
Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters

 , ,
, ,
Abstract
:1. Introduction
2. Ultrasound Parameters Selected for Examination
2.1. Cervical Dilatation
2.2. Position of the Presenting Part of the Fetus
2.3. Cervical Position
2.4. Cervical Consistency

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protocol |
|---|
| 1. The patient emptied her bladder prior to examination. |
| 2. Image orientation—The apex of the image was displayed at the top of the monitor, and the fetal part was displayed on the left side of the image sector. |
| 3. Activation of the E-cervix program and obtaining of an optimal cervical image— The image plane used for cervical elastography was the same as the one used to measure cervical length (according to the Fetal Medicine Foundation guidelines [25], without applying pressure with the probe to the anterior cervix). |
| 4. Acquisition of cervical strain— After optimal cervical image acquisition, the probe was held still until all motion bars (reliability indicator) turned green (the autofreeze setting for motion bars was used). The patient breathed normally during the acquisition. The image was discarded when active fetal movements occurred during the acquisition, especially fetal limb movement in breech presentation, as it may affect cervical strain. |
| 5. ROI (Region of Interest) caliper placement for strain measurement: (a) Calipers were placed on the grayscale image displayed on the left of the screen, as the elastographic image displayed on the right may be blurred at the margin. (b) By selecting either a 2- or 4-point ROI, a line was drawn along the endocervical canal between the internal and external os of the cervix. If the endocervical line was straight, a 2-point ROI tool was used. With a curved cervix, a 4-point ROI was used to trace the endocervical lining as accurately as possible. (c) After the cervical canal was defined, green points automatically appeared. The points were placed on the four corner edges of the cervix so that the ROI box included the entire cervix area. The entire cervix was included, without adjacent structures such as the bladder or vaginal wall (Figure 4). |
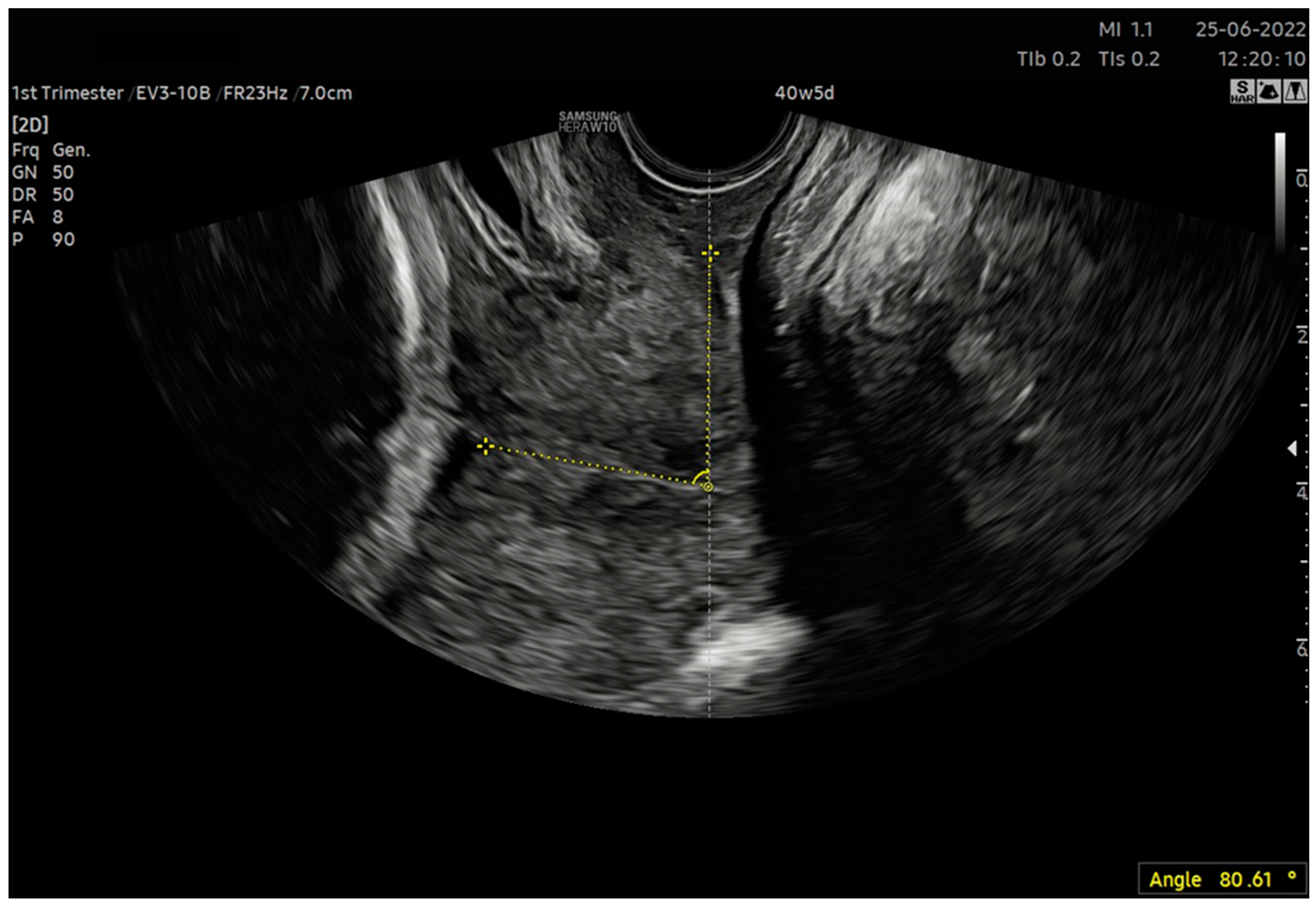
| 6. After calculating the E-Cervix parameters, volumetric image acquisition of the cervix was performed. The 3D image was rotated so that the external os of the cervix was presented en face on the screen; then, we measured the widest dimension of the external cervical os (dilatation—Figure 1). 7. We withdrew the transducer to the area of the vaginal os. 8. The transducer was placed in the vaginal axis; the vagino–cervical angle (VCA) measurement was performed after turning on the “central transducer line” option; the second line was guided tangentially to the axis of the cervical canal. In the case of a bent canal, the line was drawn tangentially to the end part contacting the vagina. We measured the angle formed at the intersection of the abovementioned lines (Figure 3). 9. We measured the AoP with the transducer located near the vaginal opening by drawing two lines—tangent to the long axis of the cross-section through the pubic symphysis and through the bone point of the fetal head being the most advanced in the birth canal (Figure 2). |
2.5. Effacement
3. Materials and Methods
Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cunningham, F.; Leveno, K.J.; Bloom, S.L.; Spong, C.Y.; Dashe, J.S.; Hoffman, B.L.; Casey, B.M.; Sheffield, J.S. Williams Obstetrics; McGraw-Hill Medical: New York, NY, USA, 2014. [Google Scholar]
- Bishop, E.H. Pelvic Scoring for Elective Induction. Obstet. Gynecol. 1964, 24, 266–268. [Google Scholar] [PubMed]
- Faltin-Traub, E.F.; Boulvain, M.; Faltin, D.L.; Extermann, P.; Irion, O. Reliability of the Bishop score before labour induction at term. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 112, 178–181. [Google Scholar] [CrossRef] [PubMed]
- ACOG. Practice Bulletin No. 107: Induction of labour. Obstet. Gynecol. 2009, 114, 386–397. [Google Scholar] [CrossRef]
- Mlodawski, J.; Mlodawska, M. Prostaglandins in the induction of labour–Do we have the optimal substance, dose, and route of administration? Literature review. Med. Stud. Stud. Med. 2021, 37, 162–167. [Google Scholar] [CrossRef]
- de Vaan, M.D.; Ten Eikelder, M.L.; Jozwiak, M.; Palmer, K.R.; Davies-Tuck, M.; Bloemenkamp, K.W.; Mol, B.W.J.; Boulvain, M. Mechanical methods for induction of labour. Cochrane Database Syst. Rev. 2023, 3, CD001233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakub, M.; Marta, M.; Jagoda, G.; Kamila, G.; Stanislaw, G. Is Unfavourable Cervix prior to Labor Induction Risk for Adverse Obstetrical Outcome in Time of Universal Ripening Agents Usage? Single Center Retrospective Observational Study. J. Pregnancy 2020, 2020, 4985693. [Google Scholar] [CrossRef]
- Bajpai, N.; Bhakta, R.; Kumar, P.; Rai, L.; Hebbar, S. Manipal Cervical Scoring System by Transvaginal Ultrasound in Predicting Successful Labour Induction. J. Clin. Diagn. Res. 2015, 9, QC04–QC09. [Google Scholar] [CrossRef]
- Kamel, R.; Garcia, F.S.M.; Poon, L.C.; Youssef, A. The usefulness of ultrasound before induction of labor. Am. J. Obstet. Gynecol. MFM. 2021, 3, 100423. [Google Scholar] [CrossRef]
- Usman, S.; Wilkinson, M.; Barton, H.; Lees, C.C. The feasibility and accuracy of ultrasound assessment in the labor room. J. Matern. Fetal Neonatal. Med. 2019, 32, 3442–3451. [Google Scholar] [CrossRef]
- Zimerman, A.L.; Smolin, A.; Maymon, R.; Weinraub, Z.; Herman, A.; Tobvin, Y. Intrapartum measurement of cervical dilatation using translabial 3-dimensional ultrasonography: Correlation with digital examination and interobserver and intraobserver agreement assessment. J. Ultrasound Med. 2009, 28, 1289–1296. [Google Scholar] [CrossRef]
- Benediktsdottir, S.; Eggebø, T.M.; Salvesen, K.Å. Agreement between transperineal ultrasound measurements and digital examinations of cervical dilatation during labor. BMC Pregnancy Childbirth 2015, 15, 273. [Google Scholar] [CrossRef] [Green Version]
- Dębska, M.; Kretowicz, P.; Dębski, R. Intrapartum sonography–Eccentricity or necessity? J. Ultrason. 2015, 15, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Hjartardóttir, D.H.; Lund, M.S.H.; Benediktsdóttir, D.S.; Geirsson, D.R.T.; Eggebø, D.T.M. Can ultrasound on admission in active labor predict labor duration and a spontaneous delivery? Am. J. Obstet. Gynecol. MFM 2021, 23, 100383. [Google Scholar] [CrossRef] [PubMed]
- Cho, G.J.; Hong, H.R.; Seol, H.J.; Koo, B.H.; Hong, S.C.; Oh, M.J.; Kim, H.J. Use of the angle of progression on ultrasonography to predict spontaneous onset of labor within 7 days. J. Perinat. Med. 2015, 43, 185–189. [Google Scholar] [CrossRef]
- Nassr, A.A.; Berghella, V.; Hessami, K.; Bibbo, C.; Bellussi, F.; Robinson, J.N.; Marsoosi, V.; Tabrizi, R.; Safari-Faramani, R.; Tolcher, M.C.; et al. Intrapartum ultrasound measurement of angle of progression at the onset of the second stage of labor for prediction of spontaneous vaginal delivery in term singleton pregnancies: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2021, 226, 205–214.e2. [Google Scholar] [CrossRef] [PubMed]
- Eser, A.; Ozkaya, E. Uterocervical angle: An ultrasound screening tool to predict satisfactory response to labor induction. J. Matern. Fetal Neonatal Med. 2020, 33, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Al-Adwy, A.M.; Sobh, S.M.; Belal, D.S.; Omran, E.F.; Hassan, A.; Saad, A.H.; Afifi, M.M.; Nada, A.M. Diagnostic accuracy of posterior cervical angle and cervical length in the prediction of successful induction of labor. Int. J. Gynaecol. Obstet. 2018, 141, 102–107. [Google Scholar] [CrossRef]
- Li, X.; Li, L.; Li, Y.; Fang, S.; Zhao, C.; Zhang, Y.; Yang, Z. Usefulness of Transperineal Virtual Touch Quantification in the Cervix for Predicting Outcome of Labor Induction. Ultrasound Med. Biol. 2020, 46, 2207–2214. [Google Scholar] [CrossRef]
- Mlodawski, J.; Mlodawska, M.; Plusajska, J.; Detka, K.; Michalska, A.; Swiercz, G.; Sikorski, M. Repeatability and reproducibility of quantitative cervical strain elastography (E-Cervix) in pregnancy. Sci. Rep. 2021, 11, 23689. [Google Scholar] [CrossRef]
- Medison; R&D Samsung; E-Cervix™. A Tool for Measuring the Stiffness of Cervix using Elastographic Images. Available online: https://www.samsungmedison.com (accessed on 8 May 2020).
- Rizzo, G.; Pietrolucci, M.E.; Mappa, I.; Bitsadze, V.; Khizroeva, J.; Makatsariya, A.; D’Antonio, F. Sonoelastographic Assessment of the Uterine Cervix in the Prediction of Imminent Delivery in Singleton Nulliparous Women Near Term: A Prospective Cohort Study. J. Ultrasound Med. 2021, 40, 559–568. [Google Scholar] [CrossRef]
- Zhou, Y.; Jin, N.; Chen, Q.; Lv, M.; Jiang, Y.; Chen, Y.; Xi, F.; Yang, M.; Zhao, B.; Huang, H.; et al. Predictive value of cervical length by ultrasound and cervical strain elastography in labor induction at term. J. Int. Med. Res. 2021, 49, 300060520985338. [Google Scholar] [CrossRef] [PubMed]
- Seol, H.-J.; Sung, J.-H.; Seong, W.J.; Kim, H.M.; Park, H.S.; Kwon, H.; Hwang, H.S.; Jung, Y.J.; Kwon, J.-Y.; Oh, S.-Y. Standardization of measurement of cervical elastography, its reproducibility, and analysis of baseline clinical factors affecting elastographic parameters. Obstet. Gynecol. Sci. 2020, 63, 42–54. [Google Scholar] [CrossRef] [PubMed]
- To, M.S.; Skentou, C.; Chan, C.; Zagaliki, A.; Nicolaides, K.H. Cervical assessment at the routine 23-week scan: Standardizing techniques. Ultrasound Obstet. Gynecol. 2001, 17, 217–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bujang, M.; Baharum, N. A simplified guide to determination of sample size requirements for estimating the value of intraclass correlation coefficient: A review. Arch. Orofac. Sci. 2017, 12, 1–11. [Google Scholar]
- Mlodawski, J.; Plusajska, J.; Mlodawska, M.; Swiercz, G. OP08.04: Is it possible to create ultrasonographic Bishop score? Repeatability and reproducibility of potential parameters–Preliminary study. Ultrasound Obstet. Gynecol. 2022, 60, 73–74. [Google Scholar] [CrossRef]
- Guilford, J.P. Fundamental Statistics in Psychology and Education; McGraw-Hill Medical: New York, NY, USA, 1973. [Google Scholar]
- Teixeira, C.; Lunet, N.; Rodrigues, T.; Barros, H. The Bishop Score as a determinant of labour induction success: A systematic review and meta-analysis. Arch. Gynecol. Obstet. 2012, 286, 739–753. [Google Scholar] [CrossRef]
- Jung, A.; Beckmann, M. Predicting the duration of induction of labour in nulliparous women. J. Obstet. Gynaecol. 2020, 40, 167–170. [Google Scholar] [CrossRef]
- Wu, Y.; Kataria, Y.; Wang, Z.; Ming, W.K.; Ellervik, C. Factors associated with successful vaginal birth after a cesarean section: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2019, 19, 360. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, R.D. Bishop Score as a Measurement Instrument [30H]. Obstet. Gynecol. 2019, 133, 92S. [Google Scholar] [CrossRef]
- McDonagh, M.; Skelly, A.C.; Tilden, E.; Brodt, E.D.; Dana, T.; Hart, E.; Kantner, S.N.; Fu, R.; Hermesch, A.C. Outpatient Cervical Ripening: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2021, 137, 1091–1101. [Google Scholar] [CrossRef]
- Ezebialu, I.U.; Eke, A.C.; Eleje, G.U.; Nwachukwu, C.E. Methods for assessing pre-induction cervical ripening. Cochrane Database Syst. Rev. 2015, 2015, CD010762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parrish, K.M.J.; D’Souza, R. Prediction models for determining the success of labor induction: A systematic review. Acta Obstet. Gynecol. Scand. 2019, 98, 1100–1112. [Google Scholar] [CrossRef]



| E-Cervix Parameter | Description |
|---|---|
| ECI (Elasticity Index) | A measure of tissue heterogeneity. This informs us of the average difference in color intensity between neighboring pixels of the elastogram. It adopts values from 0 to 81 (0—low heterogeneity, 81—high heterogeneity) |
| HR (Hardness Ratio) | The number of red pixels (defined as the top 30% of the color intensity scale) among all of the pixels in the ROI. This value is displayed as a percentage (0%—soft, 100%—hard) |
| IOS (Internal Os Strain) | Mean strain level of the internal cervical os ROI (0—hard, 1—soft) |
| EOS (External Os Strain) | Mean strain level of the external cervical os ROI (0—hard, 1—soft) |
| Ratio (IOS/EOS) | Ratio of internal and external cervical os mean strain |
| CL (Cervical Length) | Length of the cervical canal |
| Age (Years) [Mean, SD] | 29.57 (4.82) |
|---|---|
| Multipara [n, %] | 92 (36.5%) |
| Gestational age (weeks) [median, IQR] | 38 (4.74) |
| Weight (kg) [median, IQR] | 74 (12.51) |
| BMI (kg/m2) [median, IQR] | 26.75 (4.78) |
| Height (meters) [median, IQR] | 1.66 (0.06) |
| Intra-observer Variability | Inter-observer Variability | |||||
|---|---|---|---|---|---|---|
| Parameter | ICC | 95% CI | p | ICC | 95% CI | p |
| ECI | 0.917 | 0.883–0.941 | <0.001 | 0.907 | 0.864–0.936 | <0.001 |
| HR | 0.878 | 0.829–0.913 | <0.001 | 0.826 | 0.747–0.880 | <0.001 |
| IOS | 0.953 | 0.934–0.966 | <0.001 | 0.918 | 0.880–0.943 | <0.001 |
| EOS | 0.918 | 0.885–0.941 | <0.001 | 0.918 | 0.881–0.944 | <0.001 |
| IOS/EOS | 0.907 | 0.870–0.934 | <0.001 | 0.851 | 0.784–0.898 | <0.001 |
| CL | 0.993 | 0.990–0.995 | <0.001 | 0.993 | 0.990–0.995 | <0.001 |
| VCA | 0.988 | 0.983–0.991 | <0.001 | 0.987 | 0.980–0.991 | <0.001 |
| AoP | 0.983 | 0.977–0.988 | <0.001 | 0.967 | 0.952–0.978 | <0.001 |
| Dilatation | 0.994 | 0.992–0.996 | <0.001 | 0.996 | 0.995–0.997 | <0.001 |
| Bishop Parameter | ECI | IOS | EOS [Mean] | IOS/EOS | HR | CL | VCA | AoP | USG Dilatation |
|---|---|---|---|---|---|---|---|---|---|
| Dilatation | 0.09 | −0.09 | 0.11 | 0.07 | 0.11 | −0.31 * | −0.05 | 0.18 * | 0.71 * |
| Effacement | 0.16 * | −0.03 | 0.13 * | 0.04 | 0.02 | −0.75 * | 0.06 | 0.37 * | 0.35 * |
| Station | 0.13 * | 0.01 | 0.05 | 0.17 * | 0.08 | −0.44 * | 0.00 | 0.69 * | 0.16 * |
| Consistency | −0.08 | −0.05 | −0.22 * | 0.13 * | −0.33 * | −0.19 * | 0.01 | 0.10 | 0.08 |
| Position | 0.05 | 0.01 | 0.20 * | −0.13 * | 0.09 | −0.11 | −0.38 * | 0.09 | 0.09 |
| Sum | 0.12 | −0.04 | 0.09 | 0.09 | −0.03 | −0.61 * | −0.13 * | 0.52 * | 0.42 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mlodawski, J.; Mlodawska, M.; Plusajska, J.; Detka, K.; Bialek, K.; Swiercz, G. Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters. J. Clin. Med. 2023, 12, 4492. https://doi.org/10.3390/jcm12134492
Mlodawski J, Mlodawska M, Plusajska J, Detka K, Bialek K, Swiercz G. Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters. Journal of Clinical Medicine. 2023; 12(13):4492. https://doi.org/10.3390/jcm12134492
Chicago/Turabian StyleMlodawski, Jakub, Marta Mlodawska, Justyna Plusajska, Karolina Detka, Katarzyna Bialek, and Grzegorz Swiercz. 2023. "Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters" Journal of Clinical Medicine 12, no. 13: 4492. https://doi.org/10.3390/jcm12134492
APA StyleMlodawski, J., Mlodawska, M., Plusajska, J., Detka, K., Bialek, K., & Swiercz, G. (2023). Repeatability and Reproducibility of Potential Ultrasonographic Bishop Score Parameters. Journal of Clinical Medicine, 12(13), 4492. https://doi.org/10.3390/jcm12134492