
Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection and DNA Extraction
2.3. Next-Generation Sequencing of Bacterial 16S rRNA Gene
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Comparison of Cervical Fluid Microbiota Composition between Patients with Favorable or Unfavorable ART Outcome
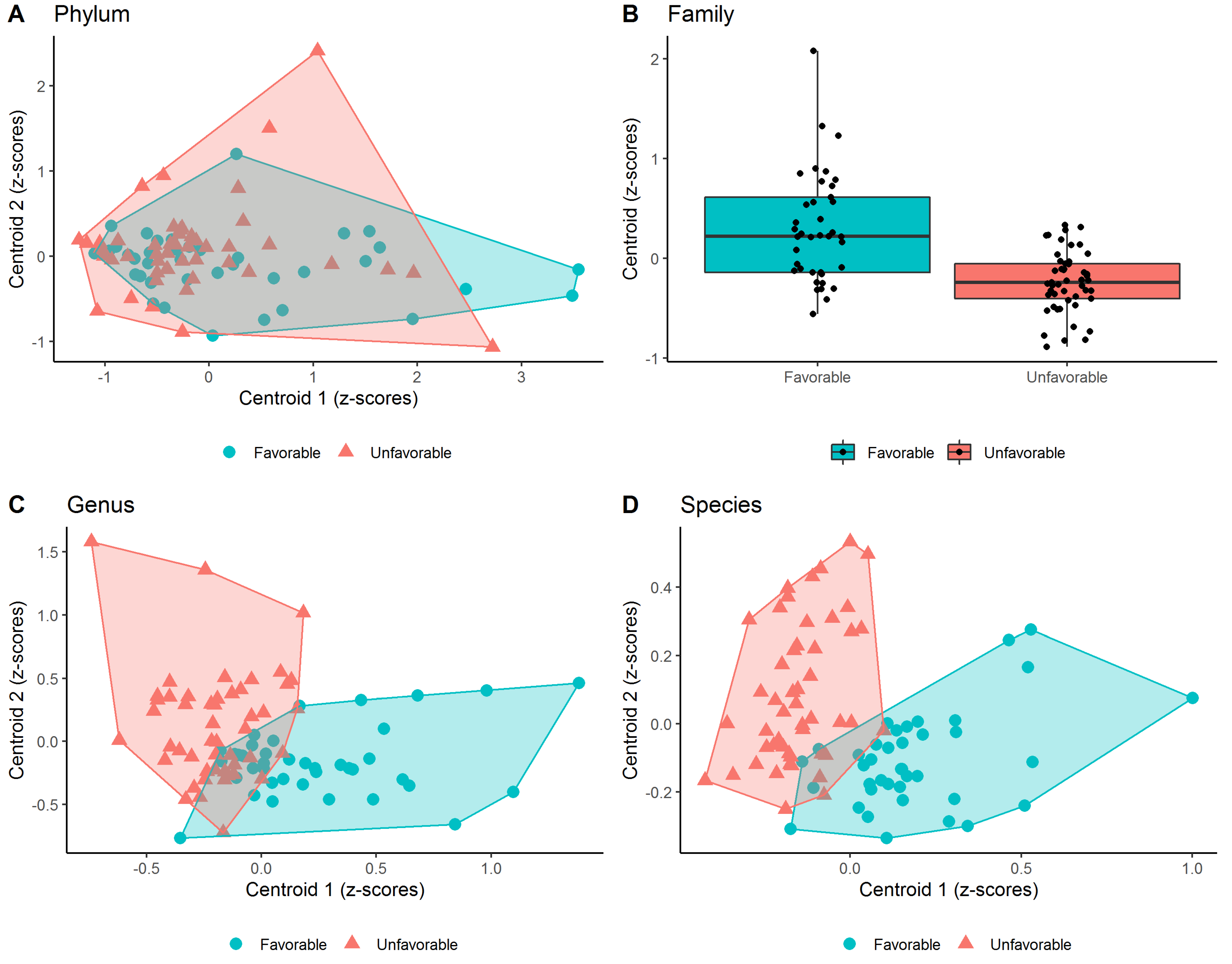
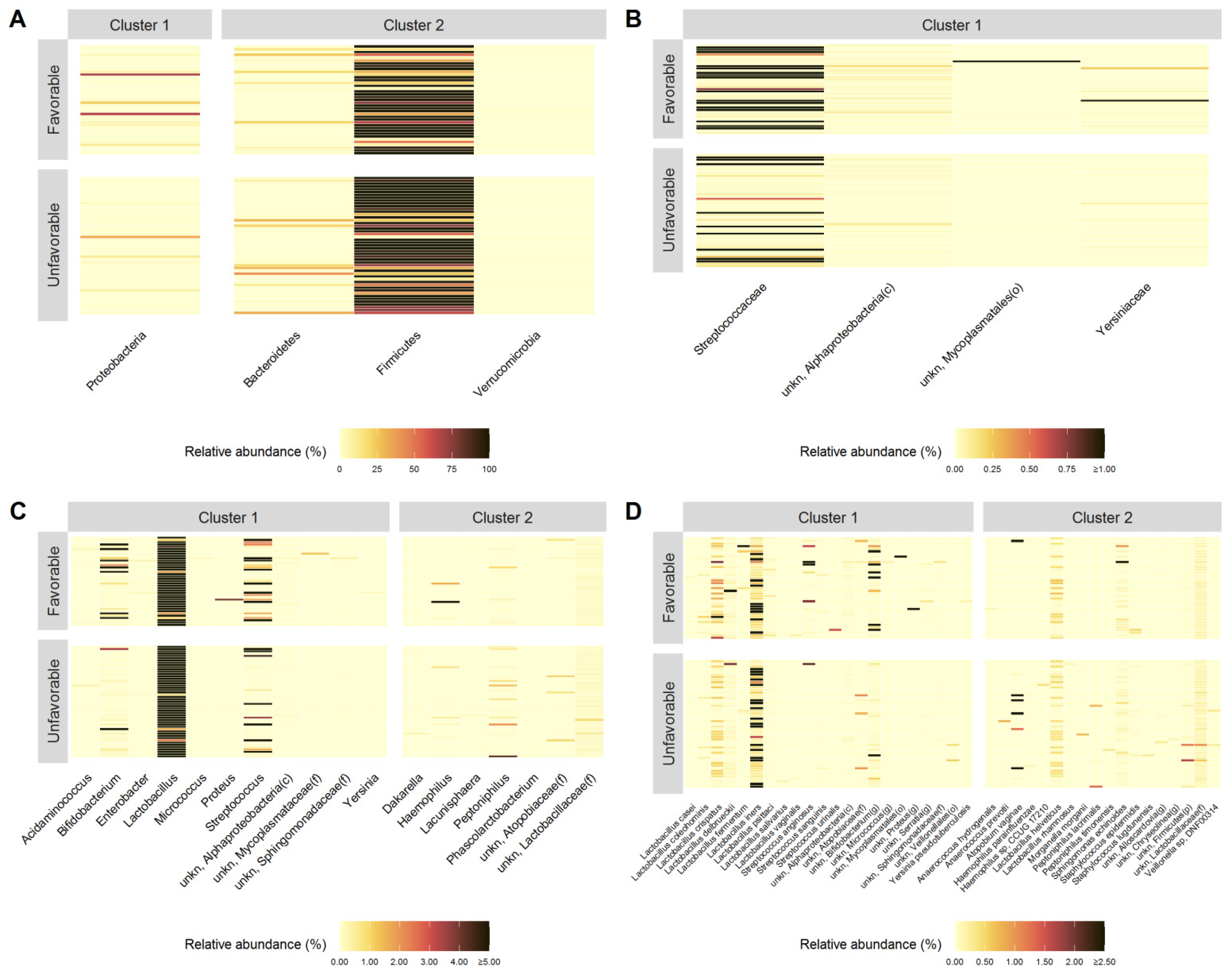
3.3. PELORA Algorithm Identified Bacterial Populations Associated to Favorable or Unfavorable Pregnancy Outcome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kervinen, K.; Kalliala, I.; Glazer-Livson, S.; Virtanen, S.; Nieminen, P.; Salonen, A. Vaginal microbiota in pregnancy: Role in induction of labor and seeding the neonate’s microbiota? J. Biosci. 2019, 44, 116. [Google Scholar] [CrossRef]
- Moosa, Y.; Kwon, D.; de Oliveira, T.; Wong, E.B. Determinants of Vaginal Microbiota Composition. Front. Cell Infect. Microbiol. 2020, 10, 467. [Google Scholar] [CrossRef] [PubMed]
- Elovitz, M.A.; Gajer, P.; Riis, V.; Brown, A.G.; Humphrys, M.S.; Holm, J.B.; Ravel, J. Cervicovaginal microbiota and local immune response modulate the risk of spontaneous preterm delivery. Nat. Commun. 2019, 10, 1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaviani, F.; Hezelgrave, N.L.; Kanno, T.; Prosdocimi, E.M.; Chin-Smith, E.; Ridout, A.E.; von Maydell, D.K.; Mistry, V.; Wade, W.G.; Shennan, A.H.; et al. Cervicovaginal microbiota and metabolome predict preterm birth risk in an ethnically diverse cohort. JCI Insight 2021, 6, e149257. [Google Scholar] [CrossRef]
- Tomaiuolo, R.; Veneruso, I.; Cariati, F.; D’Argenio, V. Microbiota and Human Reproduction: The Case of Female Infertility. High Throughput 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- De Geyter, C. Assisted Reproductive Technology: Impact on Society and Need for Surveillance. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on Spontaneous Abortion and Human Papillomavirus Infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef]
- Perino, A.; Giovannelli, L.; Schillaci, R.; Ruvolo, G.; Fiorentino, F.P.; Alimondi, P.; Cefalù, E.; Ammatuna, P. Human papillomavirus infection in couples undergoing in vitro fertilization procedures: Impact on reproductive outcomes. Fertil. Steril. 2011, 95, 1845–1848. [Google Scholar] [CrossRef]
- Giakoumelou, S.; Wheelhouse, N.; Cuschieri, K.; Entrican, G.; Howie, S.E.; Horne, A.W. The role of infection in miscarriage. Hum. Reprod. Update 2016, 22, 116–133. [Google Scholar] [CrossRef] [Green Version]
- Koedooder, R.; Singer, M.; Schoenmakers, S.; Savelkoul, P.H.M.; Morré, S.A.; De Jonge, J.D.; Poort, L.; Cuypers, W.J.S.S.; Beckers, N.G.M.; Broekmans, F.J.M.; et al. The Vaginal Microbiome as a Predictor for Outcome of In Vitro Fertilization with or without Intracytoplasmic Sperm Injection: A Prospective Study. Hum. Reprod. 2019, 34, 1042–1054. [Google Scholar] [CrossRef]
- Xao, X.; Li, P.; Wu, S. Association of the Cervical Microbiota with Pregnancy Outcome in a Subfertile Population Undergoing In Vitro Fertilization: A Case-Control Study. Front. Cell Infect. Microbiol. 2021, 11, 654202. [Google Scholar] [CrossRef]
- Moreno, I.; Codoñer, F.M.; Vilella, F.; Valbuena, D.; Martinez-Blanch, J.F.; Jimenez-Almazán, J.; Alonso, R.; Alamá, P.; Remohí, J.; Pellicer, A.; et al. Evidence That the Endometrial Microbiota has an Effect on Implantation Success or Failure. Am. J. Obstet. Gynecol. 2016, 215, 684–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef] [PubMed]
- Curty, G.; de Carvalho, P.S.; Soares, M.A. The Role of the Cervicovaginal Microbiome on the Genesis and as a Biomarker of Premalignant Cervical Intraepithelial Neoplasia and Invasive Cervical Cancer. Int. J. Mol. Sci. 2019, 21, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holm, J.B.; France, M.T.; Ma, B.; McComb, E.; Robinson, C.K.; Mehta, A.; Tallon, L.J.; Brotman, R.M.; Ravel, J. Comparative Metagenome-Assembled Genome Analysis of “Candidatus Lachnocurva vaginae”, Formerly Known as Bacterial Vaginosis-Associated Bacterium−1 (BVAB1). Front. Cell Infect. Microbiol. 2020, 10, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenmakers, S.; Laven, J. The Vaginal Microbiome as a Tool to Predict IVF Success. Curr. Opin. Obstet. Gynecol. 2020, 32, 169–178. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glockner, F.O. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef]
- Fontana, A.; Panebianco, C.; Picchianti-Diamanti, A.; Laganà, B.; Cavalieri, D.; Potenza, A.; Pracella, R.; Binda, E.; Copetti, M.; Pazienza, V. Gut Microbiota Profiles Differ among Individuals Depending on Their Region of Origin: An Italian Pilot Study. Int. J. Env. Res. Public Health 2019, 16, 4065. [Google Scholar] [CrossRef] [Green Version]
- Dettling, M.; Bühlmann, P. Finding Predictive Gene Groups from Microarray Data. J. Multivar. Anal. 2004, 90, 106–131. [Google Scholar] [CrossRef]
- García-Velasco, J.A.; Menabrito, M.; Catalán, I.B. What fertility specialists should know about the vaginal microbiome: A review. Reprod. Biomed. Online 2017, 35, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Franasiak, J.M.; Scott, R.T., Jr. Reproductive tract microbiome in assisted reproductive technologies. Fertil. Steril. 2015, 104, 1364–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Song, X.; Wei, W.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyono, K.; Hashimoto, T.; Nagai, Y.; Sakuraba, Y. Analysis of endometrial microbiota by 16S ribosomal RNA gene sequencing among infertile patients: A single-center pilot study. Reprod. Med. Biol. 2018, 17, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Benner, M.; Ferwerda, G.; Joosten, I.; van der Molen, R.G. How uterine microbiota might be responsible for a receptive, fertile endometrium. Hum. Reprod. Update 2018, 24, 393–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashimoto, T.; Kyono, K. Does dysbiotic endometrium affect blastocyst implantation in IVF patients? J. Assist. Reprod. Genet. 2019, 36, 2471–2479. [Google Scholar] [CrossRef] [Green Version]
- Haahr, T.; Jensen, J.S.; Thomsen, L.; Duus, L.; Rygaard, K.; Humaidan, P. Abnormal vaginal microbiota may be associated with poor reproductive outcomes: A prospective study in IVF patients. Hum. Reprod. 2016, 31, 795–803. [Google Scholar] [CrossRef] [Green Version]
- Haahr, T.; Humaidan, P.; Elbaek, H.O.; Alsbjerg, B.; Laursen, R.J.; Rygaard, K.; Johannesen, T.B.; Andersen, P.S.; Ng, K.L.; Jensen, J.S. Vaginal Microbiota and In Vitro Fertilization Outcomes: Development of a Simple Diagnostic Tool to Predict Patients at Risk of a Poor Reproductive Outcome. J. Infect. Dis 2019, 219, 1809–1817. [Google Scholar] [CrossRef]
- Skarin, A.; Sylwan, J. Vaginal lactobacilli inhibiting growth of Gardnerella vaginalis, Mobiluncus and other bacterial species cultured from vaginal content of women with bacterial vaginosis. Acta Pathol. Microbiol. Immunol. Scand. B 1986, 94, 399–403. [Google Scholar] [CrossRef]
- Sirota, I.; Zarek, S.M.; Segars, J.H. Potential influence of the microbiome on infertility and assisted reproductive technology. Semin. Reprod. Med. 2014, 32, 35–42. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variable | Category | All Subjects (N = 88) | Unfavorable (N = 49) | Favorable (N = 39) | p-Value |
|---|---|---|---|---|---|
| Age (years) | Mean ± SD | 35.1 ± 3.0 | 35.3 ± 3.4 | 35.0 ± 2.6 | 0.659 * |
| Median (IQR) | 36 (33–37) | 36 (32–38) | 35 (33–37) | ||
| Range (min–max) | 24–40 | 29–39 | 24–40 | ||
| BMI (Kg/m2) | Mean ± SD | 22.1 ± 3.2 | 22.2 ± 3.1 | 22.0 ± 3.4 | 0.770 * |
| Median (IQR) | 21.5 (19.9–23.1) | 21.6 (20–22.6) | 21.3 (19.9–23.3) | ||
| Range (min–max) | 16.1–32.8 | 16.1–32.5 | 17.6–32.8 | ||
| Infertility—N(%) | 1 = Male infertility | 20 (22.7) | 13 (26.5) | 7 (17.9) | 0.627 # |
| 2 = Idiopathic | 13 (14.8) | 8 (16.3) | 5 (12.8) | ||
| 3 = Low ovarian reserve | 18 (20.5) | 10 (20.4) | 8 (20.5) | ||
| 1 + 3 = Male and Low ovarian reserve | 3 (3.4) | 1 (2.0) | 2 (5.1) | ||
| 4 = Ovulatory endocrine | 10 (11.4) | 6 (12.2) | 4 (10.3) | ||
| 5 = Endometriosis | 3 (3.4) | 2 (4.1) | 1 (2.6) | ||
| 6 = Multifactorials | 15 (17.0) | 8 (16.3) | 7 (17.9) | ||
| 7 = Tubal inferitility | 6 (6.8) | 1 (2.0) | 5 (12.8) | ||
| OAT—N(%) | 1 = Normal | 29 (33.0) | 10 (20.4) | 19 (48.7) | |
| 2 = Moderate | 50 (56.8) | 36 (73.5) | 14 (35.9) | 0.002 # | |
| 3 = Severe | 9 (10.2) | 3 (6.1) | 6 (15.4) | ||
| FSH—N(%) | 1 = Meropur | 17 (19.3) | 10 (20.4) | 7 (17.9) | 0.518 # |
| 2 = Pergoveris | 27 (30.7) | 13 (26.5) | 14 (35.9) | ||
| 3 = Bemfola | 43 (48.9) | 26 (53.1) | 17 (43.6) | ||
| 4 = Meropur + Ovaleap | 1 (1.1) | 0 (0.0) | 1 (2.6) | ||
| Diet—N(%) | 1 = Mediterranean | 74 (84.1) | 42 (85.7) | 32 (82.1) | 0.862 § |
| 2 = Vegetarian/Vegan | 14 (15.9) | 7 (14.3) | 7 (17.9) | ||
| Physical activity—N(%) | 1 = Low-intensity | 16 (18.2) | 7 (14.3) | 9 (23.1) | 0.675 # |
| 2 = Moderate-intensity | 64 (72.7) | 37 (75.5) | 27 (69.2) | ||
| 3 = High-intensity | 8 (9.1) | 5 (10.2) | 3 (7.7) | ||
| Smoking habits—N(%) | 1 = Smoker | 24 (27.3) | 12 (24.5) | 12 (30.8) | 0.677 § |
| 2 = Non-smoker | 64 (72.7) | 37 (75.5) | 27 (69.2) | ||
| Drink habits—N(%) | 1 = Drinker | 20 (22.7) | 12 (24.5) | 8 (20.5) | 0.835 § |
| 2 = Non-drinker | 52 (59.1) | 29 (59.2) | 23 (59.0) | ||
| 3 = Occasional-drinker | 16 (18.2) | 8 (16.3) | 8 (20.5) | ||
| Sexual activity—N(%) | 1 = <1 a week | 33 (37.5) | 18 (36.7) | 15 (38.5) | 0.777 § |
| 2 = 1–2 a week | 41 (46.6) | 22 (44.9) | 19 (48.7) | ||
| 3 = >2 a week | 14 (15.9) | 9 (18.4) | 5 (12.8) |
| Taxa Level | Cluster Number | Selected Bacteria (within Each Cluster) | Quantity | Statistics | Unfavorable (N = 49) | Favorable (N = 39) | p-Value # |
|---|---|---|---|---|---|---|---|
| Phylum | 1 | Proteobacteria * (Cluster Centroid) | Relative abundance (%) | Mean ± SD | 1.399 ± 4.952 | 5.140 ± 15.088 | - |
| Median (IQR) | 0.216 (0.146–0.364) | 0.267 (0.138–1.238) | |||||
| Z-score° | Mean ± SD | −0.175 ± 0.804 | 0.220 ± 1.176 | 0.065 | |||
| 2 | Verrucomicrobia | Relative abundance (%) | Mean ± SD | 0.012 ± 0.074 | 0.001 ± 0.002 | - | |
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.105 ± 1.251 | −0.132 ± 0.529 | 0.273 | |||
| Bacteroidetes | Relative abundance (%) | Mean ± SD | 4.091 ± 9.730 | 2.709 ± 6.412 | - | ||
| Median (IQR) | 0.102 (0.022–0.384) | 0.062 (0.021–0.283) | |||||
| Z-score° | Mean ± SD | 0.068 ± 0.997 | −0.086 ± 1.010 | 0.477 | |||
| Firmicutes | Relative abundance (%) | Mean ± SD | 82.180 ± 27.847 | 73.507 ± 35.960 | - | ||
| Median (IQR) | 96.456 (74.673–99.494) | 96.301 (40.668–99.508) | |||||
| Z-score° | Mean ± SD | 0.084 ± 0.921 | −0.106 ± 1.095 | 0.378 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | 0.086 ± 0.545 | −0.108 ± 0.379 | 0.063 | ||
| Family | 1 | unkn, Alphaproteobacteria(c) | Relative abundance (%) | Mean ± SD | 0.013 ± 0.020 | 0.031 ± 0.036 | - |
| Median (IQR) | 0.006 (0.003–0.015) | 0.020 (0.010–0.038) | |||||
| Z-score° | Mean ± SD | −0.373 ± 0.915 | 0.468 ± 0.910 | <0.001 | |||
| Yersiniaceae | Relative abundance (%) | Mean ± SD | 0.005 ± 0.013 | 0.039 ± 0.162 | - | ||
| Median (IQR) | 0.001 (0.000–0.003) | 0.003 (0.000–0.010) | |||||
| Z-score° | Mean ± SD | −0.252 ± 0.808 | 0.317 ± 1.131 | 0.007 | |||
| Streptococcaceae | Relative abundance (%) | Mean ± SD | 1.646 ± 5.198 | 3.808 ± 10.311 | - | ||
| Median (IQR) | 0.028 (0.016–0.145) | 0.061 (0.024–2.155) | |||||
| Z-score° | Mean ± SD | −0.199 ± 0.896 | 0.250 ± 1.077 | 0.036 | |||
| unkn, Mycoplasmatales (o) | Relative abundance (%) | Mean ± SD | 0.000 ± 0.001 | 0.101 ± 0.633 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.118 ± 0.258 | 0.148 ± 1.471 | 0.219 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | −0.235 ± 0.307 | 0.296 ± 0.545 | <0.001 | ||
| Genus | 1 | unkn, Alphaproteobacteria (c) | Relative abundance (%) | Mean ± SD | 0.013 ± 0.019 | 0.031 ± 0.036 | - |
| Median (IQR) | 0.006 (0.003–0.015) | 0.020 (0.010–0.038) | |||||
| Z-score° | Mean ± SD | −0.373 ± 0.914 | 0.469 ± 0.910 | <0.001 | |||
| Yersinia | Relative abundance (%) | Mean ± SD | 0.000 ± 0.000 | 0.006 ± 0.028 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.001) | |||||
| Z-score° | Mean ± SD | −0.246 ± 0.370 | 0.309 ± 1.393 | 0.009 | |||
| Bifidobacterium | Relative abundance (%) | Mean ± SD | 1.940 ± 12.454 | 10.856 ± 26.752 | - | ||
| Median (IQR) | 0.065 (0.030–0.112) | 0.076 (0.038–0.646) | |||||
| Z-score° | Mean ± SD | −0.239 ± 0.669 | 0.300 ± 1.248 | 0.011 | |||
| unkn, Mycoplasmataceae (f) | Relative abundance (%) | Mean ± SD | 0.000 ± 0.001 | 0.032 ± 0.198 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.175 ± 0.385 | 0.219 ± 1.419 | 0.066 | |||
| Proteus | Relative abundance (%) | Mean ± SD | 0.000 ± 0.000 | 0.104 ± 0.650 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.148 ± 0.300 | 0.186 ± 1.453 | 0.120 | |||
| Enterobacter | Relative abundance (%) | Mean ± SD | 0.004 ± 0.012 | 0.020 ± 0.066 | - | ||
| Median (IQR) | 0.001 (0.000–0.003) | 0.002 (0.000–0.006) | |||||
| Z-score° | Mean ± SD | −0.249 ± 0.826 | 0.313 ± 1.117 | 0.008 | |||
| unkn, Sphingomonadaceae (f) | Relative abundance (%) | Mean ± SD | 0.004 ± 0.006 | 0.015 ± 0.058 | - | ||
| Median (IQR) | 0.002 (0.001–0.004) | 0.004 (0.003–0.007) | |||||
| Z-score° | Mean ± SD | −0.295 ± 0.876 | 0.371 ± 1.033 | 0.002 | |||
| Acidaminococcus | Relative abundance (%) | Mean ± SD | 0.009 ± 0.059 | 0.010 ± 0.043 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.061 ± 0.927 | 0.077 ± 1.092 | 0.521 | |||
| Streptococcus | Relative abundance (%) | Mean ± SD | 1.645 ± 5.195 | 3.807 ± 10.310 | - | ||
| Median (IQR) | 0.028 (0.016–0.144) | 0.059 (0.023–2.155) | |||||
| Z-score° | Mean ± SD | −0.200 ± 0.899 | 0.251 ± 1.074 | 0.035 | |||
| Lactobacillus | Relative abundance (%) | Mean ± SD | 76.525 ± 32.162 | 67.472 ± 38.152 | - | ||
| Median (IQR) | 92.876 (67.735–98.344) | 91.819 (35.048–98.003) | |||||
| Z-score° | Mean ± SD | 0.092 ± 0.931 | −0.115 ± 1.082 | 0.338 | |||
| Micrococcus | Relative abundance (%) | Mean ± SD | 0.001 ± 0.002 | 0.007 ± 0.028 | - | ||
| Median (IQR) | 0.000 (0.000–0.001) | 0.000 (0.000–0.003) | |||||
| Z-score° | Mean ± SD | −0.296 ± 0.620 | 0.372 ± 1.245 | 0.001 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | −0.199 ± 0.193 | 0.250 ± 0.381 | <0.001 | ||
| 2 | Peptoniphilus | Relative abundance (%) | Mean ± SD | 0.240 ± 0.701 | 0.053 ± 0.154 | - | |
| Median (IQR) | 0.012 (0.006–0.066) | 0.008 (0.000–0.028) | |||||
| Z-score° | Mean ± SD | 0.211 ± 1.037 | −0.266 ± 0.896 | 0.025 | |||
| unkn, Lactobacillaceae (f) | Relative abundance (%) | Mean ± SD | 0.173 ± 0.147 | 0.130 ± 0.046 | - | ||
| Median (IQR) | 0.145 (0.119–0.172) | 0.133 (0.102–0.162) | |||||
| Z-score° | Mean ± SD | 0.176 ± 1.019 | −0.222 ± 0.941 | 0.063 | |||
| Lacunisphaera | Relative abundance (%) | Mean ± SD | 0.003 ± 0.022 | 0.000 ± 0.000 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.113 ± 1.335 | −0.142 ± 0.011 | 0.236 | |||
| Dakarella | Relative abundance (%) | Mean ± SD | 0.007 ± 0.042 | 0.000 ± 0.000 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.152 ± 1.312 | −0.191 ± 0.216 | 0.110 | |||
| Haemophilus | Relative abundance (%) | Mean ± SD | 0.038 ± 0.139 | 0.169 ± 0.809 | - | ||
| Median (IQR) | 0.000 (0.000–0.003) | 0.000 (0.000–0.001) | |||||
| Z-score° | Mean ± SD | 0.057 ± 0.959 | −0.071 ± 1.058 | 0.554 | |||
| unkn, Atopobiaceae (f) | Relative abundance (%) | Mean ± SD | 0.062 ± 0.222 | 0.027 ± 0.116 | - | ||
| Median (IQR) | 0.003 (0.002–0.007) | 0.002 (0.001–0.006) | |||||
| Z-score° | Mean ± SD | 0.104 ± 1.055 | −0.131 ± 0.923 | 0.277 | |||
| Phascolarctobacterium | Relative abundance (%) | Mean ± SD | 0.003 ± 0.020 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.095 ± 1.300 | −0.119 ± 0.359 | 0.322 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | 0.130 ± 0.437 | −0.163 ± 0.271 | <0.001 | ||
| Species | 1 | unkn, Alphaproteobacteria (c) | Relative abundance (%) | Mean ± SD | 0.013 ± 0.019 | 0.031 ± 0.036 | - |
| Median (IQR) | 0.006 (0.003–0.015) | 0.020 (0.010–0.038) | |||||
| Z-score° | Mean ± SD | −0.373 ± 0.914 | 0.469 ± 0.910 | <0.001 | |||
| unkn, Serratia (g) | Relative abundance (%) | Mean ± SD | 0.003 ± 0.006 | 0.014 ± 0.047 | - | ||
| Median (IQR) | 0.001 (0.000–0.001) | 0.002 (0.000–0.008) | |||||
| Z-score° | Mean ± SD | −0.299 ± 0.775 | 0.376 ± 1.127 | 0.001 | |||
| Lactobacillus psittaci | Relative abundance (%) | Mean ± SD | 0.009 ± 0.012 | 0.036 ± 0.071 | - | ||
| Median (IQR) | 0.006 (0.003–0.010) | 0.009 (0.003–0.020) | |||||
| Z-score° | Mean ± SD | −0.190 ± 0.729 | 0.239 ± 1.230 | 0.045 | |||
| unkn, Bifidobacterium (g) | Relative abundance (%) | Mean ± SD | 1.793 ± 12.073 | 7.734 ± 22.655 | - | ||
| Median (IQR) | 0.037 (0.016–0.063) | 0.046 (0.026–0.339) | |||||
| Z-score° | Mean ± SD | −0.222 ± 0.699 | 0.279 ± 1.236 | 0.019 | |||
| Streptococcus sanguinis | Relative abundance (%) | Mean ± SD | 0.005 ± 0.016 | 0.008 ± 0.027 | - | ||
| Median (IQR) | 0.000 (0.000–0.002) | 0.000 (0.000–0.005) | |||||
| Z-score° | Mean ± SD | −0.133 ± 0.960 | 0.167 ± 1.036 | 0.163 | |||
| unkn, Mycoplasmatales (o) | Relative abundance (%) | Mean ± SD | 0.000 ± 0.001 | 0.101 ± 0.633 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.118 ± 0.258 | 0.148 ± 1.471 | 0.219 | |||
| Streptococcus anginosus | Relative abundance (%) | Mean ± SD | 0.045 ± 0.294 | 0.314 ± 0.990 | - | ||
| Median (IQR) | 0.001 (0.000–0.002) | 0.002 (0.000–0.023) | |||||
| Z-score° | Mean ± SD | −0.271 ± 0.684 | 0.340 ± 1.218 | 0.004 | |||
| Lactobacillus crispatus | Relative abundance (%) | Mean ± SD | 0.221 ± 0.226 | 0.452 ± 0.724 | - | ||
| Median (IQR) | 0.089 (0.016–0.482) | 0.171 (0.026–0.583) | |||||
| Z-score° | Mean ± SD | −0.103 ± 0.949 | 0.130 ± 1.059 | 0.280 | |||
| Yersinia pseudotuberculosis | Relative abundance (%) | Mean ± SD | 0.000 ± 0.000 | 0.005 ± 0.026 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.207 ± 0.289 | 0.260 ± 1.435 | 0.029 | |||
| Lactobacillus fermentum | Relative abundance (%) | Mean ± SD | 0.007 ± 0.035 | 0.086 ± 0.398 | - | ||
| Median (IQR) | 0.000 (0.000–0.001) | 0.000 (0.000–0.001) | |||||
| Z-score° | Mean ± SD | −0.142 ± 0.757 | 0.178 ± 1.228 | 0.137 | |||
| Lactobacillus coleohominis | Relative abundance (%) | Mean ± SD | 0.014 ± 0.053 | 0.032 ± 0.098 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.001) | |||||
| Z-score° | Mean ± SD | −0.131 ± 0.863 | 0.164 ± 1.139 | 0.170 | |||
| Streptococcus urinalis | Relative abundance (%) | Mean ± SD | 0.000 ± 0.000 | 0.039 ± 0.243 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.150 ± 0.157 | 0.189 ± 1.481 | 0.114 | |||
| Lactobacillus casei | Relative abundance (%) | Mean ± SD | 0.000 ± 0.001 | 0.003 ± 0.017 | - | ||
| Median (IQR) | 0.000 (0.000–0.001) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.242 ± 0.667 | 0.305 ± 1.248 | 0.010 | |||
| unkn, Proteus (g) | Relative abundance (%) | Mean ± SD | 0.000 ± 0.000 | 0.068 ± 0.423 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.142 ± 0.266 | 0.178 ± 1.463 | 0.137 | |||
| unkn, Sphingomonadaceae (f) | Relative abundance (%) | Mean ± SD | 0.004 ± 0.006 | 0.015 ± 0.058 | - | ||
| Median (IQR) | 0.002 (0.001–0.004) | 0.004 (0.003–0.007) | |||||
| Z-score° | Mean ± SD | −0.295 ± 0.876 | 0.371 ± 1.033 | 0.002 | |||
| Lactobacillus vaginalis | Relative abundance (%) | Mean ± SD | 0.001 ± 0.008 | 0.005 ± 0.030 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.094 ± 0.813 | 0.118 ± 1.195 | 0.327 | |||
| unkn, Micrococcus (g) | Relative abundance (%) | Mean ± SD | 0.001 ± 0.002 | 0.006 ± 0.028 | - | ||
| Median (IQR) | 0.000 (0.000–0.001) | 0.000 (0.000–0.002) | |||||
| Z-score° | Mean ± SD | −0.307 ± 0.614 | 0.386 ± 1.241 | 0.001 | |||
| Lactobacillus iners | Relative abundance (%) | Mean ± SD | 22.349 ± 36.633 | 16.920 ± 32.134 | - | ||
| Median (IQR) | 0.380 (0.214–34.653) | 0.428 (0.284–1.786) | |||||
| Z-score° | Mean ± SD | 0.068 ± 1.067 | −0.086 ± 0.916 | 0.475 | |||
| Lactobacillus delbrueckii | Relative abundance (%) | Mean ± SD | 0.093 ± 0.274 | 0.531 ± 2.978 | - | ||
| Median (IQR) | 0.037 (0.011–0.094) | 0.036 (0.013–0.103) | |||||
| Z-score° | Mean ± SD | −0.057 ± 0.995 | 0.072 ± 1.014 | 0.552 | |||
| unkn, Atopobiaceae (f) | Relative abundance (%) | Mean ± SD | 0.062 ± 0.222 | 0.027 ± 0.116 | - | ||
| Median (IQR) | 0.003 (0.002–0.007) | 0.002 (0.001–0.006) | |||||
| Z-score° | Mean ± SD | 0.104 ± 1.055 | −0.131 ± 0.923 | 0.277 | |||
| Lactobacillus salivarius | Relative abundance (%) | Mean ± SD | 0.004 ± 0.022 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.043 ± 1.317 | 0.054 ± 0.303 | 0.655 | |||
| unkn, Veillonellales (o) | Relative abundance (%) | Mean ± SD | 0.021 ± 0.098 | 0.001 ± 0.003 | - | ||
| Median (IQR) | 0.000 (0.000–0.001) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.052 ± 1.270 | −0.065 ± 0.496 | 0.591 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | −0.150 ± 0.106 | 0.188 ± 0.222 | <0.001 | ||
| 2 | unkn, Lactobacillaceae (f) | Relative abundance (%) | Mean ± SD | 0.173 ± 0.147 | 0.130 ± 0.046 | - | |
| Median (IQR) | 0.145 (0.119–0.172) | 0.133 (0.102–0.162) | |||||
| Z-score° | Mean ± SD | 0.176 ± 1.019 | −0.222 ± 0.941 | 0.063 | |||
| Anaerococcus prevotii | Relative abundance (%) | Mean ± SD | 0.018 ± 0.109 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.215 ± 1.275 | −0.270 ± 0.320 | 0.023 | |||
| Staphylococcus epidermidis | Relative abundance (%) | Mean ± SD | 0.010 ± 0.027 | 0.021 ± 0.093 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.110 ± 1.023 | −0.139 ± 0.965 | 0.249 | |||
| Atopobium vaginae | Relative abundance (%) | Mean ± SD | 3.620 ± 13.759 | 1.647 ± 10.286 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.145 ± 1.173 | −0.183 ± 0.700 | 0.127 | |||
| unkn, Firmicutes (p) | Relative abundance (%) | Mean ± SD | 0.080 ± 0.282 | 0.013 ± 0.013 | - | ||
| Median (IQR) | 0.011 (0.007–0.024) | 0.009 (0.006–0.013) | |||||
| Z-score° | Mean ± SD | 0.201 ± 1.141 | −0.253 ± 0.725 | 0.033 | |||
| unkn, Chryseolinea (g) | Relative abundance (%) | Mean ± SD | 0.003 ± 0.018 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.054 ± 1.291 | −0.068 ± 0.420 | 0.573 | |||
| Haemophilus parainfluenzae | Relative abundance (%) | Mean ± SD | 0.003 ± 0.019 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.072 ± 1.300 | −0.090 ± 0.375 | 0.454 | |||
| Anaerococcus hydrogenalis | Relative abundance (%) | Mean ± SD | 0.002 ± 0.006 | 0.004 ± 0.020 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.081 ± 1.035 | −0.101 ± 0.957 | 0.399 | |||
| Lactobacillus salivarius | Relative abundance (%) | Mean ± SD | 0.004 ± 0.022 | 0.000 ± 0.001 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.043 ± 1.317 | 0.054 ± 0.303 | 0.655 | |||
| Peptoniphilus lacrimalis | Relative abundance (%) | Mean ± SD | 0.043 ± 0.210 | Absent | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | ||||||
| Z-score° | Mean ± SD | 0.173 ± 1.321 | Absent | 0.041 § | |||
| Staphylococcus lugdunensis | Relative abundance (%) | Mean ± SD | 0.006 ± 0.040 | 0.000 ± 0.003 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.044 ± 1.205 | −0.055 ± 0.669 | 0.646 | |||
| Haemophilus sp., CCUG 17210 | Relative abundance (%) | Mean ± SD | 0.009 ± 0.061 | Absent | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | ||||||
| Z-score° | Mean ± SD | 0.085 ± 1.340 | Absent | 0.372 § | |||
| Lactobacillus rhamnosus | Relative abundance (%) | Mean ± SD | 0.003 ± 0.018 | 0.000 ± 0.002 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | −0.004 ± 1.203 | 0.005 ± 0.678 | 0.966 | |||
| Peptoniphilus timonensis | Relative abundance (%) | Mean ± SD | 0.007 (0.047) | Absent | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | ||||||
| Z-score° | Mean ± SD | 0.065 ± 1.343 | Absent | 0.041 § | |||
| Morganella morganii | Relative abundance (%) | Mean ± SD | 0.014 ± 0.098 | 0.000 ± 0.002 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.022 ± 1.244 | −0.027 ± 0.578 | 0.822 | |||
| Veillonella sp., DNF00314 | Relative abundance (%) | Mean ± SD | 0.012 ± 0.060 | Absent | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | ||||||
| Z-score° | Mean ± SD | 0.121 ± 1.334 | Absent | 0.204 § | |||
| Sphingomonas echinoides | Relative abundance (%) | Mean ± SD | 0.059 ± 0.070 | 0.206 ± 0.770 | - | ||
| Median (IQR) | 0.043 (0.000–0.079) | 0.040 (0.000–0.135) | |||||
| Z-score° | Mean ± SD | 0.052 ± 0.870 | −0.065 ± 1.151 | 0.587 | |||
| Lactobacillus iners | Relative abundance (%) | Mean ± SD | 22.349 ± 36.633 | 16.920 ± 32.134 | - | ||
| Median (IQR) | 0.380 (0.214–34.653) | 0.428 (0.284–1.786) | |||||
| Z-score° | Mean ± SD | 0.068 ± 1.067 | −0.086 ± 0.916 | 0.475 | |||
| Lactobacillus helveticus | Relative abundance (%) | Mean ± SD | 0.176 ± 0.180 | 0.183 ± 0.217 | - | ||
| Median (IQR) | 0.047 (0.019–0.384) | 0.049 (0.017–0.407) | |||||
| Z-score° | Mean ± SD | 0.040 ± 0.964 | −0.051 ± 1.054 | 0.673 | |||
| unkn, Alloscardovia (g) | Relative abundance (%) | Mean ± SD | 0.008 ± 0.039 | 0.003 ± 0.008 | - | ||
| Median (IQR) | 0.000 (0.000–0.000) | 0.000 (0.000–0.000) | |||||
| Z-score° | Mean ± SD | 0.029 ± 1.072 | −0.037 ± 0.914 | 0.760 | |||
| Cluster centroid | Z-score (means) | Mean ± SD | 0.085 ± 0.207 | −0.107 ± 0.140 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villani, A.; Fontana, A.; Barone, S.; de Stefani, S.; Primiterra, M.; Copetti, M.; Panebianco, C.; Parri, C.; Sciannamè, N.; Quitadamo, P.A.; et al. Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies. J. Clin. Med. 2022, 11, 680. https://doi.org/10.3390/jcm11030680
Villani A, Fontana A, Barone S, de Stefani S, Primiterra M, Copetti M, Panebianco C, Parri C, Sciannamè N, Quitadamo PA, et al. Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies. Journal of Clinical Medicine. 2022; 11(3):680. https://doi.org/10.3390/jcm11030680
Chicago/Turabian StyleVillani, Annacandida, Andrea Fontana, Stefano Barone, Silvia de Stefani, Mariangela Primiterra, Massimiliano Copetti, Concetta Panebianco, Cristiana Parri, Natale Sciannamè, Pasqua Anna Quitadamo, and et al. 2022. "Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies" Journal of Clinical Medicine 11, no. 3: 680. https://doi.org/10.3390/jcm11030680
APA StyleVillani, A., Fontana, A., Barone, S., de Stefani, S., Primiterra, M., Copetti, M., Panebianco, C., Parri, C., Sciannamè, N., Quitadamo, P. A., Tiezzi, A., Santana, L., Maglione, A., D’Amato, F., Perri, F., Palini, S., & Pazienza, V. (2022). Identifying Predictive Bacterial Markers from Cervical Swab Microbiota on Pregnancy Outcome in Woman Undergoing Assisted Reproductive Technologies. Journal of Clinical Medicine, 11(3), 680. https://doi.org/10.3390/jcm11030680