

Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Patient Screening
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Demographic Distribution
3.2. Sinusitis Symptoms and Causative Focus of Odontogenic Maxillary Sinusitis
3.3. Surgical Treatment
3.4. Postoperative Outcome
3.5. Multivariable Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| e.g. | exempli gratia |
| ARONJ | antiresorptive-related osteonecrosis of the jaw |
| IMA | inferior meatal antrostomy |
| FESS | functional endoscopic sinus surgery |
| CAP | chronic apical periodontitis |
| CBCT | cone beam computer tomography |
| CT | computer tomography |
References
- Craig, J.R. Odontogenic sinusitis: A state-of-the-art review. World J. Otorhinolaryngol. Head Neck Surg. 2022, 8, 8–15. [Google Scholar] [CrossRef]
- Psillas, G.; Papaioannou, D.; Petsali, S.; Dimas, G.G.; Constantinidis, J. Odontogenic maxillary sinusitis: A comprehensive review. J. Dent. Sci. 2021, 16, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Little, R.E.; Long, C.M.; Loehrl, T.A.; Poetker, D.M. Odontogenic sinusitis: A review of the current literature. Laryngoscope Investig. Otolaryngol. 2018, 3, 110–114. [Google Scholar] [CrossRef]
- Zirk, M.; Dreiseidler, T.; Pohl, M.; Rothamel, D.; Buller, J.; Peters, F.; Zöller, J.E.; Kreppel, M. Odontogenic sinusitis maxillaris: A retrospective study of 121 cases with surgical intervention. J. Cranio-Maxillo-Facial Surg. 2017, 45, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Sinusitis of odontogenic origin. Otolaryngol. Head Neck Surg. 2006, 135, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Hastan, D.; Fokkens, W.J.; Bachert, C.; Newson, R.B.; Bislimovska, J.; Bockelbrink, A.; Bousquet, P.J.; Brozek, G.; Bruno, A.; Dahlén, S.E.; et al. Chronic rhinosinusitis in Europe—An underestimated disease. A GA(2)LEN study. Allergy 2011, 66, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Dietz de Loos, D.; Lourijsen, E.S.; Wildeman, M.A.M.; Freling, N.J.M.; Wolvers, M.D.J.; Reitsma, S.; Fokkens, W.J. Prevalence of chronic rhinosinusitis in the general population based on sinus radiology and symptomatology. J. Allergy Clin. Immunol. 2019, 143, 1207–1214. [Google Scholar] [CrossRef]
- Stuck, B.A.; Beule, A.; Jobst, D.; Klimek, L.; Laudien, M.; Lell, M.; Vogl, T.J.; Popert, U. Guideline for “rhinosinusitis”-long version: S2k guideline of the German College of General Practitioners and Family Physicians and the German Society for Oto-Rhino-Laryngology, Head and Neck Surgery. HNO 2018, 66, 38–74. [Google Scholar] [CrossRef]
- Galli, M.; De Soccio, G.; Cialente, F.; Candelori, F.; Federici, F.R.; Ralli, M.; De Vincentiis, M.; Minni, A. Chronic maxillary sinusitis of dental origin and oroantral fistula: The results of combined surgical approach in an Italian university hospital. Bosn. J. Basic Med. Sci. 2020, 20, 524–530. [Google Scholar] [CrossRef]
- Shanti, R.M.; Alawi, F.; Lee, S.M.; Henderson, A.J.; Sangal, N.R.; Adappa, N.D. Multidisciplinary approaches to odontogenic lesions. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 36–45. [Google Scholar] [CrossRef]
- Maillet, M.; Bowles, W.R.; McClanahan, S.L.; John, M.T.; Ahmad, M. Cone-beam computed tomography evaluation of maxillary sinusitis. J. Endod. 2011, 37, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Aukštakalnis, R.; Simonavičiūtė, R.; Simuntis, R. Treatment options for odontogenic maxillary sinusitis: A review. Stomatologija 2018, 20, 22–26. [Google Scholar] [PubMed]
- Bachert, C.; Marple, B.; Schlosser, R.J.; Hopkins, C.; Schleimer, R.P.; Lambrecht, B.N.; Bröker, B.M.; Laidlaw, T.; Song, W.-J. Adult chronic rhinosinusitis. Nat. Rev. Dis. Primers 2020, 6, 86. [Google Scholar] [CrossRef] [PubMed]
- Nurchis, M.C.; Pascucci, D.; Lopez, M.A.; Moffa, A.; Passarelli, P.C.; Bressi, F.; Casale, M.; Damiani, G. Epidemiology of odontogenic sinusitis: An old, underestimated disease, even today. A narrative literature review. J. Biol. Regul. Homeost. Agents 2020, 34, 195–200. [Google Scholar] [PubMed]
- Saibene, A.M.; Pipolo, C.; Borloni, R.; Felisati, G. ENT and dentist cooperation in the management of odontogenic sinusitis. A review. Acta Otorhinolaryngol. Ital. 2021, 41, 116–123. [Google Scholar] [CrossRef]
- Allevi, F.; Fadda, G.L.; Rosso, C.; Martino, F.; Pipolo, C.; Cavallo, G.; Felisati, G.; Saibene, A.M. Treatment of Sinusitis Following Dental Implantation: A Systematic Review and Meta-Analysis. Am. J. Rhinol. Allergy 2022, 4, 19458924221084484. [Google Scholar] [CrossRef]
- Troeltzsch, M.; Pache, C.; Troeltzsch, M.; Kaeppler, G.; Ehrenfeld, M.; Otto, S.; Probst, F. Etiology and clinical characteristics of symptomatic unilateral maxillary sinusitis: A review of 174 cases. J. Craniomaxillofac. Surg. 2015, 43, 1522–1529. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Loomer, P.M.; Wallace, S.S. A comprehensive clinical review of maxillary sinus floor elevation: Anatomy, techniques, biomaterials and complications. Br. J. Oral. Maxillofac. Surg. 2016, 54, 724–730. [Google Scholar] [CrossRef]
- Chisci, G.; Hatia, A.; Chisci, E.; Chisci, D.; Gennaro, P.; Gabriele, G. Socket Preservation after Tooth Extraction: Particulate Autologous Bone vs. Deproteinized Bovine Bone. Bioengineering 2023, 10, 421. [Google Scholar] [CrossRef]
- Candotto, V.; Gallusi, G.; Piva, A.; Baldoni, M.; Di Girolamo, M. Complications in sinus lift. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. 1), 139–142. [Google Scholar]
- Martu, C.; Martu, M.A.; Maftei, G.A.; Diaconu-Popa, D.A.; Radulescu, L. Odontogenic Sinusitis: From Diagnosis to Treatment Possibilities—A Narrative Review of Recent Data. Diagnostics 2022, 12, 1600. [Google Scholar] [CrossRef]
- Elwany, S.; Ibrahim, A.A.; Hussein, W.K.A.; Medra, A.M.; Elwany, N. Ten-year experience with multidisciplinary diagnosis and treatment of odontogenic sinusitis. J. Laryngol. Otol. 2021, 135, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Tsuzuki, K.; Kuroda, K.; Hashimoto, K.; Okazaki, K.; Noguchi, K.; Kishimoto, H.; Nishikawa, H.; Sakagami, M. Odontogenic chronic rhinosinusitis patients undergoing tooth extraction: Oral surgeon and otolaryngologist viewpoints and appropriate management. J. Laryngol. Otol. 2020, 134, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Workman, A.D.; Granquist, E.J.; Adappa, N.D. Odontogenic sinusitis: Developments in diagnosis, microbiology, and treatment. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 27–33. [Google Scholar] [CrossRef]
- Craig, J.R.; Tataryn, R.W.; Aghaloo, T.L.; Pokorny, A.T.; Gray, S.T.; Mattos, J.L.; Poetker, D.M. Management of odontogenic sinusitis: Multidisciplinary consensus statement. Int. Forum Allergy Rhinol. 2020, 10, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Chitose, S.I.; Sato, K.; Sato, F.; Ono, T.; Umeno, H. Pathophysiology of current odontogenic maxillary sinusitis and endoscopic sinus surgery preceding dental treatment. Auris Nasus Larynx 2021, 48, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Naros, A.; Peters, J.P.; Biegner, T.; Weise, H.; Krimmel, M.; Reinert, S. Fungus Ball of the Maxillary Sinus-Modern Treatment by Osteoplastic Approach and Functional Endoscopic Sinus Surgery. J. Oral. Maxillofac. Surg. 2019, 77, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Lindorf, H.H. Osteoplastic surgery of the sinus maxillaris--the “bone lid”-method. J. Maxillofac. Surg. 1984, 12, 271–276. [Google Scholar] [CrossRef]
- Costa, F.; Emanuelli, E.; Franz, L.; Tel, A.; Robiony, M. Single-step surgical treatment of odontogenic maxillary sinusitis: A retrospective study of 98 cases. J. Craniomaxillofac. Surg. 2019, 47, 1249–1254. [Google Scholar] [CrossRef]
- Kim, S.W.; Lee, I.H.; Kim, S.W.; Kim, D.H. Points to consider before the insertion of maxillary implants: The otolaryngologist’s perspective. J. Periodontal Implant Sci. 2019, 49, 346–354. [Google Scholar] [CrossRef]
- Molteni, M.; Bulfamante, A.M.; Pipolo, C.; Lozza, P.; Allevi, F.; Pisani, A.; Chiapasco, M.; Portaleone, S.M.; Scotti, A.; Maccari, A.; et al. Odontogenic sinusitis and sinonasal complications of dental treatments: A retrospective case series of 480 patients with critical assessment of the current classification. Acta Otorhinolaryngol. Ital. 2020, 40, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Maurer, P.; Sandulescu, T.; Kriwalsky, M.S.; Rashad, A.; Hollstein, S.; Stricker, I.; Hölzle, F.; Kunkel, M. Bisphosphonate-related osteonecrosis of the maxilla and sinusitis maxillaris. Int. J. Oral Maxillofac. Surg. 2011, 40, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Bravo Cordero, G.; Minzer Ferrer, S.; Fernández, L. Odontogenic sinusitis, oro-antral fistula and surgical repair by Bichat’s fat pad: Literature review. Acta Otorrinolaringol. Esp. 2016, 67, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Parvini, P.; Obreja, K.; Begic, A.; Schwarz, F.; Becker, J.; Sader, R.; Salti, L. Decision-making in closure of oroantral communication and fistula. Int. J. Implant Dent. 2019, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Chun, B.D.; Kim, U.K.; Choi, N.R.; Choi, H.S.; Hwang, D.S. Versatility of the pedicled buccal fat pad flap for the management of oroantral fistula: A retrospective study of 25 cases. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 50. [Google Scholar] [CrossRef]
- Al-Belasy, F.A. Inferior meatal antrostomy: Is it necessary after radical sinus surgery through the Caldwell-Luc approach? J. Oral Maxillofac. Surg. 2004, 62, 559–562. [Google Scholar] [CrossRef]
- Meyers, A.D.; Hawes, M.J. Nasolacrimal obstruction after inferior meatus nasal antrostomy. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 208–211. [Google Scholar] [CrossRef]
- Kennedy, D.W.; Shaalan, H. Reevaluation of maxillary sinus surgery: Experimental study in rabbits. Ann. Otol. Rhinol. Laryngol. 1989, 98, 901–906. [Google Scholar] [CrossRef]
- Rosenfeld, E.; Ben-Zvi, Y.; Gillman, L.; Avishai, G.; Sella, A.; Chaushu, G. Is inferior meatal antrostomy still relevant? A 12-year analysis of 93 oroantral fistulae closure with concomitant Caldwell-Luc operations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 180–185. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Kumar, K.A.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical practice guideline (update): Adult Sinusitis Executive Summary. Otolaryngol. Head Neck Surg. 2015, 152, 598–609. [Google Scholar] [CrossRef]
- Yanagisawa, E.; Joe, J. Inferior meatal antrostomy: Is it still indicated? Ear Nose Throat J. 1997, 76, 368–370. [Google Scholar] [CrossRef] [PubMed]
- Landsberg, R.; Warman, M.; Margulis, A.; Masalha, M. The Rationale for Endoscopic Inferior Meatal Antrostomy. ORL J. Otorhinolaryngol. Relat. Spec. 2019, 81, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Bhattacharyya, N.; Desrosiers, M.; Khan, A.H. Burden of Disease in Chronic Rhinosinusitis with Nasal Polyps. J. Asthma Allergy 2021, 14, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Matheny, K.E.; Duncavage, J.A. Contemporary indications for the Caldwell-Luc procedure. Curr. Opin. Otolaryngol. Head Neck Surg. 2003, 11, 23–26. [Google Scholar] [CrossRef]
- Andric, M.; Saranovic, V.; Drazic, R.; Brkovic, B.; Todorovic, L. Functional endoscopic sinus surgery as an adjunctive treatment for closure of oroantral fistulae: A retrospective analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 510–516. [Google Scholar] [CrossRef]
- Hajiioannou, J.; Koudounarakis, E.; Alexopoulos, K.; Kotsani, A.; Kyrmizakis, D.E. Maxillary sinusitis of dental origin due to oroantral fistula, treated by endoscopic sinus surgery and primary fistula closure. J. Laryngol. Otol. 2020, 124, 986–989. [Google Scholar] [CrossRef]
- Ohyama, Y.; Ogawa, M.; Yokoo, S. Novel Management for Severe Odontogenic Maxillary Sinusitis Based on Pathophysiology. Case Rep. Dent. 2022, 27, 1614739. [Google Scholar] [CrossRef]
- Yoo, B.J.; Jung, S.M.; Lee, H.N.; Kim, H.G.; Chung, J.H.; Jeong, J.H. Treatment Strategy for Odontogenic Sinusitis. Am. J. Rhinol. Allergy 2021, 35, 206–212. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]


{kind=link}
| Study Population | ||
|---|---|---|
| If | n | % |
| Total | 164 | 100% |
| Gender | ||
| male | 84 | 51.2% |
| female | 80 | 48.8% |
| Patient age | ||
| <65 years | 117 | 71.3% |
| ≥65 years | 47 | 28.7% |
| Sinusitis symptoms | ||
| yes | 99 | 60.4% |
| no | 65 | 39.6% |
| Causative focus | ||
| ARONJ | 15 | 9.1% |
| CAP | 85 | 51.8% |
| foreign body | 10 | 6.1% |
| oroantral communication | 44 | 26.8% |
| odontogenic cyst | 2 | 1.2% |
| osteomyelitis | 4 | 2.4% |
| peri-implantitis | 1 | 0.6% |
| post-fracture surgery | 1 | 0.6% |
| post-sinus lift procedure | 2 | 1.2% |
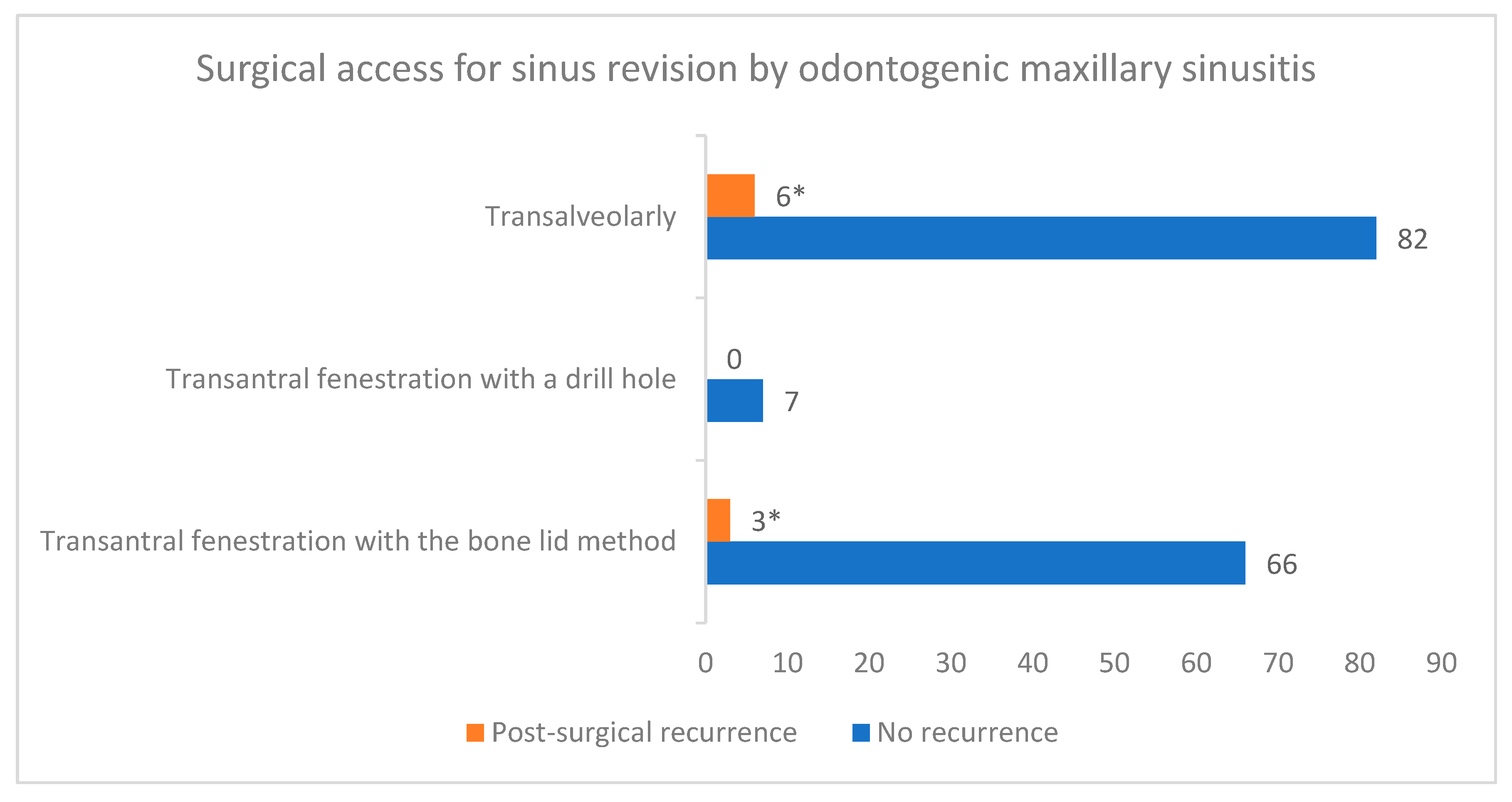
| Surgical access for sinus revision | ||
| transantral fenestration via bone lid method | 69 | 42.1% |
| transantral fenestration via a burr hole | 7 | 4.3% |
| transalveolarly | 88 | 53.7% |
| Multilayer closure with buccal fat pad | ||
| yes | 41 | 25% |
| no | 123 | 75% |
| Inferior meatal antrostomy (IMA) | ||
| yes | 72 | 43.9% |
| no | 92 | 56.1% |
| Sinusitis recurrence and surgical revision | ||
| yes | 9 | 5.5% |
| no | 155 | 94.5% |
| Causative Focus of Odontogenic Maxillary Sinusitis | Post-Surgical Disease Recurrence | ||||||
|---|---|---|---|---|---|---|---|
| Yes | No | Total | p Value * | ||||
| n/% | n/% | n/% | |||||
| ARONJ | 3 | 20% | 12 | 80% | 15 | 9.15% | 0.0375 |
| CAP | 2 | 2.35% | 83 | 97.65% | 85 | 51.83% | 0.0898 |
| foreign body | 0 | 0 | 10 | 100% | 10 | 6.10% | 1.0000 |
| oroantral communication | 3 | 6.82% | 41 | 93.18% | 44 | 26.83% | 0.7025 |
| odontogenic cyst | 0 | 0 | 2 | 100% | 2 | 1.22% | 1.0000 |
| osteomyelitis | 1 | 25% | 3 | 75% | 4 | 2.44% | 0.2038 |
| periimplantitis | 0 | 0 | 1 | 100% | 1 | 0.61% | 1.0000 |
| post-fracture surgery | 0 | 0 | 1 | 100% | 1 | 0.61% | 1.0000 |
| post-sinus lift procedure | 0 | 0 | 2 | 100% | 2 | 1.22% | 1.0000 |
| Total | 9 | 5.48% | 155 | 94.52% | 164 | 100% | 0.1046 |
| Post-Surgical Recurrence of OMS | p Value | ||
|---|---|---|---|
| Yes (n/%) | No (n/%) | ||
| Patient age | |||
| <65 years | 6 (5.12%) | 111 (94.88%) | p = 0.7166 * |
| ≥65 years | 3 (6.38%) | 44 (93.62%) | |
| Multilayer closure with buccal fat pad | |||
| Yes | 1 (2.43%) | 40 (97.57%) | p = 0.4526 ** |
| No | 8 (6.50%) | 115 (93.50%) | |
| Intraoperatively-performed IMA | |||
| Yes | 2 (2.77%) | 70 (97.33%) | p = 0.3010 *** |
| No | 7 (7.60%) | 85 (92.40%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakkas, A.; Weiß, C.; Ebeling, M.; Pietzka, S.; Wilde, F.; Evers, T.; Thiele, O.C.; Mischkowski, R.A.; Scheurer, M. Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View. J. Clin. Med. 2023, 12, 3670. https://doi.org/10.3390/jcm12113670
Sakkas A, Weiß C, Ebeling M, Pietzka S, Wilde F, Evers T, Thiele OC, Mischkowski RA, Scheurer M. Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View. Journal of Clinical Medicine. 2023; 12(11):3670. https://doi.org/10.3390/jcm12113670
Chicago/Turabian StyleSakkas, Andreas, Christel Weiß, Marcel Ebeling, Sebastian Pietzka, Frank Wilde, Theo Evers, Oliver Christian Thiele, Robert Andreas Mischkowski, and Mario Scheurer. 2023. "Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View" Journal of Clinical Medicine 12, no. 11: 3670. https://doi.org/10.3390/jcm12113670
APA StyleSakkas, A., Weiß, C., Ebeling, M., Pietzka, S., Wilde, F., Evers, T., Thiele, O. C., Mischkowski, R. A., & Scheurer, M. (2023). Factors Influencing Recurrence after Surgical Treatment of Odontogenic Maxillary Sinusitis: An Analysis from the Oral and Maxillofacial Surgery Point of View. Journal of Clinical Medicine, 12(11), 3670. https://doi.org/10.3390/jcm12113670