
Efficacy of Laryngeal Rehabilitation Therapy on Dysphagia after Anterior Cervical Surgery: Prospective, Randomized Control Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
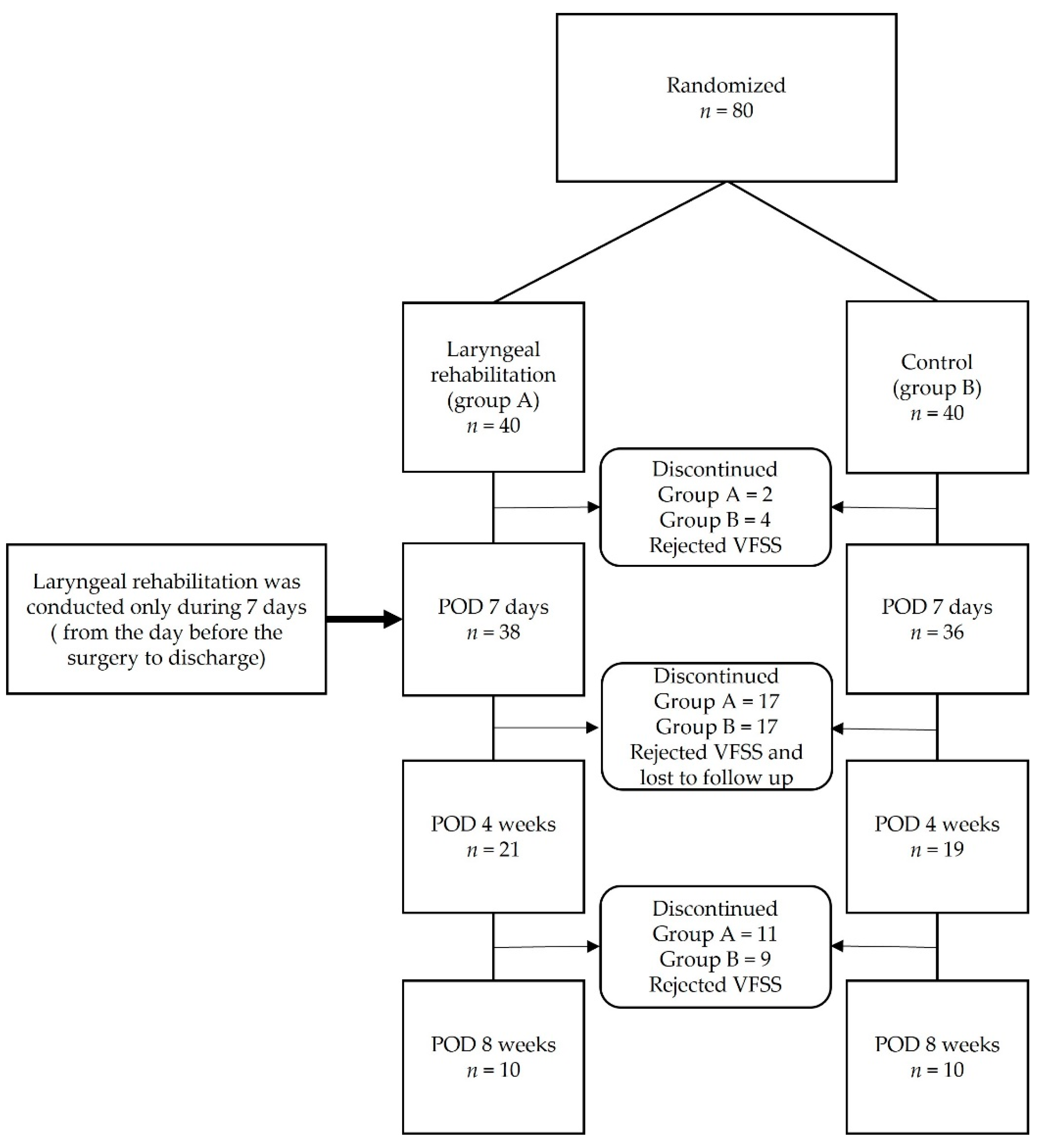
2.1.1. Trial Design
2.1.2. Participants
2.1.3. Interventions
2.1.4. Randomization
Sequence Generation and Allocation Concealment
Implementation
2.2. Materials and Methods
2.2.1. Laryngeal Rehabilitation Therapy
2.2.2. VFSS (Videofluoroscopic Swallowing Study)
2.2.3. Clinical and Radiologic Outcomes
2.2.4. Statistical Analysis
3. Results
3.1. VFSS
3.2. Clinical and Radiologic Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daniels, A.H.; Riew, D.K.; Yoo, J.U.; Ching, A.; Birchard, K.R.; Kranenburg, A.J.; Hart, R.A. Adverse events associated with anterior cervical spine surgery. J. Am. Acad. Orthop. Surg. 2008, 16, 729–738. [Google Scholar] [CrossRef] [Green Version]
- Bazaz, R.; Lee, M.J.; You, J.U. Incidence of dysphagia after anterior cervical spine surgery: A prospective study. Spine 2002, 27, 2453–2458. [Google Scholar] [CrossRef]
- Siska, P.A.; Ponnappan, R.K.; Hohl, J.B.; Lee, J.Y.; Kang, J.D.; Donaldson, W.F., III. Dysphagia after anterior cervical spine surgery: A prospective study using the swallowing-quality of life questionnaire and analysis of patient comorbidities. Spine 2011, 36, 1387–1391. [Google Scholar] [CrossRef]
- Riley, L.H., III; Skolasky, R.L.; Albert, T.J.; Vaccaro, A.R.; Heller, J.G. Dysphagia after anterior cervical decompression and fusion: Prevalence and risk factors from a longitudinal cohort study. Spine 2005, 30, 2564–2569. [Google Scholar] [CrossRef]
- Lee, M.J.; Bazaz, R.; Furey, C.G.; Yoo, J. Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J. 2007, 7, 141–147. [Google Scholar] [CrossRef]
- Papavero, L.; Heese, O.; Klotz-Regener, V.; Buchalla, R.; Schröder, F.; Westphal, M. The impact of esophagus retraction on early dysphagia after anterior cervical surgery: Does a correlation exist? Spine 2007, 32, 1089–1093. [Google Scholar] [CrossRef]
- Chin, K.R.; Eiszner, J.R.; Adams, S.B., Jr. Role of plate thickness as a cause of dysphagia after anterior cervical fusion. Spine 2007, 32, 2585–2590. [Google Scholar] [CrossRef]
- Lee, S.H.; Kim, K.T.; Suk, K.S.; Park, K.J.; Oh, K.I. Effect of retropharyngeal steroid on prevertebral soft tissue swelling following anterior cervical discectomy and fusion: A prospective, randomized study. Spine 2011, 36, 2286–2292. [Google Scholar] [CrossRef]
- Song, K.J.; Lee, S.K.; Ko, J.H.; Yoo, M.J.; Kim, D.Y.; Lee, K.B. The clinical efficacy of short-term steroid treatment in multilevel anterior cervical arthrodesis. Spine J. 2014, 14, 2954–2958. [Google Scholar] [CrossRef]
- Ratnaraj, J.; Todorov, A.; McHugh, T.; Cheng, M.A.; Lauryssen, C. Effects of decreasing endotracheal tube cuff pressures during neck retraction for anterior cervical spine surgery. J. Neurosurg. 2002, 97, 176–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Wei, X.; Li, F.; He, P.; Huang, X.; Zhang, F.; Qi, K.; Liu, X.; Shen, H.; Hou, T.; et al. Tracheal traction exercise reduces the occurrence of postoperative dysphagia after anterior cervical spine surgery. Spine 2012, 37, 1292–1296. [Google Scholar] [CrossRef]
- Leonard, R.; Belafsky, P. Dysphagia following cervical spine surgery with anterior instrumentation: Evidence from fluoroscopic swallow studies. Spine 2011, 36, 2217–2223. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Larsen, K. Oropharyngeal dysphagia: Pathophysiology and diagnosis for the anniversary issue of Diseases of the Esophagus. Dis. Esophagus 2012, 25, 299–304. [Google Scholar] [CrossRef]
- Smith-Hammond, C.A.; New, K.C.; Pietrobon, R.; Curtis, D.J.; Scharver, C.H.; Turner, D.A. Prospective analysis of incidence and risk factors of dysphagia in spine surgery patients: Comparison of anterior cervical, posterior cervical, and lumbar procedure. Spine 2004, 29, 1441–1446. [Google Scholar] [CrossRef]
- Chaudhary, S.K.; Yu, B.; Pan, F.; Li, X.; Wang, S.; Shaikh, I.I.; Wu, D. Manual preoperative tracheal retraction exercise decreases the occurrence of postoperative oropharyngeal dysphagia after anterior cervical discectomy and fusion. J. Orthop. Surg. 2017, 25, 2309499017731446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, C.C.; Karpitskaya, Y.; Cha, C.; Heller, J.G.; Lauryssen, C.; Yoon, S.T.; Riew, K.D. Accurate identification of adverse outcomes after cervical spine surgery. J. Bone Jt. Surg. Am. 2004, 86, 251–256. [Google Scholar] [CrossRef] [Green Version]
- Segebarth, B.; Datta, J.C.; Darden, B.; Janssen, M.E.; Murrey, D.B.; Rhyne, A.; Beckham, R.; Ponce, C. Incidence of dysphagia comparing cervical arthroplasty and ACDF. SAS J. 2010, 4, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Jean, A. Brain stem control of swallowing: Neuronal network and cellular mechanisms. Physiol. Rev. 2001, 81, 929–969. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, K.; Palmer, J.B. Anatomy and physiology of feeding and swallowing: Normal and abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707. [Google Scholar] [CrossRef] [Green Version]
- American Speech-Language-Hearing Association. Swallowing Disorders (Dysphagia) in Adult; American Speech-Language-Hearing Association: Rockville, MD, USA, 2013. [Google Scholar]
- American College of Radiology. ACR Appropriateness Criteria®: Dysphagia; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Debara, L.T. National Institute on Deafness and Other Communication Disorders (National Institutes of Health). Dysphagia; NIH Publication: Bethesda, MD, USA, 2013; No. 10-4307. [Google Scholar]
- Troche, M.S.; Brandimore, A.E.; Foote, K.D.; Okun, M.S. Swallowing and deep brain stimulation in Parkinson’s disease: A systemic review. Parkinsonism Relat. Disord. 2013, 19, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Emery, S.E.; Akhavan, S.; Miller, P.; Furey, C.G.; Yoo, J.U.; Rowbottom, J.R.; Bohlman, H.H. Steroids and risk factors for airway compromise in multilevel corpectomy patients. Spine 2009, 34, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Skeppholm, M.; Ingebro, C.; Engström, T.; Olerud, C. The Dysphagia Short Questionaire: An instrument for evaluation of dysphagia: A validation study with 12 months’ follow-up after anterior cervical spine surgery. Spine 2012, 37, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Kalb, S.; Reis, M.T.; Cowperthwaite, M.C.; Fox, D.J.; Lefevre, R.; Theodore, N.; Papadopoulos, S.M.; Sonntag, V.K. Dysphagia after anterior cervical spine surgery: Incidence and risk factors. World Neurosurg. 2012, 77, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Cook, I.J.; Kahrilas, P.J. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology 1999, 116, 445–478. [Google Scholar] [CrossRef]
- McAfee, P.C.; Cappuccino, A.; Cunningham, B.W.; Devine, J.G.; Phillips, F.M.; Regan, J.J.; Albert, T.J.; Ahrens, J.E. Lower incidence of dysphagia with cervical arthroplasty compared with ACDF in a prospective randomized clinical trial. J. Spinal Disord. Tech. 2010, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.K.; Arnold, P.M. Oropharyngeal Dysphagia after anterior cervical spine surgery: A review. Glob. Spine J. 2013, 3, 273–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protocol | Description |
|---|---|
| Hospitalization Period | 9 Days |
| Admission day | the day before the surgery |
| Discharge day | Postoperative day (POD) 7 days |
| High dose IV steroid administration 250 mg methylprednisolone | Every 6 h for 2 days (operation day and POD 1 day) to reduce the prevertebral soft tissue swelling for preventing airway complication or severe dysphagia |
| Closed suction drainage | Removal if the amount < 30 cc/day Usually 1~3 days after the surgery |
| Postoperative orthosis | Modified Philadelphia neck brace (Vista® Collar, Aspen, CO, USA) for POD 6 weeks |
| Follow-up protocol | Lateral X-ray: everyday check during hospitalization period |
| AP and lateral X-ray: discharge day and regular follow-up day | |
| Regular follow-up: POD 4 weeks, POD 8 weeks, POD 12 weeks, POD 6 months, POD 12 months, and annual follow-up |
| Severity | Liquid | Solid |
|---|---|---|
| None | None | None |
| Mild | None | Rare |
| Moderate | None/rare | Occasionally |
| Severe | None/rare | Frequent |
| Variables | Rehabilitation Group (n = 10) | Control Group (n = 10) | p-Value |
|---|---|---|---|
| Age (mean ± SD), year | 55.9 ± 9.6 | 54.6 ± 9.5 | 0.764 * |
| Sex (M:F) | 6:4 | 4:6 | 0.660 † |
| History of smoking | 3 (30%) | 3 (30 %) | 1.000 † |
| Operative time (mean ± SD), min | 100.8 ± 20.1 | 98.6 ± 22 | 0.818 * |
| Levels of fusion | 2 level = 2 3 level = 6 4 level = 2 | 2 level = 3 3 level = 4 4 level = 3 | N/A |
| Rehabilitation Group (n = 10) | Control Group (n = 10) | p-Value | |
|---|---|---|---|
| Preoperative (mean ± SD), s | 0.90 ± 0.05 | 0.90 ± 0.07 | 0.849 † |
| Postoperative, 7th day | 1.34 ± 0.15 | 1.59 ± 0.18 | 0.004 * |
| 4th week | 1.08 ± 0.08 | 1.15 ± 0.06 | 0.028 * |
| 8th week | 0.91 ± 0.06 | 0.95 ± 0.04 | 0.112 * |
| Rehabilitation Group (n = 10) | Control Group (n = 10) | p-Value * | |
|---|---|---|---|
| POD 1D (mean ± SD), mm | 88.6 ± 17.1 | 84.7 ± 18.2 | 0.591 |
| POD 2D | 92.2 ± 14.6 | 82.2 ± 19.2 | 0.200 |
| POD 3D | 90.4 ± 12.7 | 79.4 ± 21.8 | 0.184 |
| POD 4D | 88.7 ± 18.9 | 76.5 ± 14.6 | 0.128 |
| POD 5D | 83.6 ± 15.9 | 78.2 ± 14.3 | 0.431 |
| POD 6D | 80.8 ± 16.8 | 76.8 ± 17.0 | 0.600 |
| POD 7D | 74.3 ± 17.0 | 73.5 ± 19.0 | 0.920 |
| POD 4W | 54.8 ± 11.9 | 53.3 ± 12.6 | 0.780 |
| POD 8W | 50.4 ± 11.2 | 51.6 ± 10.8 | 0.800 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, J.-H.; Han, K.-S.; Yoon, S.-J. Efficacy of Laryngeal Rehabilitation Therapy on Dysphagia after Anterior Cervical Surgery: Prospective, Randomized Control Trial. J. Clin. Med. 2022, 11, 2470. https://doi.org/10.3390/jcm11092470
Ko J-H, Han K-S, Yoon S-J. Efficacy of Laryngeal Rehabilitation Therapy on Dysphagia after Anterior Cervical Surgery: Prospective, Randomized Control Trial. Journal of Clinical Medicine. 2022; 11(9):2470. https://doi.org/10.3390/jcm11092470
Chicago/Turabian StyleKo, Jong-Hyun, Kap-Soo Han, and Sun-Jung Yoon. 2022. "Efficacy of Laryngeal Rehabilitation Therapy on Dysphagia after Anterior Cervical Surgery: Prospective, Randomized Control Trial" Journal of Clinical Medicine 11, no. 9: 2470. https://doi.org/10.3390/jcm11092470