
Astaxanthin Relieves Testicular Ischemia-Reperfusion Injury—Immunohistochemical and Biochemical Analyses

 ,
,  , , , and
, , , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Ethics Approvals
2.3. Experimental Groups and Surgical Procedure
2.4. Immunohistochemical Method and Analysis
2.5. Biochemical Analysis
2.6. Statistical Analysis
3. Results
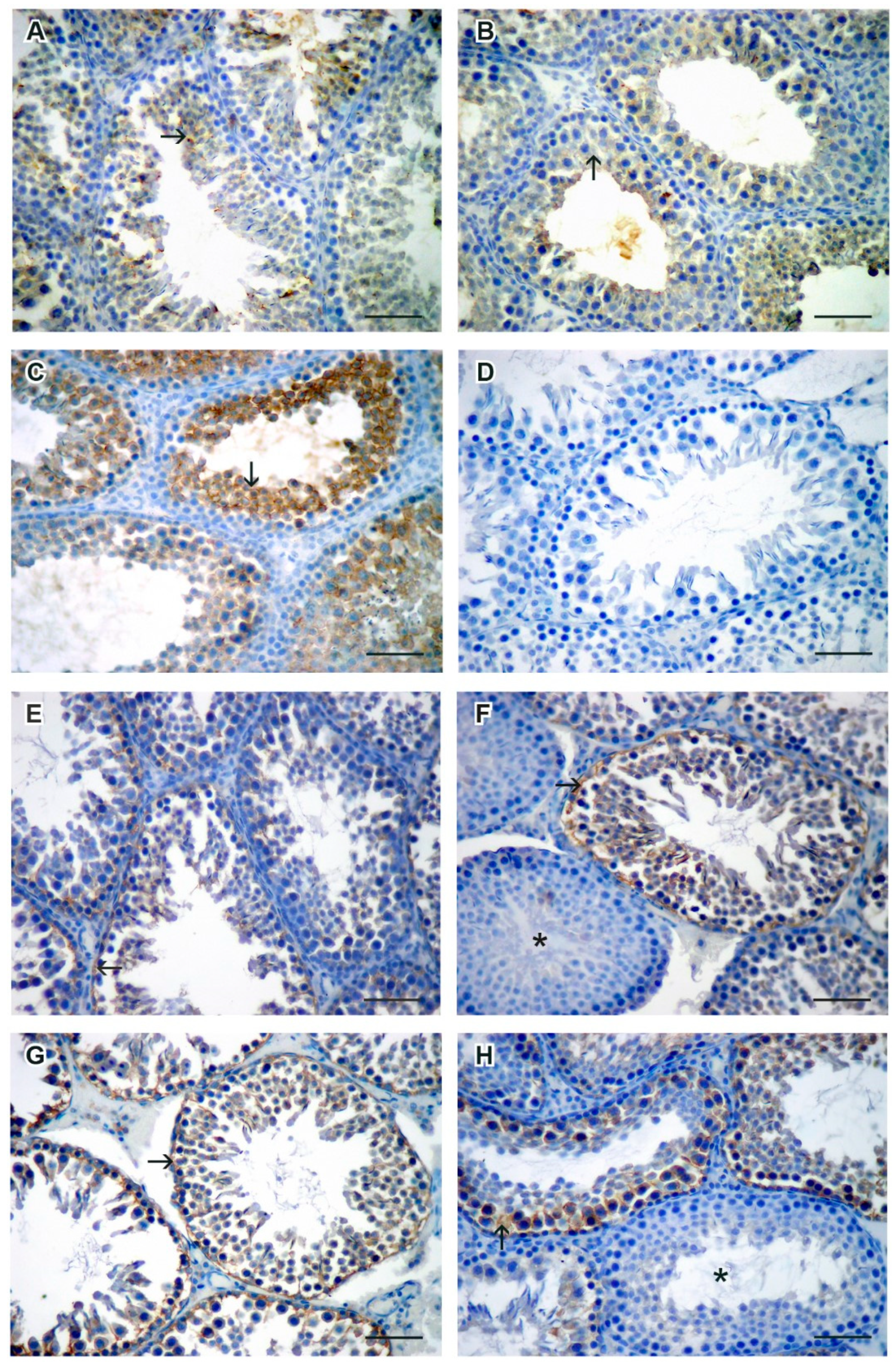
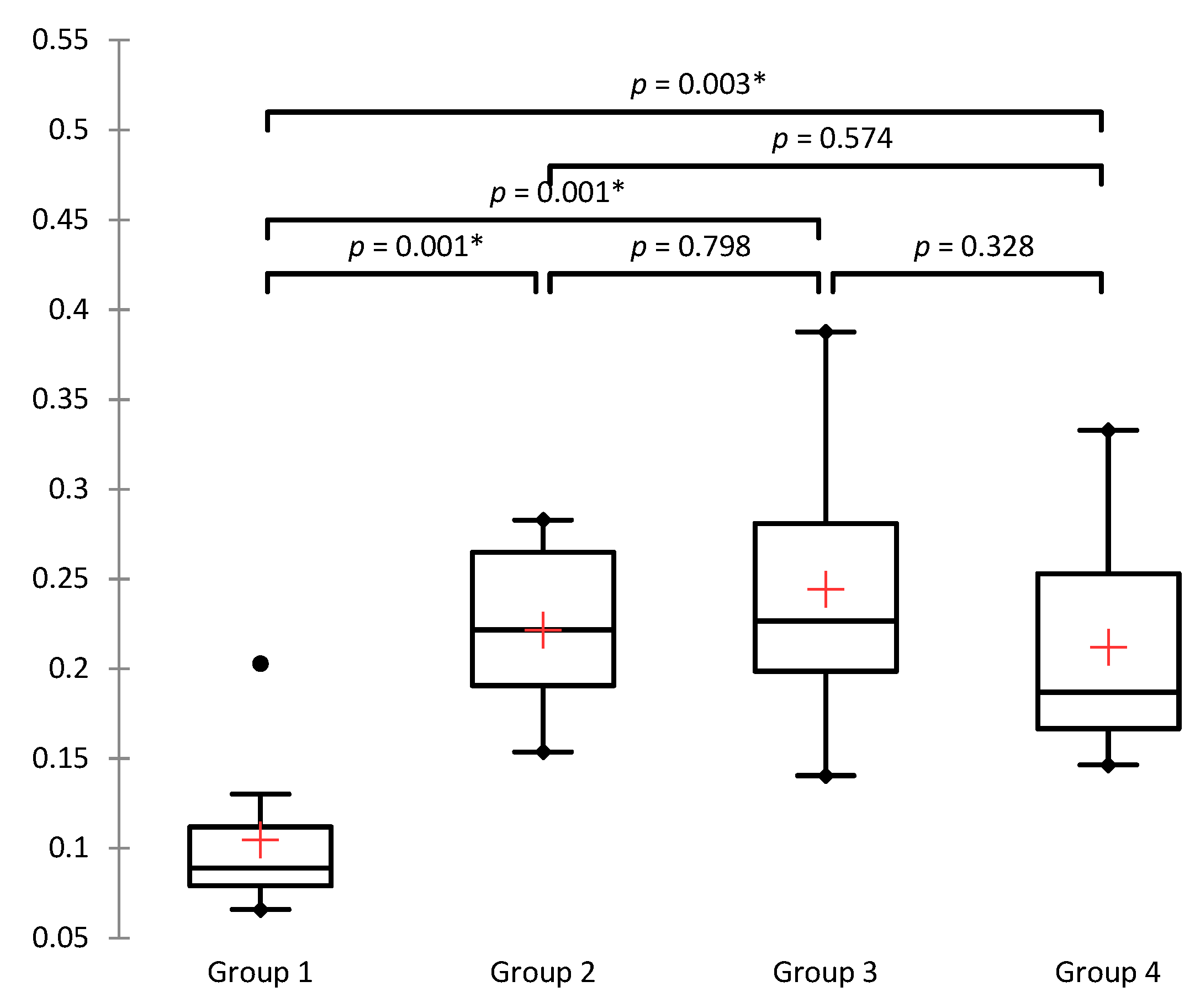
3.1. Caspase-3 Positive Cells Quantification
3.2. Histological Assessment of Oxidative Stress
3.3. Values of Malondialdehyde (MDA)
3.4. Values of Superoxide Dismutase (SOD)
3.5. Values of Glutathione Peroxidase (GPx)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mäkelä, E.; Lahdes-Vasama, T.; Rajakorpi, H.; Wikström, S. A 19-year review of paediatric patients with acute scrotum. Scand. J. Surg. 2007, 96, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Bowlin, P.R.; Gatti, J.M.; Murphy, J.P. Pediatric Testicular Torsion. Surg. Clin. N. Am. 2017, 97, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Ta, A.; D’Arcy, F.T.; Hoag, N.; D’Arcy, J.P.; Lawrentschuk, N. Testicular torsion and the acute scrotum: Current emergency management. Eur. J. Emerg. Med. 2016, 23, 160–165. [Google Scholar] [CrossRef]
- Watkin, N.A.; Reiger, N.A.; Moisey, C.U. Is the conservative management of the acute scrotum justified on clinical grounds? Br. J. Urol. 1996, 78, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Tajchner, L.; Larkin, J.O.; Bourke, M.G.; Waldron, R.; Barry, K.; Eustace, P.W. Management of the acute scrotum in a district general hospital: 10-year experience. Sci. World J. 2009, 9, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Hegarty, P.K.; Walsh, E.; Corcoran, M.O. Exploration of the acute scrotum: A retrospective analysis of 100 consecutive cases. Ir. J. Med. Sci. 2001, 170, 181–182. [Google Scholar] [CrossRef] [PubMed]
- Molokwu, C.N.; Somani, B.K.; Goodman, C.M. Outcomes of scrotal exploration for acute scrotal pain suspicious of testicular torsion: A consecutive case series of 173 patients. BJU Int. 2011, 107, 990–993. [Google Scholar] [CrossRef]
- Zhao, L.C.; Lautz, T.B.; Meeks, J.J.; Maizels, M. Pediatric testicular torsion epidemiology using a national database: Incidence, risk of orchiectomy and possible measures toward improving the quality of care. J. Urol. 2011, 186, 2009–2013. [Google Scholar] [CrossRef]
- Ben-Chaim, J.; Leibovitch, I.; Ramon, J.; Winberg, D.; Goldwasser, B. Etiology of acute scrotum at surgical exploration in children, adolescents and adults. Eur. Urol. 1992, 21, 45–47. [Google Scholar]
- Schick, M.A.; Sternard, B.T. Testicular Torsion. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Bašković, M.; Župančić, B.; Vukasović, I.; Štimac-Rojtinić, I.; Ježek, D. Validation of a TWIST Score in Diagnosis of Testicular Torsion—Single-Center Experience. Klin. Padiatr. 2019, 231, 217–219. [Google Scholar] [CrossRef]
- Kalogeris, T.; Baines, C.P.; Krenz, M.; Korthuis, R.J. Cell biology of ischemia/reperfusion injury. Int. Rev. Cell. Mol. Biol. 2012, 298, 229–317. [Google Scholar] [PubMed] [Green Version]
- Carden, D.L.; Granger, D.N. Pathophysiology of ischaemia-reperfusion injury. J. Pathol. 2000, 190, 255–266. [Google Scholar] [CrossRef]
- Grace, P.A.; Mathie, R.T. Ischemia-Reperfusion Injury; Blackwell Science: London, UK, 1999. [Google Scholar]
- Bellanti, F. Ischemia-reperfusion injury: Evidences for translational research. Ann. Transl. Med. 2016, 4, S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slegtenhorst, B.R.; Dor, F.J.; Rodriguez, H.; Voskuil, F.J.; Tullius, S.G. Ischemia/reperfusion Injury and its Consequences on Immunity and Inflammation. Curr. Transplant. Rep. 2014, 1, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Dhama, K. Oxidative stress, prooxidants, and antioxidants: The interplay. Biomed. Res. Int. 2014, 2014, 761264. [Google Scholar] [CrossRef] [Green Version]
- Chandra, J.; Samali, A.; Orrenius, S. Triggering and modulation of apoptosis by oxidative stress. Free. Radic. Biol. Med. 2000, 29, 323–333. [Google Scholar] [CrossRef]
- Hengartner, M.O. The biochemistry of apoptosis. Nature 2000, 407, 770–776. [Google Scholar] [CrossRef]
- Miguel, M.G. Antioxidant and anti-inflammatory activities of essential oils: A short review. Molecules 2010, 15, 9252–9287. [Google Scholar] [CrossRef] [Green Version]
- Manivannan, K.; Karthikai Devi, G.; Anantharaman, P.; Balasubramanian, T. Antimicrobial potential of selected brown seaweeds from Vedalai coastal waters, Gulf of Mannar. Asian Pac. J. Trop. Biomed. 2011, 1, 114–120. [Google Scholar] [CrossRef] [Green Version]
- Guerin, M.; Huntley, M.E.; Olaizola, M. Haematococcus astaxanthin: Applications for human health and nutrition. Trends Biotechnol. 2003, 21, 210–216. [Google Scholar] [CrossRef]
- Kidd, P. Astaxanthin, cell membrane nutrient with diverse clinical benefits and anti-aging potential. Altern. Med. Rev. 2011, 16, 355–364. [Google Scholar]
- Pashkow, F.J.; Watumull, D.G.; Campbell, C.L. Astaxanthin: A novel potential treatment for oxidative stress and inflammation in cardiovascular disease. Am. J. Cardiol. 2008, 101, 58–68. [Google Scholar] [CrossRef]
- Miki, W. Biological functions and activities of animal carotenoids. Pure. Appl. Chem. 1991, 63, 141–146. [Google Scholar] [CrossRef]
- Bašković, M.; Bojanac, A.K.; Sinčić, N.; Perić, M.H.; Krsnik, D.; Ježek, D. The effect of astaxanthin on testicular torsion-detorsion injury in rats-detailed morphometric evaluation of histological sections. J. Pediatr. Urol. 2021, 17, 439.e1–439.e12. [Google Scholar] [CrossRef] [PubMed]
- Bašković, M.; Ježek, D. Response to Letter to the Editor re ‘The effect of astaxanthin on testicular torsion-detorsion injury in rats-detailed morphometric evaluation of histological sections’. J. Pediatr. Urol. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Prillaman, H.M.; Turner, T.T. Rescue of testicular function after acute experimental torsion. J. Urol. 1997, 157, 340–345. [Google Scholar] [CrossRef]
- Conlon, K.A.; Zharkov, D.O.; Berrios, M. Immunofluorescent localization of the murine 8-oxoguanine DNA glycosylase (mOGG1) in cells growing under normal and nutrient deprivation conditions. DNA Repair. 2003, 2, 1337–1352. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, S.; Kajiya, H.; Okabe, K.; Ikebe, T. Effects of oxidative stress on the expression of 8-oxoguanine and its eliminating enzymes in human keratinocytes and squamous carcinoma cells. Oral Sci. Int. 2011, 8, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Sheng, Z.; Oka, S.; Tsuchimoto, D.; Abolhassani, N.; Nomaru, H.; Sakumi, K.; Yamada, H.; Nakabeppu, Y. 8-Oxoguanine causes neurodegeneration during MUTYH-mediated DNA base excision repair. J. Clin. Investig. 2012, 122, 4344–4361. [Google Scholar] [CrossRef] [Green Version]
- Sobočan, N.; Katušić Bojanac, A.; Sinčić, N.; Himelreich-Perić, M.; Krasić, J.; Majić, Ž.; Jurić-Lekić, G.; Šerman, L.; Vlahović, M.; Ježek, D.; et al. A Free Radical Scavenger Ameliorates Teratogenic Activity of a DNA Hypomethylating Hematological Therapeutic. Stem Cells Dev. 2019, 28, 717–733. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Jha, A.B.; Dubey, R.S.; Pessarakli, M. Reactive oxygen species, oxidative damage, and antioxidative defense mechanism in plants under stressful conditions. J. Bot. 2012, 2012, 217037. [Google Scholar] [CrossRef] [Green Version]
- Hekimoglu, A.; Kurcer, Z.; Aral, F.; Baba, F.; Sahna, E.; Atessahin, A. Lycopene, an antioxidant carotenoid, attenuates testicular injury caused by ischemia/reperfusion in rats. Tohoku J. Exp. Med. 2009, 218, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güzel, M.; Sönmez, M.F.; Baştuğ, O.; Aras, N.F.; Öztürk, A.B.; Küçükaydın, M.; Turan, C. Effectiveness of lycopene on experimental testicular torsion. J. Pediatr. Surg. 2016, 51, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.J., Jr.; Turner, T.T. Endocrine and exocrine effects of testicular torsion in the prepubertal and adult rat. J. Androl. 1995, 16, 342–351. [Google Scholar]
- Zuluaga, M.; Gueguen, V.; Letourneur, D.; Pavon-Djavid, G. Astaxanthin-antioxidant impact on excessive Reactive Oxygen Species generation induced by ischemia and reperfusion injury. Chem. Biol. Interact. 2018, 279, 145–158. [Google Scholar] [CrossRef]
- Sathasivam, R.; Ki, J.S. A Review of the Biological Activities of Microalgal Carotenoids and Their Potential Use in Healthcare and Cosmetic Industries. Mar. Drugs 2018, 16, 26. [Google Scholar] [CrossRef] [Green Version]
- Mishra, R.K.; Singh, S.; Singh, S.K. Natural products in regulation of male fertility. Indian J. Med. Res. 2018, 148, S107–S114. [Google Scholar]
- Dias, T.R.; Alves, M.G.; Oliveira, P.F.; Silva, B.M. Natural products as modulators of spermatogenesis: The search for a male contraceptive. Curr. Mol. Pharmacol. 2014, 7, 154–166. [Google Scholar] [CrossRef]
- Li, J.; Zhu, D.; Niu, J.; Shen, S.; Wang, G. An economic assessment of astaxanthin production by large scale cultivation of Haematococcus pluvialis. Biotechnol. Adv. 2011, 29, 568–574. [Google Scholar] [CrossRef]
- Sung, Y.J.; Sim, S.J. Multifaceted strategies for economic production of microalgae Haematococcus pluvialis-derived astaxanthin via direct conversion of CO2. Bioresour. Technol. 2021, 344, 126255. [Google Scholar] [CrossRef]
- Bauer, A.; Minceva, M. Techno-economic analysis of a new downstream process for the production of astaxanthin from the microalgae Haematococcus pluvialis. Bioresour. Bioprocess. 2021, 8, 111. [Google Scholar] [CrossRef]
- Otsuka, T.; Shimazawa, M.; Inoue, Y.; Nakano, Y.; Ojino, K.; Izawa, H.; Tsuruma, K.; Ishibashi, T.; Hara, H. Astaxanthin Protects Against Retinal Damage: Evidence from In Vivo and In Vitro Retinal Ischemia and Reperfusion Models. Curr. Eye Res. 2016, 41, 1465–1472. [Google Scholar] [CrossRef]
- Curek, G.D.; Cort, A.; Yucel, G.; Demir, N.; Ozturk, S.; Elpek, G.O.; Savas, B.; Aslan, M. Effect of astaxanthin on hepatocellular injury following ischemia/reperfusion. Toxicology 2010, 267, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Zuluaga Tamayo, M.; Choudat, L.; Aid-Launais, R.; Thibaudeau, O.; Louedec, L.; Letourneur, D.; Gueguen, V.; Meddahi-Pellé, A.; Couvelard, A.; Pavon-Djavid, G. Astaxanthin Complexes to Attenuate Muscle Damage after In Vivo Femoral Ischemia-Reperfusion. Mar. Drugs 2019, 17, 354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauver, D.A.; Lockwood, S.F.; Lucchesi, B.R. Disodium Disuccinate Astaxanthin (Cardax) attenuates complement activation and reduces myocardial injury following ischemia/reperfusion. J. Pharmacol. Exp. Ther. 2005, 314, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Qiu, X.; Fu, K.; Zhao, X.; Zhang, Y.; Yuan, Y.; Zhang, S.; Gu, X.; Guo, H. Protective effects of astaxanthin against ischemia/reperfusion induced renal injury in mice. J. Transl. Med. 2015, 13, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripathi, D.N.; Jena, G.B. Astaxanthin inhibits cytotoxic and genotoxic effects of cyclophosphamide in mice germ cells. Toxicology 2008, 248, 96–103. [Google Scholar] [CrossRef]
- Wang, J.Y.; Lee, Y.J.; Chou, M.C.; Chang, R.; Chiu, C.H.; Liang, Y.J.; Wu, L.S. Astaxanthin protects steroidogenesis from hydrogen peroxide-induced oxidative stress in mouse Leydig cells. Mar. Drugs 2015, 13, 1375–1388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britton, G. Structure and properties of carotenoids in relation to function. FASEB J. 1995, 9, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Brendler, T.; Williamson, E.M. Astaxanthin: How much is too much? A safety review. Phytother. Res. 2019, 33, 3090–3111. [Google Scholar] [CrossRef]
- Stewart, J.S.; Lignell, A.; Pettersson, A.; Elfving, E.; Soni, M.G. Safety assessment of astaxanthin-rich microalgae biomass: Acute and subchronic toxicity studies in rats. Food. Chem. Toxicol. 2008, 46, 3030–3036. [Google Scholar] [CrossRef] [PubMed]
- Vega, K.; Edwards, J.; Beilstein, P. Subchronic (13-week) toxicity and prenatal developmental toxicity studies of dietary astaxanthin in rats. Regul. Toxicol. Pharmacol. 2015, 73, 819–828. [Google Scholar] [CrossRef]
- Katsumata, T.; Ishibashi, T.; Kyle, D. A sub-chronic toxicity evaluation of a natural astaxanthin-rich carotenoid extract of Paracoccus carotinifaciens in rats. Toxicol. Rep. 2014, 1, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Kishimoto, Y.; Yoshida, H.; Kondo, K. Potential Anti-Atherosclerotic Properties of Astaxanthin. Mar. Drugs 2016, 14, 35. [Google Scholar] [CrossRef]
- Park, J.S.; Chyun, J.H.; Kim, Y.K.; Line, L.L.; Chew, B.P. Astaxanthin decreased oxidative stress and inflammation and enhanced immune response in humans. Nutr. Metab. 2010, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Ito, N.; Seki, S.; Ueda, F. The Protective Role of Astaxanthin for UV-Induced Skin Deterioration in Healthy People-A Randomized, Double-Blind, Placebo-Controlled Trial. Nutrients 2018, 10, 817. [Google Scholar] [CrossRef] [Green Version]
- Davinelli, S.; Scapagnini, G.; Marzatico, F.; Nobile, V.; Ferrara, N.; Corbi, G. Influence of equol and resveratrol supplementation on health-related quality of life in menopausal women: A randomized, placebo-controlled study. Maturitas 2017, 96, 77–83. [Google Scholar] [CrossRef]
- Eren, B.; Tuncay Tanrıverdi, S.; Aydın Köse, F.; Özer, Ö. Antioxidant properties evaluation of topical astaxanthin formulations as anti-aging products. J. Cosmet. Dermatol. 2019, 18, 242–250. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, J.J.; Lee, B.J.; Joo, M.K.; Chun, H.J.; Lee, S.W.; Bak, Y.T. Astaxanthin Inhibits Proliferation of Human Gastric Cancer Cell Lines by Interrupting Cell Cycle Progression. Gut Liver 2016, 10, 369–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilinska, M.A.; Kurinnyi, D.A.; Rushkovsky, S.R.; Dybska, O.B. Genoprotective properties of astaxanthin revealed by ionizing radiation exposure in vitro on human peripheral blood lymphocytes. Probl. Radiac. Med. Radiobiol. 2016, 21, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Comhaire, F.H.; El Garem, Y.; Mahmoud, A.; Eertmans, F.; Schoonjans, F. Combined conventional/antioxidant “Astaxanthin” treatment for male infertility: A double blind, randomized trial. Asian J. Androl. 2005, 7, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Reboul, E. Mechanisms of Carotenoid Intestinal Absorption: Where Do We Stand? Nutrients 2019, 11, 838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, R.S. Absorption, metabolism, and transport of carotenoids. FASEB J. 1996, 10, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Mel’man, E.P.; Gritsulyak, B.V.; Shutka, B.V. Changes in the ultrastructure of components of the blood-testis barrier in circulatory hypoxia. Bull. Exp. Biol. Med. 1979, 88, 928–931. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bašković, M.; Krsnik, D.; Himelreich Perić, M.; Katušić Bojanac, A.; Sinčić, N.; Sonicki, Z.; Ježek, D. Astaxanthin Relieves Testicular Ischemia-Reperfusion Injury—Immunohistochemical and Biochemical Analyses. J. Clin. Med. 2022, 11, 1284. https://doi.org/10.3390/jcm11051284
Bašković M, Krsnik D, Himelreich Perić M, Katušić Bojanac A, Sinčić N, Sonicki Z, Ježek D. Astaxanthin Relieves Testicular Ischemia-Reperfusion Injury—Immunohistochemical and Biochemical Analyses. Journal of Clinical Medicine. 2022; 11(5):1284. https://doi.org/10.3390/jcm11051284
Chicago/Turabian StyleBašković, Marko, Dajana Krsnik, Marta Himelreich Perić, Ana Katušić Bojanac, Nino Sinčić, Zdenko Sonicki, and Davor Ježek. 2022. "Astaxanthin Relieves Testicular Ischemia-Reperfusion Injury—Immunohistochemical and Biochemical Analyses" Journal of Clinical Medicine 11, no. 5: 1284. https://doi.org/10.3390/jcm11051284
APA StyleBašković, M., Krsnik, D., Himelreich Perić, M., Katušić Bojanac, A., Sinčić, N., Sonicki, Z., & Ježek, D. (2022). Astaxanthin Relieves Testicular Ischemia-Reperfusion Injury—Immunohistochemical and Biochemical Analyses. Journal of Clinical Medicine, 11(5), 1284. https://doi.org/10.3390/jcm11051284