
Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
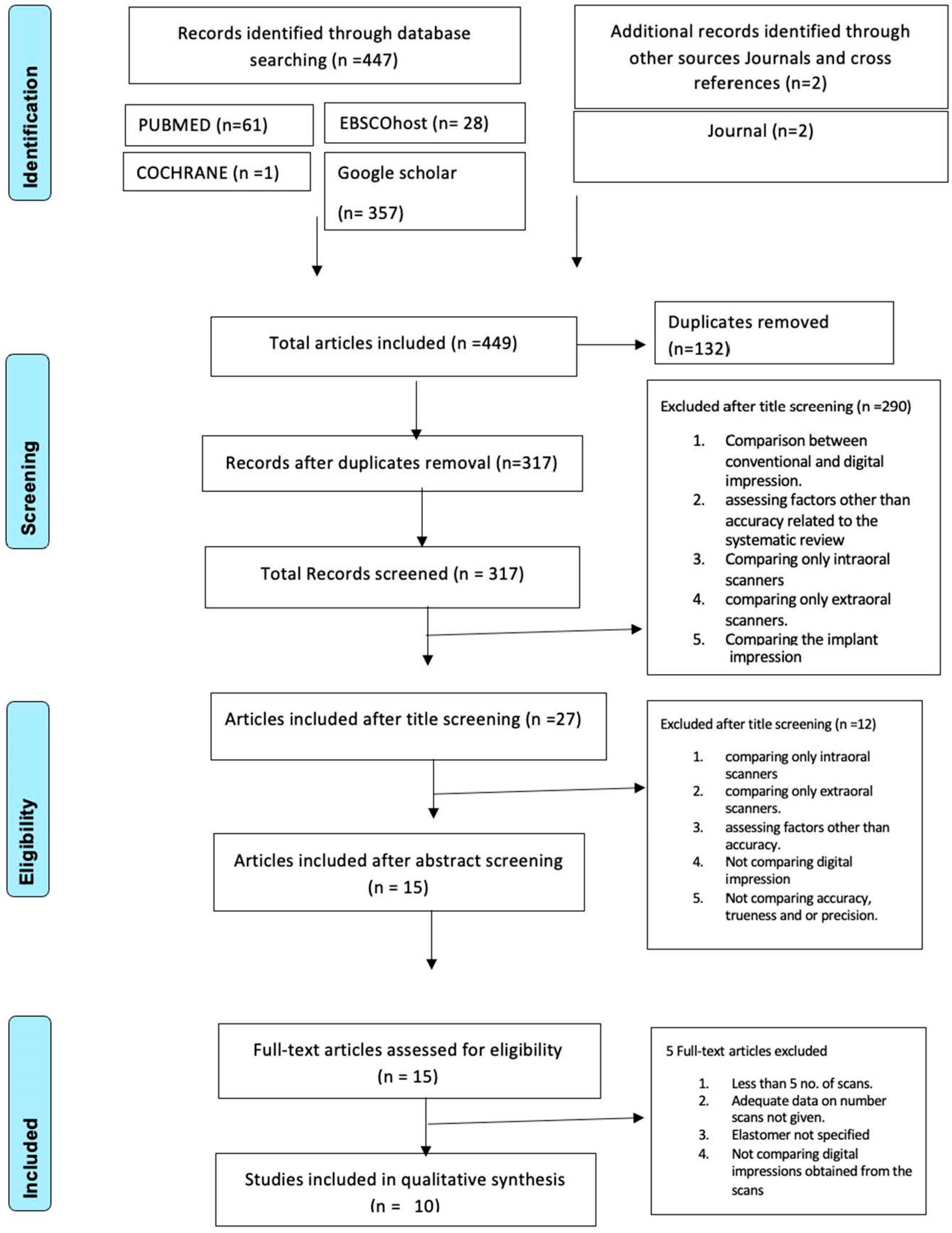
2.1. Research Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
3. Results
3.1. Studies and Quality Selection
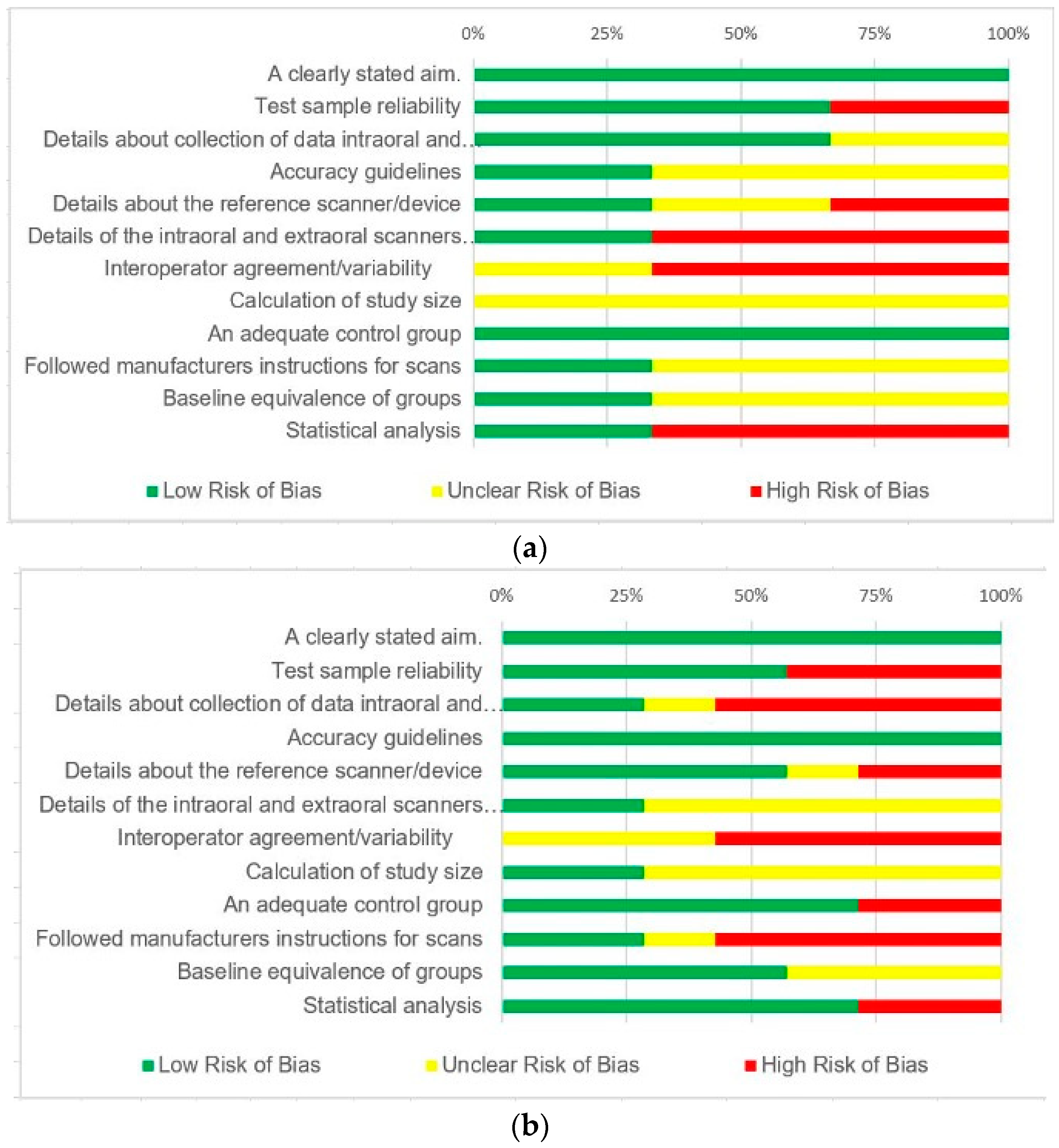
3.2. Risk of Bias
- Low risk of bias (bias unlikely to materially affect the outcomes);
- Unclear risk of bias (a bias that casts some doubt on the findings);
- High risk of bias (a bias that significantly reduces credibility regarding the findings in the paper).
4. Discussion
- Most of the studies have not individually specified the trueness and precision of scans but have instead combined the accuracy of scans.
- With an ongoing advancement in scanning technologies, it is difficult to have a standardized format to assess the scanners’ inaccuracies.
5. Conclusions
- The accuracy of digital impressions recorded using the digital scanners is affected by the scanning techniques.
- The intraoral scanner seems more accurate compared to extraoral scanners under partial arch scans. However, the accuracy shown by extraoral scanners is also within the clinically acceptable range.
- Studies comparing the accuracy of a scanner (intraoral and extraoral) in an in vivo setting are lacking for complete arch scans.
- Further studies with similar methodology (PICO question—Does the type of scanning (intraoral or extraoral) affect the accuracy of digital impression?) with strict inclusion criteria of clinical studies in all available electronic databases, specifically assessing the role and effect of clinical parameters during the use of digital scanners both intraoral and extraoral, are needed to validate the accuracy of digital scanners under clinical conditions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Lyu, P.; Wang, Y.; Sun, Y. Influence of object translucency on the scanning accuracy of a powder-free intraoral scanner: A laboratory study. J. Prosthet. Dent. 2017, 117, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Keul, C.; Güth, J.-F. Accuracy of full-arch digital impressions: An in vitro and in vivo comparison. Clin. Oral Investig. 2020, 24, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.-C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef]
- Güth, J.-F.; Edelhoff, D.; Schweiger, J.; Keul, C. A new method for the evaluation of the accuracy of full-arch digital impressions in vitro. Clin. Oral Investig. 2016, 20, 1487–1494. [Google Scholar] [CrossRef]
- Ender, A.; Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 2013, 109, 121–128. [Google Scholar] [CrossRef]
- Lin, Y.-M. Digitalisation in Dentistry: Development and Practices. The Digitization of Business in China; Springer International Publishing: Cham, Switzerland, 2018; pp. 199–217. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Khaled Addas, M.; Al Humaidi, A.S.A.; Al Qahtani, A.M.; Al Qahtani, M.D. A Novel Approach to Determine the Prevalence of Type of Soft Palate Using Digital Intraoral Impression. Int. J. Dent. 2017, 2017, 3268064. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Addas, M.K.; Alqahtani, N.M.; Al Ahmari, N.M.; Alfarsi, M.A. Clinical analysis of CAD-CAM milled and printed complete dentures using computerized occlusal force analyser. Technol. Health Care 2021, 29, 797–811. [Google Scholar] [CrossRef]
- Alsubaiy, E.F.; Chaturvedi, S.; Qutub, O.A.; Mously, H.A.; Zarbah, M.A.; Haralur, S.B.; Bhagat, T.V. Novel CAD-CAM zirconia coping design to enhance the aesthetics and strength for anterior PLZ crowns. Technol. Health Care 2021, 29, 1161–1171. [Google Scholar] [CrossRef]
- Abouzeid, H.L.; Chaturvedi, S.; Abdelaziz, K.M.; Alzahrani, F.A.; AlQarni, A.A.S.; Alqahtani, N.M. Role of Robotics and Artificial Intelligence in Oral Health and Preventive Dentistry—Knowledge, Perception and Attitude of Dentists. Oral Health Prev. Dent. 2021, 19, 353–363. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Addas, M.K.; Alqahtani, N.M.; Al Ahmari, N.M.; Alfarsi, M.A. Computerized occlusal forces analysis in complete dentures fabricated by additive and subtractive techniques. Technol. Health Care 2021, 29, 781–795. [Google Scholar] [CrossRef] [PubMed]
- Jedliński, M.; Mazur, M.; Grocholewicz, K.; Janiszewska-Olszowska, J. 3D Scanners in Orthodontics-Current Knowledge and Future Perspectives-A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1121. [Google Scholar] [CrossRef]
- Su, T.; Sun, J. Comparison of repeatability between intraoral digital scanner and extraoral digital scanner: An in-vitro study. J. Prosthodont. Res. 2015, 59, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Ender, A.; Mehl, A. Full arch scans: Conventional versus digital impressions--an in-vitro study. Int. J. Comput. Dent. 2011, 14, 11–21. [Google Scholar]
- Luthardt, R.G.; Loos, R.; Quaas, S. Accuracy of intraoral data acquisition in comparison to the conventional impression. Int. J. Comput. Dent. 2005, 8, 283–294. [Google Scholar] [PubMed]
- Mehl, A.; Ender, A.; Mörmann, W.; Attin, T. Accuracy testing of a new intraoral 3D camera. Int. J. Comput. Dent. 2009, 12, 11–28. [Google Scholar]
- Trifkovic, B.; Budak, I.; Todorovic, A.; Vukelic, D.; Lazic, V.; Puskar, T. Comparative analysis on measuring performances of dental intraoral and extraoral optical 3D digitization systems. Measurement 2014, 47, 45–53. [Google Scholar] [CrossRef]
- Ueda, K.; Beuer, F.; Stimmelmayr, M.; Erdelt, K.; Keul, C.; Güth, J.-F. Fit of 4-unit FDPs from CoCr and zirconia after conventional and digital impressions. Clin. Oral Investig. 2016, 20, 283–289. [Google Scholar] [CrossRef]
- Güth, J.-F.; Keul, C.; Stimmelmayr, M.; Beuer, F.; Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Investig. 2013, 17, 1201–1208. [Google Scholar] [CrossRef]
- ISO 12836:2012; Dentistry—Digitizing Devices for CAD-CAM Systems for Indirect Dental Restorations: Test Methods for Assessing Accuracy. International Organization for Standardization: Geneva, Switzerland, 2012.
- ISO 5725-1:1994; Accuracy (Trueness and Precision) of Measurement Methods And Results. Part 1. General Principles and Definitions. International Organization for Standardization: Geneva, Switzerland, 1994.
- Flügge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Giachetti, L.; Sarti, C.; Cinelli, F.; Russo, D.S. Accuracy of Digital Impressions in Fixed Prosthodontics: A Systematic Review of Clinical Studies. Int. J. Prosthodont. 2020, 33, 192–201. [Google Scholar] [CrossRef]
- Wesemann, C.; Kienbaum, H.; Thun, M.; Spies, B.C.; Beuer, F.; Bumann, A. Does ambient light affect the accuracy and scanning time of intraoral scans? J. Prosthet. Dent. 2021, 125, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Sason, G.K.; Mistry, G.; Tabassum, R.; Shetty, O. A comparative evaluation of intraoral and extraoral digital impressions: An in vivo study. J. Indian Prosthodont. Soc. 2018, 18, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Resende, C.C.D.; Barbosa, T.A.Q.; Moura, G.F.; do Nascimento Tavares, L.; Rizzante, F.A.P.; George, F.M.; Neves, F.D.D.; Mendonça, G. Influence of operator experience, scanner type, and scan size on 3D scans. J. Prosthet. Dent. 2021, 125, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Chochlidakis, K.M.; Papaspyridakos, P.; Geminiani, A.; Chen, C.-J.; Feng, I.J.; Ercoli, C. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 184–190.e12. [Google Scholar] [CrossRef]
- Ender, A.; Zimmermann, M.; Attin, T.; Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Investig. 2016, 20, 1495–1504. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, H.; Salmen, H.; Moldan, M.; Kuhn, K.; Sichwardt, V.; Wöstmann, B.; Luthardt, R.G. Accuracy of intraoral and extraoral digital data acquisition for dental restorations. J. Appl. Oral Sci. 2016, 24, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.M.D.C.; Pimenta, C.A.D.M.; Nobre, M.R.C. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Vecsei, B.; Joós-Kovács, G.; Borbély, J.; Hermann, P. Comparison of the accuracy of direct and indirect three-dimensional digitizing processes for CAD/CAM systems—An in vitro study. J. Prosthodont. Res. 2017, 61, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Güth, J.-F.; Runkel, C.; Beuer, F.; Stimmelmayr, M.; Edelhoff, D.; Keul, C. Accuracy of five intraoral scanners compared to indirect digitalization. Clin. Oral Investig. 2017, 21, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-J.; Jeong, I.-D.; Park, J.-Y.; Jeon, J.-H.; Kim, J.-H.; Kim, W.-C. Accuracy of single-abutment digital cast obtained using intraoral and cast scanners. J. Prosthet. Dent. 2017, 117, 253–259. [Google Scholar] [CrossRef]
- Muallah, J.; Wesemann, C.; Nowak, R.; Robben, J.; Mah, J.; Pospiech, P.; Bumann, A. Accuracy of full-arch scans using intraoral and extraoral scanners: An in vitro study using a new method of evaluation. Int. J. Comput. Dent. 2017, 20, 151–164. [Google Scholar] [PubMed]
- Bohner, L.O.L.; De Luca Canto, G.; Marció, B.S.; Laganá, D.C.; Sesma, N.; Tortamano Neto, P. Computer-aided analysis of digital dental impressions obtained from intraoral and extraoral scanners. J. Prosthet. Dent. 2017, 118, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Shinya, A.; Kuroda, S.; Gomi, H. The accuracy of the CAD system using intraoral and extraoral scanners for designing of fixed dental prostheses. Dent. Mater. J. 2017, 36, 402–407. [Google Scholar] [CrossRef]
- Wesemann, C.; Muallah, J.; Mah, J.; Bumann, A. Accuracy and efficiency of full-arch digitalization and 3D printing: A comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017, 48, 41–50. [Google Scholar] [CrossRef]
- Pagano, S.; Moretti, M.; Marsili, R.; Ricci, A.; Barraco, G.; Cianetti, S. Evaluation of the Accuracy of Four Digital Methods by Linear and Volumetric Analysis of Dental Impressions. Materials 2019, 12, 1958. [Google Scholar] [CrossRef]
- Tsirogiannis, P.; Reissmann, D.R.; Heydecke, G. Evaluation of the marginal fit of single-unit, complete-coverage ceramic restorations fabricated after digital and conventional impressions: A systematic review and meta-analysis. J. Prosthet. Dent. 2016, 116, 328–335.e2. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Brägger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implants Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implants Res. 2013, 24, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Yuzbasioglu, E.; Kurt, H.; Turunc, R.; Bilir, H. Comparison of digital and conventional impression techniques: Evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health 2014, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Hategan, S.I.; Ionel, T.F.; Goguta, L.; Gavrilovici, A.; Negrutiu, M.L.; Jivanescu, A. Powder and Powder-Free Intra-Oral Scanners: Digital Impression Accuracy. Prim. Dent. J. 2018, 7, 40–43. [Google Scholar] [CrossRef]
- Prudente, M.S.; Davi, L.R.; Nabbout, K.O.; Prado, C.J.; Pereira, L.M.; Zancopé, K.; Neves, F.D. Influence of scanner, powder application, and adjustments on CAD-CAM crown misfit. J. Prosthet. Dent. 2018, 119, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Hong-Seok, P.; Chintal, S. Development of High Speed and High Accuracy 3D Dental Intra Oral Scanner. Procedia Eng. 2015, 100, 1174–1181. [Google Scholar] [CrossRef]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpelä, A.; Mäkynen, A. Recent advances in dental optics—Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- Jamjoom, F.Z.; Aldghim, A.; Aldibasi, O.; Yilmaz, B. Impact of intraoral scanner, scanning strategy, and scanned arch on the scan accuracy of edentulous arches: An in vitro study. J. Prosthet. Dent. 2023; in press. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Emmanouilidi, A.; Stampf, S.; Strub, J.R.; Att, W. Accuracy of full-arch scans using intraoral scanners. Clin. Oral Investig. 2014, 18, 1687–1694. [Google Scholar] [CrossRef]
- Patzelt, S.B.M.; Vonau, S.; Stampf, S.; Att, W. Assessing the feasibility and accuracy of digitizing edentulous jaws. J. Am. Dent. Assoc. 2013, 144, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Hauschild, U.; Veronesi, G.; Imburgia, M.; Mangano, C.; Admakin, O. Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: A comparative in vitro study. BMC Oral Health 2019, 19, 101. [Google Scholar] [CrossRef] [PubMed]
- Piedra-Cascón, W.; Methani, M.M.; Quesada-Olmo, N.; Jiménez-Martínez, M.J.; Revilla-León, M. Scanning accuracy of nondental structured light extraoral scanners compared with that of a dental-specific scanner. J. Prosthet. Dent. 2021, 126, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Spagopoulos, D.; Kaisarlis, G.; Spagopoulou, F.; Halazonetis, D.J.; Güth, J.-F.; Papazoglou, E. In Vitro Trueness and Precision of Intraoral Scanners in a Four-Implant Complete-Arch Model. Dent. J. 2023, 11, 27. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| POPULATION | (((((Dental Impression Technique [MeSH Terms]) OR (Dental Impression Technique * [Tiab])) OR (Optical digital impression * [Tiab])) OR (Dental digital impression * [Tiab])) OR (Digital Impression * [Tiab])) OR (Virtual impression * [Tiab]) |
| INTERVENTION | ((((((((((((Intraoral scanner * [Tiab]) OR (Intraoral scanning * [Tiab])) OR (Intraoral scanning system * [Tiab])) OR (Intraoral digital scanner * [Tiab])) OR (Direct digital impression * [Tiab])) OR (Intraoral digital impression * [Tiab])) OR (Intraoral digitization * [Tiab])) OR (direct intraoral digitization * [Tiab])) OR (Intraoral acquisition * [Tiab])) OR (Direct digital scan * [Tiab])) OR (Optical scanner * [Tiab])) OR (Dental laser scanner * [Tiab])) OR (Dental light scanner * [Tiab]) |
| COMPARISION | (((((((((((Extraoral scanner * [Tiab]) OR (Extraoral scanning * [Tiab])) OR (Extraoral scanning system * [Tiab])) OR (Indirect digital impression * [Tiab])) OR (Extraoral digital impression * [Tiab])) OR (Extraoral digitization * [Tiab])) OR (extraoral digital scanner * [Tiab])) OR (Extraoral acquisition * [Tiab])) OR (Indirect digital scan * [Tiab])) OR (Optical scanner * [Tiab])) OR (Dental laser scanner * [Tiab])) OR (Dental light scanner * [Tiab]) |
| OUTCOME | ((((((((((Dimensional Measurement Accuracy[MeSH Terms]) OR (Dimensional Measurement Accuracy * [Tiab])) OR (Data Accuracy[MeSH Terms])) OR (Data Accuracy * [Tiab])) OR (Accuracy * [Tiab])) OR (accuracies * [Tiab])) OR (Trueness * [Tiab])) OR (Exactness * [Tiab])) OR (Correctness * [Tiab])) OR (Precision * [Tiab])) OR (Repeatability * [Tiab]) |
| Study ID | Author | Title | Reason for Exclusion |
|---|---|---|---|
| 1 | Su et al. [14] | Comparison of the repeatability between intraoral digital scanner and extraoral digital scanner: an in vitro study | The material used for the extraoral scan was not mentioned. |
| 2 | Rudolph et al. [30] | Accuracy of intraoral and extraoral digital data acquisition for dental restorations | An inadequate number of Intraoral Scans. |
| 3 | Shimizu et al. [40] | The Accuracy of the CAD system using intraoral and extraoral scanners for designing of fixed dental prostheses | Number of Scans not mentioned. |
| 4 | Wesemann et al. [41] | Accuracy and efficiency of full arch digitalization and 3D printing: A comparison between desktop model scanner, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing | Comparison of digital impressions not available. |
| 5 | Pagano et al. [42] | Evaluation of the Accuracy of Four Digital Methods by Linear and Volumetric Analysis of Dental Impressions | An inadequate number of scans. |
| Study Characteristics | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Standard Deviation | ||||||||||||||||||
| Number of scans | Intraoral scanner | Extraoral scanner | Intraoral scanner | Extraoral scanner | |||||||||||||||
| Id | Author | Year | Study Type | Intraoral scans | Extraoral scans | Impression material | Reference data | Test sample | method for comparing accuracy | Evaluated | Trueness | Precision | Trueness | Precision | Trueness | Precision | Trueness | Precision | |
| 1 | Flügge TV et al. [23] | 2013 | in vivo | 20 | 20 | polyether | 1st scan | full arch | Precision | 50 (mean deviation) | 25 | ||||||||
| 20 | 10 | ||||||||||||||||||
| 2 | Sason at al. [26] | 2018 | in vivo | 30 | 30 | addition silicone | prepared tooth measured intraorally with digital vernier calliper | distance between the dimples on teeth | Trueness | Precision | MD: 477 BL: 349 | 20.7 to 33.35 | MD: 456 BL: 336 | 19.5 to 37 | MD: 576.4 BL: 655 | MD: 19.6 BL: 16.4 | MD: 743 BL: 626.5 | MD: 24 BL: 22.5 | |
| 3 | Keul C and Guth JF [3] | 2019 | in vivo | 12 | 24 | polyether | metal bar data set made using coordinate measuring instrument | metal bar | Trueness | Precision | Vectorial error: M-SCAN: 287.4 | Vectorial error: M-IMP: 318 M-CAST: 256 | Vectorial error: M-SCAN: 88.4 | Vectorial error: M-IMP: 150 M-CAST: 159 | |||||
| Angulation: M-SCAN: 0.46 | Angulation: M-IMP: 0.38 M-CAST: 0.42 | Angulation: M-SCAN: 0.11 | Angulation: M-IMP: 0.13 M-CAST: 0.36 | ||||||||||||||||
| 12 | 24 | Vectorial error: P-SCAN: 305.1 | P-IMP: 412.8 P-CAST: 517 | P-SCAN: 157.1 | P-IMP: 185.3 P-CAST: 627 | ||||||||||||||
| Angulation: P-SCAN: 0.40 | Angulation: P-IMP: 0.82 P-CAST: 0.91 | Angulation: P-SCAN: 0.14 | Angulation: P-IMP: 0.45 P-CAST: 1.27 | ||||||||||||||||
| 4 | Guth et al. [20] | 2013 | in vitro | 12 | 12 | polyether | A CAD/CAM-fabricated titanium model of prepared teeth scanned with industrial ct | prepared teeth on titanium model | Trueness | Precision | 1.5 | 3.6 | 5.2 | 1.9 | |||||
| 5 | Guth et al. [5] | 2015 | in vitro | 12 | 12 | polyether | metal bar attached to polymeric full arch model and measured with cmm | metal bar | Trueness | Precision | 8.9 | 7.7 | 4.8 | 3.6 | |||||
| 6 | Vecsei et al. [35] | 2016 | in vitro | 30 | 10 | polyvinyl siloxane | pmma maxillary cast scanned with ref scanner | prepared teeth on pmma master cast | Trueness | Precision | sd: 22.31 | sd: −40.26 | sd: 40 | sd: 79.67 | |||||
| md: 115.82 | md: 5.18 | md: 50.67 | md: 111.32 | ||||||||||||||||
| ld: −163.45 | ld: −325.81 | ld: 145.47 | ld: 134.13 | ||||||||||||||||
| 7 | Guth et al. [36] | 2016 | in vitro | 12 | 12 | polyether | A CAD/CAM-fabricated titanium model of prepared teeth scanned with industrial ct | prepared teeth on titanium model | Trueness | Precision | 1. CS 3500: 1.4 (1.4 to −1.3) | D-810 1.9 (2 to −1.8) | 1. CS 3500 1 (1 to 1) | 6. D-810: 6 (8 to 7) | |||||
| 12 | 2. Zfx Intrascan: 3.3 (3.7 to −2.9) | 2. Zfx Intrascan 1.6 (1.5 to 1.9) | |||||||||||||||||
| 12 | 3. CEREC Bluecam: 2.9 (3.1 to −2.3) | 3. CEREC Bluecam 3 (3 to 3) | |||||||||||||||||
| 12 | 4. CEREC Omnicam: 3.1 (3.0 to −3.2) | 4. CEREC Omnicam 3 (4 to 2) | |||||||||||||||||
| 12 | 5. True Definition: 1.1 (1.2 to −1.0) | 5. True Definition 2 (1 to 3) | |||||||||||||||||
| 8 | Lee et al. [43] | 2016 | in vitro | 6 | 6 | polyvinyl siloxane | pmma model scanned with enginner scanner | prepared teeth on pmma master cast | Trueness | Precision | Bluecam: 17.5 | Bluecam: 12.7 | CS1: 17.4 | CS1: 9.2 | Bluecam: 1.8 | Bluecam: 2.6 | CS1: 1.7 | CS1: 1.2 | |
| 6 | 6 | Omnicam: 13.8 | Omnicam: 12.5 | CS2: 12.3 | CS2: 6.9 | Omnicam: 1.4 | Omnicam: 3.7 | CS2: 0.1 | CS2: 2.6 | ||||||||||
| 9 | Muallah et al. [38] | 2017 | in vitro | 37∗6= | 37 | polyvinyl siloxane | A resin master model was created by 3D printing and mesured by coordinate measuring instrument | full arch | Trueness | Precision | IMD: 1. apollo di: 57.669 | IMD: OrthoXscan: 34.006 | |||||||
| 2. CS3500: 99.76 | |||||||||||||||||||
| 3. iTero: 84.137 | |||||||||||||||||||
| 4. Plan Scan: 214.756 | |||||||||||||||||||
| 5. Trios: 52.872 | |||||||||||||||||||
| 6. True Definition: 169.298 | |||||||||||||||||||
| ICW: 1. apollo di: 36.007 | ICW: 37.206 | ||||||||||||||||||
| 2. CS3500: 43.39 | |||||||||||||||||||
| 3. iTero: 22.008 | |||||||||||||||||||
| 4. Plan Scan: 80.761 | |||||||||||||||||||
| 5. Trios: 22.351 | |||||||||||||||||||
| 6. True Definition: 42.347 | |||||||||||||||||||
| AL: 1. apollo di: 64.859 | AL: 57.27 | ||||||||||||||||||
| 2. CS3500: 84.442 | |||||||||||||||||||
| 3. iTero: 30.673 | |||||||||||||||||||
| 4. Plan Scan: 91.89 | |||||||||||||||||||
| 5. Trios: 23.205 | |||||||||||||||||||
| 6. True Definition: 62.065 | |||||||||||||||||||
| 10 | Bohner et al. [39] | 2017 | in vitro | 10 | 10 | polyvinyl siloxane | typhodont with acrylic teeth scanned with industrial ct | prepared teeth | Trueness | Cervical Region: 32.8 | Cervical Region: 46.7 | Cervical Region: 21.4 | Cervical Region: 56.9 | ||||||
| Axial Surface: 14.1 | Axial Surface: 18.9 | Axial Surface: 5.3 | Axial Surface: 12.7 | ||||||||||||||||
| Occlusal Surface: 65 | Occlusal Surface: 71.7 | Occlusal Surface: 10.9 | Occlusal Surface: 10.3 | ||||||||||||||||
| 10 | 10 | Cervical Region: 34.4 | Cervical Region: 32.2 | Cervical Region: 16.7 | Cervical Region: 16.4 | ||||||||||||||
| Axial Surface: 25.6 | Axial Surface: 16.7 | Axial Surface: 17.4 | Axial Surface: 12.2 | ||||||||||||||||
| Occlusal Surface: 40.6 | Occlusal Surface: 77.8 | Occlusal Surface: 22.4 | Occlusal Surface: 88.6 | ||||||||||||||||
| Minors | Minors Tool Adapted as per Systematic Review | |
|---|---|---|
| 1 | A clearly stated aim | A clearly stated aim |
| 2 | Inclusion of consecutive patients | Test sample reliability |
| 3 | Prospective collection of data | Details about the collection of data intraoral and extraoral scans |
| 4 | Endpoints appropriate to the aim of the study | Accuracy guidelines considered |
| 5 | Unbiased assessment of the study endpoint | Details about the reference scanner/device |
| 6 | Follow up period appropriate to the aim of the study | Details of the intraoral and extraoral scanners |
| 7 | Loss to follow up less than 5% | Interoperator agreement/variability |
| 8 | Prospective calculation of the study size | Calculation of study size |
| 9 | An adequate control group | An adequate control group |
| 10 | Contemporary groups | Followed manufacturer’s instructions for scans |
| 11 | Baseline equivalence of groups | Baseline equivalence of groups |
| 12 | Adequate statistical analyses | Statistical analysis |
| Sr. No. | Minors Tool Adapted as per Systematic Review | Flügge, T.V. et al. (2013) [23] | Sason, G.K. et al. (2018) [26] | Keul, Güth, J.F. (2019) [3] | Güth, J.F. et al. (2013) [20] | Güth, J.F. et al. (2015) [5] | Vecsei, B. et al. (2016) [35] | Güth, J.F. et al. (2016) [36] | Lee, J.J. et al. (2016) [37] | Muallah, J. et al. (2017) [38] | Bohner et al. (2017) [39] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| In Vivo Studies | In Vitro Studies | ||||||||||
| 1 | A clearly stated aim. | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 2 | Test sample reliability | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 2 |
| 3 | Details about collection of data intraoral and extraoral scans. | 2 | 1 | 2 | 0 | 1 | 1 | 2 | 1 | 2 | 1 |
| 4 | Accuracy guidelines | 0 | 0 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 5 | Details about the reference scanner/device | 0 | 1 | 2 | 2 | 0 | 2 | 1 | 2 | 2 | 1 |
| 6 | Details of the intraoral and extraoral scanners mentioned | 1 | 1 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 2 |
| 7 | Interoperator agreement/variability | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 |
| 8 | Calculation of study size | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 2 |
| 9 | An adequate control group | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 |
| 10 | Followed manufacturers instructions for scans | 2 | 0 | 0 | 0 | 1 | 2 | 1 | 2 | 1 | 1 |
| 11 | Baseline equivalence of groups | 0 | 0 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 0 |
| 12 | Statistical analysis | 1 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 2 |
| Total Score (Out of 24): | 13 | 11 | 17 | 11 | 15 | 18 | 17 | 18 | 18 | 18 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shah, N.; Thakur, M.; Gill, S.; Shetty, O.; Alqahtani, N.M.; Al-Qarni, M.A.; Alqahtani, S.M.; Elagib, M.F.A.; Chaturvedi, S. Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review. J. Clin. Med. 2023, 12, 5833. https://doi.org/10.3390/jcm12185833
Shah N, Thakur M, Gill S, Shetty O, Alqahtani NM, Al-Qarni MA, Alqahtani SM, Elagib MFA, Chaturvedi S. Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review. Journal of Clinical Medicine. 2023; 12(18):5833. https://doi.org/10.3390/jcm12185833
Chicago/Turabian StyleShah, Naisargi, Mrinmyaee Thakur, Shruti Gill, Omkar Shetty, Nasser M. Alqahtani, Mohammed A. Al-Qarni, Saeed M. Alqahtani, Mohamed Fadul A. Elagib, and Saurabh Chaturvedi. 2023. "Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review" Journal of Clinical Medicine 12, no. 18: 5833. https://doi.org/10.3390/jcm12185833
APA StyleShah, N., Thakur, M., Gill, S., Shetty, O., Alqahtani, N. M., Al-Qarni, M. A., Alqahtani, S. M., Elagib, M. F. A., & Chaturvedi, S. (2023). Validation of Digital Impressions’ Accuracy Obtained Using Intraoral and Extraoral Scanners: A Systematic Review. Journal of Clinical Medicine, 12(18), 5833. https://doi.org/10.3390/jcm12185833