
Randomized Comparison of Two New Methods for Chest Compressions during CPR in Microgravity—A Manikin Study


 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
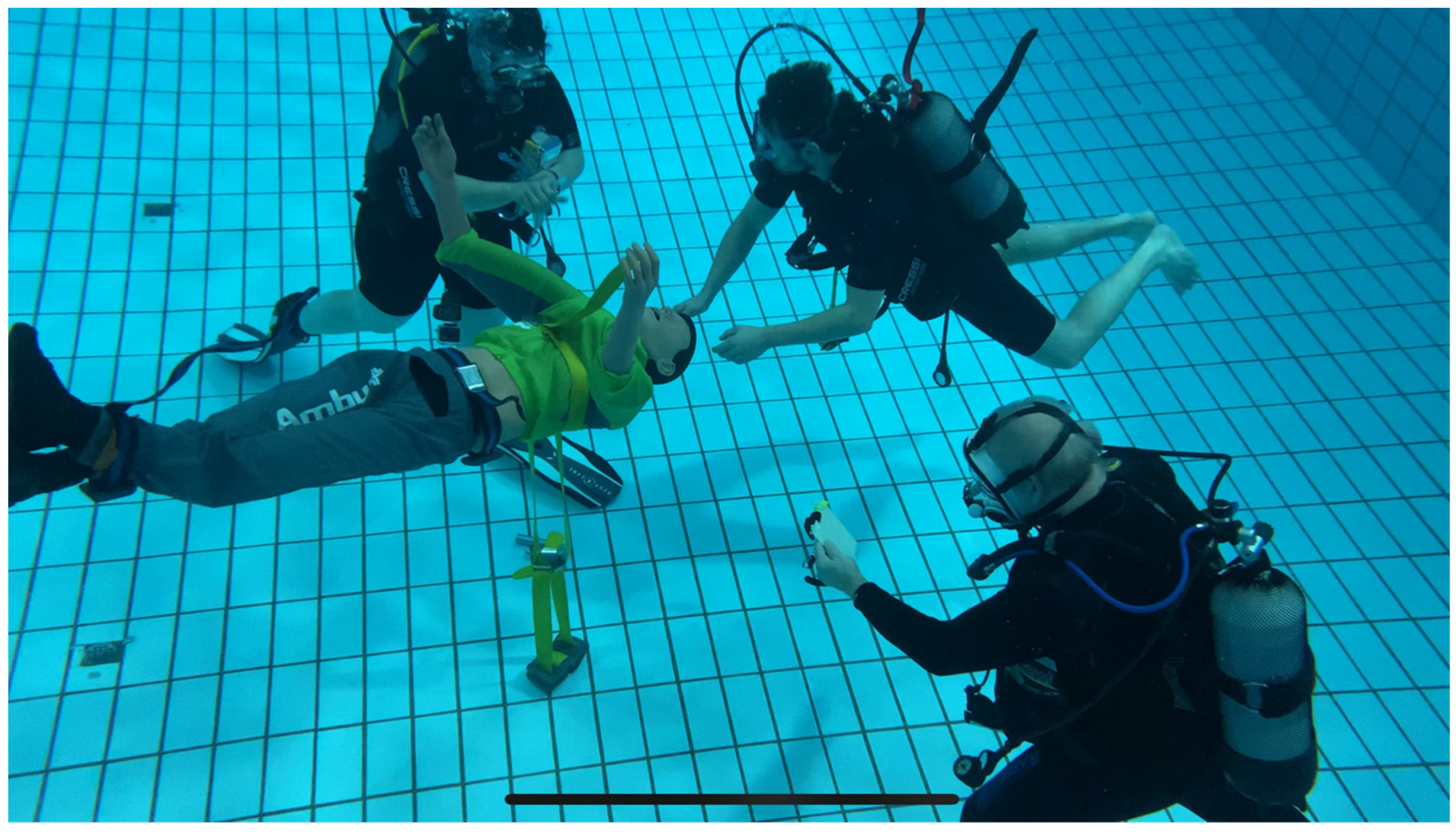
2.2. Setting
2.3. Randomisation
- (1)
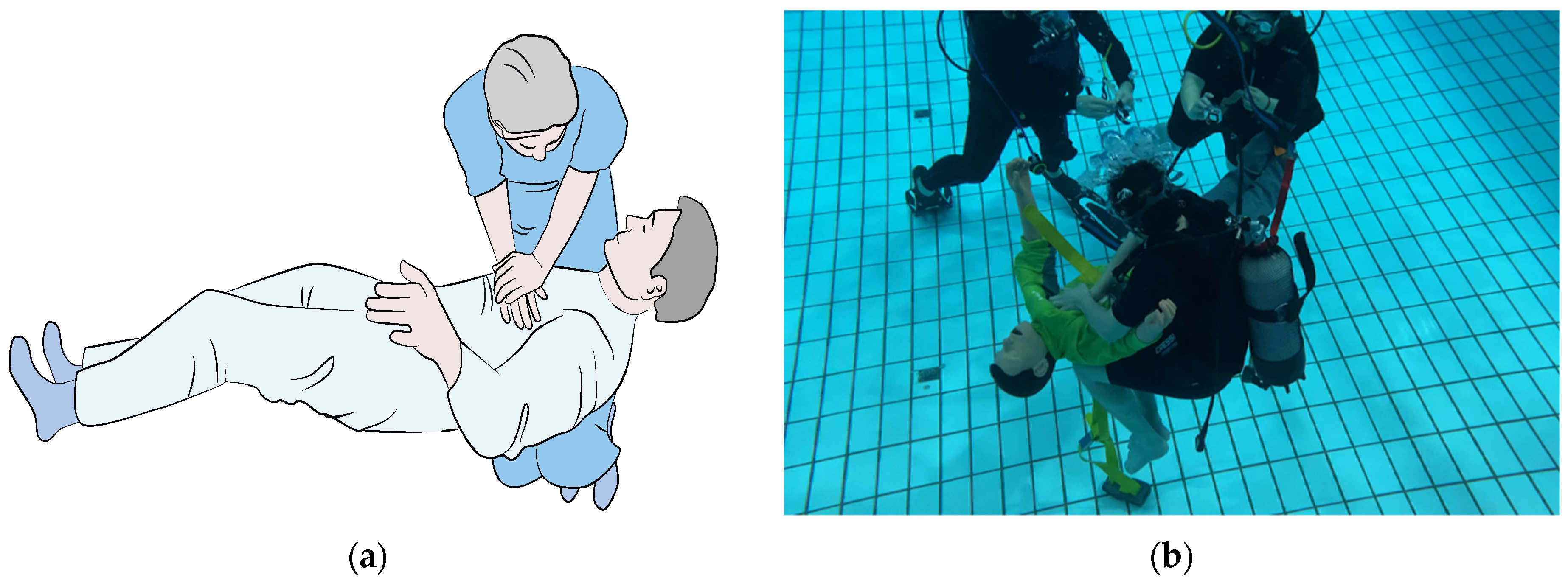
- Schmitz–Hinkelbein method
- (2)
- Cologne method
2.4. Data Collection
2.5. Video Analysis
2.6. The Primary Endpoint Was as Follows:
- Compression rate (defined as compression of the thorax) (per min).
2.7. The Secondary Endpoints Were as Follows:
- Number of chest compressions (n);
- Correct depth (defined as min. 50 to max. 60 mm of depth) (mm);
- Number of periods with no chest compression above 2 s (no-flow time) (n);
- Correct thoracic release between compressions (high = more than 66%; moderate = 33–65%; low = 0–32% of number of chest compressions with release of more than 4 cm according to indicator on manikin).
2.8. Statistics
2.9. Ethics and Registration
3. Results
3.1. Subjects
3.2. Compression Rate
3.3. Chest Compression Depth
3.4. Period of No Chest Compression >2 s (No-Flow Time)
3.5. Correct Thoracic Release between Compressions
4. Discussion
4.1. General Considerations
4.2. Number of Chest Compressions and Compression Rate
4.3. Compression Depth
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BSD | Body Suspension Device |
| CMAS | Confederation Mondiale des Activites Subaquatiques |
| CM | Cologne method |
| CMO | Crew Medical Officer |
| CMRS | Crew Medical Restraint System |
| CPR | Cardiopulmonary Resuscitation |
| CD | Compression Depth |
| CR | Compression Rate |
| ER | Evetts–Russomano method |
| ESA | European Space Agency |
| ETI | Endotracheal Intubation |
| GA | General anesthesia |
| HS | Handstand method |
| ISS | International Space Station |
| LEO | Low-earth Orbit |
| NASA | National Aeronautics and Space Administration |
| PADI | Professional Association of Diving Instructors |
| OWD | Open Water Diver |
| RBH | Reverse bear hug method |
| RCT | Randomized Controlled Trial |
| SHM | Schmitz–Hinkelbein method |
| SSI | Scuba Schools International |
References
- Witze, A. Can NASA really return people to the Moon by 2024? Nat. Cell Biol. 2019, 571, 153–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinkelbein, J.; Spelten, O. Going beyond anesthesia in space exploration missions: Emergency medicine and emergency medical care. Aviat. Space Environ. Med. 2013, 84, 747. [Google Scholar] [CrossRef] [PubMed]
- Nicogossian, A. Medicine and space exploration. Lancet 2003, 362, s8–s9. [Google Scholar] [CrossRef]
- Komorowski, M.; Fleming, S.; Mawkin, M.; Hinkelbein, J. Anaesthesia in austere environments: Literature review and considerations for future space exploration missions. NPJ Microgravity 2018, 4, 5. [Google Scholar] [CrossRef]
- Nicogossian, A.E.; Pober, D.F.; Roy, S.A. Evolution of Telemedicine in the Space Program and Earth Applications. Telemed. e-Health 2001, 7, 1–15. [Google Scholar] [CrossRef]
- Hinkelbein, J. Spaceflight: The final frontier for airway management? Br. J. Anaesth. 2020, 125, e5–e6. [Google Scholar] [CrossRef]
- Tanaka, K.; Nishimura, N.; Kawai, Y. Adaptation to microgravity, deconditioning, and countermeasures. J. Physiol. Sci. 2017, 67, 271–281. [Google Scholar] [CrossRef]
- Shen, M.; Frishman, W.H. Effects of Spaceflight on Cardiovascular Physiology and Health. Cardiol. Rev. 2019, 27, 122–126. [Google Scholar] [CrossRef]
- Hughson, R.L.; Helm, A.; Durante, M. Heart in space: Effect of the extraterrestrial environment on the cardio-vascular system. Nat. Rev. Cardiol. 2018, 15, 167–180. [Google Scholar] [CrossRef]
- Roberts, D.; Brown, T.; Nietert, P.; Eckert, M.; Inglesby, D.; Bloomberg, J.; George, M.; Asemani, D. Prolonged Microgravity Affects Human Brain Structure and Function. Am. J. Neuroradiol. 2019, 40, 1878–1885. [Google Scholar] [CrossRef] [Green Version]
- Russomano, T.; Da Rosa, M.; A Dos Santos, M. Space motion sickness: A common neurovestibular dysfunction in microgravity. Neurol. India 2019, 67, S214–S218. [Google Scholar] [CrossRef] [Green Version]
- Swaffield, T.P.; Neviaser, A.S.; Lehnhardt, K. Fracture Risk in Spaceflight and Potential Treatment Options. Aerosp. Med. Hum. Perform. 2018, 89, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Summers, R.L.; Johnston, S.L.; Marshburn, T.H.; Williams, D.R. Emergencies in space. Ann. Emerg. Med. 2005, 46, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Lott, C.; Truhlář, A.; Alfonzo, A.; Barelli, A.; González-Salvado, V.; Hinkelbein, J.; Nolan, J.P.; Paal, P.; Perkins, G.D.; Thies, K.-C.; et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef] [PubMed]
- Hinkelbein, J.; Kerkhoff, S.; Adler, C.; Ahlbäck, A.; Braunecker, S.; Burgard, D.; Cirillo, F.; De Robertis, E.; Glaser, E.; Haidl, T.K.; et al. Cardiopulmonary resuscitation (CPR) during spaceflight—A guideline for CPR in microgravity from the German Society of Aerospace Medicine (DGLRM) and the European Society of Aerospace Medicine Space Medicine Group (ESAM-SMG). Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 108. [Google Scholar] [CrossRef]
- Forti, A.; van Veelen, M.J.; Squizzato, T.; Cappello, T.D.; Palma, M.; Strapazzon, G. Mechanical cardiopulmonary resuscitation in microgravity and hypergravity conditions: A manikin study during parabolic flight. Am. J. Emerg. Med. 2021, 53, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Braunecker, S.; Douglas, B.; Hinkelbein, J. Comparison of different techniques for in microgravity—A simple mathematic estimation of cardiopulmonary resuscitation quality for space environment. Am. J. Emerg. Med. 2015, 33, 920–924. [Google Scholar] [CrossRef]
- Rehnberg, L.; Russomano, T.; Falcão, F.; Campos, F.; Evetts, S.N. Evaluation of a Novel Basic Life Support Method in Simulated Microgravity. Aviat. Space Environ. Med. 2011, 82, 104–110. [Google Scholar] [CrossRef]
- Tjelmeland, I.B.M.; Masterson, S.; Herlitz, J.; Wnent, J.; Bossaert, L.; Rosell-Ortiz, F.; Alm-Kruse, K.; Bein, B.; Lilja, G.; Gräsner, J.-T.; et al. Description of Emergency Medical Services, treatment of cardiac arrest patients and cardiac arrest registries in Europe. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 1–16. [Google Scholar] [CrossRef]
- Song, J.; Guo, W.; Lu, X.; Kang, X.; Song, Y.; Gong, D. The effect of bystander cardiopulmonary resuscitation on the survival of out-of-hospital cardiac arrests: A systematic review and meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 86. [Google Scholar] [CrossRef]
- Rehnberg, L.; Ashcroft, A.; Baers, J.H.; Campos, F.; Cardoso, R.B.; Velho, R.; Gehrke, R.D.; Dias, M.K.P.; Baptista, R.R.; Russomano, T. Three Methods of Manual External Chest Compressions During Microgravity Simulation. Aviat. Space Environ. Med. 2014, 85, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Jay, G.D.; Lee, P.; Goldsmith, H.; Battat, J.; Maurer, J.; Suner, S. CPR effectiveness in microgravity: Comparison of three positions and a mechanical device. Aviat. Space Environ. Med. 2003, 74, 1183–1189. [Google Scholar] [PubMed]
- Kordi, M.; Kluge, N.; Kloeckner, M.; Russomano, T. Gender influence on the performance of chest compressions in simulated hypogravity and microgravity. Aviat. Space Environ. Med. 2012, 83, 643–648. [Google Scholar] [CrossRef]
- Egger, A.; Niederer, M.; Tscherny, K.; Burger, J.; Fuhrmann, V.; Kienbacher, C.; Roth, D.; Schreiber, W.; Herkner, H. Influence of physical strain at high altitude on the quality of cardiopulmonary resuscitation. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kordi, M.; Cardoso, R.B.; Russomano, T. A preliminary comparison between methods of performing external chest compressions during microgravity simulation. Aviat. Space Environ. Med. 2011, 82, 1161–1163. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, Y.; Saitoh, T.; Yasui, H.; Ueno, M.; Hotta, K.; Ogawa, T.; Takahashi, Y.; Maekawa, Y.; Yoshino, A. Comparison of Chest Compression Quality Using Wing Boards versus Walking Next to a Moving Stretcher: A Randomized Crossover Simulation Study. J. Clin. Med. 2020, 9, 1584. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Number of Chest Compressions (/min) | Correct Compression Depth (50–60 mm) |
|---|---|---|
| New Methods | ||
| Schmitz–Hinkelbein method | 100.5 ± 14.4 | 0.65 ± 0.23 |
| Cologne method | 73.9 ± 25.5 | 0.28 ± 0.27 |
| Existing Methods | ||
| Handstand method | 115.4 ± 12.1 | 0.91 ± 0.07 |
| Evetts–Russomano method | 104.6 ± 5.4 | 0.74 ± 0.1 |
| Reverse bear hug method | 94.7 ± 5.4 | 0.82 ± 0.13 |
| Side straddle method | 100.0 ± 3.0 | 0.50 ± 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmitz, J.; Ahlbäck, A.; DuCanto, J.; Kerkhoff, S.; Komorowski, M.; Löw, V.; Russomano, T.; Starck, C.; Thierry, S.; Warnecke, T.; et al. Randomized Comparison of Two New Methods for Chest Compressions during CPR in Microgravity—A Manikin Study. J. Clin. Med. 2022, 11, 646. https://doi.org/10.3390/jcm11030646
Schmitz J, Ahlbäck A, DuCanto J, Kerkhoff S, Komorowski M, Löw V, Russomano T, Starck C, Thierry S, Warnecke T, et al. Randomized Comparison of Two New Methods for Chest Compressions during CPR in Microgravity—A Manikin Study. Journal of Clinical Medicine. 2022; 11(3):646. https://doi.org/10.3390/jcm11030646
Chicago/Turabian StyleSchmitz, Jan, Anton Ahlbäck, James DuCanto, Steffen Kerkhoff, Matthieu Komorowski, Vanessa Löw, Thais Russomano, Clement Starck, Seamus Thierry, Tobias Warnecke, and et al. 2022. "Randomized Comparison of Two New Methods for Chest Compressions during CPR in Microgravity—A Manikin Study" Journal of Clinical Medicine 11, no. 3: 646. https://doi.org/10.3390/jcm11030646
APA StyleSchmitz, J., Ahlbäck, A., DuCanto, J., Kerkhoff, S., Komorowski, M., Löw, V., Russomano, T., Starck, C., Thierry, S., Warnecke, T., & Hinkelbein, J. (2022). Randomized Comparison of Two New Methods for Chest Compressions during CPR in Microgravity—A Manikin Study. Journal of Clinical Medicine, 11(3), 646. https://doi.org/10.3390/jcm11030646