Abstract
Rebound-associated vertebral fractures (RVFx) following denosumab discontinuation are typically multiple, are commonly associated with acute sharp pain, increase the risk of imminent fractures, and are pathogenetically different from common osteoporotic vertebral fractures (VFx). A clinically relevant question is whether patients with RVFx should be managed differently from patients with osteoporotic VFx. To address this question, we performed a systematic search of the PubMed database, and we reviewed current evidence on the optimal management of patients with RVFx. For pain relief of patients with RVFx, potent analgesics, often opioids, are essential. Information on the effectiveness of braces in these patients is scarce. Vertebroplasty and kyphoplasty are strongly contraindicated as they confer a substantial risk for new VFx. Exercise may be helpful, but again evidence is lacking. In contrast to patients with osteoporotic VFx, in whom initial treatment with bone-forming agents is recommended, patients with RVFx should initiate treatment with potent antiresorptives. To summarize, patients who have sustained RVFx following denosumab discontinuation are at a very high risk for new fractures, especially VFx. The management of such patients requires a multidisciplinary approach that should not be restricted to pain relief and administration of antiosteoporotic medication, but should also include back protection, early mobilization, and appropriate exercise.
1. Introduction
Denosumab (Dmab), a fully human monoclonal antibody that binds with high specificity to the receptor activator of nuclear factor κB ligand (RANKL), reduces osteoclast number and activity, thereby decreasing bone resorption [1]. Given to women with postmenopausal osteoporosis once every 6 months via SC injection, Dmab treatment was associated with a low incidence of fractures, low rates of adverse events, and continued increases in BMD without plateau up to 10 years [2]. Because of its efficacy and favorable safety profile, Dmab is widely used in the treatment of patients with osteoporosis.
In 2016, three different groups of investigators almost simultaneously described five women who stopped Dmab treatment and sustained multiple vertebral fractures (VFx) 8–16 months after the last injection [3,4,5]. A year later, a review of 24 cases (13 published and 11 new) supported the association of Dmab discontinuation with the occurrence of clinical and primarily multiple VFx [6]. A rapid increase in bone turnover markers above the pretreatment levels following the arrest of Dmab treatment [7] was thought to be related to the pathogenesis of these fractures, and the term “Rebound-associated Vertebral Fractures” (RVFx) was coined to differentiate them from osteoporotic VFx [3]. Similar to osteoporotic VFx, RVFx are usually localized in the lower thoracic and lumbar spine [6].
The crude incidence of all VFx following discontinuation of placebo or Dmab treatment, as recently estimated via a post hoc analysis of the FREEDOM and FREEDOM Extension studies, was 9.5% and 11.8%, while that of multiple VFx (≥2) was 3.7% and 7.2%, respectively [8]. Moreover, the proportion of multiple VFx was higher after stopping Dmab (61%) compared to the proportion observed after stopping placebo (about 39%). Notably, the risk of multiple VFx after denosumab discontinuation increased with increased duration of treatment [8].
The mechanisms of continuous bone gain upon Dmab treatment and of rapid bone loss following its cessation are still incompletely understood [9]. Upregulation of osteoclastogenesis and osteoclast activity had been, however, reported to critically contribute to the increased vertebral fragility following Dmab discontinuation. Compared to treatment-naïve women with osteoporotic VFx, those who had sustained VFx 8–16 months after the last injection of Dmab had significantly higher blood levels of RANK (13-fold) and cathepsin K (2.6-fold) mRNA and decreased levels of microRNAs involved in osteoclastogenesis downregulation (miR-503 and miR-222-2) [10]. In addition, patients with RVFx had higher numbers of TRAP-positive osteoclasts in their iliac crest bone biopsies than either treatment-naïve patients or patients on Dmab treatment [11]. Thus, although patients with RVFx and those with osteoporotic VFx share common risk factors, such as prevalent VFx, which present a significant risk factor for new fractures, these VFx differ pathophysiologically. A clinically relevant question is, therefore, whether the management of patients with RVFx should be different from that of patients with osteoporotic VFx. To address this question, we collected data reported during the past 7 years, and we summarize herein current views on the management of individuals with RVFx and how this might differ from the management of individuals with osteoporotic VFx.
2. Methods
Literature Search
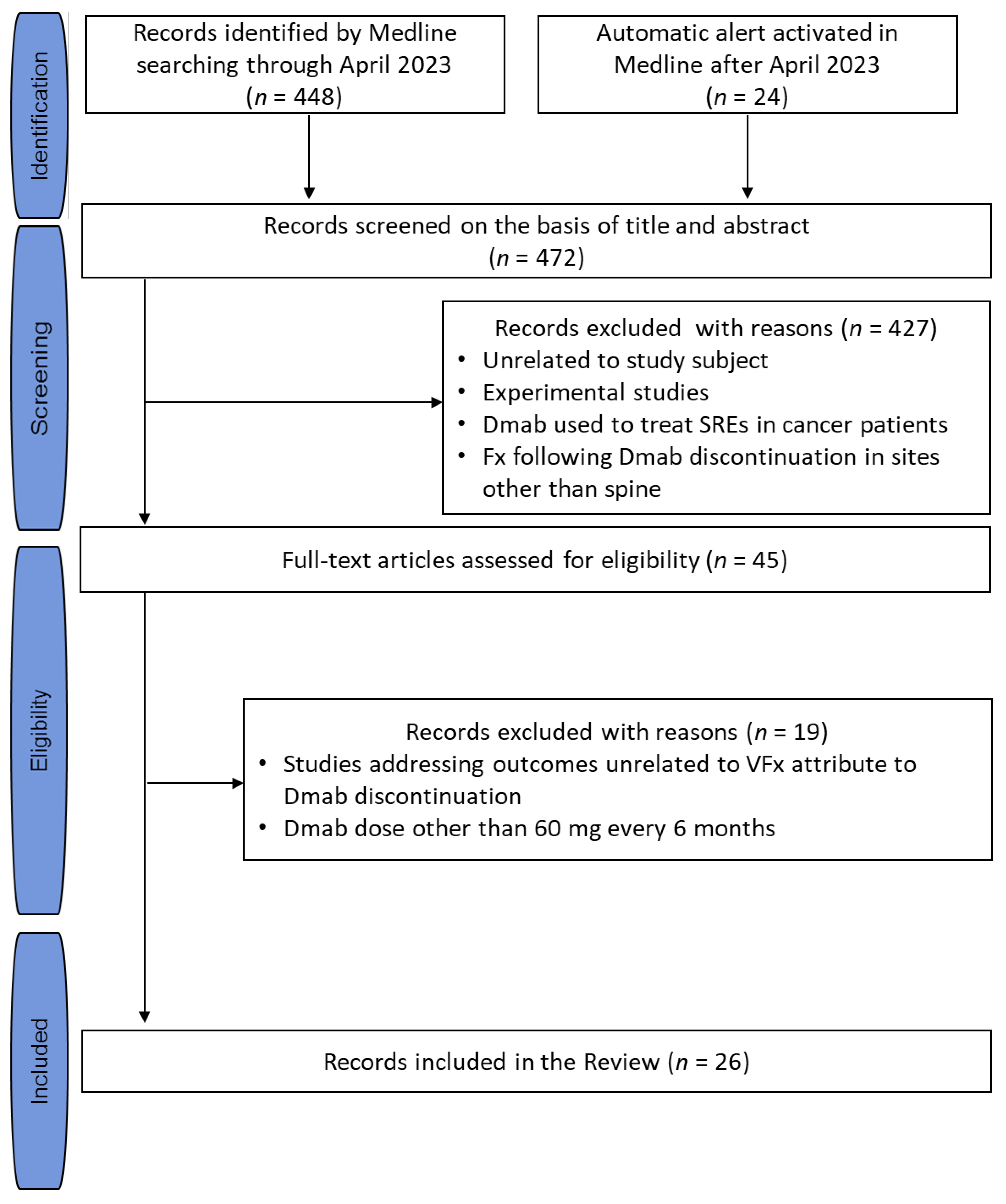
An unrestricted computerized literature search was performed using the PubMed database. Based on the Medical Subject Heading (MeSH) terms, the following query was set: (“Spinal Fractures” [Mesh] OR (rebound-associated vertebral fractures) OR (vertebral fractures)) AND (“Denosumab” [Mesh] OR denosumab OR (receptor activator of nuclear factor kappa-Β ligand inhibitor)) AND (“Osteoporosis” [Mesh] OR osteoporosis)”. This search initially provided 448 articles (5 April 2023). Subsequently, an automatic alert was activated in PubMed (“My NCBI”) to retrieve relevant articles published after the initial search, which provided another 24 articles (last update 20 July 2023). The literature search was extended by “hand searching” the “related citations” linking to the selected relevant articles (first 20 articles per included article, after sorting according to relevance) and the references of all the selected relevant articles, which, however, retrieved no additional articles. The search was not limited by publication time or language. As indicated by the search items, articles reporting vertebral fractures following discontinuation of a Dmab dose other than 60 mg once every 6 months, as used in osteoporosis, were not considered. The article selection process is depicted in a flowchart (Figure 1).
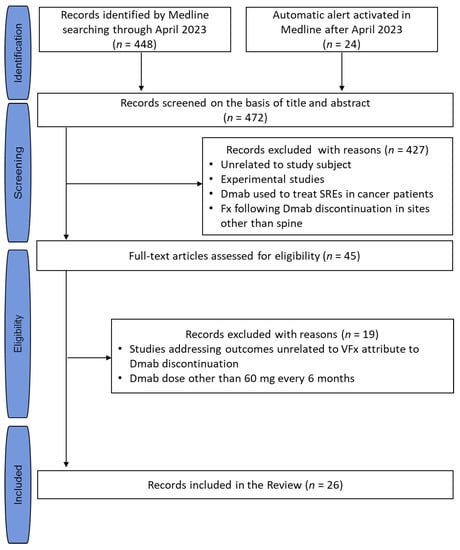
Figure 1.
Flowchart of the search strategy and article selection process. Abbreviations: Dmab, denosumab; SREs, skeletal-related events; VFx, vertebral fracture.
3. Diagnosis
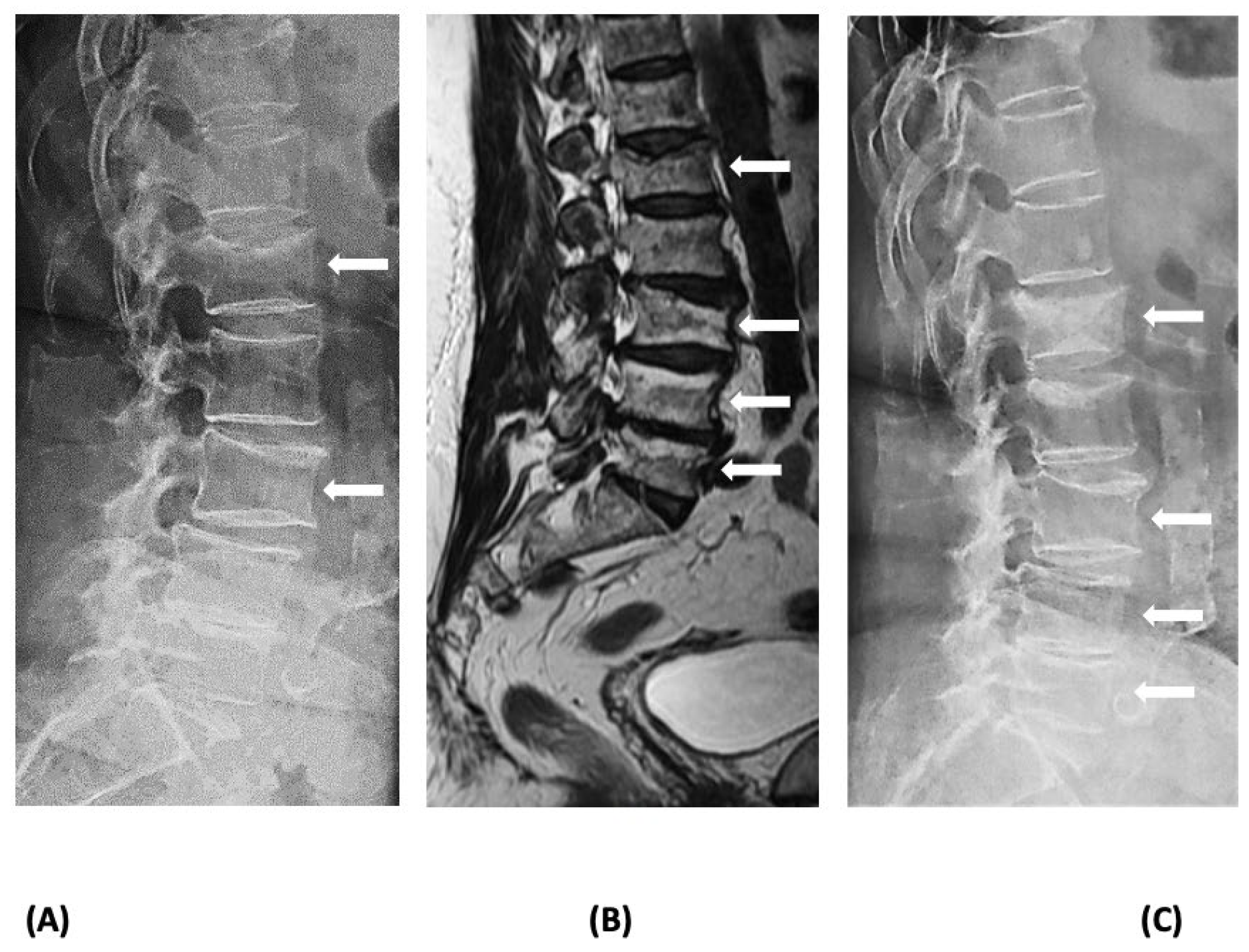
Vertebral compression fractures, which are the most common osteoporotic fractures, can cause significant back pain, limitation of activities, loss of independence, depression, chronic pain, and reduced quality of life, and increase the risk of imminent fractures and mortality [12,13]. While the most likely diagnosis in a patient presenting with a radiologically identifiable VFx 6 to 18 months after the last Dmab injection is RVFx, the recency of the fracture needs to be confirmed through an examination of earlier radiographs as back pain is a common symptom of elderly patients who may also have prevalent VFx [14,15,16]. If such radiographs are not available, recency can be verified using MRI, which can distinguish new from old VFx [17]. Severe back pain in a patient discontinuing or delaying Dmab treatment should always alert the physician of the possibility of RVFx, even if radiographs do not reveal spine deformities [17]. In such cases, described in the literature as acute non-collapsed VFx, a fracture may not be immediately identified but may be detected later in repeat radiographs; thus, MRI of the spine should be performed to confirm or exclude the diagnosis (Figure 2). In addition, other causes of VFx, e.g., malignancy, should be excluded. Establishing the diagnosis of RVFx may not be critical for the early management of patients, but it is essential for the longer-term therapeutic approach.
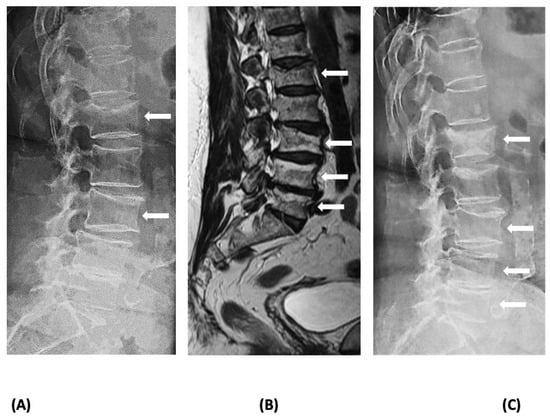
Figure 2.
Imaging of a patient with rebound-associated vertebral fractures 10 months after the last denosumab dose (4 months off treatment): (A) lateral lumbar spine X-ray at the time of acute back pain onset showing fractures at L1 and L3; (B) magnetic resonance imaging of the spine at the same time reveals additional recent fractures at L4 and L5; and (C) lateral lumbar spine X-ray 3 months later depicting deterioration of the deformities of the vertebrae (collapse of the acute, non-collapsed vertebral fractures). Fractures are indicated with white arrows.
4. Management
Following the establishment of a correct diagnosis, the management of patients with VFx consists of short- and longer-term measures that include both non-pharmacological and pharmacological interventions. Short-term measures aim mainly at alleviating the symptoms, while long-term measures additionally aim at prevention of new vertebral fractures as well as non-vertebral osteoporotic fractures.
4.1. Pain Relief
4.1.1. Pharmacological Interventions
Complaints of patients with osteoporotic VFx may vary considerably, ranging from lack of any pain (asymptomatic VFx) to sharp, breathtaking, and incapacitating pain [18]. In most cases, pain is tolerable and resolves without any treatment, and patients may recall a previous episode of pain when a VFx is incidentally identified on radiographs [19,20,21]. Acute pain usually subsides after 4–6 weeks but may persist for longer periods if the healing process is slower and can be replaced by chronic dull pain due to adjacent muscle spasms. Oral, nonopioid analgesics (acetaminophen, naproxen, and ibuprofen) are effective, especially in cases with mild to moderate pain [22]. Patients with severe pain will probably require oral or even parenteral opioids (tramadol, tapentadol, buplenorphine, hydrocodone, and oxycodone) [22]. Muscle relaxants may also reduce acute pain [23,24,25], although there is controversy regarding their ability to provide additional pain relief when they are combined with analgesics [26,27,28]. In contrast to osteoporotic VFx, RVFx are typically multiple and are commonly associated with acute [6], sharp pain that requires treatment with potent analgesics, often opioids [29]. In some cases, even opioids are ineffective in controlling the pain [30].
There are limited data about the use of antiosteoporotic agents in the management of acute pain of VFx. Intravenous pamidronate has been reported in controlled studies to provide greater pain relief compared to placebo [31] or calcitonin [32]. In a retrospective study, pain relief was achieved significantly earlier with denosumab than with alendronate [33]. Pain control was reported in two patients with RVFx treated with teriparatide [34] and denosumab [35], respectively. It should be emphasized that the use of teriparatide alone is contraindicated in patients who discontinue Dmab treatment [36] (see also Section 4.2).
4.1.2. Non-Pharmacological Interventions
Bracing
In VFx, disproportionate height loss from the anterior vertebral body is common and results in wedging, which compromises the mechanical capacity of the spine to support daily activities and increases the loads on the anterior of the other vertebrae, thus predisposing patients to new VFx [37,38]. Conservative management with pharmacological and non-pharmacological interventions reduces symptoms and improves muscle flexibility and strength, but it does not decrease the anterior vertebral loading [38,39]. The latter can be reduced with bracing, which ensures a more upright posture that may prevent deterioration of the fracture configuration. Bracing could be used to relieve pain both in the acute and subacute phases of a VFx, but it is not routinely used and is not indicated in patients with mild symptoms [40]. Wearing a brace is quite inconvenient for patients, and it is generally not recommended for long periods due to the anticipated atrophy of the trunk muscles because of inactivity and the restricted respiration that reduces compliance [41]. At present, new dynamic semirigid orthoses are preferred over conventional, rigid spinal orthoses [41].
The use of orthoses in individuals with RVFx is rarely reported. The fact that RVFx are often multiple significantly increases the risk of worsening spine biomechanics and strength, resulting in more severe thoracolumbar kyphosis which, together with the weakening of the intact vertebrae due to high bone turnover, predisposes patients to additional VFx [37]. In this setting, bracing applied during the initial phase may theoretically reduce the loads in the vertebrae, at least until the rebound of bone turnover is controlled.
Vertebroplasty/Kyphoplasty
The majority of patients with symptomatic VFx are treated conservatively [42]. However, some patients may still experience excruciating or persistent pain. In such cases, treatment by vertebroplasty or kyphoplasty has been proposed, but studies on the effectiveness and safety of these interventions have provided variable and sometimes conflicting results [43,44,45,46]. Common and clinically important adverse events, such as occurrence of new VFx in the adjacent vertebrae in the months following the procedure [47,48,49], and cement extravasation [50,51] with sometimes life-threatening consequences [52,53], have decreased the use of these procedures in the management of patients with osteoporotic VFx.
In patients with RVFx, vertebroplasty and kyphoplasty are strongly contraindicated, as an increased risk of additional, most often multiple, fractures of the adjacent vertebrae has been described in several case series and case reports [6,54,55,56,57]. It is hypothesized that in patients discontinuing Dmab, even the intact vertebrae are seriously weakened due to the highly accelerated bone turnover and are susceptible to fractures [6]. Thus, when these intact vertebrae are subjected to increased compressing forces by the neighboring cemented vertebrae, they can easily fracture.
Exercise
There is no information about the effects of exercise on patients with RVFx, and measures recommended for patients with osteoporotic VFx are advisable. Notably, exercise regimens have been reported to decrease the use of analgesics and improve quality of life in some, but not all, studies [39,58]. Complete and long bedrest should be avoided, and patients should resume physical activity as quickly as possible [59]. In patients with the so-called vertebral fracture cascade, i.e., an increased risk of subsequent VFx after an initial VFx [60], weight-bearing and muscle-strengthening exercises, with caution to avoid undue stress on the back, are advised [37]. Hyperextension exercises may relieve pain, reduce subsequent VFx risk, and prevent kyphosis, while flexion exercises may increase subsequent VFx risk [61]. Posterior pelvic tilt exercise may also be helpful. Patients must be instructed to safely perform daily activities and avoid flexion of the spine, which, as mentioned above, increases loading on the anterior part of the vertebrae and has been associated with increased risk of new VFx [61]. A safe exercise program that includes back extension exercises, weight-bearing activities, and muscle-strengthening exercises to improve balance and upright posture is recommended.
4.2. Antiosteoporotic Medication
The presence of a VFx, even if this is asymptomatic, has significant clinical implications and substantially increases the risk of new fractures independently of BMD measurement [62]. This applies to prevalent VFx, but even more so to recent VFx, which confer a multifold increase in the risk of new fractures, especially in the two subsequent years [63], necessitating a more aggressive therapeutic approach. These notions, along with the fact that all efficacious antiosteoporotic medications perform better in treatment-naïve patients [8], have led to a shift in our approach to the optimal management of high-risk patients. It is currently recommended to initiate the treatment of patients at a very high risk of fractures with a bone-forming agent, such as stimulators of PTH1R (teriparatide and abaloparatide) or inhibitors of sclerostin (romosozumab), followed by a potent antiresorptive agent, such as bisphosphonates or denosumab [64]. Individuals who have sustained RVFx have a very high risk of fractures and are prone to imminent new fractures. Therefore, prompt treatment initiation is strongly recommended to prevent occurrence of additional VFx or worsening of already existing VFx [65]. However, despite the usually more severe presentation of RVFx compared to that of osteoporotic VFx, the choice of therapeutics does not follow the treatment advice for the latter. This is due to the different pathogenesis of RVFx, which requires initial treatment with an agent that rapidly and effectively reduces increased bone turnover. This should be given about 6 months after the last Dmab injection before the occurrence of RVFx, according to expert recommendation [36].
Cohort studies and prospective clinical trials have examined the efficacy of antiresorptives, mainly bisphosphonates, in preventing bone loss that follows Dmab discontinuation [66,67,68,69,70,71,72,73,74,75]. In most of these studies, intravenous zoledronate was used with different results depending on patient- and Dmab treatment-related factors [66,67,68,69,71,72], for example, prevalent VFx and duration of Dmab treatment, respectively [8,76]. Further discussion of these studies lies outside the scope of this review. Furthermore, it is uncertain whether the findings of these studies are applicable to the small group of patients who have already sustained RVFx and are at an even higher risk for new fractures. Cases with subsequent VFx after treatment of RVFx with Dmab, zoledronate, or teriparatide have been reported [77,78,79]. Thus, treatment should be preferably offered before the development of RVFx. In a large cohort study, Burckhardt et al. demonstrated a marked protective effect of bisphosphonates on the risk of RVFx in women who discontinued Dmab [80], a result supporting the current recommendations to treat all patients following discontinuation of Dmab. These findings together with the rarity of these events suggest that prospective studies should focus on optimal prevention of RVFx.
Regarding the use of bone-forming agents which, as mentioned above, are currently the preferred treatment of patients with severe osteoporosis, teriparatide should not be given alone as an initial therapy to patients with RVFx [36] as it may accelerate the already increased rate of bone turnover and reduce BMD at cortical sites [81]. A combination of teriparatide with bisphosphonate or with Dmab has not been tested in patients with RVFx. The inhibitor of sclerostin, romosozumab, is theoretically a more rational approach as it increases bone formation while decreasing bone resorption [82]. Given to women after discontinuation of Dmab, romosozumab was shown to increase BMD [83], but a case with RVFx following three injections of romosozumab given 9 months after the last Dmab injection was reported [84].
5. Conclusions
Patients with RVFx after Dmab discontinuation have a very high risk for new fractures, especially VFx. Data about the effectiveness of pharmacological treatments for such patients are limited, and there is almost no information about other modes of treatment or conservative management. The current recommendations to treat all patients discontinuing Dmab, coupled with the rarity of RVFx, make the planning of prospective, randomized clinical trials nearly impossible. Instead, efforts should be directed at elucidating the mechanism(s) of increased vertebral fragility and identifying the optimal strategy to prevent fractures. In addition, evaluation and identification of the most appropriate non-pharmaceutical interventions are necessary. Given the severity of the condition, we believe that a multidisciplinary approach for optimal management is warranted. Such an approach should not be restricted to pain relief and administration of antiosteoporotic agents, but should also include back protection, early mobilization, and appropriate exercise while excluding surgical interventions, such as vertebroplasty.
Author Contributions
Conception of the hypothesis of the study: A.D.A. Design of the study: A.D.A. and S.E.P. Acquisition, analysis, and interpretation of data: A.D.A. and S.E.P. Drafting the manuscript: A.D.A. Revising the work critically for important intellectual content: P.M., S.A.P., J.P., I.B. and S.E.P. Final approval of the submitted version: A.D.A., P.M., S.A.P., J.P., I.B. and S.E.P. Agreement to be accountable for all aspects of the work: A.D.A., P.M., S.A.P., J.P., I.B. and S.E.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Athanasios D. Anastasilakis reports lecture fees from Amgen, Bianex, Eli-Lilly, Galenica, ITF, Unifarma, and UCB; Polyzois Makras reports fees for lectures/advisory boards and research grants from Amgen and fees for lectures/advisory boards from UCB, Elpen, and Galenica; Stergios A. Polyzos has nothing to declare; Socrates E. Papapoulos reports consulting/speaking fees from Amgen, Entera Bio, Qualix Dot, Radius Health, and UCB. Julien Paccou and Ilias Bisbinas have nothing to disclose.
References
- Bekker, P.J.; Holloway, D.L.; Rasmussen, A.S.; Murphy, R.; Martin, S.W.; Leese, P.T.; Holmes, G.B.; Dunstan, C.R.; DePaoli, A.M. A single-dose placebo-controlled study of AMG 162, a fully human monoclonal antibody to RANKL, in postmenopausal women. J. Bone Miner. Res. 2004, 19, 1059–1066. [Google Scholar] [CrossRef]
- Bone, H.G.; Wagman, R.B.; Brandi, M.L.; Brown, J.P.; Chapurlat, R.; Cummings, S.R.; Czerwinski, E.; Fahrleitner-Pammer, A.; Kendler, D.L.; Lippuner, K.; et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: Results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol. 2017, 5, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Popp, A.W.; Zysset, P.K.; Lippuner, K. Rebound-associated vertebral fractures after discontinuation of denosumab-from clinic and biomechanics. Osteoporos. Int. 2016, 27, 1917–1921. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Makras, P. Multiple clinical vertebral fractures following denosumab discontinuation. Osteoporos. Int. 2016, 27, 1929–1930. [Google Scholar] [CrossRef] [PubMed]
- Aubry-Rozier, B.; Gonzalez-Rodriguez, E.; Stoll, D.; Lamy, O. Severe spontaneous vertebral fractures after denosumab discontinuation: Three case reports. Osteoporos. Int. 2016, 27, 1923–1925. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Polyzos, S.A.; Makras, P.; Aubry-Rozier, B.; Kaouri, S.; Lamy, O. Clinical Features of 24 Patients With Rebound-Associated Vertebral Fractures After Denosumab Discontinuation: Systematic Review and Additional Cases. J. Bone Miner. Res. 2017, 32, 1291–1296. [Google Scholar] [CrossRef]
- Bone, H.G.; Bolognese, M.A.; Yuen, C.K.; Kendler, D.L.; Miller, P.D.; Yang, Y.C.; Grazette, L.; San Martin, J.; Gallagher, J.C. Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. J. Clin. Endocrinol. Metab. 2011, 96, 972–980. [Google Scholar] [CrossRef]
- Cosman, F.; Huang, S.; McDermott, M.; Cummings, S.R. Multiple Vertebral Fractures After Denosumab Discontinuation: FREEDOM and FREEDOM Extension Trials Additional Post Hoc Analyses. J. Bone Miner. Res. 2022, 37, 2112–2120. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Langdahl, B. Mechanisms underlying the long-term and withdrawal effects of denosumab therapy on Bone. Nat. Rev. Rheumatol. 2023, 19, 307–317. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Yavropoulou, M.P.; Makras, P.; Sakellariou, G.T.; Papadopoulou, F.; Gerou, S.; Papapoulos, S.E. Increased osteoclastogenesis in patients with vertebral fractures following discontinuation of denosumab treatment. Eur. J. Endocrinol. 2017, 176, 677–683. [Google Scholar] [CrossRef]
- Jähn-Rickert, K.; Wölfel, E.M.; Jobke, B.; Riedel, C.; Hellmich, M.; Werner, M.; McDonald, M.M.; Busse, B. Elevated Bone Hardness Under Denosumab Treatment, With Persisting Lower Osteocyte Viability During Discontinuation. Front. Endocrinol. 2020, 11, 250. [Google Scholar] [CrossRef]
- Palacios, S.; Neyro, J.L.; Fernández de Cabo, S.; Chaves, J.; Rejas, J. Impact of osteoporosis and bone fracture on health-related quality of life in postmenopausal women. Climacteric 2014, 17, 60–70. [Google Scholar] [CrossRef]
- Kendler, D.L.; Bauer, D.C.; Davison, K.S.; Dian, L.; Hanley, D.A.; Harris, S.T.; McClung, M.R.; Miller, P.D.; Schousboe, J.T.; Yuen, C.K.; et al. Vertebral Fractures: Clinical Importance and Management. Am. J. Med. 2016, 129, 221.e1–221.e10. [Google Scholar] [CrossRef]
- Fink, H.A.; Litwack-Harrison, S.; Ensrud, K.E.; Shen, J.; Schousboe, J.T.; Cawthon, P.M.; Cauley, J.A.; Lane, N.E.; Taylor, B.C.; Barrett-Connor, E.; et al. Association of Incident, Clinically Undiagnosed Radiographic Vertebral Fractures With Follow-Up Back Pain Symptoms in Older Men: The Osteoporotic Fractures in Men (MrOS) Study. J. Bone Miner. Res. 2017, 32, 2263–2268. [Google Scholar] [CrossRef]
- Fink, H.A.; Milavetz, D.L.; Palermo, L.; Nevitt, M.C.; Cauley, J.A.; Genant, H.K.; Black, D.M.; Ensrud, K.E. What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J. Bone Miner. Res. 2005, 20, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, M.C.; Ettinger, B.; Black, D.M.; Stone, K.; Jamal, S.A.; Ensrud, K.; Segal, M.; Genant, H.K.; Cummings, S.R. The association of radiographically detected vertebral fractures with back pain and function: A prospective study. Ann. Intern. Med. 1998, 128, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Anastasilakis, A.D.; Evangelatos, G.; Makras, P.; Iliopoulos, A. Magnetic resonance imaging has an advantage over conventional spine X-rays in the evaluation of rebound-associated vertebral fractures following denosumab discontinuation. Endocrine 2020, 69, 516–518. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, A.; Watts, N.B.; Kendler, D.L.; Yuen, C.K.; Adachi, J.D.; Ferko, N. Diagnosis and management of vertebral fractures in elderly adults. Am. J. Med. 2002, 113, 220–228. [Google Scholar] [CrossRef]
- Vogt, T.M.; Ross, P.D.; Palermo, L.; Musliner, T.; Genant, H.K.; Black, D.; Thompson, D.E. Vertebral fracture prevalence among women screened for the Fracture Intervention Trial and a simple clinical tool to screen for undiagnosed vertebral fractures. Fracture Intervention Trial Research Group. Mayo Clin. Proc. 2000, 75, 888–896. [Google Scholar] [CrossRef]
- Adams, J.E. Opportunistic Identification of Vertebral Fractures. J. Clin. Densitom 2016, 19, 54–62. [Google Scholar] [CrossRef]
- Miller, P.D. Clinical Management of Vertebral Compression Fractures. J. Clin. Densitom 2016, 19, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Koester, M.C.; Spindler, K.P. Pharmacologic agents in fracture healing. Clin. Sports Med. 2006, 25, 63–73, viii. [Google Scholar] [CrossRef]
- Beebe, F.A.; Barkin, R.L.; Barkin, S. A clinical and pharmacologic review of skeletal muscle relaxants for musculoskeletal conditions. Am. J. Ther. 2005, 12, 151–171. [Google Scholar] [CrossRef]
- Cashin, A.G.; Folly, T.; Bagg, M.K.; Wewege, M.A.; Jones, M.D.; Ferraro, M.C.; Leake, H.B.; Rizzo, R.R.N.; Schabrun, S.M.; Gustin, S.M.; et al. Efficacy, acceptability, and safety of muscle relaxants for adults with non-specific low back pain: Systematic review and meta-analysis. BMJ 2021, 374, n1446. [Google Scholar] [CrossRef]
- van Tulder, M.W.; Touray, T.; Furlan, A.D.; Solway, S.; Bouter, L.M. Muscle relaxants for non-specific low back pain. Cochrane Database Syst. Rev. 2003, 2003, Cd004252. [Google Scholar] [CrossRef]
- Friedman, B.W.; Dym, A.A.; Davitt, M.; Holden, L.; Solorzano, C.; Esses, D.; Bijur, P.E.; Gallagher, E.J. Naproxen with Cyclobenzaprine, Oxycodone/Acetaminophen, or Placebo for Treating Acute Low Back Pain: A Randomized Clinical Trial. JAMA 2015, 314, 1572–1580. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.W.; Irizarry, E.; Solorzano, C.; Zias, E.; Pearlman, S.; Wollowitz, A.; Jones, M.P.; Shah, P.D.; Gallagher, E.J. A Randomized, Placebo-Controlled Trial of Ibuprofen Plus Metaxalone, Tizanidine, or Baclofen for Acute Low Back Pain. Ann. Emerg. Med. 2019, 74, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Pareek, A.; Chandurkar, N.; Chandanwale, A.S.; Ambade, R.; Gupta, A.; Bartakke, G. Aceclofenac-tizanidine in the treatment of acute low back pain: A double-blind, double-dummy, randomized, multicentric, comparative study against aceclofenac alone. Eur. Spine J. 2009, 18, 1836–1842. [Google Scholar] [CrossRef]
- Maugars, Y.; Guillot, P.; Glémarec, J.; Berthelot, J.M.; Le Goff, B.; Darrieutort-Laffite, C. Long-term follow up after denosumab treatment for osteoporosis—Rebound associated with hypercalcemia, parathyroid hyperplasia, severe bone mineral density loss, and multiple fractures: A case report. J. Med. Case Rep. 2020, 14, 130. [Google Scholar] [CrossRef]
- Yeung, M.; Ho, K.; Fornier, M.N.; Farooki, A. Vertebral Fractures after Denosumab Discontinuation in Breast Cancer Survivors: A Single Institution Experience. HSS J. 2021, 17, 185–191. [Google Scholar] [CrossRef]
- Armingeat, T.; Brondino, R.; Pham, T.; Legré, V.; Lafforgue, P. Intravenous pamidronate for pain relief in recent osteoporotic vertebral compression fracture: A randomized double-blind controlled study. Osteoporos. Int. 2006, 17, 1659–1665. [Google Scholar] [CrossRef] [PubMed]
- Laroche, M.; Cantogrel, S.; Jamard, B.; Constantin, A.; Zabraniecki, L.; Cantagrel, A.; Mazières, B. Comparison of the analgesic efficacy of pamidronate and synthetic human calcitonin in osteoporotic vertebral fractures: A double-blind controlled study. Clin. Rheumatol. 2006, 25, 683–686. [Google Scholar] [CrossRef] [PubMed]
- Tetsunaga, T.; Tetsunaga, T.; Nishida, K.; Tanaka, M.; Sugimoto, Y.; Takigawa, T.; Takei, Y.; Ozaki, T. Denosumab and alendronate treatment in patients with back pain due to fresh osteoporotic vertebral fractures. J. Orthop. Sci. 2017, 22, 230–236. [Google Scholar] [CrossRef]
- Mori, Y.; Izumiyama, T.; Mori, N.; Aizawa, T. The Effect of Teriparatide for the Treatment of Multiple Spontaneous Clinical Vertebral Fractures after Discontinuation of Denosumab in a Female Patient with Rheumatoid Arthritis: A Case Report. Tohoku J. Exp. Med. 2021, 254, 57–61. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Terpos, E. Clinical vertebral fractures following denosumab discontinuation. Endocrine 2016, 54, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Tsourdi, E.; Zillikens, M.C.; Meier, C.; Body, J.J.; Gonzalez Rodriguez, E.; Anastasilakis, A.D.; Abrahamsen, B.; McCloskey, E.; Hofbauer, L.C.; Guañabens, N.; et al. Fracture risk and management of discontinuation of denosumab therapy: A systematic review and position statement by ECTS. J. Clin. Endocrinol. Metab. 2020, 106, 264–281. [Google Scholar] [CrossRef]
- Broy, S.B. The Vertebral Fracture Cascade: Etiology and Clinical Implications. J. Clin. Densitom. 2016, 19, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.; Huysmans, S.M.D.; van Kuijk, S.M.J.; Evers, S.; Jutten, E.M.C.; Senden, R.; Paulus, A.T.G.; van den Bergh, J.P.W.; de Bie, R.A.; Merk, J.M.R.; et al. Effectiveness and cost-effectiveness of dynamic bracing versus standard care alone in patients suffering from osteoporotic vertebral compression fractures: Protocol for a multicentre, two-armed, parallel-group randomised controlled trial with 12 months of follow-up. BMJ Open 2022, 12, e054315. [Google Scholar] [CrossRef]
- Bolton, K.; Wallis, J.A.; Taylor, N.F. Benefits and harms of non-surgical and non-pharmacological management of osteoporotic vertebral fractures: A systematic review and meta-analysis. Braz. J. Phys. Ther. 2022, 26, 100383. [Google Scholar] [CrossRef]
- Wong, C.C.; McGirt, M.J. Vertebral compression fractures: A review of current management and multimodal therapy. J. Multidiscip. Healthc. 2013, 6, 205–214. [Google Scholar] [CrossRef]
- Meccariello, L.; Muzii, V.F.; Falzarano, G.; Medici, A.; Carta, S.; Fortina, M.; Ferrata, P. Dynamic corset versus three-point brace in the treatment of osteoporotic compression fractures of the thoracic and lumbar spine: A prospective, comparative study. Aging Clin. Exp. Res. 2017, 29, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.M.; Park, S.Y.; Lee, S.H.; Suh, S.W.; Hong, J.Y. Comparative analysis of clinical outcomes in patients with osteoporotic vertebral compression fractures (OVCFs): Conservative treatment versus balloon kyphoplasty. Spine J. 2012, 12, 998–1005. [Google Scholar] [CrossRef]
- Buchbinder, R.; Johnston, R.V.; Rischin, K.J.; Homik, J.; Jones, C.A.; Golmohammadi, K.; Kallmes, D.F. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Cochrane Database Syst. Rev. 2018, 4, Cd006349. [Google Scholar] [CrossRef]
- Ebeling, P.R.; Akesson, K.; Bauer, D.C.; Buchbinder, R.; Eastell, R.; Fink, H.A.; Giangregorio, L.; Guanabens, N.; Kado, D.; Kallmes, D.; et al. The Efficacy and Safety of Vertebral Augmentation: A Second ASBMR Task Force Report. J. Bone Miner. Res. 2019, 34, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Lou, S.; Shi, X.; Zhang, X.; Lyu, H.; Li, Z.; Wang, Y. Percutaneous vertebroplasty versus non-operative treatment for osteoporotic vertebral compression fractures: A meta-analysis of randomized controlled trials. Osteoporos. Int. 2019, 30, 2369–2380. [Google Scholar] [CrossRef] [PubMed]
- Halvachizadeh, S.; Stalder, A.L.; Bellut, D.; Hoppe, S.; Rossbach, P.; Cianfoni, A.; Schnake, K.J.; Mica, L.; Pfeifer, R.; Sprengel, K.; et al. Systematic Review and Meta-Analysis of 3 Treatment Arms for Vertebral Compression Fractures: A Comparison of Improvement in Pain, Adjacent-Level Fractures, and Quality of Life Between Vertebroplasty, Kyphoplasty, and Nonoperative Management. JBJS Rev. 2021, 9, e21. [Google Scholar] [CrossRef] [PubMed]
- Blasco, J.; Martinez-Ferrer, A.; Macho, J.; San Roman, L.; Pomés, J.; Carrasco, J.; Monegal, A.; Guañabens, N.; Peris, P. Effect of vertebroplasty on pain relief, quality of life, and the incidence of new vertebral fractures: A 12-month randomized follow-up, controlled trial. J. Bone Miner. Res. 2012, 27, 1159–1166. [Google Scholar] [CrossRef]
- Che, H.; Breuil, V.; Cortet, B.; Paccou, J.; Thomas, T.; Chapuis, L.; Debiais, F.; Mehsen-Cetre, N.; Javier, R.M.; Loiseau Peres, S.; et al. Vertebral fractures cascade: Potential causes and risk factors. Osteoporos. Int. 2019, 30, 555–563. [Google Scholar] [CrossRef]
- Mudano, A.S.; Bian, J.; Cope, J.U.; Curtis, J.R.; Gross, T.P.; Allison, J.J.; Kim, Y.; Briggs, D.; Melton, M.E.; Xi, J.; et al. Vertebroplasty and kyphoplasty are associated with an increased risk of secondary vertebral compression fractures: A population-based cohort study. Osteoporos. Int. 2009, 20, 819–826. [Google Scholar] [CrossRef]
- Saad, A.; Botchu, R.; James, S. The Rates of Cement Leakage Following Vertebroplasty in Osteoporotic versus Metastatic Disease. Indian J. Radiol. Imaging 2022, 32, 46–50. [Google Scholar] [CrossRef]
- Shapiro, S.; Abel, T.; Purvines, S. Surgical removal of epidural and intradural polymethylmethacrylate extravasation complicating percutaneous vertebroplasty for an osteoporotic lumbar compression fracture. Case report. J. Neurosurg. 2003, 98, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, J.; Heini, P.F.; Villiger, P.M. Asymptomatic diffuse pulmonary embolism caused by acrylic cement: An unusual complication of percutaneous vertebroplasty. Ann. Rheum. Dis. 2003, 62, 85–86. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lee, J.W.; Park, K.W.; Yeom, J.S.; Jeong, H.S.; Park, J.M.; Kang, H.S. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: Incidence, characteristics, and risk factors. Radiology 2009, 251, 250–259. [Google Scholar] [CrossRef]
- Dupont, J.; Laurent, M.R.; Dedeyne, L.; Luyten, F.P.; Gielen, E.; Dejaeger, M. Rebound-associated vertebral fractures after stopping denosumab: Report of four cases. Jt. Bone Spine 2020, 87, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Fernández Fernández, E.; Benavent Núñez, D.; Bonilla Hernán, G.; Monjo Henry, I.; García Carazo, S.; Bernad Pineda, M.; Balsa Criado, A.; Aguado Acín, P. Multiple vertebral fractures following discontinuation of denosumab treatment: Ten clinical cases report. Reumatol. Clin. Engl. Ed. 2020, 16, 480–484. [Google Scholar] [CrossRef]
- Gonzalez-Rodriguez, E.; Aubry-Rozier, B.; Stoll, D.; Zaman, K.; Lamy, O. Sixty spontaneous vertebral fractures after denosumab discontinuation in 15 women with early-stage breast cancer under aromatase inhibitors. Breast Cancer Res. Treat. 2020, 179, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Tripto-Shkolnik, L.; Rouach, V.; Marcus, Y.; Rotman-Pikielny, P.; Benbassat, C.; Vered, I. Vertebral Fractures Following Denosumab Discontinuation in Patients with Prolonged Exposure to Bisphosphonates. Calcif. Tissue Int. 2018, 103, 44–49. [Google Scholar] [CrossRef]
- Gibbs, J.C.; MacIntyre, N.J.; Ponzano, M.; Templeton, J.A.; Thabane, L.; Papaioannou, A.; Giangregorio, L.M. Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst. Rev. 2019, 7, Cd008618. [Google Scholar] [CrossRef]
- Ponzano, M.; Tibert, N.; Brien, S.; Funnell, L.; Gibbs, J.C.; Keller, H.; Laprade, J.; Morin, S.N.; Papaioannou, A.; Weston, Z.; et al. International consensus on the non-pharmacological and non-surgical management of osteoporotic vertebral fractures. Osteoporos. Int. 2023, 34, 1065–1074. [Google Scholar] [CrossRef]
- Briggs, A.M.; Greig, A.M.; Wark, J.D. The vertebral fracture cascade in osteoporosis: A review of aetiopathogenesis. Osteoporos. Int. 2007, 18, 575–584. [Google Scholar] [CrossRef]
- Sinaki, M.; Mikkelsen, B.A. Postmenopausal spinal osteoporosis: Flexion versus extension exercises. Arch. Phys. Med. Rehabil. 1984, 65, 593–596. [Google Scholar]
- Cauley, J.A.; Hochberg, M.C.; Lui, L.Y.; Palermo, L.; Ensrud, K.E.; Hillier, T.A.; Nevitt, M.C.; Cummings, S.R. Long-term risk of incident vertebral fractures. JAMA 2007, 298, 2761–2767. [Google Scholar] [CrossRef]
- Johansson, H.; Siggeirsdóttir, K.; Harvey, N.C.; Odén, A.; Gudnason, V.; McCloskey, E.; Sigurdsson, G.; Kanis, J.A. Imminent risk of fracture after fracture. Osteoporos. Int. 2017, 28, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Harvey, N.C.; McCloskey, E.; Bruyère, O.; Veronese, N.; Lorentzon, M.; Cooper, C.; Rizzoli, R.; Adib, G.; Al-Daghri, N.; et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos. Int. 2020, 31, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Anastasilakis, A.D.; Evangelatos, G.; Makras, P.; Iliopoulos, A. Rebound-associated vertebral fractures may occur in sequential time points following denosumab discontinuation: Need for prompt treatment re-initiation. Bone Rep. 2020, 12, 100267. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Papapoulos, S.E.; Polyzos, S.A.; Appelman-Dijkstra, N.M.; Makras, P. Zoledronate for the Prevention of Bone Loss in Women Discontinuing Denosumab Treatment. A Prospective 2-Year Clinical Trial. J. Bone Miner. Res. 2019, 34, 2220–2228. [Google Scholar] [CrossRef] [PubMed]
- Everts-Graber, J.; Reichenbach, S.; Gahl, B.; Häuselmann, H.; Ziswiler, H.R.; Studer, U.; Lehmann, T. Effects of zoledronate on bone mineral density and bone turnover after long-term denosumab therapy: Observations in a real-world setting. Bone 2022, 163, 116498. [Google Scholar] [CrossRef] [PubMed]
- Everts-Graber, J.; Reichenbach, S.; Gahl, B.; Ziswiler, H.R.; Studer, U.; Lehmann, T. Risk factors for vertebral fractures and bone loss after denosumab discontinuation: A real-world observational study. Bone 2021, 144, 115830. [Google Scholar] [CrossRef] [PubMed]
- Everts-Graber, J.; Reichenbach, S.; Ziswiler, H.R.; Studer, U.; Lehmann, T. A Single Infusion of Zoledronate in Postmenopausal Women Following Denosumab Discontinuation Results in Partial Conservation of Bone Mass Gains. J. Bone Miner. Res. 2020, 35, 1207–1215. [Google Scholar] [CrossRef]
- Kendler, D.; Chines, A.; Clark, P.; Ebeling, P.R.; McClung, M.; Rhee, Y.; Huang, S.; Stad, R.K. Bone Mineral Density After Transitioning From Denosumab to Alendronate. J. Clin. Endocrinol. Metab. 2020, 105, e255–e264. [Google Scholar] [CrossRef]
- Sølling, A.S.; Harsløf, T.; Brockstedt, H.K.; Langdahl, B. Discontinuation of denosumab in men with prostate cancer. Osteoporos. Int. 2023, 34, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Sølling, A.S.; Harsløf, T.; Langdahl, B. Treatment with Zoledronate Subsequent to Denosumab in Osteoporosis: A 2-Year Randomized Study. J. Bone Miner. Res. 2021, 36, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Laroche, M.; Couture, G.; Ruyssen-Witrand, A.; Constantin, A.; Degboé, Y. Effect of risedronate on bone loss at discontinuation of denosumab. Bone Rep. 2020, 13, 100290. [Google Scholar] [CrossRef]
- Tutaworn, T.; Nieves, J.W.; Wang, Z.; Levin, J.E.; Yoo, J.E.; Lane, J.M. Bone loss after denosumab discontinuation is prevented by alendronate and zoledronic acid but not risedronate: A retrospective study. Osteoporos. Int. 2023, 34, 573–584. [Google Scholar] [CrossRef]
- Ha, J.; Kim, J.; Jeong, C.; Lim, Y.; Kim, M.K.; Kwon, H.S.; Song, K.H.; Kang, M.I.; Baek, K.H. Effect of follow-up raloxifene therapy after denosumab discontinuation in postmenopausal women. Osteoporos. Int. 2022, 33, 1591–1599. [Google Scholar] [CrossRef] [PubMed]
- Makras, P.; Appelman-Dijkstra, N.M.; Papapoulos, S.E.; van Wissen, S.; Winter, E.M.; Polyzos, S.A.; Yavropoulou, M.P.; Anastasilakis, A.D. The Duration of Denosumab Treatment and the Efficacy of Zoledronate to Preserve Bone Mineral Density After Its Discontinuation. J. Clin. Endocrinol. Metab. 2021, 106, e4155–e4162. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Polyzos, S.A.; Makras, P.; Trovas, G.; Yavropoulou, M.P.; Tournis, S. Efficacy of Antiosteoporotic Medications in Patients With Rebound-Associated Fractures after Denosumab Discontinuation. J. Clin. Densitom. 2021, 24, 591–596. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Trovas, G.; Balanika, A.; Polyzos, S.A.; Makras, P.; Tournis, S. Progression of Rebound-Associated Vertebral Fractures Following Denosumab Discontinuation Despite Reinstitution of Treatment: Suppressing Increased Bone Turnover May Not Be Enough. J. Clin. Densitom. 2021, 24, 338–340. [Google Scholar] [CrossRef]
- Niimi, R.; Kono, T.; Nishihara, A.; Hasegawa, M.; Kono, T.; Sudo, A. Second rebound-associated vertebral fractures after denosumab discontinuation. Arch. Osteoporos. 2020, 15, 7. [Google Scholar] [CrossRef]
- Burckhardt, P.; Faouzi, M.; Buclin, T.; Lamy, O. Fractures after Denosumab Discontinuation: A Retrospective Study of 797 Cases. J. Bone Miner. Res. 2021, 36, 1717–1728. [Google Scholar] [CrossRef]
- Leder, B.Z.; Tsai, J.N.; Uihlein, A.V.; Wallace, P.M.; Lee, H.; Neer, R.M.; Burnett-Bowie, S.A. Denosumab and teriparatide transitions in postmenopausal osteoporosis (the DATA-Switch study): Extension of a randomised controlled trial. Lancet 2015, 386, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Cosman, F.; Crittenden, D.B.; Adachi, J.D.; Binkley, N.; Czerwinski, E.; Ferrari, S.; Hofbauer, L.C.; Lau, E.; Lewiecki, E.M.; Miyauchi, A.; et al. Romosozumab Treatment in Postmenopausal Women with Osteoporosis. N. Engl. J. Med. 2016, 375, 1532–1543. [Google Scholar] [CrossRef] [PubMed]
- McClung, M.R.; Bolognese, M.A.; Brown, J.P.; Reginster, J.Y.; Langdahl, B.L.; Shi, Y.; Timoshanko, J.; Libanati, C.; Chines, A.; Oates, M.K. Skeletal responses to romosozumab after 12 months of denosumab. JBMR Plus 2021, 5, e10512. [Google Scholar] [CrossRef] [PubMed]
- Kashii, M.; Ebina, K.; Kitaguchi, K.; Yoshikawa, H. Romosozumab was not effective in preventing multiple spontaneous clinical vertebral fractures after denosumab discontinuation: A case report. Bone Rep. 2020, 13, 100288. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).