Abstract
In a scenario where eco-sustainability and a reduction in chemotherapeutic drug waste are certainly a prerogative to safeguard the biosphere, the use of natural products (NPs) represents an alternative therapeutic approach to counteract cancer diseases. The presence of a heterogeneous cancer stem cell (CSC) population within a tumor bulk is related to disease recurrence and therapy resistance. For this reason, CSC targeting presents a promising strategy for hampering cancer recurrence. Increasing evidence shows that NPs can inhibit crucial signaling pathways involved in the maintenance of CSC stemness and sensitize CSCs to standard chemotherapeutic treatments. Moreover, their limited toxicity and low costs for large-scale production could accelerate the use of NPs in clinical settings. In this review, we will summarize the most relevant studies regarding the effects of NPs derived from major natural sources, e.g., food, botanical, and marine species, on CSCs, elucidating their use in pre-clinical and clinical studies.
1. Introduction
Despite prominent advances in the field of cancer prevention and early diagnosis, it is expected that one in five people will develop cancer during their lifespan. One of the greatest challenges in translational oncology is limiting the onset of primary or acquired drug resistance, which is boosted by cancer stem cells (CSCs). CSCs represent a pluripotent heterogeneous population within tumor bulk, with self-renewal and differentiation abilities, contributing to the failure of conventional therapies and, therefore, to disease relapse and metastasis [1]. Increasing evidence points out that different natural products (NPs) can modulate the CSCs’ hallmarks and sensitize them to conventional treatment [2]. NPs show minimal side effects in comparison with chemotherapeutics, and many studies have demonstrated their emerging role as adjuvant agents in cancer treatment. In this review, we point out the potential effects of major NPs derived from different origins (dietary, botanical, and marine sources) on CSCs in pre-clinical and clinical settings.
2. Cancer Stem Cells: The Main Players in Drug Resistance
Drug resistance is doubtless the main challenge of treatment in cancer patients. It is possible to distinguish two categories of drug resistance: intrinsic resistance and acquired resistance after drug treatment [3]. Compelling evidence highlights that intratumoral heterogeneity is one of the major hurdles involved in intrinsic drug resistance, in which the CSCs represent the main players due to their self-renewal and differentiation abilities [4,5]. The presence of CSCs has been characterized in different tumors, such as thyroid, colorectal, breast, prostate, and other solid tumors [6,7]. CSCs are identified and can be isolated by the expression of specific surface markers such as CD133 [8], CD44 [9], CD44v6 [10], EpCAM [11], or enzyme activity such us ALDH [12]. CSCs are also defined as tumor-initiating cells, as they can generate tumor xenografts in immunocompromised mice models [13]. Moreover, the failure of conventional therapies, based on the use of radiotherapy and chemotherapy to induce DNA damage in highly proliferative cells and to eradicate tumor mass, is strictly due to the presence of CSCs, which are characterized by multiple survival mechanisms [14]. In particular, the mechanisms through which CSCs escape chemotherapeutic treatments are different, such as i) drug export (the aberrant expression of ATP-binding cassette, ABC, drug pumps); ii) high survival (the inhibition of antiapoptotic processes, the high expression of proteins involved in DNA-damage repair, high telomerase activity); iii) reactive oxygen species (ROS) decrease (high ALDH activity, high expression of detoxification enzymes);and iv) the aberrant activation of pathways involved in stemness [15,16].
2.1. Drug Export in CSCs
It is common knowledge that the high expression of ABC proteins contributes to chemotherapy resistance and that CSCs overexpress different drug-transporter pumps, including ABCB1, ABCG2, and ABCC1 [15,17]. The Hoechst 33342 side population assay is a useful method to identify and isolate the CSC subpopulation in solid and hematopoietic tumors [18]. Yin et al. reported that CD133+ EPCAM+ liver CSCs express high levels of ABCG2 and ABCB1 and are highly resistant to doxorubicin treatment. The use of specific ABC inhibitors increases doxorubicin intracellular efflux, decreasing the sphere-forming capacity and viability of CSCs [19]. Other ABC transporters, including multidrug resistance protein 1 (MRP1, ABCC1), breast cancer resistance protein (BCRP), and MRP5/ABCC5, are reported as multidrug resistance transporters in solid and hematopoietic tumors [20,21,22]. Moreover, CD133+ melanoma CSCs expressed higher levels of ABCB5 compared to CD113− cells and are resistant to the antiapoptotic activity of the natural compound caffeic acid phenethyl ester [23]. In the lung, the high expression levels of ABCB1 in CSCs mediated the resistance to PHA-665752 and crizotinib, a MET inhibitor [24]. Although the targeting of ABC transporters could be an effective strategy to target CSCs, the use of specific inhibitors causes many side effects, due to the expression of the same targets in normal cells, as well [24].
2.2. Enhanced Survival Ability in CSCs
CSCs can also circumvent the toxic effects induced by chemotherapeutic treatment activating DNA damage response (DDR) by the ATM(ataxia-telangiectasia-mutated)- and ATR (ATM- and RAD3-related)-dependent phosphorylation of targets such as Check-1, Check-2, or H2A.X (known as γH2A.X when phosphorylated) [25]. Manic and co-workers demonstrated that in colorectal CSCs the treatment with chemotherapeutic agents induces the activation of the DDR players, such as PARP1, RAD51, and/or MRE11, resulting in higher DNA damage repair machinery [26]. In breast cancer, both BRCA1wt and BRCA1mut CSCs were highly resistant to PARP inhibitors, due to the high expression of Rad51 and Sam68, and the inhibition of this critical signaling axis hampered CSC viability [27,28]. In addition, CD133+ glioma CSCs displayed resistance to radiotherapy treatment by the activation of DNA-damage repair mechanisms, where Check-1 and Check-2 are the main players. The inhibition of these two effectors reverted the radioresistance in glioma-CSCs, suggesting that targeting DNA damage could be a promising therapeutic approach for brain cancer treatment [29].
The deregulation of apoptotic pathways is another mechanism underlying CSC-mediated chemoresistance. A weak expression of death receptors, such as TRAIL and FAS, and the overexpression of inhibitor apoptosis proteins (IAPs) have been described in CSCs compared to differentiated tumor cells [6,30]. In CSCs, IAPs are often overexpressed and impair the activation of the apoptosis cascade by mediating pro-apoptotic protein degradation [31]. CD133+ colorectal CSCs highly resistant to 5-fluorouracil (5-FU) treatment expressed high levels of SURVIVIN, and the use of a specific aptamer-SURVIVIN siRNA enhanced the in vitro and in vivo 5-FU efficacy [32,33]. Moreover, in nasopharyngeal CSCs, XIAPs increased the stability of SOX2, and the use of an inhibitor of the IAP family in combination with 5-FU impaired tumor growth [34]. It has been reported that an aberrant expression of BCL-2 family members in CSCs contributes to drug resistance [20,35]. BCL-2 is overexpressed in leukemia stem cells and the use of a specific inhibitor of BCL-2, venetoclax, combined with azacitidine, resulted in disease remission in acute myeloid leukemia by CSC targeting [36,37]. In gastro-esophageal cancers, the use of the small molecule AT-101, which inhibits the BCL-2 family, decreased the expression of CSC markers (YAP1/SOX9) [38] (NCT00561197).
One of the effects of radiotherapy is the induction of DNA damage through the production of ROS and water-derived radicals. In CSCs, the presence of ROS is dramatically reduced due to the increase in ROS scavengers, limiting apoptosis induction and DDR mechanism activation [39]. The CSCs can also escape from anticancer therapies by increasing aldehyde dehydrogenase (ALDH) activity, which acts by reducing intracellular ROS levels. In turn, ROS generated from radio- and chemotherapy enhance the cytosolic expression of aldehydes, such as ALDH1A and 3A1 [40]. High levels of drug-metabolizing enzymes, such as ALDH1a1 and bleomycin hydrolase (BLMH1), have been characterized in the secretome of colorectal CSCs, increasing chemoresistance [41]. Moreover, several studies have pointed out that CSCs isolated from different tumor types display high ALDH expression levels and activity, which boost their chemoresistance [12,42]. Therefore, the upregulation of ROS levels could be an efficient strategy to counteract CSC features and sensitize CSCs to treatments.
2.3. Stemness Induction in CSCs by Different Signaling Pathways
Several signaling pathways, among which are Notch, Sonic-Hedgehog (SHH), Wnt/β-catenin, PI3K/Akt/mTOR (mTORC1 and mTORC2), TGF-β, JACK/STAT, and Hippo-YAP/TAZ, are aberrantly activated or deregulated in CSCs compared to normal stem cells [43].
The Wnt signaling pathway plays a key role during embryogenesis, and in many cancers, such as breast, colorectal, thyroid, and esophageal cancers, its activation promotes CSC growth and chemoresistance [43,44]. It has been demonstrated that the Wnt pathway is crucial for the maintenance of intestinal crypt homeostasis, and the APC mutation in transgenic mice increased the presence of LGR5+ stem cells at the bottom of crypts, boosting the transformation in microadenoma [45]. Vermeulen et al. demonstrated that the Wnt pathway is highly activated in CD133+ colorectal CSCs and can be influenced by extrinsic factors secreted by TME cells [46]. In hepatocellular carcinoma, the activation of the Wnt signaling pathway, induced by protein tyrosine kinase-2 (PTK2), boosted CSC tumorigenic potential and contributed to sorafenib resistance [47]. In endometrial CSCs, Lu and co-workers showed that SPARC-related modular calcium binding 2 (SMOC-2) interacts with Fzd6 and LRP6 (LDL-receptor-related protein 6) receptors and activates the Wnt/β-catenin pathway, increasing cisplatin and placlitaxel resistance [48].
The SHH signaling pathway is involved in normal embryogenesis development and plays a key role in the promotion of tumor growth and in drug resistance, upregulating the genes involved in CSC maintenance, such as CD44, CCND2, c-MYC, NANOG, OCT4, and ALDH1 [49,50]. The SHH signaling pathway is involved in chemoresistance mechanisms by the modulation of the ABCG2 transporter and ALDH activity [51,52].
The dual TGF-β role in tumor progression has been extensively studied [53]. In fact, TGF-β is a key regulator of stemness, promoting EMT and radio-/chemoresistance [54,55]. Moreover, it has been shown that the cooperation of TGF-β with other signaling pathways increases CSC features. TGF-β and tumor necrosis factor alpha (TNF-α) induced a mesenchymal phenotype in breast CSCs by decreasing CLDN3-4-7 gene expression and, in turn, increasing in vivo tumorigenesis and resistance to oxaliplatin, etoposide, and paclitaxel [56]. In leukemia stem cells, TGF-β regulated the activation of AKT and induced FOXO3a nuclear localization, boosting sphere-forming ability and tumor growth [57].
In addition to the mechanisms described above, other intrinsic and extrinsic factors contribute to drug resistance in CSCs. Increasing evidence sheds new light on the role of epigenetic alterations in increasing intratumoral heterogeneity and in the failure of standard therapies [58]. Several molecular mechanisms, such as DNA methylation, chromatin remodeling, regulation by non-coding RNAs, and the modification of histone proteins, contribute to the aberrant expression of ABC transporters in solid and hematological tumors [1,59]. Furthermore, numerous studies point out that the crosstalk between CSCs and the tumor microenvironment (TME) influences the plasticity of CSCs, promoting drug resistance [6,60].
To overcome this challenge in cancer treatment, many researchers have focused on the development of therapeutic approaches targeting CSCs and the different mechanisms involved in drug resistance. In this regard, NPs could be considered eligible candidates.
3. Natural Products as Adjuvant against Cancer Stem Cells
In recent years, due to rising drug costs and the need to protect the environment and give ecological credentials to chemotherapy compounds, the use of NPs is constantly growing and developing. In particular, NPs contain active compounds, which might affect multiple signaling pathways involved in self-renewal and the maintenance of CSCs, with limited side effects [61]. The use of these compounds in medicine has a historic background; in fact, the use of NPs has been reported since the time of the Egyptians for disease treatment. NPs can be extracted from several parts of plants, such as the root, stem, fruit, and leaf; dietary agents; and marine organisms [62,63].
The pharmaceutical industry shows great interest in NPs due to their unique properties, such as high diversity and steric complexity, lighter atoms, and low hydrophobicity [64]. These structural features can be used to synthesize commercial drugs useful for both cancer prevention and treatment [65]. Recent in vitro and in vivo studies have demonstrated that NPs counteract cancer progression by interfering with the self-renewal capacity of CSCs, the induction of apoptosis, the inhibition of cancer-cell spreading, and the arrest of the cell cycle [61]. Moreover, several natural compounds, such as alkaloids, terpenoids, polyphenols, and flavonoids are efficient modulators of ABC transporters and sensitize CSCs to conventional chemotherapeutic treatment [66].
To date, about 500 clinical trials are registered on the clinical trial.gov website, reporting the effects of NPs and NP-derived drugs for the treatment of different cancers (www.clinicaltrial.gov, accessed on 20 September 2022). Here, we report a large overview of the properties of NPs that sensitize CSCs to conventional chemotherapeutic treatments.
3.1. NPs Derived from Dietary Sources
A strong correlation has been demonstrated between tumor incidence and a correctly healthy lifestyle. Many NPs derive from food and belong to the polyphenols category. Polyphenols are characterized by the presence of aromatic benzene rings bonded to hydroxyl groups. These compounds are classified into stilbenes, lignans, tannins, flavonoids, and phenolic acids. Polyphenols show a role in the regulation of angiogenesis, inflammation, and the apoptosis of CSCs in in vitro settings [67]. Moreover, they can improve immune response by modulating T lymphocytes [68]. In this regard, recent studies have also highlighted that natural polyphenols can be used as adjuvants in association with conventional therapy to limit the CSCs’ drug-resistance phenomenon [69,70].
It has been demonstrated that curcumin, a polyphenol extracted from Curcuma longa, has anticancer effects against different types of tumors [71]. One of the prominent anticancer activities of curcumin is the blocking of NF-kB pathways through the inhibition of IKK activity [72]. Of note, liver cancer cells displayed different phenotypes after curcumin treatment, which can be divided into sensitivity and resistance. In sensitive cells, curcumin reduced cell viability via the reduction in CSC features, such as SP population, sphere-forming capacity, and tumorigenic potential. Conversely, curcumin treatment boosts stem-like properties in resistant cells. To identify the signaling pathways modulated by curcumin in sensitive and resistant cells, the authors performed a transcriptomic analysis which points out a downregulation of HDACs in sensitive cells. Curcumin, in combination with HDAC inhibitors, affected the sphere-forming ability and reduced the SP fraction in resistant cells [73]. In addition to the regulation of NF-kB pathways, curcumin modulates another key tumorigenic signal. Wu et al. reported that curcumin can inhibit the JAK2/STAT3 pathway in lung CSCs, reducing in vitro tumorsphere formation capacity and impairing tumor growth in a pre-clinical mouse model [74]. Moreover, this NP reduced the proliferation of and in turn promoted apoptosis in lung CSCs, causing a reduction in the main stemness markers through the downregulation of the Wnt/β-catenin and SHH pathways [75]. Curcumin, alone or in combination with piperine, inhibited the formation of tumorspheres in breast cancer cells, interfering with the stem-cell signaling pathways involved in carcinogenesis [76]. Moreover, curcumin could prevent the cell proliferation of LGR5+ colorectal cells by triggering autophagy and blocking via the TFAP2-mediated ECM pathway [77]. In recent years, several studies have shown that natural polyphenols may be used as adjuvant therapy in association with traditional treatment to reduce CSC drug resistance [69,70]. Curcumin is associated with low doses of cisplatin-induced apoptosis and reduced the migration in the CD166+/EpCAM+ CSC subpopulation in lung cancer cells by enhancing the sensitivity of the cells to chemotherapy [78]. In thyroid cancer, the combinatorial treatment with curcumin and cisplatin impaired sphere formation and the expression of stemness markers in thyrospheres via the downregulation of the JAK/STAT3 pathway [79]. Although different in vitro and in vivo studies have highlighted the role of curcumin in sensitizing CSCs to therapy, its use in clinical settings is limited by insolubility in water and fast metabolism [80].
Resveratrol is a natural product present in several types of food, such as the skin of grapes and berries, with multiple antitumoral effects, such as the inhibition of angiogenesis and detoxification enzymes and the induction of apoptosis [81,82]. In this regard, resveratrol can be considered a promising chemopreventive cancer agent. Jang et al. reported in a skin cancer mice model that the topical administration of resveratrol prevents tumor growth [83]. In osteosarcoma, resveratrol reduced cytokine synthesis (IL-6, TNF-α, IFN-γ, and oncostatin M) and inhibited STAT3 signaling to diminish the expression of CD133CSC markers [84]. According to Ferraresi et al., resveratrol could be used as a therapeutic strategy for the treatment of ovarian cancer, reducing cell migration and viability. Specifically, resveratrol counteracted the effect mediated by lysophosphatidic acid, inhibiting SHH signaling with the reduction in BMI1, a polycomb ring finger transcriptional factor involved in the activation of Hedgehog and restoring the autophagy pathway [85]. In pancreatic cancer, resveratrol impaired the stem-like features and the tumorigenic and invasive capacity of cancer cells [86]. In combination with 5-FU, resveratrol decreased the survival of CD133+ colorectal CSCs [87]. Another antitumoral resveratrol mechanism is the induction of oxidative stress. In breast cancer CSCs, resveratrol impaired mammosphere formation and xenograft tumor growth by inducing autophagy, with an increase in LC3-II, Beclin1, and Atg 7 expression levels, and reducing the Wnt pathway [88]. Moreover, this NP enhances the generation of ROS by overloading the mitochondrial electron transport chain, which ultimately influences cell apoptosis/necrosis and enhances cell death in colorectal cancer [89,90]. For these reasons, this compound can be effective in the inhibition of viability, tumorigenic potential, and self-renewal ability of CSCs. Of note, resveratrol modulates the crosstalk between TME and CSCs. In a multicellular TME system, resveratrol affected the interaction between colorectal CSCs and stromal cells and reduced the expression of stemness markers and sphere-forming capacity by blocking p65 NF-kB nuclear translocation [90]. The same mechanism of action has been reported in breast cancer. Resveratrol decreased the percentage of CD44+/CD24− subpopulations and the expression levels of SOX2 and BMI-1 in BCSCs treated with the conditioned medium of cancer-associated fibroblasts [91].
Epigallocatechin-3-gallate (EGCG), a type of catechin found in green tea, has a chemopreventive activity against different types of cancers in vitro, in vivo, and in clinical settings [92,93]. Treatment with EGCG impaired the in vivo growth of prostate, lung, and gastrointestinal cancer cells [94]. In particular, EGCG regulated the expression of CSC markers and, thus, CSC features [95,96]. Luo et al. hypothesized the use of EGCG in colon cancer prevention and treatment as dietary supplements or adjuvant therapy, due to EGCG’s anti-proliferation and anti-migration properties [97]. EGCG treatment reduced the invasive capacity and induced apoptosis through the downregulation of the STAT3 pathway and the modulation of proteins involved in EMT and apoptosis, impaired Wnt pathway activation, and increased the sensitivity to 5-FU treatment in colorectal CSCs [97,98,99]. In lung cancer, EGCG targeted CD133+ cells, decreasing the self-renewal and tumorigenic potential of CSCs through the regulation of the circadian rhythm protein CLOCK [100]. Moreover, EGCG downregulated the Wnt pathway and reduced the proliferation and stemness marker expression in lung CSCs [101].
Flavonoids are polyphenolic compounds found in nuts, teas, fruit, and vegetables with antioxidant, anti-inflammatory, and anticancer properties [102]. The classification of flavonoids depends on their level of oxidation and includes flavanones, flavones, flavanols, and anthocyanins [103]. Several studies hypothesize that diets containing a high number of flavonoids could have cancer chemopreventive effects, targeting CSCs [104].
Citrus fruits including Citrus depressa (shiikuwasa), and Citrus sinensis (oranges) contain nobiletin, a healthy dietary polymethoxylated flavone [105] with a variety of biological actions, including anti-inflammatory, anti-tumor, and neuroprotective effects [106,107]. Nobiletin enhanced the internalization of chemotherapeutic or other natural compounds viathe inhibition of ABC transporters [108,109]. In non-small cell lung cancer, treatment with nobiletin inhibited the Wnt pathway and negatively correlated with EMT and stemness, reducing CD133 and ALDH1 stem markers [110]. Our group recently demonstrated that nobiletin and xanthohumol—a prenylated flavonoid contained in hop cones—extracts reduced the viability of colorectal CSCs and synergized with FOX (5-FU plus oxaliplatin) in inducing apoptosis and reducing stemness features, such as CD44v6 expression and Wnt pathway activation [111].
Apigenin is a bioavailable flavonoid belonging to the flavone class and is present in vegetables, fruits, and drinks. Apigenin exhibits anti-inflammatory activities, antioxidant effects, and anticancer properties [112,113]. Erdogan et al. demonstrated that adjuvant therapy with apigenin enhanced the sensibility of prostate CSCs to cisplatin treatment. This combinatorial therapy increased the cisplatin-induced apoptosis via the downregulation of BCL-2, SHARPIN, and SURVIVIN mRNAs, and enhanced the expression levels of caspase-8, Apf-1, and P53 [114]. In breast cancer, apigenin reduced the CD44+/CD24− subpopulation in triple-negative breast CSCs, inducing tumor shrinkage through the downregulation of YAP/TAZ activity [115]. Moreover, apigenin in combination with cisplatin reduced the tumorigenic potential of CD133+ lung CSCs [116].
Quercetin is a secondary metabolite from fruit and vegetable flavonols with anti-inflammatory and antioxidant properties. Cao et al. described howquercetin-3-methyl ether impaired the sphere-forming capacity of breast CSCs by reducing the expression of stemness genes (SOX2, NANOG) and the Notch and PI3K/AKT pathways [117]. Moreover, quercetin inhibited the tumor growth and metastasis formation of CD44+/CD24− CSCs and reduced the expression levels of ALDH1A and CXCR4 [118,119]. In CD24+/CD133+ pancreatic CSCs, quercetin reduced the activation of the Wnt pathway and the expression of stemness markers [120].
Naringin and naringenin are flavanones obtained from citrus fruits with anti-inflammatory, antioxidant, and antitumoral properties. These natural products display chemopreventive activity in many tumors, such as lung and colorectal cancers [121,122]. Many studies have pointed out that naringin and naringenin hamper tumor growth and progression by inhibiting pathways involved in survival, apoptosis, ROX detoxification, autophagy, and metastasis formation [123]. By bioinformatics analyses, Hermawan et al. identified naringenin as a potential drug to target breast CSCs. Indeed, naringenin treatment decreased the sphere-forming and colony-forming capacity, migration, and expression of stemness-related genes (CTNNB1, ALDH1, VIMENTIN) in breast CSCs [124]. In cervical cancer spheroids, naringenin in combination with cisplatin reduced the cell viability and invasion of cancer cells [125].
Sulforaphane (SFN) is an active isothiocyanate derived from the hydrolyzation of glucoraphanin by myrosinase activity. SFN is a phytoconstituent that belongs to the Brassicaceae family, which includes vegetables such as cauliflower, kale, cabbage, and broccoli. Numerous manuscripts have highlighted SFN’s anticancer effects in both in vitro and in vivo models in different tumors, acting as an epigenetic modulator that induces apoptosis and senescence [126,127]. Li et al. highlighted that SFN treatment decreased the percentage of CD133+and ALDH+ cells in lung spheroids induced after exposure to cisplatin and enhanced the in vivo antitumor effect of cisplatin [128]. In breast cancer, SFN impaired the formation of mammospheres via the reduction in ALDH+ cells and the activation of the Wnt/β-catenin signaling pathway. Moreover, SFN treatment decreased tumor growth and the second engraftment of breast CSCs [129]. Castro et al. showed that SFN can modulate the cell proliferation, tumorsphere formation, cell viability, and phenotype of CSCs derived from triple-negative breast cancer and counteract the xenograft tumor growth in mice [130].
Fisetin is another flavonol found in some vegetables and fruits including onion, cucumber, apple, grape, and strawberry. Fisetin is a neuroprotective agent and acts as a chemopreventive/chemotherapeutic agent in different cancers [131]. In lung CSCs, treatment with fisetin inhibited cell growth by modulating mTOR and PI3K/AKT signaling and decreased the number of colonies in a dose-dependent manner [132]. Another study in lung cancer demonstrated that fisetin exhibits anti-invasion and anti-proliferative effects via the downregulation of CD44 and CD133 stem-like markers [133]. In Table 1, we summarize the studies previously described regarding the effect of NPs on CSCs (Table 1).

Table 1.
NPs derived from dietary sources and effects on CSCs.
3.2. NPs Derived from Botanical Sources
Different drugs, derived from natural compounds, are used in clinical practice as anticancer agents. Paclitaxel isolated from Taxus brevifolia was one the first anticancer agents studied in ovarian and breast adenocarcinoma. Some plants can produce toxic substances such as phenol or tannin when attacked by predators [134]. In this regard, many researchers studied plants as a possible source of NPs to counteract CSCs.
Luteolin is a flavone present in about 300 plant species [135]. Luteolin impaired the expression of the stemness markers ABCG2 and CD44 and affected the ALDH1 activity and spheroid formation capacity of breast CSCs. Moreover, luteolin sensitized CSCs to taxol treatment [136]. Luteolin in combination with quercetin impaired the sphere-forming ability and the expression levels of NANOG, SOX2, and CD44 [137]. In oral CSCs, luteolin effectively reduced proliferation, ALDH activity, and CD44, inactivating the IL6/STAT3 axis [138].
Berberine (BBR) is an isoquinoline alkaloid obtained from the roots and stems of anti-inflammatory plants and can induce apoptosis by reactive oxygen generation [139,140]. In the literature, the ability of BBR as a modulator of epigenetic modification has been widely demonstrated [141,142]. Zhao et al. showed that BBR impairs the proliferation and sphere-forming capacity of colorectal CSCs by enhancing the expression levels of p27 and p21, increasing the percentage of cells in the G1/G0 phase and, in turn, reducing CD44 and CD133 markers. In line with its epigenetic modulator activity, BBR impaired the RNA m6A methylation levels. Moreover, BBR treatment affects the tumorigenic capacity of colorectal CSCs and sensitizes the cells to 5-FU and irinotecan [143]. In pancreatic cancer, BBR and gemcitabine combinatorial treatment decreased SP percentage and the expression of the stemness genes POU5F1, SOX2, and NANOG [144]. Moreover, BBR can counteract sphere formation, the expression of EMT stemness markers, and the activation of the GLI1–BMI1 axis induced by chemotherapy in ovarian CSCs [145]. In neuroblastoma, BBR treatment was able to induce the expression of epithelial-like marker E-cadherin, downregulating crucial signaling pathways that regulate tumor progression, such as PI3K/Akt, TGF-β, and MAPK [146].
Vincristine is another alkaloid, derived from the Madagascar periwinkle, Catharanthus roseus, with anti-tumor activity. Its biological mechanism of action is based on the inhibition of microtubule aggregation and, consequently, the arrest of cell mitosis in metaphase [147]. The treatment of a neuroblastoma cell line (SH-SY5Y) with vincristine reduced cell proliferation in a dose-dependent manner by blocking the cell cycle in the G2-M phase with increased cyclin B expression and decreased cyclin D levels. Overall, these data showed that vincristine could be a promising chemotherapeutic agent for the treatment of neuroblastoma [148]. For decades, vincristine has been used in combination with chemotherapy in different tumors, as well as acute myeloid leukemia [149], lung cancer [150] (NCT00003847), colorectal cancer [151], and breast cancer [152]. Nevertheless, its anti-proliferative effects in CSCs have been little shown. Moon et al. highlighted that vincristine influences the methylation state of the runt-related transcription factor-3 gene (RUNX3) in colorectal cancer. The treatment with this alkaloid induced the demethylation of RUNX3, leading to the recovery of RUNX3 mRNA expression in colorectal cancer cells without affecting DNA methylation in healthy colon cells [153]. These observations suggest a potential therapeutic approach for CSC targeting.
Alkaloids gained from the bark of the Cinchona officinalis tree have been used for more than a century for malaria prevention and treatment. Among these alkaloids, chloroquine (CQ), derived from quinine, is a potent inhibitor of autophagy in cancer cells [154]. Cufì et al. reported that CQ treatment slightly reduced the CD44+/CD24− stem-like subpopulation and vimentin expression in triple-negative breast cancer (TNBC) cells [155]. Moreover, CQ in combination with paclitaxel decreased ALDH-positive and CD44+/CD24− cell subpopulations and the sphere-forming capacity of TNBC cells. The combination treatment impaired autophagy through the upregulation of LCB3-II and p62 expression levels and enhanced apoptosis and cleaved caspase-3 levels by inhibiting the JAK/STAT pathway. In in vivo settings, CQ and paclitaxel lessened in vivo tumor growth and lung metastatic foci [156]. Liang et al. showed that CQ targets breast CSCs by inducing mitochondrial depolarization and the accumulation of DNA double-strand breaks, and CQ in combination with carboplatin diminished autophagy and the expression levels of proteins involved in DNA repair machinery [157]. CQ affected the CD133+ subpopulation and the tumorigenic potential of pancreatic CSCs and patient-derived xenografts (PDXs) through a mechanism not previously described. In fact, CQ inhibited the CXCL12/CXCR4 axis and SHH pathway in pancreatic- CSCs [158]. A similar effect of CQ treatment was also observed in esophageal squamous cell carcinoma CSCs [159].
Recent studies have revealed that capsaicin, derived from plants of the genus Capsicum, showed considerable anticancer effects [160]. Zhu et al. reported that capsaicin decreases sphere size, hampers CSC survival in a dose-dependent manner, and downregulates markers such as CD133, CD44, OCT-4, NANOG, and SOX2, typically expressed in prostate CSCs. Moreover, the authors showed that capsaicin interfered with the Wnt/β-catenin signaling pathway in prostate CSCs. Briefly, capsaicin drastically reduced GSK3 phosphorylation and avoided β-catenin’s translocation into the nucleus, downregulating target genes such as MYC and CCND1. The activation of the Wnt/β-catenin pathway restored the sphere-forming ability of prostate CSCs and induced the upregulation of the above-described stemness markers [161].
A saturated derivative of capsaicin, dihydrocapsaicin (DHC), is a potent inducer of autophagy [162]. DHC-induced autophagy in a catalase-dependent manner in colon and breast cancer cell lines has been reported. Oh and co-workers showed that DHC induced breast and colorectal cancer cell arrest in G0-G1, upregulating the expression levels of autophagy-related proteins [163]. Thanks to its ability to induce autophagy, DHC could be considered a promising anticancer agent. In this regard, DHC efficiently targeted the CD133+ neural cell population, inducing cell death [164] (US20090076019A1). However, due to its low bioavailability, DHC isno longer being tested as a CSC-targeting agent (Table 2).
Table 2.
NPs derived from botanical sources and their effects on CSCs.
3.3. NPs Derived from Marine Sources
The marine microenvironment is a heterogeneous environment, characterized by unique conditions (low oxygen and sunlight, as well as high salinity and pressure) that favor the presence of micro- and macro-organisms producing particular metabolites. It has been demonstrated that these molecules with unique biochemistry structures, containing various heterocyclic rings and diverse heteroatoms, can be used to prevent and treat cancer [62]. Given the growing number of marine natural compounds (MNC) used in medicine, more researchers have focused on the structure and synthesis of analogs with anticancer properties [165].
Nortopsentin, a bis-indolyl alkaloid isolated from deep-sea sponges (Spongosoritesruetzleri), exhibits significant antitumor activity against P388 murine leukemia [166]. Cascioferro et al. synthesized nortopsentin analogs by introducing the substitution of a central imidazole ring with a 1,2,4-oxadiazole motif and a 7-azaindole in place of the original indole motif. Among these compounds, 1k and 1n displayed cytotoxic effects on MCF-7, Caco-2, HeLa, and HCT-116 cells. The anti-proliferative activity on MCF-7 of these compounds was associated with a pro-apoptotic activity involving chromatin condensation and membrane blebbing. Moreover, these chemicals induced a buildup of cells in the G0-G1 phase, indicating that they could influence DNA replication [167]. Similar results were obtained by Di Franco et al. using another analogous of nortopsentin, NORA234. This compound reduced, at early timepoints, the clonogenic potential and the proliferation rate of colorectal CSCs. However, NORA234’sprolonged administration drove the selection of resistant subclones, characterized by high expression levels of CD44v6 and β-catenin activity, with an increased CHK1-driven DNA damage response. Treatment with NORA234 in combination with CHK1 inhibitor enhanced apoptosis and hampered the proliferation and clonogenic capacity of colorectal CSCs together with the decrease in CD44v6+/Wnthigh subpopulations [168].
Renieramycin M (RM) is the major bis-tetrahydroisoquinolinequinone alkaloid derived from the blue sponge Xestospongia species. Treatment with non-toxic concentrations of RM reduced colony and spheroid formation and the expression of CD133, CD44, and ALDH1A1 stem-like markers in lung CSCs [169]. According to these findings, RM could be considered a promising anticancer compound.
Fucoxanthin and its metabolite fucoxanthinol (FxOH), carotenoids isolated from different brown algae species, exhibit beneficial cancer prevention and anticancer features [170]. Terasaki et al. demonstrated that FxOH impaired the growth, sphere-forming ability, and tumorigenic potential ofCD44high/EpCAMhigh colorectal CSCs by the inactivation of AKT signaling and the downregulation of PPARβ/δ and PPARγ protein expression levels [171]. Moreover, FxOH treatment reduced the expression levels of N-cadherin and vimentin EMT markers, which correlate with lessened levels of glycine and succinic acid, in colorectal CSCs [172]. Sulfated polysaccharides called fucoidans derived from brown algae have a variety of biological functions. According to Vishchuk and colleagues, sulfated (1→3)-L-fucan, obtained by Saccharinacichorioides, reduced the colony-formation capacity of different cancer cell lines [173].
Bryostatin-1 is a macrocyclic lactone of marine origin derived from the Bugula neritina invertebrate. Different pre-clinical and clinical studies demonstrated its role as an antitumor agent [174,175]. Sikorska et al. showed that among different natural compounds, bryostatin-1 promoted a differentiated state in melanoma CSCs, reducing their high proliferative rate and the ABCB5+ subpopulation [176]. Bryostatin-1 increased the Gleevec-mediatedapoptosis of chronic myeloid leukemia SCs, reducing the fraction of G0/G1 CD34+ cells [177] (Table 3) (Figure 1).
Table 3.
NPs derived from marine sources and their effects on CSCs.
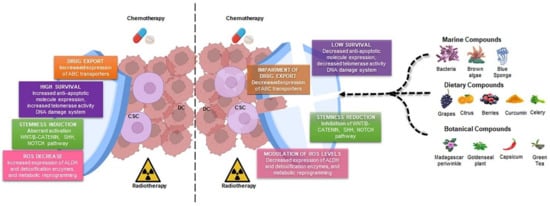
Figure 1.
Natural products destroy the shield of CSCs. Radio- and chemotherapy target differentiated cancer cells, which represent most cells within the tumor mass, sparing the CSC subpopulation, characterized by the high expression of ABC transporters, anti-apoptotic molecules, and detoxification enzymes and the aberrant activation of stemness pathways and DNA repair machinery (left part). Natural products derived from different sources (marine, food, and botanical compounds) are able to reduce CSC features and increase their sensitivity to radio- and chemotherapy (right part). DCs, differentiated cells; CSC, cancer stem cell; ABC, ATP-binding cassette.
3.4. Other Natural Compounds
Other NPs such as retinoids, which do not fit into the classifications of polyphenols, flavonoids, or alkaloids, have shown promising effects for targeting CSCs [178]. Retinoids, which are classified as terpenes, induce the differentiation of CSCs, making them more sensitive to chemotherapeutic agents [179]. All-Trans Retinoic Acid (ATRA) is a biologically active compound belonging to the retinoid group and is a metabolite of vitamin A. It is essential for a variety of biological processes, such as cell division, organogenesis, differentiation, and cell death. ATRA can inhibit ALDH activity and revert MDR in CSCs. Ginestier et al. displayed that ATRA decreased mammosphere formation by regulating signaling pathways involved in CSC differentiation [180]. In glioblastoma, treatment with ATRA increased the expression levels of astrocytic (GFAP) and neuronal (TUJI) markers and reduced proliferation and self-renewal in neurospheres through the modulation of the ERK1/2 pathway [181]. Furthermore, ATRA impaired the in vitro and in vivo proliferation of CSCs by decreasing the expression of OCT4, SOX2, Nestin, and CD44 and the activation of Wnt/β-catenin signaling in head and neck cancer [182]. In lung cancer, ATRA, in combination with gefitinib, reduced the ALDH1A1high/CD44high CSC subpopulation and growth boosted by chemotherapy [183]. Several studies have shown how ATRA’s epigenetic processes work [184,185].
Although the use of NPs might be faced with some problems, such as screening difficulties, NPs are characterized by peculiar biological structures, which make them an appealing approach to anticancer therapy [186].
4. Natural Products in Clinical Trial for Cancer Treatment
The high costs and side effects of chemotherapy and radiotherapy have led to a great interest in natural medicine. NPs being readily available and more tolerable in comparison with synthetic compounds make them attractive agents for cancer treatment [187]. Many NPs, such as curcumin, EGCG, resveratrol, quercetin, and apigenin, have shown strong anticancer effects in numerous pre-clinical studies, but the feasibility of translating the efficacy of these compounds in clinical trials is an ongoing challenge. Differences in genetics and metabolism between pre-clinical models and humans, as well as the solubility and the time of action of these compounds, could limit their use in clinical settings. Pharmacokinetics and pharmacodynamics studies could better elucidate NPs’ effects on humans. Despite several pre-clinical studies showing the therapeutic potential of curcumin, a few clinical trials assessed the effectiveness of curcumin in the treatment of cancer patients due to its reduced bioavailability [188]. Nonetheless, the use of curcumin as a substitute for corticosteroids (standard therapeutic agents) in combination with immunomodulatory compounds (lenalidomide) or as a proteasome inhibitor (bortezomib) in 15 multiple myeloma patients showed progression-free survival without the negative side effects linked to the steroid-based combination therapy [189]. Moreover, in multiple myeloma and prostate cancer patients, curcumin and piperine in combination delayed cancer progression (NCT04731844). The effect of curcumin on myeloma patients was also evaluated in a pilot randomized clinical trial. The treatment with melphalan, prednisone, and curcumin displayed an increased overall remission with a reduction in IL-6, VEGF, and TNF-α levels compared with myeloma patients treated with melphalan and prednisone alone [190] (ISRCTN14131419). In another clinical study enrolling 150 patients with advanced or metastatic breast cancer, the intravenous administration of curcumin (300mg) with paclitaxel (80 mg/m2) for 12 weeks induced a tumor reduction of 50.7% [191] (NCT03072992). There are many active clinical trials to evaluate curcumin’s chemopreventive, neoadjuvant, and radioprotective effects in breast cancer patients (NCT01975363, NCT03847623, NCT01246973). The phase IIa CUFOX clinical trial assessed the safety and effect of curcumin in combination with FOLFOX-based chemotherapy in metastatic colorectal cancer patients [192] (NCT01490996).
EGCG is a polyphenol with multiple antitumor activities [93]. In a second phase clinical trial, the effects of indole-3-carbinol (I3C) and EGCG in combination with taxane and platinum-based chemotherapy were tested in stage III–IV serous ovarian cancer patients. Patients treated with I3C and EGCG plus chemotherapy showed an increased median overall survival (60 months) and median progression-free survival (48.5 months) compared with single treatment and chemotherapy alone. Moreover, I3C and EGCG treatment reduced cancer recurrence [193] (ACTRN12616000394448). In a phase II study, EGCG treatment was evaluated in chemotherapy-treated advanced lung cancer patients who had developed acute radiation esophagitis as a side effect. Both EGCG preventive treatment and EGCG administration in radiation-treated patients decreased the esophagitis grade and the serum levels of pro-inflammatory factors compared with standard treatments in lung cancer patients [194] (NCT02577393). Similarly, a phase II study evaluated the effect of EGCG in esophageal cancer patients with esophageal obstruction [195] (NCT05039983). In bladder cancer patients, a phase II randomized pre-clinical trial assessed the effect of Polyphenon E (a green tea polyphenol formulation in which EGCG is a main component) in neoadjuvant therapy before the transurethral resection of a bladder tumor or cystectomy. Although there are no differences in EGCG tumor levels between the EGCG-treated and placebo patient groups, a dose-dependent downregulation of two tumor biomarkers, clusterin (apoptosis marker) and PCNA (proliferation marker), was observed in EGCG-treated patients, supporting the chemoprotective activity of this compound [196]. The impact of Polyphenon E on serum and tissue levels of progression biomarkers was characterized in a randomized phase II single-arm open-label clinical study including breast cancer patients. In particular, Polyphenon E neoadjuvant daily administration induced a decreasein serum HGF levels without altering those of VEGF (NCT00676793). The serum HGF and VEGF levels together with the measurement of oxidative damage and inflammatory biomarkers were also evaluated in a phase IB randomized dose-escalation trial in stage I–III hormone receptor-negative breast cancer patients treated with Polyphenon E for 6 months. After the treatment with adjuvant therapy, a significant, but transient, decrease in serum HGF and VEGF was observed [197].
Although many in vitro and in vivo studies have highlighted the potential use of resveratrol in clinical settings, a limited number of clinical trials have been carried out [198]. A phase I clinical study in breast cancer found that resveratrol was tolerated throughout a 12-week treatment period on 39 patients and increased levels of resveratrol were found in blood serum patient samples. After resveratrol treatment, no significant changes in p16, CCND2, APC, orRASSF-1α DNA methylation were observed, but only a decreased methylation profile of RASSF-1α and an increase in the APC profile [199]. These findings imply that resveratrol may operate as a chemopreventive agent for breast cancer by affecting the epigenetics of breast cancer-related genes. Alternatively, in a phase I clinical study, treatment with MPX (pulverized muscadine grape skin composed ofellagic acid, quercetin, and resveratrol) in biochemically recurrent prostate cancer patients (BRPC), at different concentrations (500 mg up to 4000 mg/day), was shown to be safe and tolerable [200]. Taken together, these data result in the possibility of investigating MPX’s effects in a randomized, multicenter phase II trial. In 112 patients of BRPC enrolled in a randomized, multicenter, placebo-controlled clinical trial, no significant difference was observed in terms of PSA doubling time in control and MPX-treated cohorts. Moreover, within the clinical trial, the authors identified a patient population that could benefit from treatment with MPX, but further studies are needed [201].
In another phase I pilot trial (NCT00256334), the effects of low doses of resveratrol derived from plants and resveratrol-containing freeze-dried grape powder (GP) were evaluated on Wnt-signaling modulation in colon cancer patients. Resveratrol/GP treatment (80 g/day containing 0.07 mg of resveratrol) significantly inhibited Wnt target gene expression (myc, jun, TCF7, cyclin D1, axin II) in healthy colonic mucosa without effects on tumor mucosa. This study highlights that GP treatment could have a role in the prevention of colon tumor formation [202]. In this clinical pilot study, SRT501, a micronized form of resveratrol, was administered to patients with colorectal cancer and hepatic metastases, who were scheduled to undergo hepatectomy, at a dose of 5.0 g daily for 14 days. This treatment method increased drug availability and absorption. After 1–2 weeks of therapy with resveratrol or SRT501, the observed amounts of parent resveratrol and its primary metabolites in the colon tissue of patients were comparable to the efficacious doses of resveratrol utilized in pre-clinical investigations. In addition, cleaved caspase-3, an indication of death, dramatically increased in malignant hepatic tissue after SRT501 therapy by 39% in comparison to tissue from patients who received a placebo [203]. Furthermore, a similar first-phase clinical trial has also confirmed the diminishing of ki-67 levels (a proliferation marker) in colorectal cancer patients [204] (NCT00433576). While overall data suggest that resveratrol has some pharmacological properties, it is uncertain if these effects are sufficient to make it an effective treatment agent for colon cancer. To date, 11 of 16 marine drugs are used in the treatment of different cancers [205]. In particular, Plitidepsin (Aplidin®, produced by PharmaMar) is a drug approved in Australia for multiple myeloma leukemia and lymphoma [206]. Polatuzumabvedotin (peptide derived from marine cyanobacteria), by inhibiting tubulin polymerization, induced CSC death. This NP was approved in 2019 by the FDA for the treatment of non-Hodgkin lymphomas, chronic lymphocytic leukemia, and B-cell lymphomas [207]. Lurbinectedin (a synthetic derivative of trabectedin) showed anticancer activity by the degradation and inhibition of RNA polymerase II; in 2020, it was approved for metastatic small lung cancer treatment [208]. In this regard, other molecules derived from the marine environment are undergoing clinical evaluation.
Vincristine belongs to antimitotic agent groups that interfere with microtubule organization. Several pre-clinical studies have demonstrated its role as an anticancer agent. Nonetheless, it has been shown that vincristine provokes neurotoxicity, suggesting its use at low dosages. In several clinical trials, vincristine was used at low concentrations in combination with doxorubicin, dacarbazine, methotrexate, and also rituximab [209]. In a clinical study carried out on children affected by low-grade glioma, treatment with vincristine and carboplatin was defined as eligible first-line therapy, representing the first European clinical randomized study and the second of European chemotherapy in childhood LGG [210] (European Union Clinical Trials Register No. 2005-005377-29). In an open-label, multicentre II phase clinical trial, pretreatment with ofatumumab (antibody against CD20) and miniCHOP (a combination with vinacristine, reduced-dose cyclophosphamide, prednisone, and doxorubicin) in 80-year-old patients improved overall survival in comparison with standard therapy [211] (NCT01195714).
Bryostatin-1 showed different effects mediated by the modulation of protein kinase PKC activity. Due to a lack of pharmacokinetics data in humans, the first clinical trials were hampered [212]. Alone or in combination with another drug, bryostatin-1 has been evaluated in phase I and II clinical trials. These multiple trials showed that this lactone, alone or in combination with other compounds, exerts synergistic anti-tumor activity. In a phase II trial, patients with metastatic renal carcinoma, treated with an intravenous infusion of bryostatin-1 with formulation PET (polyethyleneglycol, ethanol, and Tween 80), responded to the treatment without severe adverse effects [213]. The treatment of 25 patients with chronic lymphocytic leukemia (CLL) and relapsed low-grade non-Hodgkin lymphoma with bryostatin-1 resulted in one patient in complete remission and two in partial remission. Moreover, this treatment promoted a differentiative state of CLL cells, demonstrated by the presence of CD11c/CD22/CD20 B-cell subpopulation [214]. Nevertheless, Bryostatin-1 is not very available in nature, and it could need to be synthesized.
Chemicals produced from cruciferous vegetables, such as sulforaphane (SFN), a breakdown product of glucoraphanin, may help inhibit prostate cancer development and progression. A double-blind, randomized controlled trial, conducted on ninety-eight men scheduled for prostate biopsy, evaluated the effect of broccoli sprout extract (BSE) on the expression of different prostate cancer biomarkers such as histone H3 lysine 18 acetylation (H3K18ac), HDAC3, HDAC6, Ki67, p21, and histone deacetylase (HDAC). Unfortunately, BSE-treated patients did not significantly display a reduction in HDAC activity or prostate tissue biomarkers. By performing an RNA-seq analysis on prostate biopsies, 40 differently expressed genes linked to BSE treatment were characterized, including two prostate cancer-related genes, AMACR and ARLNC1. According to this study, supplementing with BSE is associated with alterations in gene expression but not with changes in prostate tissue biomarkers [215] (NCT01265953). Furthermore, an interventional clinical trial evaluated the effect of a diet rich in broccoli in reducing the risk of cancer progression, especially in men diagnosed with low- and intermediate-risk prostate cancer on active surveillance. Trans-perineal template biopsies from forty-nine men on active surveillance, who were fed different glucoraphanin-rich broccoli soups for 12 months, were analyzed by RNA sequencing. The obtained results displayed a reduced expression of genes linked to inflammation processes and EMT in men consuming the glucoraphanin-rich broccoli diet. Although the trial lacked the necessary power to evaluate clinical progression, an inverse relationship was found between the consumption of cruciferous vegetables and a decreased risk of prostate cancer advancement [216] (NCT01950143).
In a phase I clinical study, 37 colorectal cancer patients treated with chemotherapy were randomized to receive either 100 mg fisetin (n = 18) or placebo (n = 19) for seven consecutive weeks. Fisetin administration reduced the plasma levels of IL-8, hs-CRP, and the expression of MMP-7. Accordingly, fisetin might decrease the inflammatory state in colorectal cancer patients, supporting fisetin treatment as a potential supplementary anticancer drug for these patients and warranting future investigations [217] (code: IRCT2015110511288N9) (Table 4).
Table 4.
Natural products in clinical trials for cancer treatment.
5. Conclusions and Perspectives
In recent years, the rising costs of cancer treatment and the urgent need for eco-sustainability endorse a new paradigm in oncology, known by the term “Green Oncology”. To date, the ecological model, in which oncologists consider not only individual illness but also population health as a component of the biosphere, is increasingly replacing the biomedical and biopsychosocial ones. In this context, Green Oncology’s aim is to preserve the environment and the ecosystem by promoting the use of NP-derived drugs, which avoids treatments with chemotherapeutics that are not easily disposable and are also characterized by fewer side effects. Compelling evidence points out that NPs effectively lessen the stem-like properties of CSCs, which are refractory to standard and targeted therapies. In this review, we reported the most appealing pre-clinical studies regarding the ability of NPs to lessen the expression of CSC markers and the activation of pro-tumorigenic signaling pathways. Despite the promising results obtained with the use of NPs in in vitro systems and pre-clinical models, the limited systemic availability of these all-natural molecules as well as their faster metabolism pose a challenge to their efficacy in targeting cancer cells in organs far from the site of absorption. Although NPs could really improve the malignant progression of tumors, further efforts are needed to reduce the timeline of bench to bedside.
Author Contributions
Writing—original draft preparation, M.L.I., P.B., M.G. and G.S.; writing—review and editing; M.L.I., P.B., O.R.B., G.M., C.M., N.R., K.S., L.C., C.C., L.M., A.T., V.V., S.D.F., M.T. and M.G.; graphical contribution, G.M.; supervision, M.L.I., M.G. and G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministero dell’Università e della Ricerca, grant code PRIN 201WNKSLR to G.S. and RF 2018-12367044 and PSN2015, 6.2 CUP176J17000470001. A.T. and V.V. are researchers funded by European Union-FESR FSE PON Ricerca e Innovazione 2014-2020. M.L.I. and C.M. are researchers funded by European Union-FESR FSE PON Ricerca e Innovazione 2014-2020 DM 1062/2021. P.B., G.M., N.R. and K.S. are students in the Molecular and Clinical Medicine PhD Program. O.R.B. is a student in the Experimental Oncology and Surgery PhD Program.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Turdo, A.; Veschi, V.; Gaggianesi, M.; Chinnici, A.; Bianca, P.; Todaro, M.; Stassi, G. Meeting the Challenge of Targeting Cancer Stem Cells. Front. Cell Dev. Biol. 2019, 7, 16. [Google Scholar] [CrossRef]
- Moselhy, J.; Srinivasan, S.; Ankem, M.K.; Damodaran, C. Natural Products That Target Cancer Stem Cells. Anticancer Res. 2015, 35, 5773–5788. [Google Scholar]
- Schmidt, F.; Efferth, T. Tumor Heterogeneity, Single-Cell Sequencing, and Drug Resistance. Pharmaceuticals 2016, 9, 33. [Google Scholar] [CrossRef]
- Phi, L.T.H.; Sari, I.N.; Yang, Y.G.; Lee, S.H.; Jun, N.; Kim, K.S.; Lee, Y.K.; Kwon, H.Y. Cancer Stem Cells (CSCs) in Drug Resistance and their Therapeutic Implications in Cancer Treatment. Stem. Cells Int. 2018, 2018, 5416923. [Google Scholar] [CrossRef]
- Hausser, J.; Alon, U. Tumour heterogeneity and the evolutionary trade-offs of cancer. Nat. Rev. Cancer 2020, 20, 247–257. [Google Scholar] [CrossRef]
- Gaggianesi, M.; Di Franco, S.; Pantina, V.D.; Porcelli, G.; D’Accardo, C.; Verona, F.; Veschi, V.; Colarossi, L.; Faldetta, N.; Pistone, G.; et al. Messing Up the Cancer Stem Cell Chemoresistance Mechanisms Supported by Tumor Microenvironment. Front. Oncol. 2021, 11, 702642. [Google Scholar] [CrossRef]
- Veschi, V.; Verona, F.; Lo Iacono, M.; D’Accardo, C.; Porcelli, G.; Turdo, A.; Gaggianesi, M.; Forte, S.; Giuffrida, D.; Memeo, L.; et al. Cancer Stem Cells in Thyroid Tumors: From the Origin to Metastasis. Front. Endocrinol. 2020, 11, 566. [Google Scholar] [CrossRef]
- Ricci-Vitiani, L.; Lombardi, D.G.; Pilozzi, E.; Biffoni, M.; Todaro, M.; Peschle, C.; De Maria, R. Identification and expansion of human colon-cancer-initiating cells. Nature 2007, 445, 111–115. [Google Scholar] [CrossRef]
- Al-Hajj, M.; Wicha, M.S.; Benito-Hernandez, A.; Morrison, S.J.; Clarke, M.F. Prospective identification of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 2003, 100, 3983–3988. [Google Scholar] [CrossRef]
- Todaro, M.; Gaggianesi, M.; Catalano, V.; Benfante, A.; Iovino, F.; Biffoni, M.; Apuzzo, T.; Sperduti, I.; Volpe, S.; Cocorullo, G.; et al. CD44v6 is a marker of constitutive and reprogrammed cancer stem cells driving colon cancer metastasis. Cell Stem Cell 2014, 14, 342–356. [Google Scholar] [CrossRef]
- Loening-Baucke, V. Lichen sclerosus et atrophicus in children. Am. J. Dis. Child. 1991, 145, 1058–1061. [Google Scholar] [CrossRef] [PubMed]
- Ginestier, C.; Hur, M.H.; Charafe-Jauffret, E.; Monville, F.; Dutcher, J.; Brown, M.; Jacquemier, J.; Viens, P.; Kleer, C.G.; Liu, S.; et al. ALDH1 is a marker of normal and malignant human mammary stem cells and a predictor of poor clinical outcome. Cell Stem Cell 2007, 1, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.F.; Dick, J.E.; Dirks, P.B.; Eaves, C.J.; Jamieson, C.H.; Jones, D.L.; Visvader, J.; Weissman, I.L.; Wahl, G.M. Cancer stem cells--perspectives on current status and future directions: AACR Workshop on cancer stem cells. Cancer Res. 2006, 66, 9339–9344. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Zhang, J.G.; Zhang, X.; Li, Q. Targeting cancer stem cells for reversing therapy resistance: Mechanism, signaling, and prospective agents. Signal Transduct. Target Ther. 2021, 6, 62. [Google Scholar] [CrossRef]
- Begicevic, R.R.; Falasca, M. ABC Transporters in Cancer Stem Cells: Beyond Chemoresistance. Int. J. Mol. Sci. 2017, 18, 2362. [Google Scholar] [CrossRef]
- Rezayatmand, H.; Razmkhah, M.; Razeghian-Jahromi, I. Drug resistance in cancer therapy: The Pandora’s Box of cancer stem cells. Stem Cell Res.Ther. 2022, 13, 181. [Google Scholar] [CrossRef]
- Fletcher, J.I.; Haber, M.; Henderson, M.J.; Norris, M.D. ABC transporters in cancer: More than just drug efflux pumps. Nat. Rev. Cancer 2010, 10, 147–156. [Google Scholar] [CrossRef]
- Ho, M.M.; Ng, A.V.; Lam, S.; Hung, J.Y. Side population in human lung cancer cell lines and tumors is enriched with stem-like cancer cells. Cancer Res. 2007, 67, 4827–4833. [Google Scholar] [CrossRef]
- Yin, W.; Xiang, D.; Wang, T.; Zhang, Y.; Pham, C.V.; Zhou, S.; Jiang, G.; Hou, Y.; Zhu, Y.; Han, Y.; et al. The inhibition of ABCB1/MDR1 or ABCG2/BCRP enables doxorubicin to eliminate liver cancer stem cells. Sci. Rep. 2021, 11, 10791. [Google Scholar] [CrossRef]
- Safa, A.R. Resistance to drugs and cell death in cancer stem cells (CSCs). J. Transl. Sci. 2020, 6, 341. [Google Scholar] [CrossRef]
- Lu, J.F.; Pokharel, D.; Bebawy, M. MRP1 and its role in anticancer drug resistance. Drug Metab. Rev. 2015, 47, 406–419. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, A.C.; Cloos, J.; Lemos, C.; Stam, R.W.; Kaspers, G.J.L.; Jansen, G.; Peters, G.J. Ex vivo resistance in childhood acute lymphoblastic leukemia: Correlations between BCRP, MRP1, MRP4 and MRP5 ABC transporter expression and intracellular methotrexate polyglutamate accumulation. Leuk. Res. 2019, 79, 45–51. [Google Scholar] [CrossRef] [PubMed]
- El-Khattouti, A.; Sheehan, N.T.; Monico, J.; Drummond, H.A.; Haikel, Y.; Brodell, R.T.; Megahed, M.; Hassan, M. CD133(+) melanoma subpopulation acquired resistance to caffeic acid phenethyl ester-induced apoptosis is attributed to the elevated expression of ABCB5: Significance for melanoma treatment. Cancer Lett. 2015, 357, 83–104. [Google Scholar] [CrossRef]
- Sugano, T.; Seike, M.; Noro, R.; Soeno, C.; Chiba, M.; Zou, F.; Nakamichi, S.; Nishijima, N.; Matsumoto, M.; Miyanaga, A.; et al. Inhibition of ABCB1 Overcomes Cancer Stem Cell-like Properties and Acquired Resistance to MET Inhibitors in Non-Small Cell Lung Cancer. Mol. Cancer Ther. 2015, 14, 2433–2440. [Google Scholar] [CrossRef] [PubMed]
- Maugeri-Sacca, M.; Bartucci, M.; De Maria, R. DNA damage repair pathways in cancer stem cells. Mol. Cancer Ther. 2012, 11, 1627–1636. [Google Scholar] [CrossRef] [PubMed]
- Manic, G.; Musella, M.; Corradi, F.; Sistigu, A.; Vitale, S.; Soliman Abdel Rehim, S.; Mattiello, L.; Malacaria, E.; Galassi, C.; Signore, M.; et al. Control of replication stress and mitosis in colorectal cancer stem cells through the interplay of PARP1, MRE11 and RAD51. Cell Death Differ. 2021, 28, 2060–2082. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Burness, M.L.; Martin-Trevino, R.; Guy, J.; Bai, S.; Harouaka, R.; Brooks, M.D.; Shang, L.; Fox, A.; Luther, T.K.; et al. RAD51 Mediates Resistance of Cancer Stem Cells to PARP Inhibition in Triple-Negative Breast Cancer. Clin. Cancer Res. 2017, 23, 514–522. [Google Scholar] [CrossRef]
- Turdo, A.; Gaggianesi, M.; Di Franco, S.; Veschi, V.; D’Accardo, C.; Porcelli, G.; Lo Iacono, M.; Pillitteri, I.; Verona, F.; Militello, G.; et al. Effective targeting of breast cancer stem cells by combined inhibition of Sam68 and Rad51. Oncogene 2022, 41, 2196–2209. [Google Scholar] [CrossRef]
- Bao, S.; Wu, Q.; McLendon, R.E.; Hao, Y.; Shi, Q.; Hjelmeland, A.B.; Dewhirst, M.W.; Bigner, D.D.; Rich, J.N. Glioma stem cells promote radioresistance by preferential activation of the DNA damage response. Nature 2006, 444, 756–760. [Google Scholar] [CrossRef]
- Grzybowska-Izydorczyk, O.; Cebula, B.; Robak, T.; Smolewski, P. Expression and prognostic significance of the inhibitor of apoptosis protein (IAP) family and its antagonists in chronic lymphocytic leukaemia. Eur. J. Cancer 2010, 46, 800–810. [Google Scholar] [CrossRef]
- Eckelman, B.P.; Salvesen, G.S.; Scott, F.L. Human inhibitor of apoptosis proteins: Why XIAP is the black sheep of the family. EMBO Rep. 2006, 7, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.R.; Ji, S.Y.; Mia-Jan, K.; Cho, M.Y. Chemoresistance of CD133(+) colon cancer may be related with increased survivin expression. Biochem. Biophys. Res. Commun. 2015, 463, 229–234. [Google Scholar] [CrossRef] [PubMed]
- AlShamaileh, H.; Wang, T.; Xiang, D.; Yin, W.; Tran, P.H.; Barrero, R.A.; Zhang, P.Z.; Li, Y.; Kong, L.; Liu, K.; et al. Aptamer-mediated survivin RNAi enables 5-fluorouracil to eliminate colorectal cancer stem cells. Sci. Rep. 2017, 7, 5898. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Yu, Y.; Li, Z.L.; Chen, M.Y.; Deng, R.; Huang, X.; Wang, G.F.; Zhang, M.X.; Yang, Q.; Ravichandran, S.; et al. XIAP Limits Autophagic Degradation of Sox2 and Is A Therapeutic Target in Nasopharyngeal Carcinoma Stem Cells. Theranostics 2018, 8, 1494–1510. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.H.; Scadden, D.T. Harnessing the apoptotic programs in cancer stem-like cells. EMBO Rep. 2015, 16, 1084–1098. [Google Scholar] [CrossRef] [PubMed]
- Lagadinou, E.D.; Sach, A.; Callahan, K.; Rossi, R.M.; Neering, S.J.; Minhajuddin, M.; Ashton, J.M.; Pei, S.; Grose, V.; O’Dwyer, K.M.; et al. BCL-2 inhibition targets oxidative phosphorylation and selectively eradicates quiescent human leukemia stem cells. Cell Stem Cell 2013, 12, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Pollyea, D.A.; Stevens, B.M.; Jones, C.L.; Winters, A.; Pei, S.; Minhajuddin, M.; D’Alessandro, A.; Culp-Hill, R.; Riemondy, K.A.; Gillen, A.E.; et al. Venetoclax with azacitidine disrupts energy metabolism and targets leukemia stem cells in patients with acute myeloid leukemia. Nat. Med. 2018, 24, 1859–1866. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Chen, Q.; Li, Y.; Lei, G.; Scott, A.; Huo, L.; Li, C.Y.; Estrella, J.S.; Correa, A.; Pizzi, M.P.; et al. Targeting cancer stem cells with a pan-BCL-2 inhibitor in preclinical and clinical settings in patients with gastroesophageal carcinoma. Gut 2021, 70, 2238–2248. [Google Scholar] [CrossRef]
- Diehn, M.; Cho, R.W.; Lobo, N.A.; Kalisky, T.; Dorie, M.J.; Kulp, A.N.; Qian, D.; Lam, J.S.; Ailles, L.E.; Wong, M.; et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature 2009, 458, 780–783. [Google Scholar] [CrossRef]
- Zanoni, M.; Bravaccini, S.; Fabbri, F.; Arienti, C. Emerging Roles of Aldehyde Dehydrogenase Isoforms in Anti-cancer Therapy Resistance. Front. Med. 2022, 9, 795762. [Google Scholar] [CrossRef] [PubMed]
- Emmink, B.L.; Verheem, A.; Van Houdt, W.J.; Steller, E.J.; Govaert, K.M.; Pham, T.V.; Piersma, S.R.; Borel Rinkes, I.H.; Jimenez, C.R.; Kranenburg, O. The secretome of colon cancer stem cells contains drug-metabolizing enzymes. J. Proteomics 2013, 91, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.; Pierscianek, D.; El Hindy, N.; Ahmadipour, Y.; Keyvani, K.; Sure, U.; Zhu, Y. The predominant expression of cancer stem cell marker ALDH1A3 in tumor infiltrative area is associated with shorter overall survival of human glioblastoma. BMC Cancer 2020, 20, 672. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Shi, P.; Zhao, G.; Xu, J.; Peng, W.; Zhang, J.; Zhang, G.; Wang, X.; Dong, Z.; Chen, F.; et al. Targeting cancer stem cell pathways for cancer therapy. Signal Transduct. Target Ther. 2020, 5, 8. [Google Scholar] [CrossRef] [PubMed]
- De Sousa, E.M.F.; Vermeulen, L. Wnt Signaling in Cancer Stem Cell Biology. Cancers 2016, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- Barker, N.; Ridgway, R.A.; van Es, J.H.; van de Wetering, M.; Begthel, H.; van den Born, M.; Danenberg, E.; Clarke, A.R.; Sansom, O.J.; Clevers, H. Crypt stem cells as the cells-of-origin of intestinal cancer. Nature 2009, 457, 608–611. [Google Scholar] [CrossRef]
- Vermeulen, L.; De Sousa, E.M.F.; van der Heijden, M.; Cameron, K.; de Jong, J.H.; Borovski, T.; Tuynman, J.B.; Todaro, M.; Merz, C.; Rodermond, H.; et al. Wnt activity defines colon cancer stem cells and is regulated by the microenvironment. Nat. Cell Biol. 2010, 12, 468–476. [Google Scholar] [CrossRef]
- Fan, Z.; Duan, J.; Wang, L.; Xiao, S.; Li, L.; Yan, X.; Yao, W.; Wu, L.; Zhang, S.; Zhang, Y.; et al. PTK2 promotes cancer stem cell traits in hepatocellular carcinoma by activating Wnt/beta-catenin signaling. Cancer Lett. 2019, 450, 132–143. [Google Scholar] [CrossRef]
- Lu, H.; Ju, D.D.; Yang, G.D.; Zhu, L.Y.; Yang, X.M.; Li, J.; Song, W.W.; Wang, J.H.; Zhang, C.C.; Zhang, Z.G.; et al. Targeting cancer stem cell signature gene SMOC-2 Overcomes chemoresistance and inhibits cell proliferation of endometrial carcinoma. EBioMedicine 2019, 40, 276–289. [Google Scholar] [CrossRef]
- Yoon, C.; Park, D.J.; Schmidt, B.; Thomas, N.J.; Lee, H.J.; Kim, T.S.; Janjigian, Y.Y.; Cohen, D.J.; Yoon, S.S. CD44 expression denotes a subpopulation of gastric cancer cells in which Hedgehog signaling promotes chemotherapy resistance. Clin. Cancer Res. 2014, 20, 3974–3988. [Google Scholar] [CrossRef]
- Zhu, R.; Gires, O.; Zhu, L.; Liu, J.; Li, J.; Yang, H.; Ju, G.; Huang, J.; Ge, W.; Chen, Y.; et al. TSPAN8 promotes cancer cell stemness via activation of sonic Hedgehog signaling. Nat. Commun. 2019, 10, 2863. [Google Scholar] [CrossRef]
- Bai, X.Y.; Zhang, X.C.; Yang, S.Q.; An, S.J.; Chen, Z.H.; Su, J.; Xie, Z.; Gou, L.Y.; Wu, Y.L. Blockade of Hedgehog Signaling Synergistically Increases Sensitivity to Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors in Non-Small-Cell Lung Cancer Cell Lines. PLoS ONE 2016, 11, e0149370. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Mathur, A.; Zhang, Y.; Xi, S.; Atay, S.; Hong, J.A.; Datrice, N.; Upham, T.; Kemp, C.D.; Ripley, R.T.; et al. Mithramycin represses basal and cigarette smoke-induced expression of ABCG2 and inhibits stem cell signaling in lung and esophageal cancer cells. Cancer Res. 2012, 72, 4178–4192. [Google Scholar] [CrossRef] [PubMed]
- Massague, J. TGFbeta in Cancer. Cell 2008, 134, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.A.; Chen, Y.F.; Bao, Y.; Mahara, S.; Yatim, S.; Oguz, G.; Lee, P.L.; Feng, M.; Cai, Y.; Tan, E.Y.; et al. Hypoxic tumor microenvironment activates GLI2 via HIF-1alpha and TGF-beta2 to promote chemoresistance in colorectal cancer. Proc. Natl. Acad. Sci. USA 2018, 115, E5990–E5999. [Google Scholar] [CrossRef] [PubMed]
- Akhurst, R.J.; Hata, A. Targeting the TGFbeta signalling pathway in disease. Nat. Rev. Drug Discov. 2012, 11, 790–811. [Google Scholar] [CrossRef]
- Asiedu, M.K.; Ingle, J.N.; Behrens, M.D.; Radisky, D.C.; Knutson, K.L. TGFbeta/TNF(alpha)-mediated epithelial-mesenchymal transition generates breast cancer stem cells with a claudin-low phenotype. Cancer Res. 2011, 71, 4707–4719. [Google Scholar] [CrossRef]
- Naka, K.; Hoshii, T.; Muraguchi, T.; Tadokoro, Y.; Ooshio, T.; Kondo, Y.; Nakao, S.; Motoyama, N.; Hirao, A. TGF-beta-FOXO signalling maintains leukaemia-initiating cells in chronic myeloid leukaemia. Nature 2010, 463, 676–680. [Google Scholar] [CrossRef]
- Verona, F.; Pantina, V.D.; Modica, C.; Lo Iacono, M.; D’Accardo, C.; Porcelli, G.; Cricchio, D.; Turdo, A.; Gaggianesi, M.; Di Franco, S.; et al. Targeting epigenetic alterations in cancer stem cells. Front. Mol. Med. 2022, 2, 882. [Google Scholar] [CrossRef]
- Wajapeyee, N.; Gupta, R. Epigenetic Alterations and Mechanisms That Drive Resistance to Targeted Cancer Therapies. Cancer Res. 2021, 81, 5589–5595. [Google Scholar] [CrossRef]
- Di Franco, S.; Bianca, P.; Sardina, D.S.; Turdo, A.; Gaggianesi, M.; Veschi, V.; Nicotra, A.; Mangiapane, L.R.; Lo Iacono, M.; Pillitteri, I.; et al. Adipose stem cell niche reprograms the colorectal cancer stem cell metastatic machinery. Nat. Commun. 2021, 12, 5006. [Google Scholar] [CrossRef]
- Taylor, W.F.; Jabbarzadeh, E. The use of natural products to target cancer stem cells. Am. J. Cancer Res. 2017, 7, 1588–1605. [Google Scholar] [PubMed]
- Dyshlovoy, S.A. Recent Updates on Marine Cancer-Preventive Compounds. Mar. Drugs 2021, 19, 558. [Google Scholar] [CrossRef] [PubMed]
- Deldar Abad Paskeh, M.; Asadi, S.; Zabolian, A.; Saleki, H.; Khoshbakht, M.A.; Sabet, S.; Naghdi, M.J.; Hashemi, M.; Hushmandi, K.; Ashrafizadeh, M.; et al. Targeting Cancer Stem Cells by Dietary Agents: An Important Therapeutic Strategy against Human Malignancies. Int. J. Mol. Sci. 2021, 22, 1669. [Google Scholar] [CrossRef] [PubMed]
- Stratton, C.F.; Newman, D.J.; Tan, D.S. Cheminformatic comparison of approved drugs from natural product versus synthetic origins. Bioorg. Med. Chem. Lett. 2015, 25, 4802–4807. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.S.; Yang, S.F.; Sethi, G.; Hu, D.N. Natural bioactives in cancer treatment and prevention. Biomed. Res. Int. 2015, 2015, 182835. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, B.M.F.; Cardoso, D.S.P.; Ferreira, M.-J.U. Overcoming Multidrug Resistance: Flavonoid and Terpenoid Nitrogen-Containing Derivatives as ABC Transporter Modulators. Molecules 2020, 25, 3364. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.J.; Yen, G.C. Chemopreventive effects of dietary phytochemicals against cancer invasion and metastasis: Phenolic acids, monophenol, polyphenol, and their derivatives. Cancer Treat. Rev. 2012, 38, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Md Sakib Hossain, D.; Mohanty, S.; Sankar Sen, G.; Chattopadhyay, S.; Banerjee, S.; Chakraborty, J.; Das, K.; Sarkar, D.; Das, T.; et al. Curcumin reverses T cell-mediated adaptive immune dysfunctions in tumor-bearing hosts. Cell Mol. Immunol. 2010, 7, 306–315. [Google Scholar] [CrossRef]
- Lev-Ari, S.; Zinger, H.; Kazanov, D.; Yona, D.; Ben-Yosef, R.; Starr, A.; Figer, A.; Arber, N. Curcumin synergistically potentiates the growth inhibitory and pro-apoptotic effects of celecoxib in pancreatic adenocarcinoma cells. Biomed. Pharmacother. 2005, 59 (Suppl. S2), S276–S280. [Google Scholar] [CrossRef]
- Kang, H.J.; Lee, S.H.; Price, J.E.; Kim, L.S. Curcumin suppresses the paclitaxel-induced nuclear factor-kappaB in breast cancer cells and potentiates the growth inhibitory effect of paclitaxel in a breast cancer nude mice model. Breast J. 2009, 15, 223–229. [Google Scholar] [CrossRef]
- Zoi, V.; Galani, V.; Lianos, G.D.; Voulgaris, S.; Kyritsis, A.P.; Alexiou, G.A. The Role of Curcumin in Cancer Treatment. Biomedicines 2021, 9, 1086. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.G.; Veena, M.S.; Basak, S.K.; Han, E.; Tajima, T.; Gjertson, D.W.; Starr, J.; Eidelman, O.; Pollard, H.B.; Srivastava, M.; et al. Curcumin treatment suppresses IKKbeta kinase activity of salivary cells of patients with head and neck cancer: A pilot study. Clin. Cancer Res. 2011, 17, 5953–5961. [Google Scholar] [CrossRef] [PubMed]
- Marquardt, J.U.; Gomez-Quiroz, L.; Arreguin Camacho, L.O.; Pinna, F.; Lee, Y.H.; Kitade, M.; Dominguez, M.P.; Castven, D.; Breuhahn, K.; Conner, E.A.; et al. Curcumin effectively inhibits oncogenic NF-kappaB signaling and restrains stemness features in liver cancer. J. Hepatol. 2015, 63, 661–669. [Google Scholar] [CrossRef]
- Wu, L.; Guo, L.; Liang, Y.; Liu, X.; Jiang, L.; Wang, L. Curcumin suppresses stem-like traits of lung cancer cells via inhibiting the JAK2/STAT3 signaling pathway. Oncol. Rep. 2015, 34, 3311–3317. [Google Scholar] [CrossRef]
- Zhu, J.Y.; Yang, X.; Chen, Y.; Jiang, Y.; Wang, S.J.; Li, Y.; Wang, X.Q.; Meng, Y.; Zhu, M.M.; Ma, X.; et al. Curcumin Suppresses Lung Cancer Stem Cells via Inhibiting Wnt/beta-catenin and Sonic Hedgehog Pathways. Phytother. Res. 2017, 31, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Kakarala, M.; Brenner, D.E.; Korkaya, H.; Cheng, C.; Tazi, K.; Ginestier, C.; Liu, S.; Dontu, G.; Wicha, M.S. Targeting breast stem cells with the cancer preventive compounds curcumin and piperine. Breast Cancer Res. Treat. 2010, 122, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Zhang, X.; Zheng, X.; Chen, Y.; Xuan, Z.; Huang, P. Curcumin suppresses LGR5(+) colorectal cancer stem cells by inducing autophagy and via repressing TFAP2A-mediated ECM pathway. J. Nat. Med. 2021, 75, 590–601. [Google Scholar] [CrossRef]
- Baharuddin, P.; Satar, N.; Fakiruddin, K.S.; Zakaria, N.; Lim, M.N.; Yusoff, N.M.; Zakaria, Z.; Yahaya, B.H. Curcumin improves the efficacy of cisplatin by targeting cancer stem-like cells through p21 and cyclin D1-mediated tumour cell inhibition in non-small cell lung cancer cell lines. Oncol. Rep. 2016, 35, 13–25. [Google Scholar] [CrossRef]
- Khan, A.Q.; Ahmed, E.I.; Elareer, N.; Fathima, H.; Prabhu, K.S.; Siveen, K.S.; Kulinski, M.; Azizi, F.; Dermime, S.; Ahmad, A.; et al. Curcumin-Mediated Apoptotic Cell Death in Papillary Thyroid Cancer and Cancer Stem-Like Cells through Targeting of the JAK/STAT3 Signaling Pathway. Int. J. Mol. Sci. 2020, 21, 438. [Google Scholar] [CrossRef]
- Shaikh, S.; Shaikh, J.; Naba, Y.S.; Doke, K.; Ahmed, K.; Yusufi, M. Curcumin: Reclaiming the lost ground against cancer resistance. Cancer Drug Resist. 2021, 4, 298–320. [Google Scholar] [CrossRef]
- Gusman, J.; Malonne, H.; Atassi, G. A reappraisal of the potential chemopreventive and chemotherapeutic properties of resveratrol. Carcinogenesis 2001, 22, 1111–1117. [Google Scholar] [CrossRef]
- Gescher, A.J. Resveratrol from red grapes-pedestrian polyphenol or useful anticancer agent? Planta Med. 2008, 74, 1651–1655. [Google Scholar] [CrossRef]
- Jang, M.; Cai, L.; Udeani, G.O.; Slowing, K.V.; Thomas, C.F.; Beecher, C.W.; Fong, H.H.; Farnsworth, N.R.; Kinghorn, A.D.; Mehta, R.G.; et al. Cancer chemopreventive activity of resveratrol, a natural product derived from grapes. Science 1997, 275, 218–220. [Google Scholar] [CrossRef]
- Peng, L.; Jiang, D. Resveratrol eliminates cancer stem cells of osteosarcoma by STAT3 pathway inhibition. PLoS ONE 2018, 13, e0205918. [Google Scholar] [CrossRef]
- Ferraresi, A.; Esposito, A.; Girone, C.; Vallino, L.; Salwa, A.; Ghezzi, I.; Thongchot, S.; Vidoni, C.; Dhanasekaran, D.N.; Isidoro, C. Resveratrol Contrasts LPA-Induced Ovarian Cancer Cell Migration and Platinum Resistance by Rescuing Hedgehog-Mediated Autophagy. Cells 2021, 10, 3213. [Google Scholar] [CrossRef]
- Qin, T.; Cheng, L.; Xiao, Y.; Qian, W.; Li, J.; Wu, Z.; Wang, Z.; Xu, Q.; Duan, W.; Wong, L.; et al. NAF-1 Inhibition by Resveratrol Suppresses Cancer Stem Cell-Like Properties and the Invasion of Pancreatic Cancer. Front. Oncol. 2020, 10, 1038. [Google Scholar] [CrossRef]
- Huang, L.; Zhang, S.; Zhou, J.; Li, X. Effect of resveratrol on drug resistance in colon cancer chemotherapy. RSC Adv. 2019, 9, 2572–2580. [Google Scholar] [CrossRef]
- Fu, Y.; Chang, H.; Peng, X.; Bai, Q.; Yi, L.; Zhou, Y.; Zhu, J.; Mi, M. Resveratrol inhibits breast cancer stem-like cells and induces autophagy via suppressing Wnt/beta-catenin signaling pathway. PLoS ONE 2014, 9, e102535. [Google Scholar] [CrossRef]
- Blanquer-Rossello, M.D.; Hernandez-Lopez, R.; Roca, P.; Oliver, J.; Valle, A. Resveratrol induces mitochondrial respiration and apoptosis in SW620 colon cancer cells. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 431–440. [Google Scholar] [CrossRef]
- Juan, M.E.; Alfaras, I.; Planas, J.M. Colorectal cancer chemoprevention by trans-resveratrol. Pharmacol.Res. 2012, 65, 584–591. [Google Scholar] [CrossRef]
- Suh, J.; Kim, D.H.; Surh, Y.J. Resveratrol suppresses migration, invasion and stemness of human breast cancer cells by interfering with tumor-stromal cross-talk. Arch. Biochem. Biophys. 2018, 643, 62–71. [Google Scholar] [CrossRef]
- Singh, B.N.; Shankar, S.; Srivastava, R.K. Green tea catechin, epigallocatechin-3-gallate (EGCG): Mechanisms, perspectives and clinical applications. Biochem. Pharmacol. 2011, 82, 1807–1821. [Google Scholar] [CrossRef]
- Landis-Piwowar, K.R.; Huo, C.; Chen, D.; Milacic, V.; Shi, G.; Chan, T.H.; Dou, Q.P. A novel prodrug of the green tea polyphenol (-)-epigallocatechin-3-gallate as a potential anticancer agent. Cancer Res. 2007, 67, 4303–4310. [Google Scholar] [CrossRef]
- Yang, C.S.; Wang, H. Cancer Preventive Activities of Tea Catechins. Molecules 2016, 21, 1679. [Google Scholar] [CrossRef]
- Naujokat, C.; McKee, D.L. The “Big Five” Phytochemicals Targeting Cancer Stem Cells: Curcumin, EGCG, Sulforaphane, Resveratrol and Genistein. Curr. Med. Chem. 2021, 28, 4321–4342. [Google Scholar] [CrossRef]
- Fujiki, H.; Sueoka, E.; Rawangkan, A.; Suganuma, M. Human cancer stem cells are a target for cancer prevention using (-)-epigallocatechin gallate. J. Cancer Res. Clin. Oncol. 2017, 143, 2401–2412. [Google Scholar] [CrossRef]
- Luo, K.W.; Xia, J.; Cheng, B.H.; Gao, H.C.; Fu, L.W.; Luo, X.L. Tea polyphenol EGCG inhibited colorectal-cancer-cell proliferation and migration via downregulation of STAT3. Gastroenterol. Rep. 2021, 9, 59–70. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.Q.; Zhang, Q.; Zhu, J.Y.; Li, Y.; Xie, C.F.; Li, X.T.; Wu, J.S.; Geng, S.S.; Zhong, C.Y.; et al. (-)-Epigallocatechin-3-Gallate Inhibits Colorectal Cancer Stem Cells by Suppressing Wnt/beta-Catenin Pathway. Nutrients 2017, 9, 572. [Google Scholar] [CrossRef]
- Toden, S.; Tran, H.M.; Tovar-Camargo, O.A.; Okugawa, Y.; Goel, A. Epigallocatechin-3-gallate targets cancer stem-like cells and enhances 5-fluorouracil chemosensitivity in colorectal cancer. Oncotarget 2016, 7, 16158–16171. [Google Scholar] [CrossRef]
- Jiang, P.; Xu, C.; Zhang, P.; Ren, J.; Mageed, F.; Wu, X.; Chen, L.; Zeb, F.; Feng, Q.; Li, S. Epigallocatechin3gallate inhibits selfrenewal ability of lung cancer stemlike cells through inhibition of CLOCK. Int. J. Mol. Med. 2020, 46, 2216–2224. [Google Scholar] [CrossRef]
- Zhu, J.; Jiang, Y.; Yang, X.; Wang, S.; Xie, C.; Li, X.; Li, Y.; Chen, Y.; Wang, X.; Meng, Y.; et al. Wnt/beta-catenin pathway mediates (-)-Epigallocatechin-3-gallate (EGCG) inhibition of lung cancer stem cells. Biochem. Biophys. Res. Commun. 2017, 482, 15–21. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, C.; Sanchez-Quesada, C.; Gaforio, J.J. Dietary Flavonoids as Cancer Chemopreventive Agents: An Updated Review of Human Studies. Antioxidants 2019, 8, 137. [Google Scholar] [CrossRef]
- Atrahimovich, D.; Vaya, J.; Khatib, S. The effects and mechanism of flavonoid-rePON1 interactions. Structure-activity relationship study. Bioorg. Med. Chem. 2013, 21, 3348–3355. [Google Scholar] [CrossRef]
- Montales, M.T.; Rahal, O.M.; Kang, J.; Rogers, T.J.; Prior, R.L.; Wu, X.; Simmen, R.C. Repression of mammosphere formation of human breast cancer cells by soy isoflavone genistein and blueberry polyphenolic acids suggests diet-mediated targeting of cancer stem-like/progenitor cells. Carcinogenesis 2012, 33, 652–660. [Google Scholar] [CrossRef]
- Nogata, Y.; Sakamoto, K.; Shiratsuchi, H.; Ishii, T.; Yano, M.; Ohta, H. Flavonoid composition of fruit tissues of citrus species. Biosci. Biotechnol. Biochem. 2006, 70, 178–192. [Google Scholar] [CrossRef]
- Meiyanto, E.; Hermawan, A.; Anindyajati. Natural products for cancer-targeted therapy: Citrus flavonoids as potent chemopreventive agents. Asian Pac. J. Cancer Prev. 2012, 13, 427–436. [Google Scholar] [CrossRef]
- Murakami, A.; Nakamura, Y.; Torikai, K.; Tanaka, T.; Koshiba, T.; Koshimizu, K.; Kuwahara, S.; Takahashi, Y.; Ogawa, K.; Yano, M.; et al. Inhibitory effect of citrus nobiletin on phorbol ester-induced skin inflammation, oxidative stress, and tumor promotion in mice. Cancer Res. 2000, 60, 5059–5066. [Google Scholar]
- Nabekura, T.; Yamaki, T.; Kitagawa, S. Effects of chemopreventive citrus phytochemicals on human P-glycoprotein and multidrug resistance protein 1. Eur. J. Pharmacol. 2008, 600, 45–49. [Google Scholar] [CrossRef]
- Ma, W.; Feng, S.; Yao, X.; Yuan, Z.; Liu, L.; Xie, Y. Nobiletin enhances the efficacy of chemotherapeutic agents in ABCB1 overexpression cancer cells. Sci. Rep. 2015, 5, 18789. [Google Scholar] [CrossRef]
- Han, S.H.; Han, J.H.; Chun, W.J.; Lee, S.S.; Kim, H.S.; Lee, J.W. Nobiletin Inhibits Non-Small-Cell Lung Cancer by Inactivating WNT/beta-Catenin Signaling through Downregulating miR-15-5p. Evid.-Based Complement. Alternat. Med. 2021, 2021, 7782963. [Google Scholar] [CrossRef]
- Turdo, A.; Glaviano, A.; Pepe, G.; Calapa, F.; Raimondo, S.; Fiori, M.E.; Carbone, D.; Basilicata, M.G.; Di Sarno, V.; Ostacolo, C.; et al. Nobiletin and Xanthohumol Sensitize Colorectal Cancer Stem Cells to Standard Chemotherapy. Cancers 2021, 13, 3927. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Gupta, S. Apigenin: A promising molecule for cancer prevention. Pharm. Res. 2010, 27, 962–978. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Huang, K.M. In vitro anti-inflammatory effect of apigenin in the Helicobacter pylori-infected gastric adenocarcinoma cells. Food Chem. Toxicol. 2013, 53, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, S.; Turkekul, K.; Serttas, R.; Erdogan, Z. The natural flavonoid apigenin sensitizes human CD44(+) prostate cancer stem cells to cisplatin therapy. Biomed. Pharmacother. 2017, 88, 210–217. [Google Scholar] [CrossRef]
- Li, Y.W.; Xu, J.; Zhu, G.Y.; Huang, Z.J.; Lu, Y.; Li, X.Q.; Wang, N.; Zhang, F.X. Apigenin suppresses the stem cell-like properties of triple-negative breast cancer cells by inhibiting YAP/TAZ activity. Cell Death Discov. 2018, 4, 105. [Google Scholar] [CrossRef]
- Li, Y.; Chen, X.; He, W.; Xia, S.; Jiang, X.; Li, X.; Bai, J.; Li, N.; Chen, L.; Yang, B. Apigenin Enhanced Antitumor Effect of Cisplatin in Lung Cancer via Inhibition of Cancer Stem Cells. Nutr. Cancer 2021, 73, 1489–1497. [Google Scholar] [CrossRef]
- Cao, L.; Yang, Y.; Ye, Z.; Lin, B.; Zeng, J.; Li, C.; Liang, T.; Zhou, K.; Li, J. Quercetin3methyl ether suppresses human breast cancer stem cell formation by inhibiting the Notch1 and PI3K/Akt signaling pathways. Int. J. Mol. Med. 2018, 42, 1625–1636. [Google Scholar] [CrossRef]
- Li, X.; Zhou, N.; Wang, J.; Liu, Z.; Wang, X.; Zhang, Q.; Liu, Q.; Gao, L.; Wang, R. Quercetin suppresses breast cancer stem cells (CD44(+)/CD24(-)) by inhibiting the PI3K/Akt/mTOR-signaling pathway. Life Sci. 2018, 196, 56–62. [Google Scholar] [CrossRef]
- Wang, R.; Yang, L.; Li, S.; Ye, D.; Yang, L.; Liu, Q.; Zhao, Z.; Cai, Q.; Tan, J.; Li, X. Quercetin Inhibits Breast Cancer Stem Cells via Downregulation of Aldehyde Dehydrogenase 1A1 (ALDH1A1), Chemokine Receptor Type 4 (CXCR4), Mucin 1 (MUC1), and Epithelial Cell Adhesion Molecule (EpCAM). Med. Sci. Monit. 2018, 24, 412–420. [Google Scholar] [CrossRef]
- Cao, C.; Sun, L.; Mo, W.; Sun, L.; Luo, J.; Yang, Z.; Ran, Y. Quercetin Mediates beta-Catenin in Pancreatic Cancer Stem-Like Cells. Pancreas 2015, 44, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari-Movahed, M.; Jackson, G.; Farzaei, M.H.; Bishayee, A. A Systematic Review of the Preventive and Therapeutic Effects of Naringin Against Human Malignancies. Front. Pharmacol. 2021, 12, 639840. [Google Scholar] [CrossRef] [PubMed]
- Rauf, A.; Shariati, M.A.; Imran, M.; Bashir, K.; Khan, S.A.; Mitra, S.; Emran, T.B.; Badalova, K.; Uddin, M.S.; Mubarak, M.S.; et al. Comprehensive review on naringenin and naringin polyphenols as a potent anticancer agent. Environ. Sci. Pollut. Res. Int. 2022, 29, 31025–31041. [Google Scholar] [CrossRef]
- Stabrauskiene, J.; Kopustinskiene, D.M.; Lazauskas, R.; Bernatoniene, J. Naringin and Naringenin: Their Mechanisms of Action and the Potential Anticancer Activities. Biomedicines 2022, 10, 1686. [Google Scholar] [CrossRef] [PubMed]
- Hermawan, A.; Ikawati, M.; Jenie, R.I.; Khumaira, A.; Putri, H.; Nurhayati, I.P.; Angraini, S.M.; Muflikhasari, H.A. Identification of potential therapeutic target of naringenin in breast cancer stem cells inhibition by bioinformatics and in vitro studies. Saudi Pharm. J. 2021, 29, 12–26. [Google Scholar] [CrossRef]
- Martinez-Rodriguez, O.P.; Gonzalez-Torres, A.; Alvarez-Salas, L.M.; Hernandez-Sanchez, H.; Garcia-Perez, B.E.; Thompson-Bonilla, M.D.R.; Jaramillo-Flores, M.E. Effect of naringenin and its combination with cisplatin in cell death, proliferation and invasion of cervical cancer spheroids. RSC Adv. 2020, 11, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Burnett, J.P.; Lim, G.; Li, Y.; Shah, R.B.; Lim, R.; Paholak, H.J.; McDermott, S.P.; Sun, L.; Tsume, Y.; Bai, S.; et al. Sulforaphane enhances the anticancer activity of taxanes against triple negative breast cancer by killing cancer stem cells. Cancer Lett. 2017, 394, 52–64. [Google Scholar] [CrossRef]
- Hu, L.; Li, H.; Lee, E.D.; Grandis, J.R.; Bauman, J.E.; Johnson, D.E. Gene targets of sulforaphane in head and neck squamous cell carcinoma. Mol. Med. Rep. 2019, 20, 5335–5344. [Google Scholar] [CrossRef]
- Li, Q.Q.; Xie, Y.K.; Wu, Y.; Li, L.L.; Liu, Y.; Miao, X.B.; Liu, Q.Z.; Yao, K.T.; Xiao, G.H. Sulforaphane inhibits cancer stem-like cell properties and cisplatin resistance through miR-214-mediated downregulation of c-MYC in non-small cell lung cancer. Oncotarget 2017, 8, 12067–12080. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, T.; Korkaya, H.; Liu, S.; Lee, H.F.; Newman, B.; Yu, Y.; Clouthier, S.G.; Schwartz, S.J.; Wicha, M.S.; et al. Sulforaphane, a dietary component of broccoli/broccoli sprouts, inhibits breast cancer stem cells. Clin. Cancer Res. 2010, 16, 2580–2590. [Google Scholar] [CrossRef]
- Castro, N.P.; Rangel, M.C.; Merchant, A.S.; MacKinnon, G.; Cuttitta, F.; Salomon, D.S.; Kim, Y.S. Sulforaphane Suppresses the Growth of Triple-negative Breast Cancer Stem-like Cells In vitro and In vivo. Cancer Prev. Res. 2019, 12, 147–158. [Google Scholar] [CrossRef]
- Khan, N.; Syed, D.N.; Ahmad, N.; Mukhtar, H. Fisetin: A dietary antioxidant for health promotion. Antioxid. Redox Signal. 2013, 19, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Afaq, F.; Khusro, F.H.; Mustafa Adhami, V.; Suh, Y.; Mukhtar, H. Dual inhibition of phosphatidylinositol 3-kinase/Akt and mammalian target of rapamycin signaling in human nonsmall cell lung cancer cells by a dietary flavonoid fisetin. Int. J. Cancer 2012, 130, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Tabasum, S.; Singh, R.P. Fisetin suppresses migration, invasion and stem-cell-like phenotype of human non-small cell lung carcinoma cells via attenuation of epithelial to mesenchymal transition. Chem. Biol. Interact. 2019, 303, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Da Rocha, A.B.; Lopes, R.M.; Schwartsmann, G. Natural products in anticancer therapy. Curr. Opin. Pharmacol. 2001, 1, 364–369. [Google Scholar] [CrossRef]
- Cao, D.; Zhu, G.Y.; Lu, Y.; Yang, A.; Chen, D.; Huang, H.J.; Peng, S.X.; Chen, L.W.; Li, Y.W. Luteolin suppresses epithelial-mesenchymal transition and migration of triple-negative breast cancer cells by inhibiting YAP/TAZ activity. Biomed. Pharmacother. 2020, 129, 110462. [Google Scholar] [CrossRef]
- Tsai, K.J.; Tsai, H.Y.; Tsai, C.C.; Chen, T.Y.; Hsieh, T.H.; Chen, C.L.; Mbuyisa, L.; Huang, Y.B.; Lin, M.W. Luteolin Inhibits Breast Cancer Stemness and Enhances Chemosensitivity through the Nrf2-Mediated Pathway. Molecules 2021, 26, 6452. [Google Scholar] [CrossRef]
- Tsai, P.H.; Cheng, C.H.; Lin, C.Y.; Huang, Y.T.; Lee, L.T.; Kandaswami, C.C.; Lin, Y.C.; Lee, K.P.; Hung, C.C.; Hwang, J.J.; et al. Dietary Flavonoids Luteolin and Quercetin Suppressed Cancer Stem Cell Properties and Metastatic Potential of Isolated Prostate Cancer Cells. Anticancer. Res. 2016, 36, 6367–6380. [Google Scholar] [CrossRef]
- Tu, D.G.; Lin, W.T.; Yu, C.C.; Lee, S.S.; Peng, C.Y.; Lin, T.; Yu, C.H. Chemotherapeutic effects of luteolin on radio-sensitivity enhancement and interleukin-6/signal transducer and activator of transcription 3 signaling repression of oral cancer stem cells. J. Formos Med. Assoc. 2016, 115, 1032–1038. [Google Scholar] [CrossRef]
- Meeran, S.M.; Katiyar, S.; Katiyar, S.K. Berberine-induced apoptosis in human prostate cancer cells is initiated by reactive oxygen species generation. Toxicol. Appl. Pharmacol. 2008, 229, 33–43. [Google Scholar] [CrossRef]
- Iizuka, N.; Miyamoto, K.; Okita, K.; Tangoku, A.; Hayashi, H.; Yosino, S.; Abe, T.; Morioka, T.; Hazama, S.; Oka, M. Inhibitory effect of Coptidis Rhizoma and berberine on the proliferation of human esophageal cancer cell lines. Cancer Lett. 2000, 148, 19–25. [Google Scholar] [CrossRef]
- Qing, Y.; Hu, H.; Liu, Y.; Feng, T.; Meng, W.; Jiang, L.; Sun, Y.; Yao, Y. Berberine induces apoptosis in human multiple myeloma cell line U266 through hypomethylation of p53 promoter. Cell. Biol. Int. 2014, 38, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Liu, Y.; Xue, Y.; Hu, H.; Ye, J.; Li, X.; Lu, Z.; Meng, F.; Liang, S. Berberine acts as a putative epigenetic modulator by affecting the histone code. Toxicol. In Vitro 2016, 36, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zeng, J.; Guo, Q.; Pu, K.; Yang, Y.; Chen, N.; Zhang, G.; Zhao, M.; Zheng, Q.; Tang, J.; et al. Berberine Suppresses Stemness and Tumorigenicity of Colorectal Cancer Stem-Like Cells by Inhibiting m(6)A Methylation. Front. Oncol. 2021, 11, 775418. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Sung, J.H.; Chung, N. Berberine diminishes side population and down-regulates stem cell-associated genes in the pancreatic cancer cell lines PANC-1 and MIA PaCa-2. Mol. Cell. Biochem. 2014, 394, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Yang, X.; Zhao, J.; Gao, M.; Zhang, M.; Shi, T.; Zhang, F.; Zheng, X.; Pan, Y.; Shao, D.; et al. Berberine inhibits chemotherapy-exacerbated ovarian cancer stem cell-like characteristics and metastasis through GLI1. Eur. J. Pharmacol. 2021, 895, 173887. [Google Scholar] [CrossRef]
- Naveen, C.R.; Gaikwad, S.; Agrawal-Rajput, R. Berberine induces neuronal differentiation through inhibition of cancer stemness and epithelial-mesenchymal transition in neuroblastoma cells. Phytomedicine 2016, 23, 736–744. [Google Scholar] [CrossRef]
- Camplejohn, R.S. A critical review of the use of vincristine (VCR) as a tumour cell synchronizing agent in cancer therapy. Cell Tissue Kinet. 1980, 13, 327–335. [Google Scholar] [CrossRef]
- Tu, Y.; Cheng, S.; Zhang, S.; Sun, H.; Xu, Z. Vincristine induces cell cycle arrest and apoptosis in SH-SY5Y human neuroblastoma cells. Int. J. Mol. Med. 2013, 31, 113–119. [Google Scholar] [CrossRef]
- Gingrich, R.D.; Armitage, J.O.; Burns, C.P. Treatment of adult acute lymphoblastic leukemia with cytosine arabinoside, vincristine, and prednisone. Cancer Treat. Rep. 1978, 62, 1389–1391. [Google Scholar]
- Gandhi, L.; Harding, M.W.; Neubauer, M.; Langer, C.J.; Moore, M.; Ross, H.J.; Johnson, B.E.; Lynch, T.J. A phase II study of the safety and efficacy of the multidrug resistance inhibitor VX-710 combined with doxorubicin and vincristine in patients with recurrent small cell lung cancer. Cancer 2007, 109, 924–932. [Google Scholar] [CrossRef]
- Gustavsson, B.; Carlsson, G.; Machover, D.; Petrelli, N.; Roth, A.; Schmoll, H.J.; Tveit, K.M.; Gibson, F. A review of the evolution of systemic chemotherapy in the management of colorectal cancer. Clin. Colorectal. Cancer 2015, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.W.; Dalton, W.S.; Mosley, K.; Dorr, R.T.; Salmon, S.E. Combination chemotherapy with cyclophosphamide, vincristine, adriamycin, and dexamethasone (CVAD) plus oral quinine and verapamil in patients with advanced breast cancer. Breast Cancer Res. Treat. 1997, 42, 7–14. [Google Scholar] [CrossRef]
- Moon, J.W.; Lee, S.K.; Lee, J.O.; Kim, J.H.; Kim, N.; Kim, J.; Kim, H.S.; Park, S.H. Demethylation of RUNX3 by vincristine in colorectal adenocarcinoma cells. Anticancer Res. 2014, 34, 133–140. [Google Scholar] [PubMed]
- Kimura, T.; Takabatake, Y.; Takahashi, A.; Isaka, Y. Chloroquine in cancer therapy: A double-edged sword of autophagy. Cancer Res. 2013, 73, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Cufi, S.; Vazquez-Martin, A.; Oliveras-Ferraros, C.; Martin-Castillo, B.; Vellon, L.; Menendez, J.A. Autophagy positively regulates the CD44+ CD24-/low breast cancer stem-like phenotype. Cell Cycle 2011, 10, 3871–3885. [Google Scholar] [CrossRef]
- Choi, D.S.; Blanco, E.; Kim, Y.S.; Rodriguez, A.A.; Zhao, H.; Huang, T.H.; Chen, C.L.; Jin, G.; Landis, M.D.; Burey, L.A.; et al. Chloroquine eliminates cancer stem cells through deregulation of Jak2 and DNMT1. Stem Cells 2014, 32, 2309–2323. [Google Scholar] [CrossRef]
- Liang, D.H.; Choi, D.S.; Ensor, J.E.; Kaipparettu, B.A.; Bass, B.L.; Chang, J.C. The autophagy inhibitor chloroquine targets cancer stem cells in triple negative breast cancer by inducing mitochondrial damage and impairing DNA break repair. Cancer Lett. 2016, 376, 249–258. [Google Scholar] [CrossRef]
- Balic, A.; Sorensen, M.D.; Trabulo, S.M.; Sainz, B., Jr.; Cioffi, M.; Vieira, C.R.; Miranda-Lorenzo, I.; Hidalgo, M.; Kleeff, J.; Erkan, M.; et al. Chloroquine targets pancreatic cancer stem cells via inhibition of CXCR4 and hedgehog signaling. Mol. Cancer Ther. 2014, 13, 1758–1771. [Google Scholar] [CrossRef]
- Yue, D.; Zhang, D.; Shi, X.; Liu, S.; Li, A.; Wang, D.; Qin, G.; Ping, Y.; Qiao, Y.; Chen, X.; et al. Chloroquine Inhibits Stemness of Esophageal Squamous Cell Carcinoma Cells Through Targeting CXCR4-STAT3 Pathway. Front. Oncol. 2020, 10, 311. [Google Scholar] [CrossRef]
- Lau, J.K.; Brown, K.C.; Dom, A.M.; Witte, T.R.; Thornhill, B.A.; Crabtree, C.M.; Perry, H.E.; Brown, J.M.; Ball, J.G.; Creel, R.G.; et al. Capsaicin induces apoptosis in human small cell lung cancer via the TRPV6 receptor and the calpain pathway. Apoptosis 2014, 19, 1190–1201. [Google Scholar] [CrossRef]
- Zhu, M.; Yu, X.; Zheng, Z.; Huang, J.; Yang, X.; Shi, H. Capsaicin suppressed activity of prostate cancer stem cells by inhibition of Wnt/beta-catenin pathway. Phytother. Res. 2020, 34, 817–824. [Google Scholar] [CrossRef]
- Shi, S.; Li, C.; Zhang, Y.; Deng, C.; Liu, W.; Du, J.; Li, Q.; Ji, Y.; Guo, L.; Liu, L.; et al. Dihydrocapsaicin Inhibits Cell Proliferation and Metastasis in Melanoma via Down-regulating beta-Catenin Pathway. Front. Oncol. 2021, 11, 648052. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.H.; Kim, Y.S.; Lim, S.C.; Hou, Y.F.; Chang, I.Y.; You, H.J. Dihydrocapsaicin (DHC), a saturated structural analog of capsaicin, induces autophagy in human cancer cells in a catalase-regulated manner. Autophagy 2008, 4, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Arya, R.; Bhutkar, S.; Dhulap, S.; Hirwani, R.R. Patent analysis as a tool for research planning: Study on natural based therapeutics against cancer stem cells. Recent Pat. Anticancer Drug Discov. 2015, 10, 72–86. [Google Scholar] [CrossRef]
- Schwartsmann, G. Marine organisms and other novel natural sources of new cancer drugs. Ann. Oncol. 2000, 11 (Suppl. S3), 235–243. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Parrino, B.; Barraja, P.; Spano, V.; Cirrincione, G.; Diana, P.; Maier, A.; Kelter, G.; Fiebig, H.H. Synthesis and antiproliferative activity of 2,5-bis(3’-indolyl)pyrroles, analogues of the marine alkaloid nortopsentin. Mar. Drugs 2013, 11, 643–654. [Google Scholar] [CrossRef]
- Cascioferro, S.; Attanzio, A.; Di Sarno, V.; Musella, S.; Tesoriere, L.; Cirrincione, G.; Diana, P.; Parrino, B. New 1,2,4-Oxadiazole Nortopsentin Derivatives with Cytotoxic Activity. Mar. Drugs 2019, 17, 35. [Google Scholar] [CrossRef]
- Di Franco, S.; Parrino, B.; Gaggianesi, M.; Pantina, V.D.; Bianca, P.; Nicotra, A.; Mangiapane, L.R.; Lo Iacono, M.; Ganduscio, G.; Veschi, V.; et al. CHK1 inhibitor sensitizes resistant colorectal cancer stem cells to nortopsentin. iScience 2021, 24, 102664. [Google Scholar] [CrossRef]
- Sirimangkalakitti, N.; Chamni, S.; Suwanborirux, K.; Chanvorachote, P. Renieramycin M Attenuates Cancer Stem Cell-like Phenotypes in H460 Lung Cancer Cells. Anticancer Res. 2017, 37, 615–621. [Google Scholar] [CrossRef]
- Peng, J.; Yuan, J.P.; Wu, C.F.; Wang, J.H. Fucoxanthin, a marine carotenoid present in brown seaweeds and diatoms: Metabolism and bioactivities relevant to human health. Mar. Drugs 2011, 9, 1806–1828. [Google Scholar] [CrossRef]
- Terasaki, M.; Maeda, H.; Miyashita, K.; Tanaka, T.; Miyamoto, S.; Mutoh, M. A marine bio-functional lipid, fucoxanthinol, attenuates human colorectal cancer stem-like cell tumorigenicity and sphere formation. J. Clin. Biochem. Nutr. 2017, 61, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Terasaki, M.; Mima, M.; Kudoh, S.; Endo, T.; Maeda, H.; Hamada, J.; Osada, K.; Miyashita, K.; Mutoh, M. Glycine and succinic acid are effective indicators of the suppression of epithelial-mesenchymal transition by fucoxanthinol in colorectal cancer stem-like cells. Oncol. Rep. 2018, 40, 414–424. [Google Scholar] [CrossRef] [PubMed]
- Vishchuk, O.S.; Ermakova, S.P.; Zvyagintseva, T.N. The fucoidans from brown algae of Far-Eastern seas: Anti-tumor activity and structure-function relationship. Food Chem. 2013, 141, 1211–1217. [Google Scholar] [CrossRef]
- Prendiville, J.; Crowther, D.; Thatcher, N.; Woll, P.J.; Fox, B.W.; McGown, A.; Testa, N.; Stern, P.; McDermott, R.; Potter, M.; et al. A phase I study of intravenous bryostatin 1 in patients with advanced cancer. Br. J. Cancer 1993, 68, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Philip, P.A.; Zonder, J.A. Pharmacology and clinical experience with bryostatin 1: A novel anticancer drug. Expert Opin. Investig. Drugs 1999, 8, 2189–2199. [Google Scholar] [CrossRef]
- Sztiller-Sikorska, M.; Koprowska, K.; Majchrzak, K.; Hartman, M.; Czyz, M. Natural compounds’ activity against cancer stem-like or fast-cycling melanoma cells. PLoS ONE 2014, 9, e90783. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, H.G.; Allan, E.K.; Mountford, J.C.; Richmond, L.; Harrison, S.; Elliott, M.A.; Holyoake, T.L. Enhanced CML stem cell elimination in vitro by bryostatin priming with imatinib mesylate. Exp. Hematol. 2005, 33, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Allenspach, E.J.; Maillard, I.; Aster, J.C.; Pear, W.S. Notch signaling in cancer. Cancer Biol. Ther. 2002, 1, 466–476. [Google Scholar] [CrossRef]
- Gudas, L.J.; Wagner, J.A. Retinoids regulate stem cell differentiation. J. Cell Physiol. 2011, 226, 322–330. [Google Scholar] [CrossRef]
- Ginestier, C.; Wicinski, J.; Cervera, N.; Monville, F.; Finetti, P.; Bertucci, F.; Wicha, M.S.; Birnbaum, D.; Charafe-Jauffret, E. Retinoid signaling regulates breast cancer stem cell differentiation. Cell Cycle 2009, 8, 3297–3302. [Google Scholar] [CrossRef]
- Karsy, M.; Albert, L.; Tobias, M.E.; Murali, R.; Jhanwar-Uniyal, M. All-trans retinoic acid modulates cancer stem cells of glioblastoma multiforme in an MAPK-dependent manner. Anticancer Res. 2010, 30, 4915–4920. [Google Scholar] [PubMed]
- Lim, Y.C.; Kang, H.J.; Kim, Y.S.; Choi, E.C. All-trans-retinoic acid inhibits growth of head and neck cancer stem cells by suppression of Wnt/beta-catenin pathway. Eur. J. Cancer 2012, 48, 3310–3318. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Wang, L.; Huang, H.; Li, X.; Wang, P.; Mi, K.; Cheng, J.; Liu, H.; Gu, C.; Huang, L.; et al. All-trans retinoic acid reduces cancer stem cell-like cell-mediated resistance to gefitinib in NSCLC adenocarcinoma cells. BMC Cancer 2020, 20, 315. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.H.; Kwak, J.; Jang, K.L. All-trans retinoic acid induces p53-depenent apoptosis in human hepatocytes by activating p14 expression via promoter hypomethylation. Cancer Lett. 2015, 362, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Kaufman-Szymczyk, A.; Majda, K.; Szulawska-Mroczek, A.; Fabianowska-Majewska, K.; Lubecka, K. Clofarabinephytochemical combination exposures in CML cells inhibit DNA methylation machinery, upregulate tumor suppressor genes and promote caspasedependent apoptosis. Mol. Med. Rep. 2019, 20, 3597–3608. [Google Scholar] [CrossRef] [PubMed]
- Dave, B.; Mittal, V.; Tan, N.M.; Chang, J.C. Epithelial-mesenchymal transition, cancer stem cells and treatment resistance. Breast Cancer Res. 2012, 14, 202. [Google Scholar] [CrossRef]
- Gullett, N.P.; Ruhul Amin, A.R.; Bayraktar, S.; Pezzuto, J.M.; Shin, D.M.; Khuri, F.R.; Aggarwal, B.B.; Surh, Y.J.; Kucuk, O. Cancer prevention with natural compounds. Semin. Oncol. 2010, 37, 258–281. [Google Scholar] [CrossRef]
- Park, W.; Amin, A.R.; Chen, Z.G.; Shin, D.M. New perspectives of curcumin in cancer prevention. Cancer Prev. Res. 2013, 6, 387–400. [Google Scholar] [CrossRef]
- Ramakrishna, R.; Diamond, T.H.; Alexander, W.; Manoharan, A.; Golombick, T. Use of Curcumin in Multiple Myeloma patients intolerant of steroid therapy. Clin. Case Rep. 2020, 8, 739–744. [Google Scholar] [CrossRef]
- Santosa, D.; Suharti, C.; Riwanto, I.; Dharmana, E.; Pangarsa, E.A.; Setiawan, B.; Suyono, S.; Tobing, M.L.; Suhartono, S.; Hadisapurto, S. Curcumin as adjuvant therapy to improve remission in myeloma patients: A pilot randomized clinical trial. Caspian J. Intern. Med. 2022, 13, 375–384. [Google Scholar] [CrossRef]
- Saghatelyan, T.; Tananyan, A.; Janoyan, N.; Tadevosyan, A.; Petrosyan, H.; Hovhannisyan, A.; Hayrapetyan, L.; Arustamyan, M.; Arnhold, J.; Rotmann, A.R.; et al. Efficacy and safety of curcumin in combination with paclitaxel in patients with advanced, metastatic breast cancer: A comparative, randomized, double-blind, placebo-controlled clinical trial. Phytomedicine 2020, 70, 153218. [Google Scholar] [CrossRef] [PubMed]
- Howells, L.M.; Iwuji, C.O.O.; Irving, G.R.B.; Barber, S.; Walter, H.; Sidat, Z.; Griffin-Teall, N.; Singh, R.; Foreman, N.; Patel, S.R.; et al. Curcumin Combined with FOLFOX Chemotherapy Is Safe and Tolerable in Patients with Metastatic Colorectal Cancer in a Randomized Phase IIa Trial. J. Nutr. 2019, 149, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Kiselev, V.I.; Ashrafyan, L.A.; Muyzhnek, E.L.; Gerfanova, E.V.; Antonova, I.B.; Aleshikova, O.I.; Sarkar, F.H. A new promising way of maintenance therapy in advanced ovarian cancer: A comparative clinical study. BMC Cancer 2018, 18, 904. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Jia, L.; Chen, G.; Li, X.; Meng, X.; Zhao, X.; Xing, L.; Zhu, W. A prospective, three-arm, randomized trial of EGCG for preventing radiation-induced esophagitis in lung cancer patients receiving radiotherapy. Radiother. Oncol. 2019, 137, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xing, L.; Zhang, Y.; Xie, P.; Zhu, W.; Meng, X.; Wang, Y.; Kong, L.; Zhao, H.; Yu, J. Phase II Trial of Epigallocatechin-3-Gallate in Acute Radiation-Induced Esophagitis for Esophagus Cancer. J. Med. Food 2020, 23, 43–49. [Google Scholar] [CrossRef]
- Gee, J.R.; Saltzstein, D.R.; Kim, K.; Kolesar, J.; Huang, W.; Havighurst, T.C.; Wollmer, B.W.; Stublaski, J.; Downs, T.; Mukhtar, H.; et al. A Phase II Randomized, Double-blind, Presurgical Trial of Polyphenon E in Bladder Cancer Patients to Evaluate Pharmacodynamics and Bladder Tissue Biomarkers. Cancer Prev. Res. 2017, 10, 298–307. [Google Scholar] [CrossRef]
- Crew, K.D.; Ho, K.A.; Brown, P.; Greenlee, H.; Bevers, T.B.; Arun, B.; Sneige, N.; Hudis, C.; McArthur, H.L.; Chang, J.; et al. Effects of a green tea extract, Polyphenon E, on systemic biomarkers of growth factor signalling in women with hormone receptor-negative breast cancer. J. Hum. Nutr. Diet 2015, 28, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.Y.; Motechin, R.A.; Wiesenfeld, M.Y.; Holz, M.K. The therapeutic potential of resveratrol: A review of clinical trials. NPJ Precis. Oncol. 2017, 1, 35. [Google Scholar] [CrossRef]
- Zhu, W.; Qin, W.; Zhang, K.; Rottinghaus, G.E.; Chen, Y.C.; Kliethermes, B.; Sauter, E.R. Trans-resveratrol alters mammary promoter hypermethylation in women at increased risk for breast cancer. Nutr. Cancer 2012, 64, 393–400. [Google Scholar] [CrossRef]
- Paller, C.J.; Rudek, M.A.; Zhou, X.C.; Wagner, W.D.; Hudson, T.S.; Anders, N.; Hammers, H.J.; Dowling, D.; King, S.; Antonarakis, E.S.; et al. A phase I study of muscadine grape skin extract in men with biochemically recurrent prostate cancer: Safety, tolerability, and dose determination. Prostate 2015, 75, 1518–1525. [Google Scholar] [CrossRef]
- Paller, C.J.; Zhou, X.C.; Heath, E.I.; Taplin, M.E.; Mayer, T.; Stein, M.N.; Bubley, G.J.; Pili, R.; Hudson, T.; Kakarla, R.; et al. Muscadine Grape Skin Extract (MPX) in Men with Biochemically Recurrent Prostate Cancer: A Randomized, Multicenter, Placebo-Controlled Clinical Trial. Clin. Cancer Res. 2018, 24, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.V.; Martinez, M.; Stamos, M.J.; Moyer, M.P.; Planutis, K.; Hope, C.; Holcombe, R.F. Results of a phase I pilot clinical trial examining the effect of plant-derived resveratrol and grape powder on Wnt pathway target gene expression in colonic mucosa and colon cancer. Cancer Manag. Res. 2009, 1, 25–37. [Google Scholar] [PubMed]
- Howells, L.M.; Berry, D.P.; Elliott, P.J.; Jacobson, E.W.; Hoffmann, E.; Hegarty, B.; Brown, K.; Steward, W.P.; Gescher, A.J. Phase I randomized, double-blind pilot study of micronized resveratrol (SRT501) in patients with hepatic metastases--safety, pharmacokinetics, and pharmacodynamics. Cancer Prev. Res. 2011, 4, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.R.; Brown, V.A.; Jones, D.J.; Britton, R.G.; Hemingway, D.; Miller, A.S.; West, K.P.; Booth, T.D.; Perloff, M.; Crowell, J.A.; et al. Clinical pharmacology of resveratrol and its metabolites in colorectal cancer patients. Cancer Res. 2010, 70, 7392–7399. [Google Scholar] [CrossRef] [PubMed]
- Dyshlovoy, S.A.; Honecker, F. Marine Compounds and Cancer: Updates 2020. Mar. Drugs 2020, 18, 643. [Google Scholar] [CrossRef] [PubMed]
- Bronstrup, M.; Sasse, F. Natural products targeting the elongation phase of eukaryotic protein biosynthesis. Nat. Prod. Rep. 2020, 37, 752–762. [Google Scholar] [CrossRef]
- Deeks, E.D. Polatuzumab Vedotin: First Global Approval. Drugs 2019, 79, 1467–1475. [Google Scholar] [CrossRef]
- Markham, A. Lurbinectedin: First Approval. Drugs 2020, 80, 1345–1353. [Google Scholar] [CrossRef]
- Skubnik, J.; Pavlickova, V.S.; Ruml, T.; Rimpelova, S. Vincristine in Combination Therapy of Cancer: Emerging Trends in Clinics. Biology 2021, 10, 849. [Google Scholar] [CrossRef]
- Gnekow, A.K.; Walker, D.A.; Kandels, D.; Picton, S.; Giorgio, P.; Grill, J.; Stokland, T.; Sandstrom, P.E.; Warmuth-Metz, M.; Pietsch, T.; et al. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (</=16 years) low grade glioma-A final report. Eur. J. Cancer 2017, 81, 206–225. [Google Scholar] [CrossRef]
- Peyrade, F.; Bologna, S.; Delwail, V.; Emile, J.F.; Pascal, L.; Ferme, C.; Schiano, J.M.; Coiffier, B.; Corront, B.; Farhat, H.; et al. Combination of ofatumumab and reduced-dose CHOP for diffuse large B-cell lymphomas in patients aged 80 years or older: An open-label, multicentre, single-arm, phase 2 trial from the LYSA group. Lancet Haematol. 2017, 4, e46–e55. [Google Scholar] [CrossRef] [PubMed]
- Clamp, A.; Jayson, G.C. The clinical development of the bryostatins. Anticancer Drugs 2002, 13, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Pagliaro, L.; Daliani, D.; Amato, R.; Tu, S.M.; Jones, D.; Smith, T.; Logothetis, C.; Millikan, R. A Phase II trial of bryostatin-1 for patients with metastatic renal cell carcinoma. Cancer 2000, 89, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Varterasian, M.L.; Mohammad, R.M.; Shurafa, M.S.; Hulburd, K.; Pemberton, P.A.; Rodriguez, D.H.; Spadoni, V.; Eilender, D.S.; Murgo, A.; Wall, N.; et al. Phase II trial of bryostatin 1 in patients with relapsed low-grade non-Hodgkin’s lymphoma and chronic lymphocytic leukemia. Clin. Cancer Res. 2000, 6, 825–828. [Google Scholar] [PubMed]
- Zhang, Z.; Garzotto, M.; Davis, E.W., 2nd; Mori, M.; Stoller, W.A.; Farris, P.E.; Wong, C.P.; Beaver, L.M.; Thomas, G.V.; Williams, D.E.; et al. Sulforaphane Bioavailability and Chemopreventive Activity in Men Presenting for Biopsy of the Prostate Gland: A Randomized Controlled Trial. Nutr. Cancer 2020, 72, 74–87. [Google Scholar] [CrossRef]
- Traka, M.H.; Melchini, A.; Coode-Bate, J.; Al Kadhi, O.; Saha, S.; Defernez, M.; Troncoso-Rey, P.; Kibblewhite, H.; O’Neill, C.M.; Bernuzzi, F.; et al. Transcriptional changes in prostate of men on active surveillance after a 12-mo glucoraphanin-rich broccoli intervention-results from the Effect of Sulforaphane on prostate CAncer PrEvention (ESCAPE) randomized controlled trial. Am. J. Clin. Nutr. 2019, 109, 1133–1144. [Google Scholar] [CrossRef]
- Farsad-Naeimi, A.; Alizadeh, M.; Esfahani, A.; Darvish Aminabad, E. Effect of fisetin supplementation on inflammatory factors and matrix metalloproteinase enzymes in colorectal cancer patients. Food Funct. 2018, 9, 2025–2031. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).