
Nailfold Videocapillaroscopic Alterations as Markers of Microangiopathy in COVID-19 Patients

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
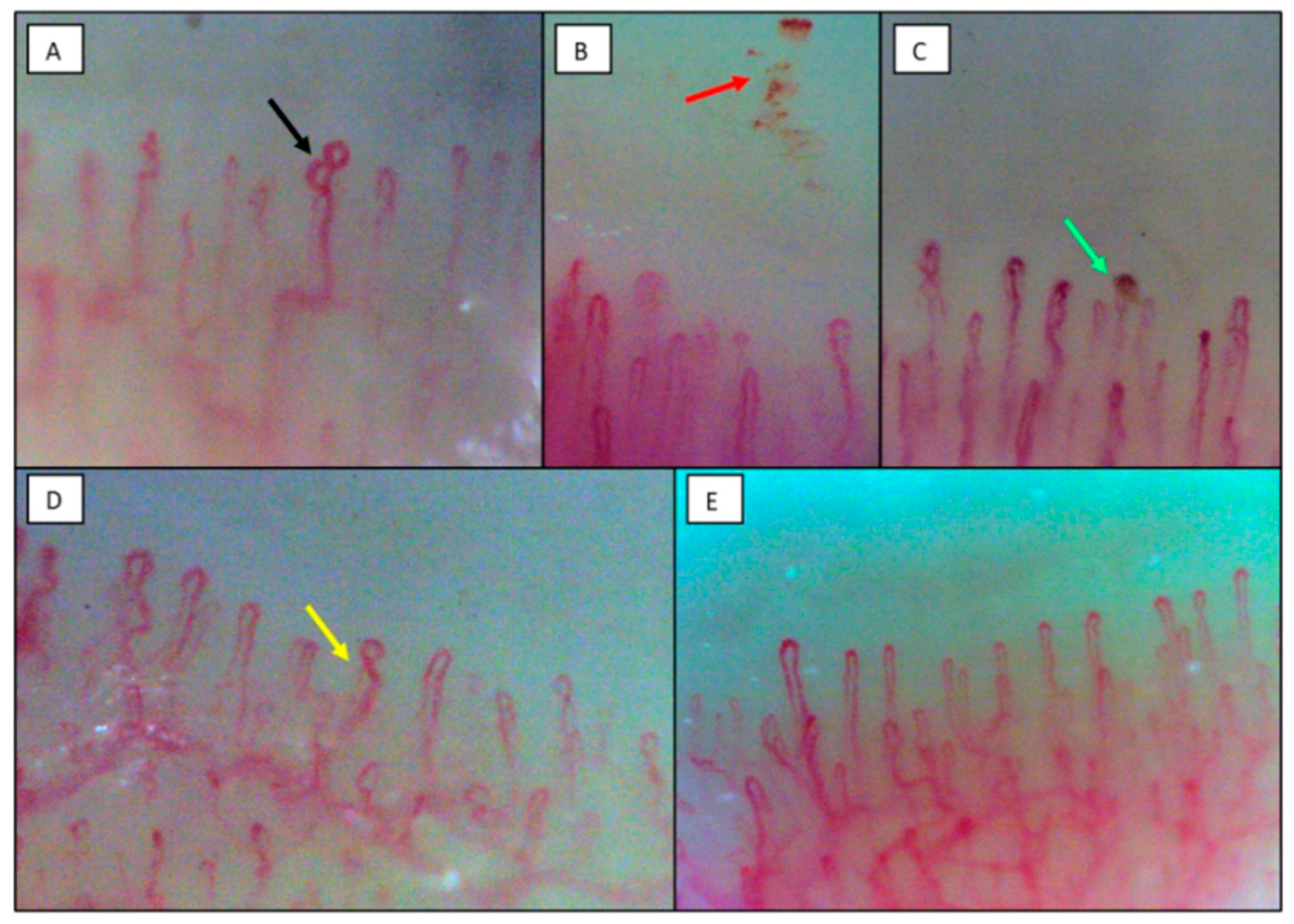
2.2. Nailfold Videocapillaroscopy
2.3. Laboratory Tests
2.4. Histopathology
2.5. Statistical Analysis
3. Results
3.1. Clinical, Laboratory and Nailfold Videocapillaroscopic Findings of COVID-19 Patients in the Milan Cohort
3.2. Clinical and Histopathological Findings in Patients Died of COVID-19 in the New Orleans Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Bonaventura, A.; Vecchié, A.; Dagna, L.; Martinod, K.; Dixon, D.L.; Van Tassell, B.W.; Dentali, F.; Montecucco, F.; Massberg, S.; Levi, M.; et al. Endothelial dysfunction and immunothrombosis as key pathogenic mechanisms in COVID-19. Nat. Rev. Immunol. 2021, 21, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Griffini, S.; Lamorte, G.; Grovetti, E.; Uceda Renteria, S.C.; Malvestiti, F.; Scudeller, L.; Bandera, A.; Peyvandi, F.; Prati, D.; et al. Chromosome 3 cluster rs11385942 variant links complement activation with severe COVID-19. J. Autoimmun. 2021, 117, 102595. [Google Scholar] [CrossRef]
- Herrick, A.L.; Cutolo, M. Clinical implications from capillaroscopic analysis in patients with Raynaud’s phenomenon and systemic sclerosis. Arthritis Rheum. 2010, 62, 2595–2604. [Google Scholar] [CrossRef]
- Bernero, E.; Sulli, A.; Ferrari, G.; Ravera, F.; Pizzorni, C.; Ruaro, B.; Zampogna, G.; Alessandri, E.; Cutolo, M. Prospective capillaroscopy-based study on transition from primary to secondary Raynaud’s phenomenon: Preliminary results. Reumatismo 2013, 65, 186–191. [Google Scholar] [CrossRef] [PubMed]
- D’Oria, M.; Gandin, I.; Riccardo, P.; Hughes, M.; Lepidi, S.; Salton, F.; Confalonieri, P.; Confalonieri, M.; Tavano, S.; Ruaro, B. Correlation between Microvascular Damage and Internal Organ Involvement in Scleroderma: Focus on Lung Damage and Endothelial Dysfunction. Diagnostics 2022, 13, 55. [Google Scholar] [CrossRef] [PubMed]
- Ingegnoli, F.; Gualtierotti, R. A systematic overview on the use and relevance of capillaroscopy in systemic sclerosis. Expert Rev. Clin. Immunol. 2013, 9, 1091–1097. [Google Scholar] [CrossRef]
- Sikorska, D.; Kamińska, D.; Catar, R.; Wu, D.; Zhao, H.; Wang, P.; Kamhieh-Milz, J.; Banasik, M.; Kusztal, M.; Cielecka, M.; et al. Nailfold Videocapillaroscopy for Non-Invasive Assessment of Microcirculation and Prognostic Correlation with Endothelial Dysfunction, Cardiovascular Risk Factors, and Non-HLA Antibodies in Heart Transplant Recipients: A Pilot Study. J. Clin. Med. 2023, 12, 2302. [Google Scholar] [CrossRef] [PubMed]
- Andrade, L.E.; Gabriel Júnior, A.; Assad, R.L.; Ferrari, A.J.; Atra, E. Panoramic nailfold capillaroscopy: A new reading method and normal range. Semin. Arthritis Rheum. 1990, 20, 21–31. [Google Scholar] [CrossRef]
- Smith, V.; Herrick, A.L.; Ingegnoli, F.; Damjanov, N.; De Angelis, R.; Denton, C.P.; Distler, O.; Espejo, K.; Foeldvari, I.; Frech, T.; et al. Standardisation of nailfold capillaroscopy for the assessment of patients with Raynaud’s phenomenon and systemic sclerosis. Autoimmun. Rev. 2020, 19, 102458. [Google Scholar] [CrossRef] [PubMed]
- Maricq, H.R.; LeRoy, E.C. Patterns of finger capillary abnormalities in connective tissue disease by “wide-field” microscopy. Arthritis Rheum. 1973, 16, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Ciaffi, J.; Ajasllari, N.; Mancarella, L.; Brusi, V.; Meliconi, R.; Ursini, F. Nailfold capillaroscopy in common non-rheumatic conditions: A systematic review and applications for clinical practice. Microvasc. Res. 2020, 131, 104036. [Google Scholar] [CrossRef] [PubMed]
- Rosei, C.A.; Gaggero, A.; Famà, F.; Malerba, P.; Chiarini, G.; Nardin, M.; Brami, V.; Rossini, C.; Coschignano, M.A.; Porteri, E.; et al. Skin capillary alterations in patients with acute SARS-CoV-2 infection. J. Hypertens. 2022, 40, 2385–2393. [Google Scholar] [CrossRef] [PubMed]
- Sulli, A.; Gotelli, E.; Bica, P.F.; Schiavetti, I.; Pizzorni, C.; Aloè, T.; Grosso, M.; Barisione, E.; Paolino, S.; Smith, V.; et al. Detailed videocapillaroscopic microvascular changes detectable in adult COVID-19 survivors. Microvasc. Res. 2022, 142, 104361. [Google Scholar] [CrossRef]
- Çakmak, F.; Demirbuga, A.; Demirkol, D.; Gümüş, S.; Torun, S.H.; Kayaalp, G.K.; Ömeroglu, R.E.; Somer, A.; Uysalol, M.; Yıldız, R.; et al. Nailfold capillaroscopy: A sensitive method for evaluating microvascular involvement in children with SARS-CoV-2 infection. Microvasc. Res. 2021, 138, 104196. [Google Scholar] [CrossRef]
- Natalello, G.; De Luca, G.; Gigante, L.; Campochiaro, C.; De Lorenzis, E.; Verardi, L.; Paglionico, A.; Petricca, L.; Martone, A.M.; Calvisi, S.; et al. Nailfold capillaroscopy findings in patients with coronavirus disease 2019: Broadening the spectrum of COVID-19 microvascular involvement. Microvasc. Res. 2021, 133, 104071. [Google Scholar] [CrossRef]
- Mostmans, Y.; Smith, V.; Cutolo, M.; Melsens, K.; Battist, S.; Benslimane, A.; Corazza, F.; Richert, B.; Michel, O.; Kolivras, A. Nailfold videocapillaroscopy and serum vascular endothelial growth factor in probable COVID-19-induced chilblains: A cross-sectional study to assess microvascular impairment. Br. J. Dermatol. 2022, 187, 1017–1019. [Google Scholar] [CrossRef]
- Starkey, S.Y.; Mar, K.; Kashetsky, N.; Lam, J.M.; Dutz, J.; Mukovozov, I. Chilblain-like lesions coinciding with the SARS-CoV-2 pandemic. Clin. Dermatol. 2022. S0738-081X(22)00126-2. [Google Scholar] [CrossRef]
- Cutolo, M.; Sulli, A.; Smith, V.; Gotelli, E. Emerging nailfold capillaroscopic patterns in COVID-19: From acute patients to survivors. Reumatismo 2023, 74, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Moore, T.; O’Leary, N.; Tracey, A.; Ennis, H.; Dinsdale, G.; Murray, A.; Roberts, C.; Herrick, A.L. A study comparing videocapillaroscopy and dermoscopy in the assessment of nailfold capillaries in patients with systemic sclerosis-spectrum disorders. Rheumatology 2015, 54, 1435–1442. [Google Scholar] [CrossRef]
- Sambataro, D.; Sambataro, G.; Zaccara, E.; Maglione, W.; Polosa, R.; Afeltra, A.M.; Vitali, C.; Del Papa, N. Nailfold videocapillaroscopy micro-haemorrhage and giant capillary counting as an accurate approach for a steady state definition of disease activity in systemic sclerosis. Arthritis Res. Ther. 2014, 16, 462. [Google Scholar] [CrossRef] [PubMed]
- Sulli, A.; Secchi, M.E.; Pizzorni, C.; Cutolo, M. Scoring the nailfold microvascular changes during the capillaroscopic analysis in systemic sclerosis patients. Ann. Rheum. Dis. 2008, 67, 885–887. [Google Scholar] [CrossRef]
- Ingegnoli, F.; Gualtierotti, R.; Lubatti, C.; Bertolazzi, C.; Gutierrez, M.; Boracchi, P.; Fornili, M.; De Angelis, R. Nailfold capillary patterns in healthy subjects: A real issue in capillaroscopy. Microvasc. Res. 2013, 90, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Bernardino, V.; Rodrigues, A.; Lladó, A.; Panarra, A. Nailfold capillaroscopy and autoimmune connective tissue diseases in patients from a Portuguese nailfold capillaroscopy clinic. Rheumatol. Int. 2020, 40, 295–301. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Damoiseaux, J.; Kallenberg, C.; Sack, U.; Witte, T.; Herold, M.; Bossuyt, X.; Musset, L.; Cervera, R.; Plaza-Lopez, A.; et al. International recommendations for the assessment of autoantibodies to cellular antigens referred to as anti-nuclear antibodies. Ann. Rheum. Dis. 2014, 73, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Chighizola, C.B.; Cesana, L.; Privitera, D.; Ingegnoli, F.; Mastaglio, C.; Meroni, P.L.; Borghi, M.O. Immune complexes containing scleroderma-specific autoantibodies induce a profibrotic and proinflammatory phenotype in skin fibroblasts. Arthritis Res. Ther. 2018, 20, 187. [Google Scholar] [CrossRef]
- Fox, B.J.; Hockley, J.; Rigsby, P.; Dolman, C.; Meroni, P.L.; Rönnelid, J. A WHO Reference Reagent for lupus (anti-dsDNA) antibodies: International collaborative study to evaluate a candidate preparation. Ann. Rheum. Dis. 2019, 78, 1677–1680. [Google Scholar] [CrossRef]
- Valenti, L.; Tripodi, A.; La Mura, V.; Pelusi, S.; Bianco, C.; Scalambrino, E.; Margarita, S.; Malvestiti, F.; Ronzoni, L.; Clerici, M.; et al. Clinical and genetic determinants of the fatty liver-coagulation balance interplay in individuals with metabolic dysfunction. JHEP Rep. Innov. Hepatol. 2022, 4, 100598. [Google Scholar] [CrossRef]
- Franchini, M.; Crestani, S.; Frattini, F.; Sissa, C.; Bonfanti, C. ABO blood group and von Willebrand factor: Biological implications. Clin. Chem. Lab. Med. 2014, 52, 1273–1276. [Google Scholar] [CrossRef]
- Valenti, L.; Villa, S.; Baselli, G.; Temporiti, R.; Bandera, A.; Scudeller, L.; Prati, D. Association of ABO blood group and secretor phenotype with severe COVID-19. Transfusion 2020, 60, 3067–3070. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, F.; Ellinghaus, D.; Juzenas, S.; Lerga-Jaso, J.; Wendorff, M.; Maya-Miles, D.; Uellendahl-Werth, F.; ElAbd, H.; Rühlemann, M.C.; Arora, J.; et al. Detailed stratified GWAS analysis for severe COVID-19 in four European populations. Hum. Mol. Genet. 2022, 31, 3945–3966. [Google Scholar] [CrossRef]
- Ellinghaus, D.; Degenhardt, F.; Bujanda, L.; Buti, M.; Albillos, A.; Invernizzi, P.; Fernández, J.; Prati, D.; Baselli, G.; Asselta, R.; et al. Genomewide Association Study of Severe Covid-19 with Respiratory Failure. N. Engl. J. Med. 2020, 383, 1522–1534. [Google Scholar] [PubMed]
- Mapping the human genetic architecture of COVID-19. Nature 2021, 600, 472–477. [CrossRef] [PubMed]
- Gualtierotti, R.; Ingegnoli, F.; Griffini, S.; Grovetti, E.; Borghi, M.O.; Bucciarelli, P.; Meroni, P.L.; Cugno, M. Detection of early endothelial damage in patients with Raynaud’s phenomenon. Microvasc. Res. 2017, 113, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Falgout, L.; Vander Heide, R.S. COVID-19 myocarditis: Quantitative analysis of the inflammatory infiltrate and a proposed mechanism. Cardiovasc. Pathol. Off. J. Soc. Cardiovasc. Pathol. 2021, 54, 107361. [Google Scholar] [CrossRef] [PubMed]
- Herrick, A.L.; Illingworth, K.; Blann, A.; Hay, C.R.; Hollis, S.; Jayson, M.I. Von Willebrand factor, thrombomodulin, thromboxane, beta-thromboglobulin and markers of fibrinolysis in primary Raynaud’s phenomenon and systemic sclerosis. Ann. Rheum. Dis. 1996, 55, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Cerinic, M.M.; Valentini, G.; Sorano, G.G.; D’Angelo, S.; Cuomo, G.; Fenu, L.; Generini, S.; Cinotti, S.; Morfini, M.; Pignone, A.; et al. Blood coagulation, fibrinolysis, and markers of endothelial dysfunction in systemic sclerosis. Semin. Arthritis Rheum. 2003, 32, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Biguzzi, E.; Siboni, S.M.; le Cessie, S.; Baronciani, L.; Rosendaal, F.R.; van Hylckama Vlieg, A.; Peyvandi, F. Increasing levels of von Willebrand factor and factor VIII with age in patients affected by von Willebrand disease. J. Thromb. Haemost. 2021, 19, 96–106. [Google Scholar] [CrossRef]
- Marasini, B.; Cugno, M.; Bassani, C.; Stanzani, M.; Bottasso, B.; Agostoni, A. Tissue-type plasminogen activator and von Willebrand factor plasma levels as markers of endothelial involvement in patients with Raynaud’s phenomenon. Int. J. Microcirc. Clin. Exp. 1992, 11, 375–382. [Google Scholar] [PubMed]
- Jenkins, P.V.; O’Donnell, J.S. ABO blood group determines plasma von Willebrand factor levels: A biologic function after all? Transfusion 2006, 46, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, T.; Pigazzini, S.; Degenhardt, F.; Cordioli, M.; Butler-Laporte, G.; Maya-Miles, D.; Bujanda, L.; Bouysran, Y.; Niemi, M.E.; Palom, A.; et al. Age-dependent impact of the major common genetic risk factor for COVID-19 on severity and mortality. J. Clin. Investig. 2021, 131, e152386. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.E.; Li, G.; Akmatbekov, A.; Harbert, J.L.; Lameira, F.S.; Brown, J.Q.; Vander Heide, R.S. Unexpected Features of Cardiac Pathology in COVID-19 Infection. Circulation 2020, 142, 1123–1125. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| COVID-19 Patients | Healthy Controls | Significance | |
|---|---|---|---|
| AGE (years) | |||
| Median (range) | 56.0 (40.0–84.0) | 52 (39.0–82.0) | n.s. |
| SEX | |||
| M | 10 (66.7%) | 10 (66.7%) | |
| F | 5 (33.3%) | 5 (33.3%) | n.s. |
| BMI (kg/m2) | n.a. | ||
| Median (range) | 28.4 (21.1–37.5) | ||
| Missing | 6 (40.0%) | ||
| BLOOD PRESSURE AT ADMISSION (mmHg) | |||
| Systolic blood pressure, median (range) | 125 (105–145) | n.a. | |
| Diastolic blood pressure, median (range) | 80 (60–90) | ||
| TIME FROM ONSET (days) | |||
| Median (range) | 3.7 (1.6–6.6) | n.a. | |
| MAIN COMORBIDITIES | |||
| Arterial Hypertension | 6 (40%) | 5 (33.3%) | n.s. |
| Betablockers | 3 (20%) | 2 (13.3%) | n.s. |
| Diuretics | 3 (20%) | 1 (6.7%) | n.s. |
| ACE inhibitors | 1 (6.7%) | 2 (13.3%) | n.s. |
| ARB | 4 (26.7%) | 1 (6.7%) | n.s. |
| Dyslipidemia | 4 (26.7%) | 3 (30%) | n.s. |
| Statin | 3 (20%) | 2 (13.3%) | n.s. |
| Diabetes | 2 (13.3%) | 1 (6.7%) | n.s. |
| OXYGEN THERAPY | |||
| Total | 12 (80%) | n.a. | |
| Non-invasive ventilation | 4 (26.7%) | ||
| Invasive ventilation | 0 | ||
| TREATMENT FOR COVID-19 | n.a. | ||
| Steroids | 4 (26.7%) | ||
| LMWH | 14 (93.3%) | ||
| Remdesivir | 3 (20%) | ||
| Hydroxychloroquine | 9 (60%) | ||
| Biological drugs (tocilizumab) | 1 (6.7%) |
| Parameter | Median (Range) | Reference Range |
|---|---|---|
| WBC/mm3 | 6900 (3170–13,780) | (4800–10,800) |
| Neutrophils/mm3 | 4290 (1800–10,410) | (1500–6500) |
| Lymphocytes/mm3 | 1510 (650–2760) | (1200–3400) |
| Hemoglobin, g/dL | 12.2 (9.6–15.5) | (13.5–17.5) |
| MCV, fL | 84.1 (76.4–94.5) | (80–94) |
| Platelets, ×103/mm3 | 344 (175–529) | (130–400) |
| MPV, fL | 10.0 (8.4–11.3) | (9.5–13.1) |
| FBG, mg/dL | 419 (252–894) | (165–350) |
| D-dimer, ng/mL | 991 (437–2128) | (<500) |
| Ferritin, mg/dL | 587 (44–3266) | (30–400) |
| Creatinine, mg/dL | 0.85 (0.44–1.23) | (0.72–1.18) |
| CRP, mg/dL | 1.03 (0.06–18.31) | (<0.5) |
| ALT, IU | 43 (18–109) | (9–59) |
| LDH, IU | 215 (168–333) | (135–225) |
| Glucose, mg/dL | 94 (65–311) | (70–110) |
| Triglycerides, mg/dL | 139 (78–306) | (<150) |
| Total cholesterol, mg/dL | 151 (110–184) | (<190) |
| Parameter | Median (Range) | Reference Range |
|---|---|---|
| VEGF, pg/mL, median (range) | 156 (25–310) | (62–707) |
| VWF, %, median (range) | 198 (48–704) | (50–130) |
| Blood type, n (%) | ||
| A | 6 (40.0%) | |
| AB | 2 (13.3%) | |
| B | 1 (6.7%) | |
| O | 6 (40.0%) | |
| Chromosome 3 cluster rs11385942 G > GA, n (%) | 3 (20%) | |
| Chromosome 9 cluster rs657152 C > A, n (%) | 9 (60%) | |
| Chromosome 19 cluster rs601338 G > A, n (%) | 6 (40%) | |
| ANA positivity, n (%) | 3 (20%) | Negative |
| ANA AC-16, n (%) | 1 (6.7%) | |
| ANA AC-4, n (%) | 1 (6.7%) | |
| ANA AC-8, n (%) | 1 (6.7%) | |
| anti-ENA positivity (RNP, Sm, SSA/B, Scl-70, Jo-1, anti-dsDNA), n (%) | 0 (0%) | Negative |
| COVID-19 Subjects (n = 15) | Healthy Controls (n = 15) | p-Value | |
|---|---|---|---|
| Number of fingers with at least one alteration, median (range) | 2 (0–8) | 1 (0–6) | 0.41 |
| Number of capillaries/mm, median (range) | 7.8 (4.9–10.0) | 8.5 (5.7–10.1) | 0.54 |
| Intercapillary distance, μm, median (range) | 143.1 (90.7–199.2) | 116.9 (31.8–168.9) | 0.03 |
| Internal loop distance, μm, median (range) | 13.9 (9.3–16.6) | 15.4 (12.1–20.2) | 0.02 |
| Loop diameter, μm, median (range) | 42.0 (29.0–63.6) | 47 (32.6–51.6) | 0.34 |
| Apical loop distance, μm, median (range) | 18.5 (13.3–33.9) | 21.4 (12.9–29.1) | 0.28 |
| Loop length, μm, median (range) | 348.0 (180.8–399.2) | 268.5 (190.4–363.9) | 0.01 |
| At least one hemosiderin deposit, n (%) | 14 (93.3) | 4 (26.7) | <0.001 |
| Microhemorrhage, n (%) | 14 (93.3) | 4 (26.7) | <0.001 |
| Microthrombosis, n (%) | 4 (26.7) | 0 (0) | 0.22 |
| Total hemosiderin deposits per patient, n, median (range) | 4 (0–27) | 0 (0-1) | <0.001 |
| More than one enlarged loop, n (%) | 10 (66.7) | 2 (12.5) | 0.002 |
| At least one loop with one cross, n (%) | 15 (100) | 11 (73.3) | 0.10 |
| At least one loop with two or more intersections, n (%) | 15 (100) | 7 (46.7) | 0.002 |
| At least one meandering capillary, n (%) | 10 (66.7) | 1 (6.7) | <0.001 |
| At least one bushy capillary, n (%) | 11 (73.3) | 1 (6.7) | <0.001 |
| AGE (Years) | |
| Median (range) | 62 (47–79) |
| SEX | |
| M | 7 (47%) |
| F | 8 (53%) |
| BMI (kg/m2) | |
| Median (range) | 36.2 (21.4–62.3) |
| TIME FROM ONSET TO DEATH (days) | |
| Median (range) | 17 (0–31) |
| MAIN COMORBIDITIES AND RISK FACTORS | |
| Arterial Hypertension Diabetes | 10 (66%) 7 (47%) |
| OXYGEN THERAPY | |
| Total Invasive ventilation | 14 (93%) 13 (87%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gualtierotti, R.; Fox, S.E.; Da Silva Lameira, F.; Giachi, A.; Valenti, L.; Borghi, M.O.; Meroni, P.L.; Cugno, M.; Peyvandi, F.; on behalf of the CAPCOVID Study Group. Nailfold Videocapillaroscopic Alterations as Markers of Microangiopathy in COVID-19 Patients. J. Clin. Med. 2023, 12, 3727. https://doi.org/10.3390/jcm12113727
Gualtierotti R, Fox SE, Da Silva Lameira F, Giachi A, Valenti L, Borghi MO, Meroni PL, Cugno M, Peyvandi F, on behalf of the CAPCOVID Study Group. Nailfold Videocapillaroscopic Alterations as Markers of Microangiopathy in COVID-19 Patients. Journal of Clinical Medicine. 2023; 12(11):3727. https://doi.org/10.3390/jcm12113727
Chicago/Turabian StyleGualtierotti, Roberta, Sharon E. Fox, Fernanda Da Silva Lameira, Andrea Giachi, Luca Valenti, Maria Orietta Borghi, Pier Luigi Meroni, Massimo Cugno, Flora Peyvandi, and on behalf of the CAPCOVID Study Group. 2023. "Nailfold Videocapillaroscopic Alterations as Markers of Microangiopathy in COVID-19 Patients" Journal of Clinical Medicine 12, no. 11: 3727. https://doi.org/10.3390/jcm12113727