
Association of CHA2DS2-VASc Score with Long-Term Incidence of New-Onset Atrial Fibrillation and Ischemic Stroke after Myocardial Infarction

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Design
2.2. Outcomes and Follow-Up
2.3. Data Sources
2.4. Statistical Analysis
3. Results
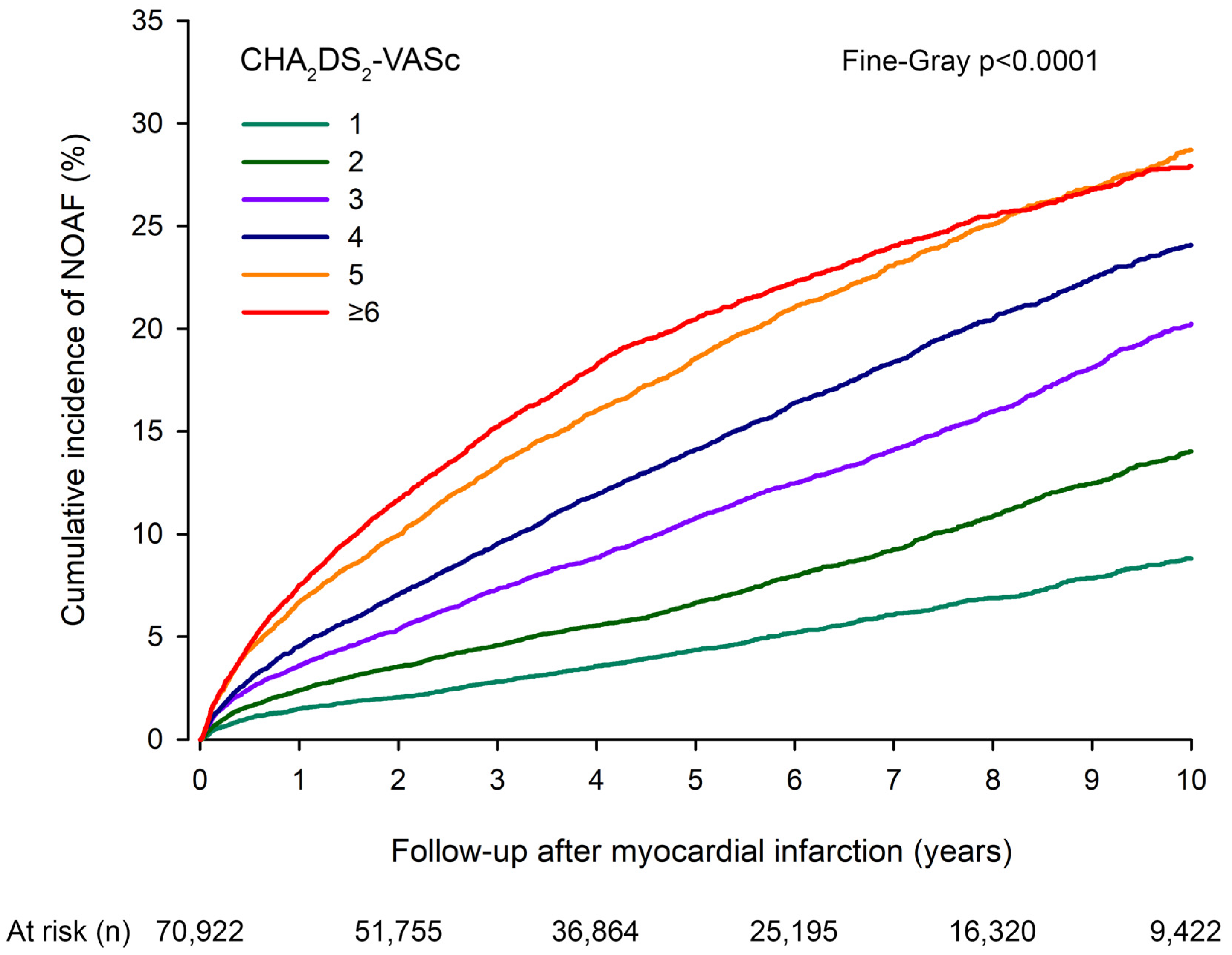
3.1. New-Onset Atrial Fibrillation
3.2. Ischemic Stroke
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lam, C.C.; Tse, H.F.; Siu, C.W. Transient atrial fibrillation complicating acute myocardial infarction: A nuisance or a nemesis? Thromb. Haemost. 2012, 107, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Siu, C.W.; Jim, M.H.; Ho, H.H.; Miu, R.; Lee, S.W.; Lau, C.P.; Tse, H.F. Transient atrial fibrillation complicating acute inferior myocardial infarction: Implications for future risk of ischemic stroke. Chest 2007, 132, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Jabre, P.; Jouven, X.; Adnet, F.; Thabut, G.; Bielinski, S.J.; Weston, S.A.; Roger, V.L. Atrial fibrillation and death after myocardial infarction: A community study. Circulation 2011, 123, 2094–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carnicelli, A.P.; Owen, R.; Pocock, S.J.; Brieger, D.B.; Yasuda, S.; Nicolau, J.C.; Goodman, S.G.; Cohen, M.G.; Simon, T.; Westermann, D.; et al. Atrial fibrillation and clinical outcomes 1 to 3 years after myocardial infarction. Open Heart 2021, 8, e001726. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Levy, D.; Vaziri, S.M.; D’Agostino, R.B.; Belanger, A.J.; Wolf, P.A. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA 1994, 271, 840–844. [Google Scholar] [CrossRef]
- Pamukcu, B.; Lip, G.Y.; Lane, D.A. Simplifying stroke risk stratification in atrial fibrillation patients: Implications of the CHA2DS2-VASc risk stratification scores. Age Ageing 2010, 39, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Kerola, A.M.; Juonala, M.; PaPalomäki, A.; Semb, A.G.; Rautava, P.; Kytö, V. Case Fatality of Patients With Type 1 Diabetes After Myocardial Infarction. Diabetes Care 2022, 45, 1657–1665. [Google Scholar] [CrossRef]
- Kerola, A.M.; Palomaki, A.; Rautava, P.; Nuotio, M.; Kyto, V. Sex Differences in Cardiovascular Outcomes of Older Adults After Myocardial Infarction. J. Am. Heart Assoc. 2021, 10, e022883. [Google Scholar] [CrossRef]
- Webster-Clark, M.; Huang, T.Y.; Hou, L.; Toh, S. Translating claims-based CHA2 DS2-VaSc and HAS-BLED to ICD-10-CM: Impacts of mapping strategies. Pharmacoepidemiol. Drug Saf. 2020, 29, 409–418. [Google Scholar] [CrossRef]
- Kerola, A.M.; Palomaki, A.; Rautava, P.; Kyto, V. Less revascularization in young women but impaired long-term outcomes in young men after myocardial infarction. Eur. J. Prev. Cardiol. 2022, 29, 1437–1445. [Google Scholar] [CrossRef]
- Lehtonen, A.O.; Langen, V.L.; Porthan, K.; Kähönen, M.; Nieminen, M.S.; Jula, A.M.; Niiranen, T. Electrocardiographic predictors of atrial fibrillation in nonhypertensive and hypertensive individuals. J. Hypertens. 2018, 36, 1874–1881. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Lee, D.S.; Fine, J.P. Introduction to the Analysis of Survival Data in the Presence of Competing Risks. Circulation 2016, 133, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Bang, C.N.; Gislason, G.H.; Greve, A.M.; Bang, C.A.; Lilja, A.; Torp-Pedersen, C.; Andersen, P.K.; Køber, L.; Devereux, R.B.; Wachtell, K. New-onset atrial fibrillation is associated with cardiovascular events leading to death in a first time myocardial infarction population of 89,703 patients with long-term follow-up: A nationwide study. J. Am. Heart Assoc. 2014, 3, e000382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alasady, M.; Shipp, N.J.; Brooks, A.G.; Lim, H.S.; Lau, D.H.; Barlow, D.; Kuklik, P.; Worthley, M.I.; Roberts-Thomson, K.C.; Saint, D.A.; et al. Myocardial infarction and atrial fibrillation: Importance of atrial ischemia. Circ. Arrhythm. Electrophysiol. 2013, 6, 738–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, K.K.; Chan, P.H.; Yiu, K.H.; Chan, Y.H.; Liu, S.; Chan, K.H.; Yeung, C.Y.; Li, S.W.; Tse, H.F.; Siu, C.W. Roles of the CHADS2 and CHA2DS2-VASc scores in post-myocardial infarction patients: Risk of new occurrence of atrial fibrillation and ischemic stroke. Cardiol. J. 2014, 21, 474–483. [Google Scholar] [CrossRef] [Green Version]
- Kosmidou, I.; Chen, S.; Kappetein, A.P.; Serruys, P.W.; Gersh, B.J.; Puskas, J.D.; Kandzari, D.E.; Taggart, D.P.; Morice, M.-C.; Buszman, P.E.; et al. New-Onset Atrial Fibrillation After PCI or CABG for Left Main Disease: The EXCEL Trial. J. Am. Coll. Cardiol. 2018, 71, 739–748. [Google Scholar] [CrossRef]
- Benedetto, U.; Gaudino, M.F.; Dimagli, A.; Gerry, S.; Gray, A.; Lees, B.; Flather, M.; Taggart, D.P.; Westaby, S.; Cook, J.; et al. Postoperative Atrial Fibrillation and Long-Term Risk of Stroke After Isolated Coronary Artery Bypass Graft Surgery. Circulation 2020, 142, 1320–1329. [Google Scholar] [CrossRef]
- Tseng, C.H.; Chung, W.J.; Li, C.Y.; Tsai, T.H.; Lee, C.H.; Hsueh, S.K.; Wu, C.C.; Cheng, C.I. Statins reduce new-onset atrial fibrillation after acute myocardial infarction: A nationwide study. Medicine 2020, 99, e18517. [Google Scholar] [CrossRef]
- Merkler, A.E.; Diaz, I.; Wu, X.; Murthy, S.B.; Gialdini, G.; Navi, B.B.; Yaghi, S.; Weinsaft, J.W.; Okin, P.M.; Safford, M.M.; et al. Duration of Heightened Ischemic Stroke Risk After Acute Myocardial Infarction. J. Am. Heart Assoc. 2018, 7, e010782. [Google Scholar] [CrossRef] [Green Version]
- Kamel, H.; Healey, J.S. Cardioembolic Stroke. Circ. Res. 2017, 120, 514–526. [Google Scholar] [CrossRef]
- Son, M.K.; Lim, N.K.; Kim, H.W.; Park, H.Y. Risk of ischemic stroke after atrial fibrillation diagnosis: A national sample cohort. PLoS ONE 2017, 12, e0179687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaakkola, J.; Mustonen, P.; Kiviniemi, T.; Hartikainen, J.E.K.; Palomäki, A.; Hartikainen, P.; Nuotio, I.; Ylitalo, A.; Airaksinen, K.E.J. Stroke as the First Manifestation of Atrial Fibrillation. PLoS ONE 2016, 11, e0168010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rexrode, K.M.; Madsen, T.E.; Yu, A.Y.; Carcel, C.; Lichtman, J.H.; Miller, E.C. The Impact of Sex and Gender on Stroke. Circ. Res. 2022, 130, 512–528. [Google Scholar] [CrossRef] [PubMed]
- Gasbarrino, K.; Di Iorio, D.; Daskalopoulou, S.S. Importance of sex and gender in ischaemic stroke and carotid atherosclerotic disease. Eur. Heart J. 2022, 43, 460–473. [Google Scholar] [CrossRef]
- Witt, B.J.; Ballman, K.V.; Brown, R.D., Jr.; Meverden, R.A.; Jacobsen, S.J.; Roger, V.L. The incidence of stroke after myocardial infarction: A meta-analysis. Am. J. Med. 2006, 119, 354.e1–354.e9. [Google Scholar] [CrossRef]
- Head, S.J.; Milojevic, M.; Daemen, J.; Ahn, J.-M.; Boersma, E.; Christiansen, E.H.; Domanski, M.J.; Farkouh, M.E.; Flather, M.; Fuster, V.; et al. Stroke Rates Following Surgical Versus Percutaneous Coronary Revascularization. J. Am. Coll. Cardiol. 2018, 72, 386–398. [Google Scholar] [CrossRef]
- Astrom, A.; Soderstrom, L.; Mooe, T. Risk of Ischemic Stroke After Acute Myocardial Infarction in Patients Undergoing Coronary Artery Bypass Graft Surgery. Sci. Rep. 2020, 10, 3831. [Google Scholar] [CrossRef] [Green Version]
- Prami, T.; Khanfir, H.; Deleskog, A.; Hasvold, P.; Kytö, V.; Reissell, E.; Airaksinen, J. Clinical factors associated with initiation of and persistence with ADP receptor-inhibiting oral antiplatelet treatment after acute coronary syndrome: A nationwide cohort study from Finland. BMJ Open 2016, 6, e012604. [Google Scholar] [CrossRef] [Green Version]
- Lehto, M.; Halminen, O.; Mustonen, P.; Putaala, J.; Linna, M.; Kinnunen, J.; Kouki, E.; Niiranen, J.; Hartikainen, J.; Haukka, J.; et al. The nationwide Finnish anticoagulation in atrial fibrillation (FinACAF): Study rationale, design, and patient characteristics. Eur. J. Epidemiol. 2022, 37, 95–102. [Google Scholar] [CrossRef]


{kind=link}
| Patients (n = 70,922) n (%) | |
|---|---|
| Age (years) mean (SD) | 68.2 (12.6) |
| <65 | 27,365 (38.6%) |
| 65–74 | 19,155 (27.0%) |
| ≥75 | 24,402 (34.4%) |
| Female sex | 24,655 (34.7%) |
| Congestive heart failure | 12,253 (17.3%) |
| Hypertension | 35,252 (49.7%) |
| Diabetes | 15,967 (22.5%) |
| Stroke/TIA/Thromboembolism | 7191 (10.1%) |
| CHA2DS2-VASc score | |
| 1 | 11,559 (16.3%) |
| 2 | 13,755 (19.4%) |
| 3 | 13,939 (19.6%) |
| 4 | 12,601 (17.8%) |
| 5 | 9640 (13.6%) |
| ≥6 | 9438 (13.3%) |
| ST-elevation MI | 27,589 (38.9%) |
| Revascularization | |
| None | 26,423 (37.3%) |
| PCI | 39,191 (55.3%) |
| CABG * | 5308 (7.5%) |
| CHA2DS2-VASc Score | Cumulative Incidence n (%) | Unadjusted sHR (95%CI) | Adjusted sHR (95%CI) | |||
|---|---|---|---|---|---|---|
| (n) | 1 Year | 10 Year | 1 Year | 10 Year | 1 Year | 10 Year |
| 1 (11,559) | 169 (1.5%) | 673 (8.8%) | Reference | Reference | Reference | Reference |
| 2 (13,755) | 326 (2.4%) | 1233 (14.0%) | 1.63 (1.35–1.96) | 1.61 (1.47–1.77) | 1.60 (1.32–1.92) | 1.59 (1.45–1.74) |
| 3 (13,929) | 491 (3.6%) | 1837 (20.2%) | 2.46 (2.06–2.93) | 2.46 (2.25–2.69) | 2.24 (1.96–2.78) | 2.40 (2.20–2.62) |
| 4 (12,601) | 557 (4.6%) | 2048 (24.1%) | 3.12 (2.63–3.71) | 3.14 (2.88–3.43) | 2.91 (2.45–3.46) | 3.04 (2.78–3.32) |
| 5 (9640) | 622 (6.7%) | 1924 (28.7%) | 4.64 (3.92–5.50) | 4.05 (3.71–4.42) | 4.24 (3.57–5.04) | 3.89 (3.56–4.26) |
| ≥6 (9438) | 668 (7.5%) | 1899 (27.9%) | 5.21 (4.40–6.16) | 4.22 (3.87–4.61) | 4.66 (3.92–5.55) | 4.03 (3.68–4.42) |
| CHA2DS2-VASc | Patients with IS | NOAF-Related IS |
|---|---|---|
| Score | n | n (%) |
| 1 | 227 | 38 (16.7%) |
| 2 | 447 | 76 (17.0%) |
| 3 | 679 | 134 (19.7%) |
| 4 | 751 | 194 (25.8%) |
| 5 | 723 | 198 (27.4%) |
| ≥6 | 964 | 213 (22.1%) |
| CHA2DS2-VASc Score | Cumulative Incidence n (%) | Unadjusted sHR (95%CI) | Adjusted sHR (95%CI) | |||
|---|---|---|---|---|---|---|
| (n) | 1 Year | 10 Year | 1 Year | 10 Year | 1 Year | 10 Year |
| 1 (673) | 25 (3.9%) | 38 (7.1%) | Reference | Reference | Reference | Reference |
| 2 (1233) | 49 (4.3%) | 76 (7.9%) | 1.07 (0.66–1.72) | 1.09 (0.74–1.61) | 1.05 (0.65–1.70) | 1.10 (0.74–1.61) |
| 3 (1837) | 88 (5.1%) | 134 (9.1%) | 1.26 (0.81–1.96) | 1.26 (0.88–1.80) | 1.24 (0.80–1.92) | 1.25 (0.88–1.79) |
| 4 (2048) | 133 (6.9%) | 194 (11.6%) | 1.69 (1.11–2.59) | 1.62 (1.15–2.29) | 1.66 (1.08–2.54) | 1.61 (1.14–2.27) |
| 5 (1924) | 137 (7.5%) | 198 (12.5%) | 1.84 (1.21–2.81) | 1.76 (1.25–2.48) | 1.78 (1.16–2.74) | 1.72 (1.21–2.44) |
| ≥6 (1899) | 149 (8.2%) | 213 (13.5%) | 2.02 (1.33–3.08) | 1.91 (1.36–2.69) | 1.95 (1.27–2.99) | 1.85 (1.31–2.62) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaakkola, S.; Paana, T.; Airaksinen, J.; Sipilä, J.; Kytö, V. Association of CHA2DS2-VASc Score with Long-Term Incidence of New-Onset Atrial Fibrillation and Ischemic Stroke after Myocardial Infarction. J. Clin. Med. 2022, 11, 7090. https://doi.org/10.3390/jcm11237090
Jaakkola S, Paana T, Airaksinen J, Sipilä J, Kytö V. Association of CHA2DS2-VASc Score with Long-Term Incidence of New-Onset Atrial Fibrillation and Ischemic Stroke after Myocardial Infarction. Journal of Clinical Medicine. 2022; 11(23):7090. https://doi.org/10.3390/jcm11237090
Chicago/Turabian StyleJaakkola, Samuli, Tuomas Paana, Juhani Airaksinen, Jussi Sipilä, and Ville Kytö. 2022. "Association of CHA2DS2-VASc Score with Long-Term Incidence of New-Onset Atrial Fibrillation and Ischemic Stroke after Myocardial Infarction" Journal of Clinical Medicine 11, no. 23: 7090. https://doi.org/10.3390/jcm11237090