
Patient Safety during Propofol Sedation before and after Implementation of Capnography Monitoring

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Service Evaluation
2.2. Data Collection
2.3. Collected Parameters
2.4. Additional Data
2.5. Primary Outcome
2.6. Data Analysis
3. Results
3.1. Population Statistics
3.2. Adverse Events
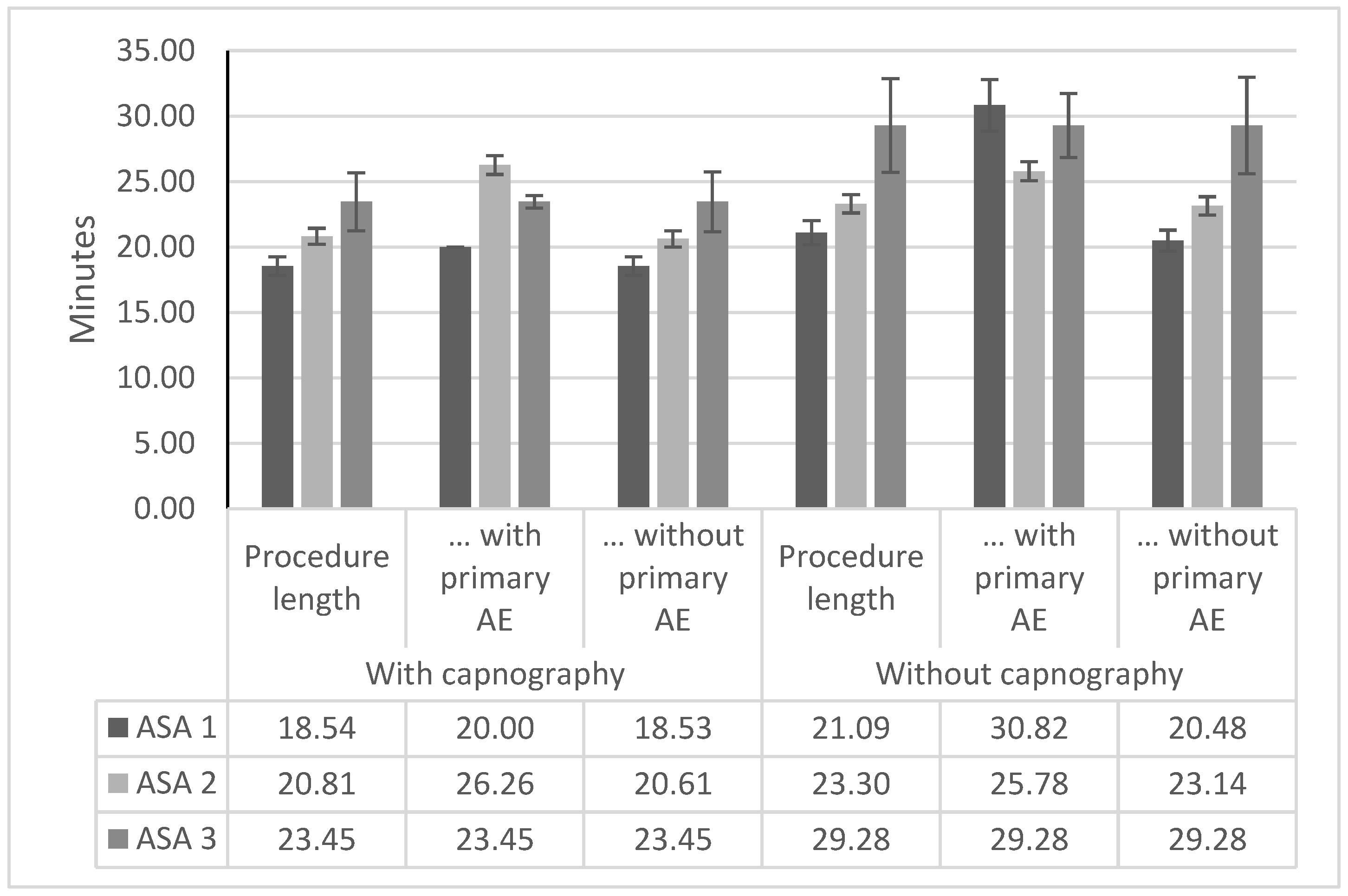
3.3. Procedure Duration
3.4. Interventions
4. Discussion
5. Conclusions
6. Limitations
7. Disclosures
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Koc, H.O.; Sari, Y.S.; Bektas, H.; Tunali, V.; Sahin, O.; Ozakay, K.; Feyzullah, E. Do we adequately diagnose early gastric cancer in Turkey. Turk. J. Gastroenterol. 2011, 22, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Tierney, M.; Bevan, R.; Rees, C.J.; Trebble, T.M. What do patients want from their endoscopy experience? The importance of measuring and understanding patient attitudes to their care. Frontline Gastroenterol. 2016, 7, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Hinkelbein, J.; Lamperti, M.; Akeson, J.; Santos, J.; Costa, J.; De Robertis, E.; Longrois, D.; Novak-Jankovic, V.; Petrini, F.; Struys, M.M.; et al. European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults. Eur. J. Anaesthesiol. 2018, 35, 6–24. [Google Scholar] [CrossRef] [PubMed]
- İnal, F.Y.; Daşkaya, H.; Yılmaz, Y.; Kayar, Y. Attitudes and Behaviors of Gastroenterology Specialists Toward Sedation Practices in Endoscopy Units in Turkey: Is Anesthesia Mandatory? İstanb. Med. J. 2022, 23, 20–28. [Google Scholar]
- Dossa, F.; Dube, C.; Tinmouth, J.; Sorvari, A.; Rabeneck, L.; McCurdy, B.R.; Dominitz, J.A.; Baxter, N.N. Practice recommendations for the use of sedation in routine hospital-based colonoscopy. BMJ Open Gastroenterol. 2020, 7, e000348. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Anaesthesists. Chapter 7: Guidelines for the Provision of Anaesthesia Services in the Non-Theatre Environment; Royal College of Anaesthesists: London, UK, 2021. [Google Scholar]
- Acedemy of Medical Royal Colleges. Safe Sedation Practice for Healthcare; Acedemy of Medical Royal Colleges: London, UK, 2021. [Google Scholar]
- ASGE Standards of Practice Committee; Early, D.S.; Lightdale, J.R.; Vargo, J.J., 2nd; Acosta, R.D.; Chandrasekhara, V.; Chathadi, K.V.; Evans, J.A.; Fisher, D.A.; Fonkalsrud, L.; et al. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest. Endosc. 2018, 87, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Poluha, W.; Cheung, M.; Choptain, N.; Baron, K.I.; Taback, S.P. Propofol for sedation during colonoscopy. Cochrane Database Syst. Rev. 2008, 2008, CD006268. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Xu, H.; Li, H.T. Safety and efficacy of propofol alone or in combination with other agents for sedation of patients undergoing colonoscopy: An updated meta-analysis. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4506–4518. [Google Scholar] [PubMed]
- Dossa, F.; Medeiros, B.; Keng, C.; Acuna, S.A.; Baxter, N.N. Propofol versus midazolam with or without short-acting opioids for sedation in colonoscopy: A systematic review and meta-analysis of safety, satisfaction, and efficiency outcomes. Gastrointest. Endosc. 2020, 91, 1015–1026.e7. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.; Struys, M.; Pollock, R.F.; Mestek, M.; Lightdale, J.R. Patient safety during procedural sedation using capnography monitoring: A systematic review and meta-analysis. BMJ Open 2017, 7, e013402. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.P.; Green, S.M.; Piacevoli, Q.; International Sedation Task, F. Adverse event reporting tool to standardize the reporting and tracking of adverse events during procedural sedation: A consensus document from the World SIVA International Sedation Task Force. Br. J Anaesth. 2012, 108, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Team, R. RStudio: Integrated Development Environment for R RStudio; RStudio: Boston, MA, USA, 2021. [Google Scholar]
- Gurbulak, B.; Uzman, S.; Kabul Gurbulak, E.; Gul, Y.G.; Toptas, M.; Baltali, S.; Savas, O.A. Cardiopulmonary safety of propofol versus midazolam/meperidine sedation for colonoscopy: A prospective, randomized, double-blinded study. Iran Red Crescent Med. J. 2014, 16, e19329. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Uzman, S.; Gurbulak, B.; Gurbulak, E.K.; Donmez, T.; Hut, A.; Yildirim, D. A comparison of propofol and midazolam/meperidine sedation in upper gastrointestinal endoscopy. Wideochir. Inne Tech. Maloinwazyjne 2016, 11, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Vargo, J.J.; Holub, J.L.; Faigel, D.O.; Lieberman, D.A.; Eisen, G.M. Risk factors for cardiopulmonary events during propofol-mediated upper endoscopy and colonoscopy. Aliment. Pharmacol. Ther. 2006, 24, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Bisschops, R.; Saunders, R.; Dooms, C.; Hoffman, I.; van der Merwe, S.; Weissbrod, R.; Torres, R.T.; Van Assche, G.; Demedts, I. Implementing capnography to help improve patient safety during procedural sedation: Quality improvement in a high-volume gastroenterology department. Eur. J. Gastroenterol. Hepatol. 2021, 33, e522–e528. [Google Scholar] [CrossRef] [PubMed]
- Kilic, E.T.; Sayar, S.; Kahraman, R.; Ozdil, K. The effects of obesity on sedation-related outcomes of advanced endoscopic procedures. North Clin. Istanb. 2019, 6, 321–326. [Google Scholar] [PubMed]
- Koruk, S.; Koruk, I.; Arslan, A.M.; Bilgi, M.; Gul, R.; Bozgeyik, S. Dexmedetomidine or midazolam in combination with propofol for sedation in endoscopic retrograde cholangiopancreatography: A randomized double blind prospective study. Wideochir. Inne Tech. Maloinwazyjne 2020, 15, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.; Davis, J.A.; Kranke, P.; Weissbrod, R.; Whitaker, D.K.; Lightdale, J.R. Clinical and economic burden of procedural sedation-related adverse events and their outcomes: Analysis from five countries. Ther. Clin. Risk Manag. 2018, 14, 393–401. [Google Scholar] [CrossRef] [PubMed]
- WHO. Prevalence of Noncommunicable Disease Risk Factors; WHO Regional Office for Europe: Geneva, Switzerland, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Procedure Type |
|---|
| Percutaneous endoscopic gastrostomy |
| Endoscopic esophageal variceal ligation |
| Endoscopic cysto-gastrostomy |
| Endoscopic retrograde cholangiopancreatography |
| Percutaneous transhepatic cholangiography |
| Endoscopic submucosal dissection |
| Endoscopic mucosal dissection |
| Endoscopic diagnostic ultrasonography |
| Gastroscopy |
| Esophagoscopy |
| Esophagoscopy and endoscopic submucosal dissection |
| Esophagoscopy and endoscopic diagnostic ultrasonography |
| Colonoscopy |
| Colonoscopy and Gastroscopy |
| Parameter | Non-Capnography N Patients | Capnography N Patients | p-Values |
|---|---|---|---|
| Total | 730 | 880 | |
| Procedure | <0.05 | ||
| Gastroscopy | 177 (24.25%) | 311 (35.34%) | |
| Colonoscopy | 124 (16.99%) | 140 (15.91%) | |
| Gastroscopy + Colonoscopy | 254 (34.79%) | 288 (32.73%) | |
| PEG | 2 (0.27%) | 1 (0.11%) | |
| ERCP | 98 (13.42%) | 95 (10.80%) | |
| ESD | 3 (0.41%) | 0 (0.00%) | |
| EMD | 3 (0.41%) | 3 (0.34%) | |
| EDU | 31 (4.25%) | 41 (4.66%) | |
| Escopy + EUD | 36 (4.93%) | 1 (0.11%) | |
| Escopy + ESD | 2 (0.27%) | 0 (0.00%) | |
| Age group | 0.902 | ||
| ≤50 years | 273 (37.40%) | 328 (37.27%) | |
| 51–60 years | 191 (26.16%) | 224 (25.45%) | |
| 61–70 years | 165 (22.60%) | 221 (25.11%) | |
| 71–80 years | 79 (10.82%) | 88 (10.00%) | |
| >80 years | 22 (3.01%) | 19 (2.16%) | |
| ASA classification | 0.388 | ||
| ASA I | 354 (48.49%) | 315 (35.80%) | |
| ASA II | 339 (46.44%) | 526 (59.77%) | |
| ASA III | 37 (5.07%) | 38 (4.32%) | |
| ASA IV | 0 (0.00%) | 1 (0.11%) | |
| Sedative | <0.05 | ||
| Propofol | 660 (90.41%) | 819 (93.07%) | |
| Propofol + fentanyl | 28 (3.84%) | 33 (3.75%) | |
| Propofol + ketamine | 12 (1.64%) | 5 (0.57%) | |
| Propofol + midazolam | 18 (2.47%) | 6 (0.68%) | |
| Propofol + fentanyl + midazolam | 12 (1.64%) | 17 (1.93%) | |
| Parameter | Mild Oxygen Desaturation | Severe Oxygen Desaturation | Bradycardia | Tachycardia | ||||
|---|---|---|---|---|---|---|---|---|
| N Events (% of Procedures with Event) | ||||||||
| Without Capnography | With Capnography | Without Capnography | With Capnography | Without Capnography | With Capnography | Without Capnography | With Capnography | |
| Total | 44 (6.03%) | 14 (1.59%) | 7 (0.96%) | 6 (0.68%) | 2 (0.27%) | 5 (0.57%) | 2 (0.27%) | 1 (0.11%) |
| Procedure | ||||||||
| Gastroscopy | 10 (5.65%) | 3 (0.96%) | 1 (0.56%) | 1 (0.32%) | 0 | 0 | 0 | 0 |
| Colonoscopy | 3 (2.42%) | 1 (0.71%) | 2 (1.61%) | 0 | 0 | 1 (0.71%) | 0 | 0 |
| Gastroscopy + Colonoscopy | 11 (4.33%) | 5 (1.74%) | 1 (0.39%) | 2 (0.69%) | 0 | 2 (0.69%) | 0 | 0 |
| PEG | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| ERCP | 14 (14.29%) | 4 (4.21%) | 1 (1.02%) | 1 (1.05%) | 2 (2.04%) | 1 (1.05%) | 1 (1.02%) | 1 (1.05%) |
| ESD | 1 (33.33%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EMD | 1 (33.33%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| EDU | 0 | 1 (2.44%) | 0 | 2 (4.88%) | 0 | 1 (2.44%) | 0 | 0 |
| Escopy + EDU | 3 (8.33%) | 0 | 1 (2.78%) | 0 | 0 | 0 | 0 | 0 |
| Escopy + ESD | 1 (50.00%) | 0 | 1 (50.00%) | 0 | 0 | 0 | 1 (50.00%) | 0 |
| Risk classification | ||||||||
| ASA I | 16 (4.52%) | 1 (0.32%) | 3 (0.85%) | 0 | 1 (0.28%) | 1 (0.32%) | 0 | 0 |
| ASA II | 23 (6.78%) | 10 (1.90%) | 1 (0.29%) | 6 (1.14%) | 1 (0.29%) | 4 (0.76%) | 1 (0.29%) | 1 (0.19%) |
| ASA III | 5 (13.51%) | 3 (7.89%) | 3 (8.11%) | 0 | 0 | 0 | 1 (2.70%) | 0 |
| ASA IV | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Adverse Event | Odds Ratio (95% CI) |
|---|---|
| Mild oxygen desaturation (75–90% for <60 s) | 0.25 (95% CI 0.14 to 0.46) |
| Severe oxygen desaturation, <75% for any duration or <90% for over 60 s | 0.71 (95% CI 0.24 to 2.12) |
| Bradycardia | 2.08 (95% CI 0.40 to 10.75) |
| Tachycardia, >25% from baseline | 0.41 (95% CI 0.04 to 4.58) |
| All n = 1609 | Male n = 748 | Female n = 861 | ||||
|---|---|---|---|---|---|---|
| With Capnography | Without Capnography | With Capnography | Without Capnography | With Capnography | Without Capnography | |
| Events [N] | 23 | 48 | 12 | 14 | 11 | 34 |
| Procedure length (min) | 20.14 ± 13.4 | 21.87 ± 27.23 | 20.85± 13.19 | 23.3 ± 13.81 | 19.43 ± 13.59 | 20.8 ± 33.88 |
| … with primary outcome event (min) | 24.96 ± 15.07 | 26.5 ± 22.39 | 23.42 ± 10.66 | 27.57 ± 14.6 | 26.64 ± 19.21 | 26.06 ± 25.09 |
| … without primary outcome event (min) | 20.01 ± 13.34 | 21.54 ± 27.53 | 20.77 ± 13.26 | 23.1 ± 13.76 | 19.25± 13.4 | 20.34 ± 34.54 |
| Meaningful response (min) | 4.34 ± 2.8 | 5.38 ± 3.93 | 4.42 ± 3.08 | 5.33 ± 3.91 | 4.26 ± 2.49 | 5.41± 3.95 |
| … with primary outcome event (min) | 6.91 ± 6.54 | 8.23 ± 4.47 | 8.5 ± 8.53 | 8.36 ± 4.53 | 5.18 ± 2.79 | 8.18± 4.51 |
| … without primary outcome event (min) | 4.27 ± 2.6 | 5.18± 3.81 | 4.3 ± 2.72 | 5.19 ± 3.83 | 4.23 ± 2.48 | 5.17 ± 3.8 |
| Standing up (min) | 57.48 ± 16.67 | 42.63 ± 14.15 | 57.16 ± 16.79 | 43.11 ± 14.5 | 57.81 ± 16.57 | 42.27 ± 13.89 |
| … with primary outcome event (min) | 70.83 ± 17.41 | 46.02 ± 13.68 | 69.92 ± 17.93 | 42.79 ± 10.6 | 71.82 ± 17.65 | 47.35 ± 14.7 |
| … without primary outcome event (min) | 57.12 ± 16.52 | 42.39 ± 14.16 | 56.8 ± 16.64 | 43.13 ± 14.67 | 57.45 ± 16.41 | 41.82 ± 13.74 |
| Parameter | Estimate | Standard Error | p-Value |
|---|---|---|---|
| ASA1 | 21.70 | 3.19 | <0.001 |
| ASA2 | 0.45 | 0.79 | 0.57 |
| ASA3 | 3.16 | 1.75 | 0.07 |
| ASA4 | 8.08 | 13.89 | 0.56 |
| Adverse event | 3.49 | 1.70 | <0.05 |
| Capnography | −2.50 | 0.70 | <0.001 |
| Age < 30 | −0.40 | 3.06 | 0.90 |
| Age < 40 | −2.90 | 2.90 | 0.32 |
| Age < 50 | 0.34 | 2.84 | 0.90 |
| Age < 60 | 1.66 | 2.82 | 0.56 |
| Age < 70 | 4.35 | 2.84 | 0.13 |
| Age < 80 | 3.27 | 2.91 | 0.26 |
| Age < 90 | 9.47 | 3.42 | <0.01 |
| Female | −1.27 | 0.69 | 0.07 |
| BMI(Median 26) | −0.03 | 0.07 | 0.66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baytaş, V.; Vural, Ç.; Özçelik, M.; Torres, R.T.; Saunders, R.; Alkış, N. Patient Safety during Propofol Sedation before and after Implementation of Capnography Monitoring. J. Clin. Med. 2023, 12, 5959. https://doi.org/10.3390/jcm12185959
Baytaş V, Vural Ç, Özçelik M, Torres RT, Saunders R, Alkış N. Patient Safety during Propofol Sedation before and after Implementation of Capnography Monitoring. Journal of Clinical Medicine. 2023; 12(18):5959. https://doi.org/10.3390/jcm12185959
Chicago/Turabian StyleBaytaş, Volkan, Çağıl Vural, Menekşe Özçelik, Rafael Torrejon Torres, Rhodri Saunders, and Neslihan Alkış. 2023. "Patient Safety during Propofol Sedation before and after Implementation of Capnography Monitoring" Journal of Clinical Medicine 12, no. 18: 5959. https://doi.org/10.3390/jcm12185959
APA StyleBaytaş, V., Vural, Ç., Özçelik, M., Torres, R. T., Saunders, R., & Alkış, N. (2023). Patient Safety during Propofol Sedation before and after Implementation of Capnography Monitoring. Journal of Clinical Medicine, 12(18), 5959. https://doi.org/10.3390/jcm12185959