total | 6 (12.24%) | 6 (12.24%) | 37 (75.51%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coppola, N.; Cantile, T.; Canfora, F.; Adamo, D.; Bucci, P.; Mignogna, M.D.; Leuci, S. Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review. J. Clin. Med. 2022, 11, 6550. https://doi.org/10.3390/jcm11216550
Coppola N, Cantile T, Canfora F, Adamo D, Bucci P, Mignogna MD, Leuci S. Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review. Journal of Clinical Medicine. 2022; 11(21):6550. https://doi.org/10.3390/jcm11216550
Chicago/Turabian StyleCoppola, Noemi, Tiziana Cantile, Federica Canfora, Daniela Adamo, Paolo Bucci, Michele Davide Mignogna, and Stefania Leuci. 2022. "Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review" Journal of Clinical Medicine 11, no. 21: 6550. https://doi.org/10.3390/jcm11216550
APA StyleCoppola, N., Cantile, T., Canfora, F., Adamo, D., Bucci, P., Mignogna, M. D., & Leuci, S. (2022). Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review. Journal of Clinical Medicine, 11(21), 6550. https://doi.org/10.3390/jcm11216550