
A Systematic Literature Review of the Relationship between Serum Ferritin and Outcomes in Myelodysplastic Syndromes

 ,
,
Abstract
:1. Introduction
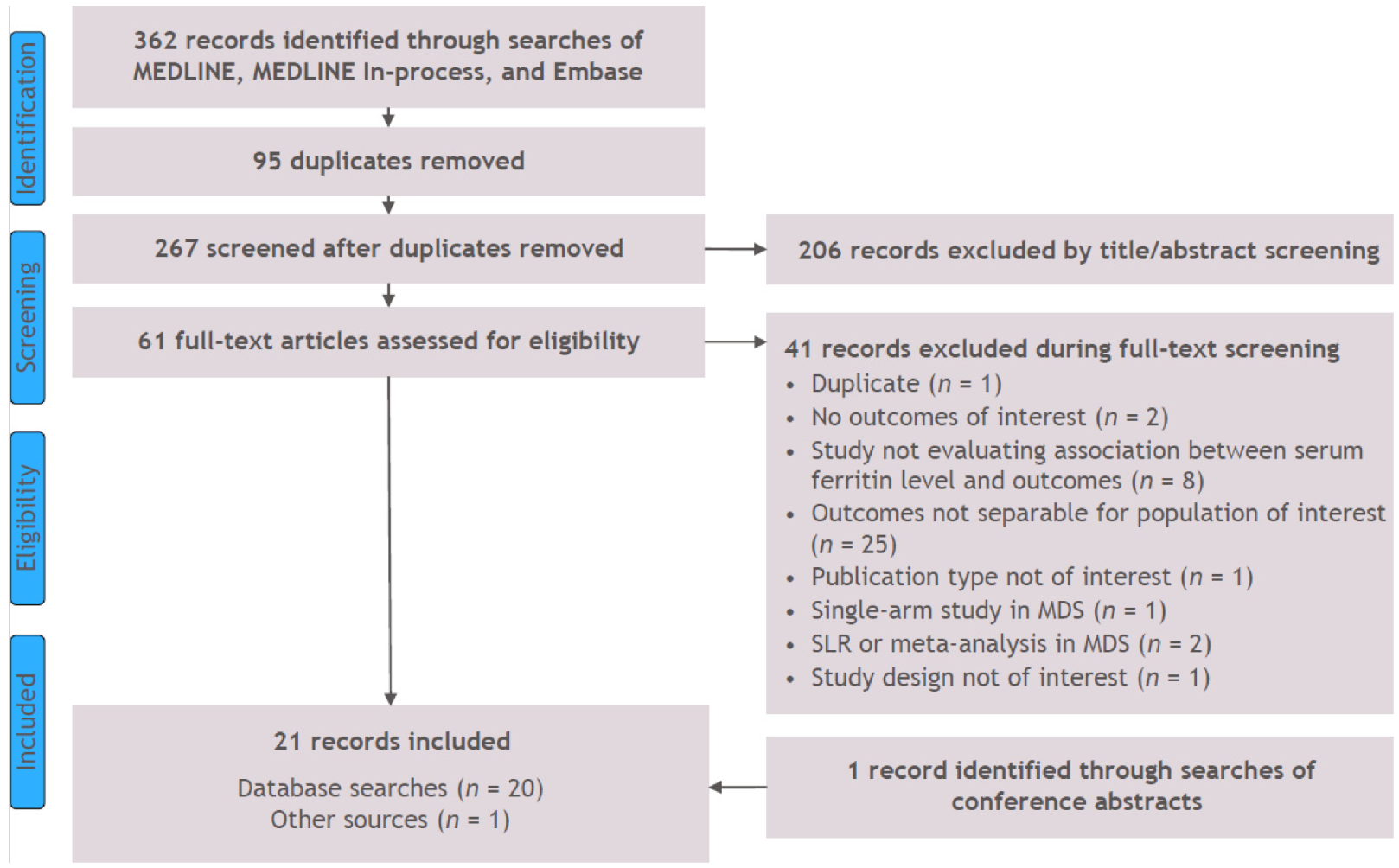
2. Methods
3. Results
3.1. Survival and Mortality
3.2. Progressive Disease and Relapse
3.2.1. Event-Free Survival
3.2.2. Relapse-Free Survival
3.2.3. Relapse Incidence
3.2.4. Leukemia-Free Survival
3.2.5. Transformation to AML
3.3. Additional Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cogle, C.R. Incidence and burden of the myelodysplastic syndromes. Curr. Hematol. Malig. Rep. 2015, 10, 272–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ades, L.; Itzykson, R.; Fenaux, P. Myelodysplastic syndromes. Lancet 2014, 383, 2239–2252. [Google Scholar] [CrossRef]
- Chan, L.S.; Shapiro, R.; Buckstein, R.; Lin, Y.; Callum, J.; Chodirker, L.; Lee, C.D.; Prica, A.; Lam, A.; Mamedov, A.; et al. Initial transfusion intensity predicts survival in myelodysplastic syndrome. Leuk. Lymphoma 2014, 55, 2296–2300. [Google Scholar] [CrossRef] [PubMed]
- Ribeil, J.A.; Arlet, J.B.; Dussiot, M.; Moura, I.C.; Courtois, G.; Hermine, O. Ineffective erythropoiesis in ß-Thalassemia. Sci. World J. 2013, 2013, 394295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temraz, S.; Santini, V.; Musallam, K.; Taher, A. Iron overload and chelation therapy in myelodysplastic syndromes. Crit. Rev. Oncol. Hematol. 2014, 91, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Sirlin, C.B.; Reeder, S.B. Magnetic resonance imaging quantification of liver iron. Magn. Reson. Imaging Clin. N. Am. 2010, 18, 359–381. [Google Scholar] [CrossRef] [Green Version]
- Majd, Z.; Haghpanah, S.; Ajami, G.H.; Matin, S.; Namazi, H.; Bardestani, M.; Karimi, M. Serum ferritin levels correlation with heart and liver MRI and LIC in patients with transfusion-dependent thalassemia. Iran Red Crescent Med. J. 2015, 17, e24959. [Google Scholar] [CrossRef] [Green Version]
- Brittenham, G.M. Iron-chelating therapy for transfusional iron overload. N. Engl. J. Med. 2011, 364, 146–156. [Google Scholar] [CrossRef]
- Sanz, G.; Nomdedeu, B.; Such, E.; Bernal, T.; Belkaid, M.; Ardanaz, M.T.; Marco, V.; Pedro, C.; Ramos, F.; del Cañizo, M.C.; et al. Independent impact of iron overload and transfusion dependency on survival and leukemic evolution in patients with myelodysplastic syndrome. Blood 2008, 112, 640. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; PRISMA Group. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Int. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- National Institute for Health and Care Excellence (NICE). NICE Guidance PMG9: Guide to the Methods of Technology Appraisal. 2013. Available online: https://www.nice.org.uk/process/pmg9/chapter/foreword (accessed on 1 February 2022).
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Cote, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Int. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Cakar, M.K.; Yegin, Z.A.; Baysal, N.A.; Altindal, S.; Pamukcuoglu, M.; Celik, B.; Yenicesu, I. Adverse impact of hyperferritinemia and transfusion dependency on treatment success in myelodysplastic syndrome. Transfus. Apher. Sci. 2013, 48, 397–401. [Google Scholar] [CrossRef]
- Cermak, J.; Kacirkova, P.; Mikulenkova, D.; Michalova, K. Impact of transfusion dependency on survival in patients with early myelodysplastic syndrome without excess of blasts. Leuk. Res. 2009, 33, 1469–1474. [Google Scholar] [CrossRef] [PubMed]
- Cremers, E.M.P.; de Witte, T.; de Wreede, L.; Eikema, D.J.; Koster, L.; van Biezen, A.; Finke, J.; Socie, G.; Beelen, D.; Maertens, J.; et al. A prospective non-interventional study on the impact of transfusion burden and related iron toxicity on outcome in myelodysplastic syndromes undergoing allogeneic hematopoietic cell transplantation. Leuk. Lymphoma 2019, 60, 2404–2414. [Google Scholar] [CrossRef]
- Diamantopoulos, P.T.; Kotsianidis, I.; Symeonidis, A.; Pappa, V.; Galanpoulos, A.; Gogos, D.; Karakatsanis, S.; Papadaki, H.; Hatzmichael, E.; Dimou, M.; et al. Chronic myelomonocytic leukemia treated with 5-azacytidine-results from the Hellenic 5-Azacytidine Registry: Proposal of a new risk stratification system. Leuk. Lymphoma 2019, 60, 1721–1730. [Google Scholar] [CrossRef]
- Escudero-Vilaplana, V.; Garcia-Gonzalez, X.; Osorio-Prendes, S.; Romero-Jimenez, R.M.; Sanjurjo-Saez, M. Impact of medication adherence on the effectiveness of deferasirox for the treatment of transfusional iron overload in myelodysplastic syndrome. J. Clin. Pharm. Ther. 2016, 41, 59–63. [Google Scholar] [CrossRef]
- Irwin, J.; D’Souza, A.; Johnson, L.; Carter, J. Myelodysplasia in the Wellington region 2002-2007: Disease incidence and treatment patterns. Intern. Med. J. 2011, 41, 399–407. [Google Scholar] [CrossRef]
- Kadlckova, E.; Rohon, P.; Fürst, T.; Cervinek, L.; Jonasova, A.; Salek, T.; Tesar, J.; Stavarova, Y. Verification of survival predictors in elderly patients with myelodysplastic syndrome from outpatient clinical practice. Int. J. Gerontol. 2018, 12, 27–31. [Google Scholar] [CrossRef]
- Kawabata, H.; Usuki, K.; Shindo-Ueda, M.; Kanda, J.; Tohyama, K.; Matsuda, A.; Araseki, K.; Hata, T.; Suzuki, T.; Kayano, H.; et al. Serum ferritin levels at diagnosis predict prognosis in patients with low blast count myelodysplastic syndromes. Int. J. Hematol. 2019, 110, 533–542. [Google Scholar] [CrossRef]
- Kikuchi, S.; Kobune, M.; Iyama, S.; Sato, T.; Murase, K.; Kawano, Y.; Takada, K.; Ono, K.; Hayashi, T.; Miyanishi, K.; et al. Prognostic significance of serum ferritin level at diagnosis in myelodysplastic syndrome. Int. J. Hematol. 2012, 95, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Xu, Z.; Gale, R.P.; Qin, T.; Zhang, Y.; Xiao, Z. Serum ferritin is an independent prognostic factor in Chinese with myelodysplastic syndromes classified as IPSS Intermediate-1. Acta. Haematol. 2013, 129, 243–250. [Google Scholar] [CrossRef]
- Lucijanic, M.; Pejsa, V.; Mitrovic, Z.; Štoos-Veić, T.; Livun, A.; Jakšić, O.; Vasilj, T.; Piršić, M.; Hariš, V.; Prka, Z.; et al. Hemochromatosis gene mutations may affect the survival of patients with myelodysplastic syndrome. Hematology 2016, 21, 170–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oran, B.; Kongtim, P.; Popat, U.; de Lima, M.; Jabbour, E.; Lu, X.; Chen, J.; Rondon, R.; Kebriaei, P.; Ahmed, S.; et al. Cytogenetics, donor type, and use of hypomethylating agents in myelodysplastic syndrome with allogeneic stem cell transplantation. Biol. Blood Marrow Transplant. 2014, 20, 1618–1625. [Google Scholar] [CrossRef] [Green Version]
- Osanai, S.; Shiseki, M.; Yoshinaga, K.; Mori, N.; Tanaka, J. Clinical implication of serum ferritin level at diagnosis in patients with myelodysplastic syndromes. Hemasphere 2018, 2, 945. [Google Scholar]
- Park, S.; Sapena, R.; Kelaidi, C.; Vassilieff, D.; Bordessoule, D.; Stamatoullas, A.; Cheze, S.; Beyne-Rauzy, O.; Vey, N.; Rose, C.; et al. Ferritin level at diagnosis is not correlated with poorer survival in non RBC transfusion dependent lower risk de novo MDS. Leuk. Res. 2011, 35, 1530–1533. [Google Scholar] [CrossRef]
- Patnaik, M.M.; Lasho, T.L.; Finke, C.M.; Gangat, N.; Caramazza, D.; Holtan, S.G.; Pardanani, A.; Knudson, R.A.; Ketterling, R.P.; Chen, D.; et al. WHO-defined ‘myelodysplastic syndrome with isolated del(5q)’ in 88 consecutive patients: Survival data, leukemic transformation rates and prevalence of JAK2, MPL and IDH mutations. Leukemia 2010, 24, 1283–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prem, S.; Atenafu, E.G.; Lam, W.; Law, A.; Michelis, F.V.; Kim, D.; Viswabandya, A.; Lipton, J.H.; Mattsson, J.; Kumar, R. Allogeneic stem cell transplant in myelodysplastic syndrome-factors impacting survival. Eur. J. Haematol. 2020, 104, 116–124. [Google Scholar] [CrossRef]
- Risum, M.; Barfod, T.; Raaschou-Jensen, K. Transient elastography for the detection of hepatic iron overload in patients with myelodysplastic syndrome. Eur. Oncol. Haematol. 2016, 12, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Senturk Yikilmaz, A.; Akinci, S.; Bakanay, S.M.; Dilek, I. In myelodysplastic syndrome cases, what should be the level of ferritin which has prognostic value? Trans. Clin. Biol. 2019, 26, 217–223. [Google Scholar] [CrossRef]
- Sperr, W.R.; Wimazal, F.; Kundi, M.; Baumgartner, C.; Nösslinger, T.; Makrai, A.; Stauder, R.; Krieger, O.; Pfeilstöcker, M.; Valent, P. Comorbidity as prognostic variable in MDS: Comparative evaluation of the HCT-CI and CCI in a core dataset of 419 patients of the Austrian MDS study group. Ann. Oncol. 2010, 21, 114–119. [Google Scholar] [CrossRef]
- Waszczuk-Gajda, A.; Madry, K.; Machowicz, R.; Drozd-Sokolowska, J.; Stella-Holowiecka, B.; Mital, A.; Obara, A.; Szmigielska-Kaplon, A. Red blood cell transfusion dependency and hyperferritinemia are associated with impaired survival in patients diagnosed with myelodysplastic syndromes: Results from the first Polish MDS-PALG Registry. Adv. Clin. Exp. Med. 2016, 25, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.A.; Leitch, H.A. Iron chelation therapy in lower IPSS risk myelodysplastic syndromes; Which subtypes benefit? Leuk. Res. 2018, 64, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Thuret, I.; Hacini, M.; Pegourie-Bandelier, B.; Gardembas-Pain, M.; Bisot-Locard, S.; Merlat-Guitard, A.; Bachir, D. Socio-psychological impact of infused iron chelation therapy with deferoxamine in metropolitan France: ISOSFER study results. Hematology 2009, 14, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Efficace, F.; Santini, V.; La Nasa, G.; Cottone, F.; Finelli, C.; Borin, L.; Quaresmini, G.; Di Tucci, A.A.; Volpe, A.; Cilloni, D.; et al. Health-related quality of life in transfusion-dependent patients with myelodysplastic syndromes: A prospective study to assess the impact of iron chelation therapy. BMJ Support Palliat. Care. 2016, 6, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Durairaj, S.; Chew, S.; Hyslop, A.; Keenan, N.; Groves, M.J.; Tauro, S. Predicted costs of iron-chelators in myelodysplastic syndromes: A 10-year analysis based on actual prevalence and red cell transfusion rates. Am. J. Hematol. 2011, 86, 406–410. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Domain | Inclusion Criteria | Exclusion Criteria |
| Population | Adult (≥18 years) patients with MDS | Publications reporting on patient populations in the following categories:
|
| Prognostic/predictive factors | Studies must have assessed and reported SF levels using quantitative methods * | NA |
| Outcomes | Clinical outcomes
Economic outcomes:
| Publications that only report data on the following types of outcomes: pharmacokinetics/pharmacodynamics |
| Study designs |
| Publications of studies with the following designs:
|
| Systematic reviews and meta-analysis (will be included for reference checking only. Full papers will be excluded using a separate exclusion code) | ||
| Duplicate | If duplicates are identified, the copy of the record with the lower ref ID number will be included | Publications that are duplicates of other publications in the search yield The copy of the record with higher ref ID number will be excluded |
| Study limits | Only English language articles/conference abstracts were included | Journal articles and conference abstracts not in the English language |
| Studies published outside the timeframe of interest | |
| Geography | None | |
| Study Author, Year, Country | Study Design, Setting, Sample Size | Age | Male Gender | Duration Since Diagnosis | Proportion Transfusion Dependent and Definition | IPSS Risk Groups | FAB Risk Groups | WHO Risk Groups | Mean SF at Baseline * |
| Irwin, 2011 [20] New Zealand | Retrospective cohort Hospital 70 | Mean (SD), years: 69.8 (NR) | 60% | NR | NR defined as the requirement of at least 1 RBC unit per 8 weeks, over at least 4 months | Low: 41.5% Int-1: 35.0% Int-2: 15.0% High: 8.3% | Not diagnostic but consistent with MDS: 11.4% RA: 37.0% RARS: 12.8% RAEB: 28.6% RAEB-t: 0% CMML: 10.0% | Not diagnostic but consistent with MDS: 7.8% del(5q): 4.7% RA: 12.5% RARS: 12.5% RCMD: 25.0% RCMD-RS: 1.6% RAEB-1: 20.3% RAEB-2: 10.3% MU: 4.4% | 2963 µg/L |
| Park, 2011 [28] France | Registry NR/unclear 318 | Median (range), years: 77 (29–103) | 56% | NR | 0 (at registry entry) | 0: 44% 0.5: 25% 1: 11% NA by ≤1: 20% | NR | RA: 21% RCMD: 18% RARS and RCMD-RS: 25% RAEB-1: 20% del(5q): 5% Unclassifiable: 14% | Median (range), ng/mL: 283 (20–5558) |
| Waszczuk-Gajda, 2016 [34] Poland | Retrospective cohort In- or outpatient hematologic unit 190 | <50 years: 8%;50–80 years: 77%; >80 years: 15% | 58% | NR | 58 Defined as having at least 1 RBC transfusion within the last 8 weeks over a period of 4 months | (Available for a subset of 62 patients) Low risk: 16% Int-1: 34% Int-2: 29% High risk: 21% | NR | RA: 12.6% RARS: 3.7% RCMD: 26.3% RCMD-RS: 0.5% RAEB-1: 14.2% RAEB-2: 27.9% del(5q): 2.1% MDS-U: 4.2% | ≤1000 µg/L: 89 patients (81.7%) >1000 µg/L: 20 patients (18.3%) |
| Cakar, 2013 [15] Turkey | Retrospective cohort Blood center records 35 | Median (IQR), years: 60 (22–84) | 60% | NR | 62.8% needed a transfusion during follow-up | (Available for a subset of 33 patients) Low: 30.3% Int-1: 60.6% Int-2: 9.1% | NR | RCUD: 48.6% RCMD: 2.9% RAEB-1: 28.6% RAEB-2: 17.1% Isolated del(5q): 2.9% | At diagnosis: median (range), ng/mL: 198 (6.6–794) |
| Cermak, 2009 [16] Czech Republic | Retrospective cohort NR/unclear 137 | Mean (SD), years: 49.4 (17.8) | 54% | NR | NR | Low: 21.2% Int-1 and Int-2: 78.8% | NR | RCMD, RCMD-RS: 64.2% RA, RARS, del(5q): 35.8% | >2000 µg/L: 68 patients (49.6%) |
| Cremers, 2019 [17] European multi-country | Prospective cohort Hospital 222 | Median (range), years: 59.3 (19–76) | NR | Median interval between diagnosis and HSCT: 10 months (range 1–128) | NR | NR | NR | RA/RAS/del(5q)/RCMD-RS: 26% RAEB-1/RAEB-2: 56% AML-MDS: 7% CMML: 11% | Median (1st–3rd Quartile): 700 (261–1554) ≤1000 ng/mL: 115 patients (58%) >1000 ng/mL: 81 patients (41%) |
| Diamantopoulos, 2019 [18] Greece | Retrospective cohort NR/unclear 88 | Median (range), years: 73.4 (35–89) | 70.6% | NR | RBC transfusion needed: 46.6% | Low: 9% Int-1: 53.8% Int-2: 37.2% High: 0% | NR | CMML-1: 65.9% CMML-2: 34.1% | Median (range), ng/dL: 333 (24–1541) |
| Escudero-Vilaplana, 2015 [19] Spain | Retrospective cohort Hospital 35 | Median age at beginning of deferasirox treatment: 68.0 years | 51.4% | NR | NR | NR | NR | NR | Median (p25–p75), µg/L: 1636 µg/L (1100–1834) |
| Kadlckova, 2017 [21] Czech Republic | Prospective cohort Outpatient or clinic 73 | NR | 47% | NR | 50.1% | NR | NR | RA, RCUD, RARS, RCMD, MDS-U and MDS with isolated del(5q): 68.5% RAEB-1/RAEB-2: 23.3% CMML: 8.2% | NR |
| Kawabata, 2019 [22] Japan | Prospective cohort NR/unclear 107 | Median (range), years: 70 (20–94) | 67.3% | NR | NR | NR | RA: 79.4% RARS: 17.8% CMML: 2.8% | MDS-isolated-del(5q): 1.9% MDS-SLD: 21.5% MDS-RS-SLD: 1.9% MDS-MLD: 42.1% MDS-RS-MLD: 14% MDS-F: 0.9% MDS-U: 11.2% CMML-0: 2.8% MDS/MPN-RS-T: 1.9% MDS/MPN-U: 1.9% | Median (range), ng/mL: 204 (<7 to 14,040) |
| Kikuchi, 2012 [23] Japan | Retrospective cohort Hospital 47 | Low SF group, median (range), years: 67 (27–86); High SF group, median (range), years: 63 (39–74) | Low SF group (n = 37): 51.4%; High SF group (n = 10): 90% | NR | 0 | Low SF group (n = 37): Low: 18.9% Int-1: 56.8% Int-2: 18.9% High: 5.4%; High SF group (n = 10): Low: 0% Int-1: 40% Int-2: 50% High: 10% | NR | Overall: RCUD: 34% RCMD: 36.2% RA + RAEB-1: 19.1% RA + RAEB-2: 10.6% | Low SF group (n = 37): Median (range), ng/mL: 158.7 (4.0–475.6); High SF group (n = 10): Median (range), ng/mL: 793.5 (519.0–1844.0) |
| Li, 2013 [24] China | Prospective cohort Hospital 191 | Median (range), years: 50 (12–83) | 62% | NR | NR | Int-1: 100% | NR | RA: 9% RARS: 9% RCMD: 58% RAEB-t: 15% del(5q): 0.5% MDS-U: 8% | Median (range), µg/L: 368 (8–3256) |
| Lucijanic, 2016 [25] Croatia | Prospective cohort NR/unclear 36 | Median (range), years: 74 (53–89) | 53% | NR | NR | NR | NR | RA: 36% RARS: 33% RAEB: 19% RAEB-1: 2/36 (6%) RAEB-2: 5/36 (14%) MDS-U: 8% del(5q): 1/36 (3%) | Unclear timepoint; median (range), µg/L: HFE mutated patients: 1113; HFE wild-type patients: 458 |
| Oran, 2014 [26] USA | Retrospective cohort Cancer center 256 | Median (IQR), years: 56 (48–62) | NR | Median (IQR), months): 8 (5.2–15.3) | NR | IPSS-R at diagnosis: Very Low/Low: 27.8% Int: 12.5% High: 15.3% Very High: 25.7% Missing: 18.8% | NR | RA or RARS: 15.6% RCMD: 13.7% Low/Int: 28.9% High risk: 39.1% RAEB-1: 17.6% RAEB-2: 21.5% CMML: 9% MDS-U: 23% T-MDS: 35.9% | Median (IQR), µg/L: 1131 (521–2246) |
| Patnaik, 2010 [29] USA | Retrospective cohort NR/unclear 88 | Median (range): 74 (28–89) years | 68.2% | NR | Transfusion need at diagnosis: 69% | NR | NR | MDS with isolated del(5q): 100% | At diagnosis: median (range), µg/L: 330 * (8–3599) |
| Prem, 2020 [30] Canada | Retrospective cohort Cancer center 125 | ≤65 years: 69.6% >65 years: 30.4% | 66.1% | NR | 44.8% | IPSS score: Low: 5.7% Int-1: 16.9% Int-2: 56.5% High: 21% Missing: n = 2 IPSS-R score: Very Low/Low: 12.2% Intermediate: 20.3% High: 33.3% Very High: 34.2% Missing: n = 2 | NR | MDS subtype: RA/RCMD/Hypoplastic MDS: 36% RAEB-1: 20.8% RAEB-2: 43.2% | >1000 ng/mL: 52.5% of patients ≤1000 ng/mL: 47.5% of patients |
| Risum, 2016 [31] Denmark | Prospective cohort hematologic center at hospital 60 | Median (range), years: 75.5 (46–94) | 63.3% | Median (range), months: 16.5 (0.5–186.5) | 35% | At diagnosis: (n) IPSS: (out of 56) Low: 24 Int-1: 24 Int-2: 5 High: 3 IPSS-R: (out of 56) Very Low: 12 Low: 29 Int: 7 High: 4 Very High: 4 At time of TE: (n) IPSS: (out of 57) Low: 29 Int-1: 16 Int-2: 5 High: 7 IPSS-R: (out of 57) Very Low: 21 Low: 18 Int: 6 High: 5 Very High: 7 | NR | At time of TE: (n) RA: 2 RARS: 16 RCMD: 19 RAEB-1: 4 RAEB-2: 4 MDS del(5q): 5 AML (progressed from MDS): 3 CMML: 6 MDS/MPN: 1 | Unclear timepoint: Transfusion dependent (n = 21), median (range), µg/L: 1035 (249–30,195); Transfusion independent (n = 39), median (range), µg/L: 390 (6–1866) |
| Senturk-Yikilmaz, 2019 [32] Turkey | Retrospective cohort Hospital 62 | Mean (SD), years: 67.7 (12.3) | 67.7% | NR | NR | NR | NR | MDS subtype: SF ≥ 400 ng/mL: RA: 9.7% RARS: 1.6% RCMD: 14.5% RCMD-RS: 1.6% RAEB-1/-2: 19.4% SF < 400 ng/mL: RA: 22.6% RARS: 1.6% RCMD: 19.4% RCMD-RS: 3.2% RAEB-1/-2: 6.5% | Median (range), ng/mL: 358.5 (29.8–2000) |
| Sperr, 2010 [33] Austria | Retrospective cohort Outpatient or clinic hematologic center 419 | Median (IQR), years: 71 (24–91) | 54.4% | NR | NR | Low: 135 (32.2%) Int-1: 158 (37.7%) Int-2: 79 (18.9%) High: 47 (11.2%) | RA: 128 (30.5%) RARS: 94 (23.4%) RAEB: 109 (26.0%) RAEB-t: 63 (15.0%) CMML: 25 (6.0%) | NR | NR |
| Wong, 2018 [35] Canada | Retrospective cohort Hospital 182 | ICT patients, median (range), years: 67 (32–87); Non-ICT patients, median (range), years: 74 (39–93) | ICT: 60.3% Non-ICT: 57.1% | NR | NR | ICT: Low: 47.6% Int-1: 42.9% ≤Int-1: 9.5% Non-ICT: Low: 38.7% Int-1: 58.0% ≤Int-1: 3.4% | FAB or WHO, depending on era ICT: RA: 20.6% RARS, RARS-t: 44.4% RCMD, RCMD-RS: 23.8% del(5q): 4.8% RAEB-1: 3.2% MDS-U/MDS/MPN-U: 3.2% Non-ICT: RA: 20.2% RARS, RARS-t: 26.1% RCMD, RCMD-RS: 31.1% del(5q): 5.0% RAEB-1: 10.1% MDS-U/MDS/ MPN-U: 9.4% | FAB or WHO, depending on era ICT: RA: 20.6% RARS, RARS-t: 44.4% RCMD, RCMD-RS: 23.8% del(5q): 4.8% RAEB-1: 3.2% MDS-U/MDS/MPN-U: 3.2% Non-ICT: RA: 20.2% RARS, RARS-t: 26.1% RCMD, RCMD-RS: 31.1% del(5q): 5.0% RAEB-1: 10.1% MDS-U/MDS/MPN-U: 9.4% | Median (range), ng/mL: ICT: 687 (49–6447); Non-ICT: 260 (31–7783) |
| Osanai, 2018 [27] Japan | Retrospective cohort NR/unclear 98 | Median (range), years: 71 (20–91) | 60.2% | NR | NR | NR | NR | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliva, E.N.; Huey, K.; Deshpande, S.; Turner, M.; Chitnis, M.; Schiller, E.; Tang, D.; Yucel, A.; Hughes, C.; Shah, F. A Systematic Literature Review of the Relationship between Serum Ferritin and Outcomes in Myelodysplastic Syndromes. J. Clin. Med. 2022, 11, 895. https://doi.org/10.3390/jcm11030895
Oliva EN, Huey K, Deshpande S, Turner M, Chitnis M, Schiller E, Tang D, Yucel A, Hughes C, Shah F. A Systematic Literature Review of the Relationship between Serum Ferritin and Outcomes in Myelodysplastic Syndromes. Journal of Clinical Medicine. 2022; 11(3):895. https://doi.org/10.3390/jcm11030895
Chicago/Turabian StyleOliva, Esther Natalie, Krystal Huey, Sohan Deshpande, Monica Turner, Madhura Chitnis, Emma Schiller, Derek Tang, Aylin Yucel, Christina Hughes, and Farrukh Shah. 2022. "A Systematic Literature Review of the Relationship between Serum Ferritin and Outcomes in Myelodysplastic Syndromes" Journal of Clinical Medicine 11, no. 3: 895. https://doi.org/10.3390/jcm11030895
APA StyleOliva, E. N., Huey, K., Deshpande, S., Turner, M., Chitnis, M., Schiller, E., Tang, D., Yucel, A., Hughes, C., & Shah, F. (2022). A Systematic Literature Review of the Relationship between Serum Ferritin and Outcomes in Myelodysplastic Syndromes. Journal of Clinical Medicine, 11(3), 895. https://doi.org/10.3390/jcm11030895