Abstract
(1) Background: The use of antiangiogenic TKIs (AA-TKIs) has recently emerged as a major paradigm shift in the treatment of advanced sarcoma. However, the feasibility of drug holidays for patients demonstrating a very favorable response remains unknown. (2) Methods: We aim to explore the outcomes of patients with advanced sarcoma who discontinued AA-TKIs after a (near-) complete remission or were long-term responders. Patients with advanced disease were included if they had bilateral or multiple lung metastases, extrapulmonary recurrence, a short disease-free interval, etc., at the initiation of AA-TKIs. (3) Results: A total of 22 patients with AA-TKI discontinuation were analyzed, with a median follow-up of 22.3 months post-discontinuation. Prior to discontinuation, there were four drug-induced complete remissions (CRs), twelve surgical CRs, and six long-term responders. Disease progression was observed in 17/22 (77.3%) patients, with a median of 4.2 months. However, since the majority were still sensitive to the original AA-TKIs and amenable to a second surgical remission, 7 out of these 17 patients achieved a second CR after disease progression and were thus considered as relapse-free post-discontinuation (pd-RFS). Therefore, the pd-RFS and post-discontinuation overall survival (pd-OS) in the last follow-up were 12/22 (54.5%) and 16/22 (72.7%), respectively. Remarkably, surgical CR and drug tapering off (versus abrupt stopping) were associated with a greater pd-RFS and pd-OS (p < 0.05). Furthermore, higher necrosis rates (p = 0.040) and lower neutrophil-to-lymphocyte ratios (NLR) (p = 0.060) before discontinuation tend to have a better pd-RFS. (4) Conclusions: Our results suggest that AA-TKI discontinuation with a taper-off strategy might be safe and feasible in highly selected patients with advanced sarcoma. Surgical CR, NLR, and tumor necrosis rates before discontinuation were potential biomarkers for AA-TKI withdrawal.
1. Introduction
The use of tyrosine kinase inhibitors (TKIs) targeting tumor angiogenesis has emerged as a major paradigm shift in the treatment of recurrent or advanced sarcoma in recent years [1,2]. According to previous clinical trials, bone sarcoma demonstrated an objective response rate (ORR) of 8–22% to novel antiangiogenic TKIs (AA-TKIs), such as regorafenib [2], cabozantinib [3], and apatinib [4], while soft tissue sarcoma demonstrated an ORR of 5–13% to regorafenib [5], pazopanib [6], and anlotinib [7]. Moreover, antiangiogenics in combination with chemotherapy might further increase such anti-tumor activity, with an ORR of 24–29% in advanced sarcoma [8,9]. For long-lasting responders to these TKIs, it is common for the patients to interrupt the TKIs due to toxicity, noncompliance, or considering their disease fully controlled. However, to our knowledge, the feasibility of discontinuing TKIs in sarcoma responders has only been explored in gastrointestinal stromal tumor (GIST) patients with imatinib treatment [10,11]. Whether a drug holiday from AA-TKIs could be considered in sarcoma patients still remains unknown. Therefore, in this report, we aim to explore the safety and outcome of a drug holiday or discontinuation of AA-TKIs in patients with advanced sarcoma who demonstrate a (near-)complete remission or are long-term responders (duration of response of >6 months) [12,13] to the therapy.
2. Materials and Methods
The medical records of advanced bone and soft tissue sarcoma patients treated with AA-TKIs in our institution from 1 March 2017 to 30 December 2020 were reviewed. Only patients who were unlikely to be cured at the initiation of AA-TKIs were included. The definition of “unlikely-to-be-cured” was based on the previous literature (the era before the use of AA-TKIs) demonstrating that less than 5~10% patients could be long-term tumor-free, even after metastasectomy, if exhibiting the following risk factors: (a) bilateral pulmonary recurrence [14]; (b) pulmonary metastasis with local recurrence [15] or extrapulmonary lesions [16]; (c) a disease-free interval (DFI) of shorter than 18 months [14]; (d) the tumor was inoperable or incompletely resected (cytoreductive resection) [17]; and (e) multiple lesions (>5 metastases) [17,18]. Patients with one or more of the aforementioned risk factors were evaluated for their tumor status at the time of drug discontinuation. We only included cases of advanced sarcoma which demonstrated a favorable response, defined as (near-)complete remission (either by drug induction or surgical removal) or long-term responders (with a duration of response of >6 months [12]), according to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 [19]. A temporary interruption and re-introduction of the drugs due to adverse effects or surgical procedures was not considered as drug discontinuation in our study.
Twenty-two patients with a favorable response were included in the analysis. All patients were informed about the potential outcome before the attempt to discontinue the AA-TKIs by the attending physicians, who balanced the risk of tumor progression and the patients’ demands or preferences for a drug holiday. In our study, discontinuation of AA-TKIs in this group of patients was mostly discouraged but considered relatively acceptable only in patients who completed at least 12 months of regimens with no evidence of disease (tumor-free) and had agreed to be compliant with close surveillance post-discontinuation, as well as if the patients had a strong demand for a drug holiday for any reasons (“planned”). Otherwise, it was defined as “unplanned” discontinuation if the patients insisted on discontinuing the drug against the physicians’ recommendation or without informing physicians despite a substantial risk of tumor relapse. Due to the fact that rapid tumor rebound is frequently observed following the abrupt discontinuation of AA-TKIs, we recommended a “taper-off” strategy to all patients, which included one dose level reduction for ~two cycles and a second dose level reduction for ~two cycles prior to permanent discontinuation. Tumor responses was assessed every 2–3 months of treatment, based on imaging with CT or magnetic resonance imaging (MRI) scans according to the RECIST 1.1 criteria [19], and were defined as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). In pulmonary lesions with substantial cavitation, we adopted a modified RECIST in which the longest diameter of cavitation was subtracted from the longest total diameter of the lesion in the same plane according to Crabb et al. [20]. Furthermore, on-treatment biopsy was available for 13 out of 22 patients and was analyzed for the tumor necrosis rate. Patients were also stratified based on whether their neutrophil-to-lymphocyte ratio (NLR) was ≥2.5 and platelet-to-lymphocyte ratio (PLR) ≥150 at the time of discontinuation [21,22].
The outcome after drug discontinuation was assessed with the following endpoints: (a) Progression-free survival post-discontinuation (pd-PFS), defined as the time between TKI discontinuation and the date of first noticeable disease recurrence, progression, or death, whichever occurred first. (b) Overall survival post discontinuation (pd-OS), defined as the time between TKI discontinuation and the date of death from any cause. Since some patients achieved a second CR upon re-challenging TKI and/or another surgical removal of the recurrence, we also measured the (c), relapse-free survival post discontinuation (pd-RFS), which was the same as pd-PFS except in cases where patients achieved a second CR of all known recurrence (i.e., tumor-free) after progression, and thus were still considered relapse-free until the recurrence re-relapsed into an irremovable state. The aggressiveness of tumor recurrence post-discontinuation was quantified using tumor doubling time (TDT) with the method proposed by Schwartz [23]. The objective response rate (ORR, CR + PR) and disease control rate (DCR, CR + PR + SD) were used to evaluate the sensitivity of a recurrence upon re-administration of AA-TKIs [24,25].
3. Results
3.1. Clinicopathological Data of the Patients
Out of 182 patients receiving AA-TKIs with advanced bone and soft tissue sarcoma, 22 patients were included according to our criteria (Figure 1). The AA-TKIs included apatinib (n = 14), anlotinib (n = 6), and pazopanib (n = 2). There were 10 males and 12 females, with a median age of 22.5 years (IQR, 16.3–26.5). Ten of them were diagnosed with osteosarcoma (OS), and eleven were diagnosed with other sarcomas. As of the data cutoff (1 May 2022), the median follow-up was 36.9 (IQR, 30.8–46.4) months in total and 22.3 (IQR, 16.6–28.4) months post-discontinuation. The median time off TKIs in all the patients was 15.3 months (IQR, 8.2–20.5). A total of 14 patients had an unplanned discontinuation due to the patients’ preference (n = 3), toxicity (n = 10), or comorbidity (n = 1). The dose reduction strategy involved abrupt discontinuation (n = 11) and tapering off (n = 11). At the time of drug discontinuation, there were 12 surgical CRs, 4 drug-induced CRs, and 6 long-term responders (Table 1). The median tumor necrosis rate was 46.67% (IQR, 25.00–90.00) in 13 of 22 cases where on-treatment biopsy was available. In patients who were long-term responders, the median duration of tumor response was 16.5 months (IQR, 13.6–21.2). No significant differences in age (p = 0.926), sex (p = 0.662), tumor quantity (p = 0.479), tumor burden (p = 0.513), or DFI (p = 0.694) were observed among these three groups of patients.
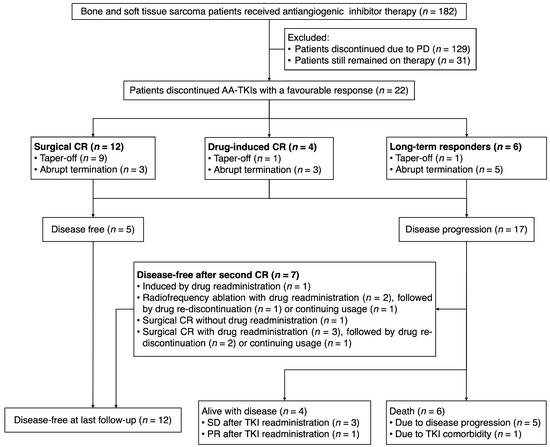
Figure 1.
Consort flow diagram of our study. Long-term responders were defined as having a duration of response of > 6 months. PD = disease progression. CR = complete response. PR = partial response. SD = stable disease.

Table 1.
Clinical characteristics of 22 patients before the AA-TKI discontinuation.
3.2. Oncological Outcomes of AA-TKI Discontinuation
The characteristics and outcomes of 22 patients following AA-TKI discontinuation are shown in Table 2 and Figure 2A. Disease progression following discontinuation was observed in 17 out of 22 patients (77.3%), including 2 cases with new metastatic sites. The median pd-PFS was 6.5 months (IQR, 2.8–13.3) in the entire cohort. A total of 5 patients were progression-free until the last follow-up, with a median time of 28.8 months post-discontinuation. In patients with disease progression following discontinuation, the median time to recurrence or progression after discontinuation was 4.2 months (IQR, 2.7–9.3). The median TDT was 53.8 days (IQR, 44.0–76.4). Since a significant proportion of recurrent tumors were still sensitive to the original AA-TKI therapy or amenable to surgical remission (including metastasectomy and radiofrequency ablation), 7 out of 17 patients achieved a second CR after disease progression and, thus, were still considered as having no evidence of disease until the last follow-up (defined as relapse-free in our study). Therefore, a total of 12 patients (54.5%) were relapse-free until the last follow-up, with a median follow-up of 25.1 months (IQR, 20.1–31.6) (Figure 2B). Therefore, the rate of pd-RFS and pd-OS was 63.6% (95% CI 46.4–87.3) and 81.8% (95% CI 67.2–99.6) at 6 months, and 63.6% (95% CI 46.4–87.3) and 77.3% (95% CI 61.6–96.9) at 12 months, respectively, in the total cohort. The median TDT of the 22 patients before taking AA-TKIs was 26.5 days (IQR, 18.8–58.1). In contrast, TDT appeared to be prolonged (53.8 days, IQR 44.0–76.4) in 17 patients with disease progression after discontinuation (p = 0.002).
Table 2.
Clinical and oncological data for the 22 patients’ outcomes following AA-TKI discontinuation.
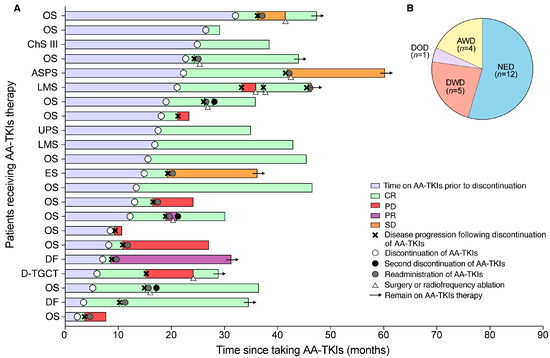
Figure 2.
Clinical outcomes following discontinuation of TKIs. (A) Each bar represents one patient in this study (n = 22) and sarcoma subtypes are shown on Y-axis labels. Black crosses are the time-point at which radiographic disease progression occurred that was used in the analysis. Twelve patients re-administered TKI therapy after discontinuation due to disease progression. Green bars show no radiographic confirmation of tumor lesions. ASPS = alveolar soft-part sarcoma. OS = osteosarcoma. ChS III = chondrosarcoma grade III. LMS = leiomyosarcomas. UPS = undifferentiated pleomorphic sarcoma. ES = Ewing sarcoma. DF = desmoid fibromatosis. D-TGCT = diffuse-type tenosynovial giant cell tumor. CR = complete response. PD = disease progression. PR = partial response. SD = stable disease. (B) Pie chart shows the 22 patients’ outcomes. NED = no evidence of disease; AWD = alive with disease; DWD = died with disease; DOD = died of other disease.
In patients with disease progression following drug discontinuation, drug re-administration was taken in 14 cases, of which 4 were resistant to AA-TKIs while 10 had the disease controlled, including 6 CR, 1 PR, and 3 SD. Upon re-challenge of the original therapy, the ORR was similar to the original response (50.0% versus 72.7%, p = 0.29) while the DCR was significantly lower than the original therapeutic response (71.4% versus 100.0%, p = 0.017). In the last follow-up, six patients deceased, mostly due to oncological reasons, except one patient who died of infectious disease (pneumonitis and empyema).
3.3. Risk Factors Associated with the Outcomes Following Drug Discontinuation
We next sought to determine whether clinicopathological variables were associated with the prognoses after TKI discontinuation. In the univariate analysis, there was no significant association of pd-RFS or pd-OS with age, sex, time on TKI, concurrent radiotherapy, concurrent chemotherapy, body mass index (BMI), pathological diagnosis, DFI, tumor burden, or TKI re-administration (Table 3). Remarkably, the initial change rate of a tumor response (p = 0.721) had no significant association with the outcome after drug discontinuation (Figure 3). However, we found that drug withdrawal by tapering off, surgical removal of all lesions before discontinuation, and planned discontinuation were associated with improved pd-RFS and pd-OS (Table 3 and Figure 4). Furthermore, a higher tumor necrosis rate was associated with a better pd-RFS (p = 0.040) but not pd-OS (p = 0.280) (Table 3 and Supplementary Figure S1). Interestingly, an NLR greater than 2.5 before discontinuation (p = 0.060, borderline significance) was also correlated with a worse pd-RFS in patients with AA-TKI withdrawal.
Table 3.
Kaplan–Meier Analysis of the independent prognostic factors for pd-RFS and pd-OS among the patients.
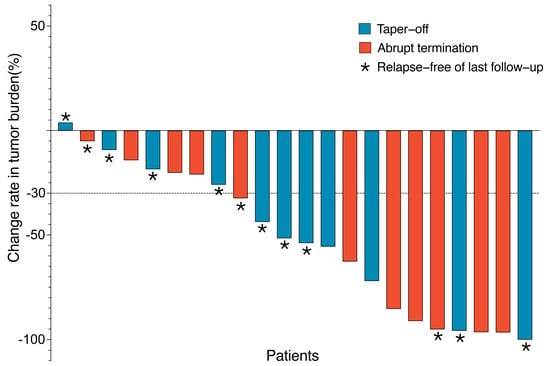
Figure 3.
Change rate from baseline of the total tumor burden. Each bar represents one patient (n = 22). * These patients were disease-free in last follow-up by surgery or radiofrequency ablation. Red bars represent patients who discontinued TKI by tapering off, and the blue represents those with abrupt termination. Dashed lines indicate RECIST criteria for progressive disease (+20%) or partial response (−30%).
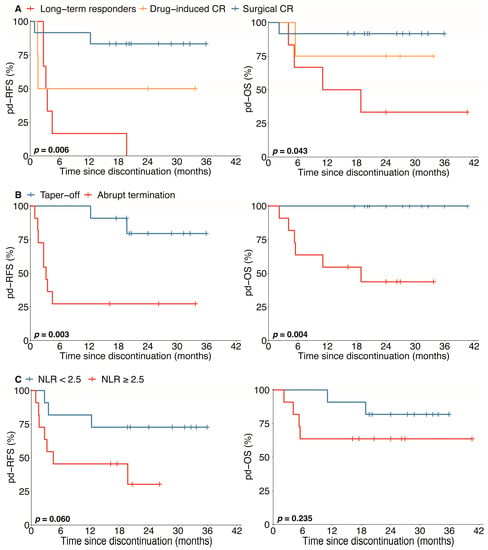
Figure 4.
Kaplan–Meier curves for pd-RFS and pd-OS. Pd-RFS = disease-free survival since the discontinuation of TKI, Pd-OS = overall survival since the discontinuation of TKI, NLR = neutrophil-to-lymphocyte ratio, and CR = complete response. Kaplan–Meier analysis estimates show the distribution of RFS and OS for all patients with TKI discontinuation analysis (n = 22). Crosses indicate censored patients. Surgical CR before discontinuation (A) was independently associated with improved survival (p = 0.006 for pd-RFS and p = 0.043 for pd-OS). Discontinuation by tapering off (B) significantly improved the RFS and OS of patients with TKI therapy (p = 0.003 for pd-RFS and p = 0.004 for pd-OS). A lower NLR (C) might be a prognostic marker in pd-RFS (p = 0.060, borderline significance), while it showed no sensitivity in pd-OS (p = 0.235).
3.4. The Potential Benefit of Drug Taper-Off Strategy
Since AA-TKI withdrawal with a taper-off strategy is associated with a better prognosis compared with abrupt discontinuation, we next address the hypothesis that it is due to prolonged disease quiescence and/or slower tumor growth following relapse. Interestingly, the disease progression risk was significantly higher in abrupt discontinuation patients compared to taper-off patients (p = 0.008) (Supplementary Figure S2A). Furthermore, we found that the growth rate of the relapsed disease tends to be slower than that of the baseline before initiating AA-TKIs (median TDT 58.08 versus 32.23 days, borderline significance, p = 0.054) in taper-off patients (Supplementary Figure S2B). In contrast, no significant difference was found in the TDT between a baseline and relapsed tumor (p = 0.230) in patients with abrupt discontinuation (Supplementary Figure S2C). As we expected, the percentage of patients receiving a second CR (surgery or radiofrequency ablation) was also significantly higher in the taper-off compared with the abrupt withdrawal strategy (71.4% versus 20.0%, borderline significance, p = 0.058) (Supplementary Figure S2D). Therefore, we proposed that the taper-off strategy might be beneficial in terms of lowering the likelihood (quiescence) and growth rate of tumor relapse, with a higher resectability of the relapse after drug discontinuation Section 3.1.
4. Discussion
To our knowledge, our report might be the first to investigate the outcome of AA-TKI discontinuation in advanced sarcoma following a favorable tumor response. Conventionally, patients with advanced bone and soft tissue sarcoma are given a dismal prognosis because of the limited options of further-line chemotherapy. However, the use of AA-TKIs has become a major treatment modality in relapsed and chemorefractory sarcoma in recent years. While AA-TKI monotherapy demonstrated a favorable tumor response in some patients (5–22% ORR), such a ratio is likely to increase with the combination therapy of AA-TKIs with chemotherapy [8], and immunotherapy [26,27], and other modalities [28] are currently being explored. Practically, the AA-TKI regimens continued indefinitely or until progressive disease was advocated in the majority of patients with advanced sarcoma. However, it is unsurprising that patients with drastic or long-term tumor responses might seek a “drug holiday” due to surgical remission after tumor downstaging, chronic toxicity limiting daily living, or economic considerations. The outcome of discontinuing AA-TKIs in these patients remains yet to be explored.
We, for the first time, demonstrated that discontinuation of AA-TKIs with active surveillance was safe and feasible in highly selected individuals. Specifically, patients who achieve tumor downstaging with surgical CR after AA-TKIs, and, less preferably, patients with a drug-induced CR are the reasonable candidates for drug discontinuation after a favorable tumor response. The association of planned discontinuation with better prognosis could also be attributable to surgical remission since seven of the eight planned discontinuation patients underwent surgical CR. Conversely, patients with identifiable residual disease were associated with early relapse and poor survival despite long-term control of the disease, thus being strongly discouraged from a drug holiday. Remarkably, most of the advanced sarcoma involved in our study could be considered “unlikely to be cured” even if mastectomy were performed and benefited less from surgical treatment alone. Therefore, the optimal duration of TKI maintenance (12 months in our cohort) before discontinuation in these patients remains unknown. The fact that nearly 80% of the patients experienced tumor progression after a median of 4.2 months post-discontinuation further supports the existence of residual tumors in most of these cases, albeit invisible by standard radiological criteria. This finding is consistent with the result of non-progressing GIST, where even targeting known oncogenic mutations of KIT failed to eradicate all the residual disease and drug interruption led to early tumor progression in advanced and adjuvant setting [29,30]. However, unlike the common involvement of visceral organs in GIST, more than half of the patients (12 out of 22) were still tumor-free in the last follow-up due to the possibility of a second CR (n = 7), which likely contributed to the favorable overall survival of the patients in our cohort.
Remarkably, our study proposed the use of tapering off over abrupt withdrawal as a potential strategy for drug discontinuation in advanced sarcoma. Interestingly, we found that the taper-off approach is potentially associated with a prolonged control of invisible residual disease (tumor quiescence) before tumor progression as well as a reduced kinetics (longer TDT) after tumor progression. The later and slower recurrence of the disease might be advantageous for patients to recover TKI usage and seek a second surgical resection, as indicated by the higher percentage of resectability in patients with the taper-off strategy than those with abrupt discontinuation in our cohort (Supplementary Figure S2C). Notably, we failed to demonstrate the role of a longer initial duration of AA-TKI treatment in inducing disease quiescence, as patients with >12 months on TKIs are not associated with a better prognosis following drug discontinuation. However, such results should be interpreted with caution since the choice of cutoff might be strongly biased by the fact that most patients were advised to stop AA-TKIs after at least 12 months in our hands. Therefore, the optimal duration of AA-TKIs before drug discontinuation warrants further investigation.
There are several limitations to our study. First, due to the rarity of (near-) CR of sarcoma due to AA-TKIs, our cohort lacks an appropriate control, where no drug holiday is given to patients with a favorable response, for comparing the oncological outcome following drug discontinuation. Additionally, patient selection bias with the limited sample size could not be excluded, given the retrospective nature of our study. However, our results provide the first proof of the concept that, unlike GIST, drug discontinuation might be feasible in highly selected patients with advanced sarcoma with favorable responses. Drug tapering off, close surveillance, and the multi-disciplinary remission of early recurrence appear to be potential strategies for patients seeking AA-TKI withdrawal.
5. Conclusions
Our results suggest that patients with surgical CR after TKI therapy, with high tumor necrosis rates and low NLRs before discontinuation were reasonable candidates for a drug holiday, and the taper-off strategy is a potentially safe and recommended way for AA-TKI discontinuation.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm12010325/s1, Figure S1: The association of tumor necrosis rate with relapse-free survival; Figure S2: The potential benefits of taper-off strategy.
Author Contributions
Conceptualization, Z.Z. and Q.B.; data curation, Z.Z. and Q.B.; writing—original draft preparation, Z.Z.; writing—review and editing, Q.B.; visualization, Z.Z.; software, Y.F., J.W., M.L., Z.L., G.H. and B.W.; supervision, Y.S. and W.Z.; funding acquisition, Q.B. and W.Z.; Z.Z. and Q.B. contributed equally to this work and share the role of the primary author. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Facility for Translational Medicine (Shanghai), grant numbers TMSK-2021-145; National Natural Science Foundation of China (NSFC), grant number 82141116; the Shanghai Municipal Health Commission, grant number 202140124 and the China Anti-Cancer Association, grant number 2021001023.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We gratefully acknowledge all authors for their contributions to the statistical analysis, writing assistance, the collection of data, etc. We also thank the patients and their families for their trust in us.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Folkman, J. Antiangiogenesis in Cancer Therapy—Endostatin and Its Mechanisms of Action. Exp. Cell Res. 2006, 312, 594–607. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.E.; Bolejack, V.; Ryan, C.W.; Ganjoo, K.N.; Loggers, E.T.; Chawla, S.; Agulnik, M.; Livingston, M.B.; Reed, D.; Keedy, V.; et al. Randomized Double-Blind Phase II Study of Regorafenib in Patients with Metastatic Osteosarcoma. J. Clin. Oncol. 2019, 37, 1424–1431. [Google Scholar] [CrossRef] [PubMed]
- Italiano, A.; Mir, O.; Mathoulin-Pelissier, S.; Penel, N.; Piperno-Neumann, S.; Bompas, E.; Chevreau, C.; Duffaud, F.; Entz-Werlé, N.; Saada, E.; et al. Cabozantinib in Patients with Advanced Ewing Sarcoma or Osteosarcoma (CABONE): A Multicentre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2020, 21, 446–455. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Xu, J.; Sun, X.; Tang, X.; Yan, T.; Yang, R.; Guo, W. Apatinib for Advanced Osteosarcoma after Failure of Standard Multimodal Therapy: An Open Label Phase II Clinical Trial. Oncologist 2019, 24, e542–e550. [Google Scholar] [CrossRef]
- Mir, O.; Brodowicz, T.; Italiano, A.; Wallet, J.; Blay, J.-Y.; Bertucci, F.; Chevreau, C.; Piperno-Neumann, S.; Bompas, E.; Salas, S.; et al. Safety and Efficacy of Regorafenib in Patients with Advanced Soft Tissue Sarcoma (REGOSARC): A Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Oncol. 2016, 17, 1732–1742. [Google Scholar] [CrossRef] [PubMed]
- van der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for Metastatic Soft-Tissue Sarcoma (PALETTE): A Randomised, Double-Blind, Placebo-Controlled Phase 3 Trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Fang, Z.; Hong, X.-N.; Yao, Y.; Sun, P.; Wang, G.; Du, F.; Sun, Y.; Wu, Q.; Qu, G.; et al. Safety and Efficacy of Anlotinib, a Multikinase Angiogenesis Inhibitor, in Patients with Refractory Metastatic Soft Tissue Sarcoma. Clin. Cancer Res. 2018, 24, 5233–5238. [Google Scholar] [CrossRef] [PubMed]
- Pautier, P.; Penel, N.; Ray-Coquard, I.; Italiano, A.; Bompas, E.; Delcambre, C.; Bay, J.-O.; Bertucci, F.; Delaye, J.; Chevreau, C.; et al. A Phase II of Gemcitabine Combined with Pazopanib Followed by Pazopanib Maintenance, as Second-Line Treatment in Patients with Advanced Leiomyosarcomas: A Unicancer French Sarcoma Group Study (LMS03 Study). Eur. J. Cancer 2020, 125, 31–37. [Google Scholar] [CrossRef]
- Navid, F.; Baker, S.D.; McCarville, M.B.; Stewart, C.F.; Billups, C.A.; Wu, J.; Davidoff, A.M.; Spunt, S.L.; Furman, W.L.; McGregor, L.M.; et al. Phase I and Clinical Pharmacology Study of Bevacizumab, Sorafenib, and Low-Dose Cyclophosphamide in Children and Young Adults with Refractory/Recurrent Solid Tumors. Clin. Cancer Res. 2013, 19, 236–246. [Google Scholar] [CrossRef][Green Version]
- Cesne, A.L.; Ray-Coquard, I.; Bui, B.N.; Adenis, A.; Rios, M.; Bertucci, F.; Duffaud, F.; Chevreau, C.; Cupissol, D.; Cioffi, A.; et al. Discontinuation of Imatinib in Patients with Advanced Gastrointestinal Stromal Tumours after 3 Years of Treatment: An Open-Label Multicentre Randomised Phase 3 Trial. Lancet Oncol. 2010, 11, 942–949. [Google Scholar] [CrossRef]
- Iino, M.; Yamamoto, T.; Sakamoto, Y. Outcomes of Unplanned Tyrosine Kinase Inhibitor Discontinuation in Patients with Chronic Myeloid Leukemia: Retrospective Analysis of Real-World Experience in a Single Institution. Hematology 2019, 24, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Kasper, B.; Sleijfer, S.; Litière, S.; Marreaud, S.; Verweij, J.; Hodge, R.A.; Bauer, S.; Kerst, J.M.; Graaf, W.T.A. van der Long-Term Responders and Survivors on Pazopanib for Advanced Soft Tissue Sarcomas: Subanalysis of Two European Organisation for Research and Treatment of Cancer (EORTC) Clinical Trials 62043 and 62072. Ann. Oncol. 2014, 25, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, J.A.; Federman, N.C.; Anderson, P.M.; Macy, M.E.; Riedel, R.F.; Davis, L.E.; Daw, N.C.; Wulff, J.; Kim, A.; Ratan, R.; et al. TK216 for Relapsed/Refractory Ewing Sarcoma: Interim Phase 1/2 Results. J. Clin. Oncol. 2021, 39, 11500. [Google Scholar] [CrossRef]
- Leary, S.E.S.; Wozniak, A.W.; Billups, C.A.; Wu, J.; McPherson, V.; Neel, M.D.; Rao, B.N.; Daw, N.C. Survival of Pediatric Patients after Relapsed Osteosarcoma: The St. Jude Children’s Research Hospital Experience. Cancer 2013, 119, 2645–2653. [Google Scholar] [CrossRef] [PubMed]
- Briccoli, A.; Rocca, M.; Salone, M.; Bacci, G.; Ferrari, S.; Balladelli, A.; Mercuri, M. Resection of Recurrent Pulmonary Metastases in Patients with Osteosarcoma. Cancer 2005, 104, 1721–1725. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Wang, Y.; Luo, Y.; Pang, Z.; Zhou, Y.; Min, L.; Tu, C. Synchronous Lung and Multiple Soft Tissue Metastases Developed from Osteosarcoma of Tibia: A Rare Case Report and Genetic Profile Analysis. BMC Musculoskelet. Disord. 2022, 23, 74. [Google Scholar] [CrossRef]
- Mizuno, T.; Taniguchi, T.; Ishikawa, Y.; Kawaguchi, K.; Fukui, T.; Ishiguro, F.; Nakamura, S.; Yokoi, K. Pulmonary Metastasectomy for Osteogenic and Soft Tissue Sarcoma: Who Really Benefits from Surgical Treatment? Eur. J. Cardio-Thorac. 2012, 43, 795–799. [Google Scholar] [CrossRef]
- Kim, S.; Ott, H.C.; Wright, C.D.; Wain, J.C.; Morse, C.; Gaissert, H.A.; Donahue, D.M.; Mathisen, D.J.; Lanuti, M. Pulmonary Resection of Metastatic Sarcoma: Prognostic Factors Associated with Improved Outcomes. Ann. Thorac. Surg. 2011, 92, 1780–1787. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Crabb, S.J.; Patsios, D.; Sauerbrei, E.; Ellis, P.M.; Arnold, A.; Goss, G.; Leighl, N.B.; Shepherd, F.A.; Powers, J.; Seymour, L.; et al. Tumor Cavitation: Impact on Objective Response Evaluation in Trials of Angiogenesis Inhibitors in Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2009, 27, 404–410. [Google Scholar] [CrossRef]
- Sato, Y.; Nakano, K.; Wang, X.; Fukuda, N.; Urasaki, T.; Ohmoto, A.; Hayashi, N.; Yunokawa, M.; Ono, M.; Tomomatsu, J.; et al. Pre-Treatment Neutrophil-to-Lymphocyte Ratio (NLR) as a Predictive Marker of Pazopanib Treatment for Soft-Tissue Sarcoma. Cancers 2021, 13, 6266. [Google Scholar] [CrossRef] [PubMed]
- Viñal, D.; Martinez, D.; Garcia-Cuesta, J.A.; Gutierrez-Sainz, L.; Martinez-Recio, S.; Villamayor, J.; Martinez-Marin, V.; Gallego, A.; Ortiz-Cruz, E.; Mendiola, M.; et al. Prognostic Value of Neutrophil-to-Lymphocyte Ratio and Other Inflammatory Markers in Patients with High-Risk Soft Tissue Sarcomas. Clin. Transl. Oncol. 2020, 22, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M. A Biomathematical Approach to Clinical Tumor Growth. Cancer 1961, 14, 1272–1294. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Pizzutilo, E.G.; Amatu, A.; Bencardino, K.; Palmeri, L.; Bonazzina, E.F.; Tosi, F.; Stella, G.C.; Burrafato, G.; Scaglione, F.; et al. Retreatment with Anti-EGFR Monoclonal Antibodies in Metastatic Colorectal Cancer: Systematic Review of Different Strategies. Cancer Treat. Rev. 2018, 73, 41–53. [Google Scholar] [CrossRef]
- Yao, H.; Chen, X.; Tan, X. Efficacy and Safety of Apatinib in the Treatment of Osteosarcoma: A Single-Arm Meta-Analysis among Chinese Patients. BMC Cancer 2021, 21, 449. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Xu, J.; Sun, X.; Guo, W.; Gu, J.; Liu, K.; Zheng, B.; Ren, T.; Huang, Y.; Tang, X.; et al. Apatinib plus Camrelizumab (Anti-PD1 Therapy, SHR-1210) for Advanced Osteosarcoma (APFAO) Progressing after Chemotherapy: A Single-Arm, Open-Label, Phase 2 Trial. J. Immunother. Cancer 2020, 8, e000798. [Google Scholar] [CrossRef]
- Wilky, B.A.; Trucco, M.M.; Subhawong, T.K.; Florou, V.; Park, W.; Kwon, D.; Wieder, E.D.; Kolonias, D.; Rosenberg, A.E.; Kerr, D.A.; et al. Axitinib plus Pembrolizumab in Patients with Advanced Sarcomas Including Alveolar Soft-Part Sarcoma: A Single-Centre, Single-Arm, Phase 2 Trial. Lancet Oncol. 2019, 20, 837–848. [Google Scholar] [CrossRef]
- Mangoni, M.; Sottili, M.; Salvatore, G.; Campanacci, D.; Scoccianti, G.; Beltrami, G.; Paoli, C.D.; Dominici, L.; Maragna, V.; Olmetto, E.; et al. Soft Tissue Sarcomas: New Opportunity of Treatment with PARP Inhibitors? La Radiol. Med. 2019, 124, 282–289. [Google Scholar] [CrossRef]
- Blay, J.-Y.; Pérol, D.; Cesne, A.L. Imatinib Rechallenge in Patients with Advanced Gastrointestinal Stromal Tumors. Ann. Oncol. 2012, 23, 1659–1665. [Google Scholar] [CrossRef]
- Balachandran, V.P.; DeMatteo, R.P. Gastrointestinal Stromal Tumors Who Should Get Imatinib and for How Long? Serono Sym. 2014, 48, 165–183. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).