

Conduction System Pacing versus Conventional Biventricular Pacing for Cardiac Resynchronization Therapy: Where Are We Heading?

 ,
,
Abstract
:1. Introduction
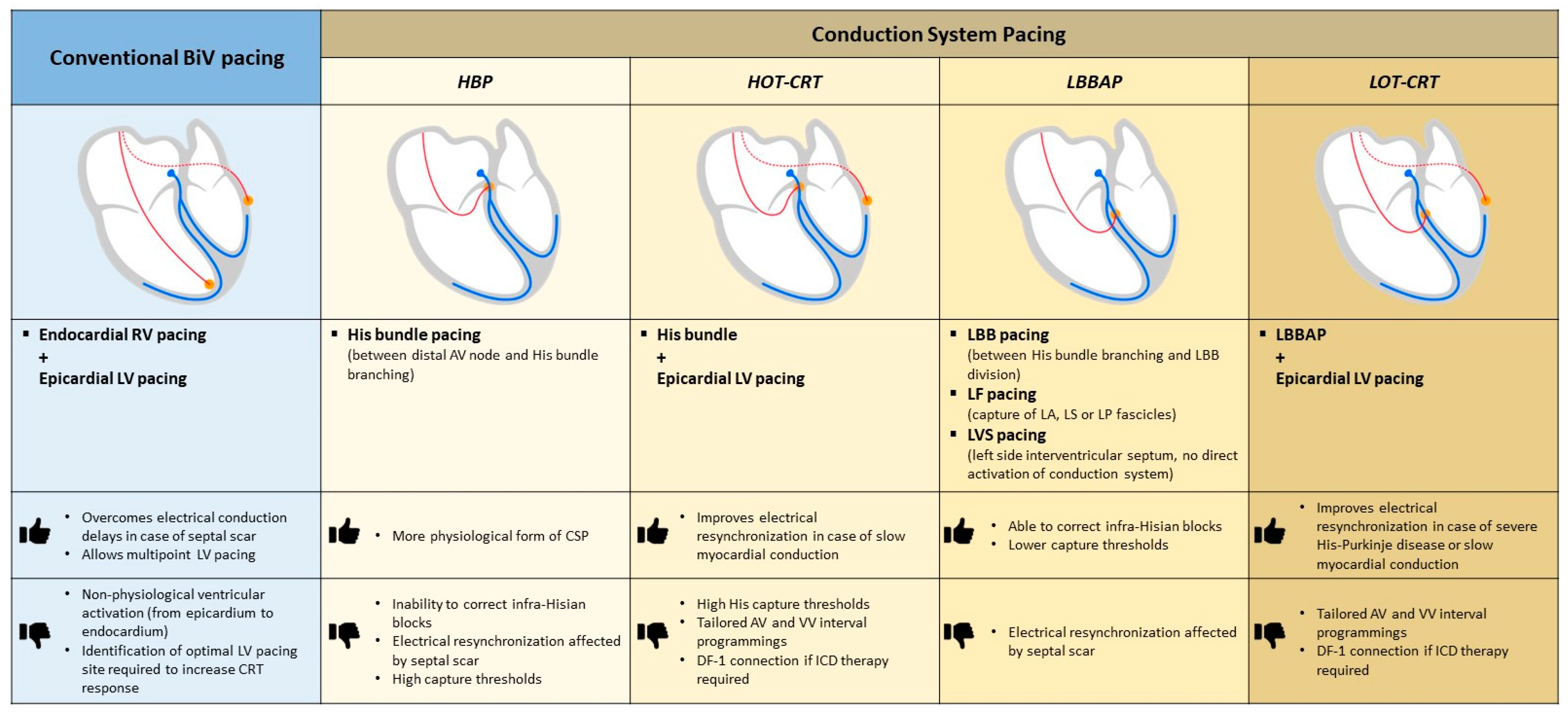
2. Conduction System Pacing to Deliver Cardiac Resynchronization Therapy
2.1. Rational and Techniques
2.2. LBBAP: Comparison with Biventricular Pacing and Implications in Clinical Practice
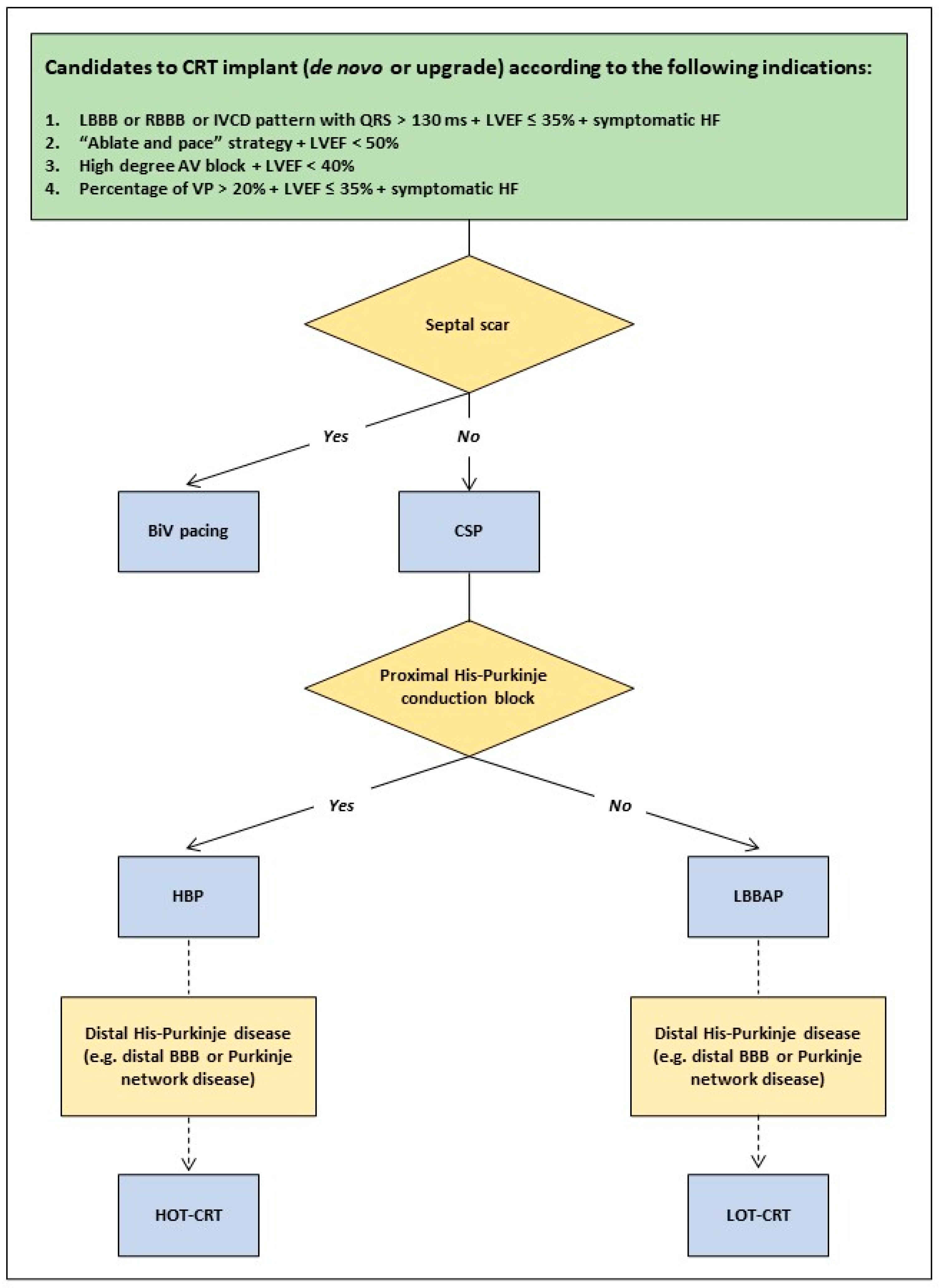
2.3. Evidence Gaps and Practical Considerations
3. Future Directions for CRT Delivery
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdelrahman, M.; Subzposh, F.A.; Beer, D.; Durr, B.; Naperkowski, A.; Sun, H.; Oren, J.W.; Dandamudi, G.; Vijayaraman, P. Clinical Outcomes of His Bundle Pacing Compared to Right Ventricular Pacing. J. Am. Coll. Cardiol. 2018, 71, 2319–2330. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.S.; Patel, N.R.; Ravi, V.; Zalavadia, D.V.; Dommaraju, S.; Garg, V.; Larsen, T.R.; Naperkowski, A.M.; Wasserlauf, J.; Krishnan, K.; et al. Clinical outcomes of left bundle branch area pacing compared to right ventricular pacing: Results from the Geisinger-Rush Conduction System Pacing Registry. Heart Rhythm 2022, 19, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.O.; Prinzen, F.W. A new paradigm for physiologic ventricular pacing. J. Am. Coll. Cardiol. 2006, 47, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.D.; Shun-Shin, M.J.; Keene, D.; Howard, J.P.; Sohaib, S.M.A.; Wright, I.J.; Cole, G.D.; Qureshi, N.A.; Lefroy, D.C.; Koa-Wing, M.; et al. His Resynchronization Versus Biventricular Pacing in Patients With Heart Failure and Left Bundle Branch Block. J. Am. Coll. Cardiol. 2018, 72, 3112–3122. [Google Scholar] [CrossRef]
- Upadhyay, G.A.; Vijayaraman, P.; Nayak, H.M.; Verma, N.; Dandamudi, G.; Sharma, P.S.; Saleem, M.; Mandrola, J.; Genovese, D.; Oren, J.W.; et al. His-SYNC Investigators. On-treatment comparison between corrective His bundle pacing and biventricular pacing for cardiac resynchronization: A secondary analysis of the His-SYNC Pilot Trial. Heart Rhythm 2019, 16, 1797–1807. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Ponnusamy, S.; Cano, Ó.; Sharma, P.S.; Naperkowski, A.; Subsposh, F.A.; Moskal, P.; Bednarek, A.; Dal Forno, A.R.; Young, W.; et al. Left Bundle Branch Area Pacing for Cardiac Resynchronization Therapy: Results From the International LBBAP Collaborative Study Group. JACC Clin. Electrophysiol. 2021, 7, 135–147. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Cano, O.; Ponnusamy, S.S.; Molina-Lerma, M.; Chan, J.Y.S.; Padala, S.K.; Sharma, P.S.; Whinnett, Z.I.; Herweg, B.; Upadhyay, G.A.; et al. Left bundle branch area pacing in patients with heart failure and right bundle branch block: Results from International LBBAP Collaborative-Study Group. Heart Rhythm 2022, 3, 358–367. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Herweg, B.; Ellenbogen, K.A.; Gajek, J. His-Optimized Cardiac Resynchronization Therapy to Maximize Electrical Resynchronization: A Feasibility Study. Circ. ArRhythm Electrophysiol. 2019, 12, e006934. [Google Scholar] [CrossRef]
- Jastrzębski, M.; Moskal, P.; Huybrechts, W.; Curila, K.; Sreekumar, P.; Rademakers, L.M.; Ponnusamy, S.S.; Herweg, B.; Sharma, P.S.; Bednarek, A.; et al. Left bundle branch-optimized cardiac resynchronization therapy (LOT-CRT): Results from an international LBBAP collaborative study group. Heart Rhythm 2022, 19, 13–21. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Zalavadia, D.; Haseeb, A.; Dye, C.; Madan, N.; Skeete, J.R.; Vipparthy, S.C.; Young, W.; Ravi, V.; Rajakumar, C.; et al. Clinical outcomes of conduction system pacing compared to biventricular pacing in patients requiring cardiac resynchronization therapy. Heart Rhythm 2022, 19, 1263–1271. [Google Scholar] [CrossRef]
- Chen, X.; Ye, Y.; Wang, Z.; Jin, Q.; Qiu, Z.; Wang, J.; Qin, S.; Bai, J.; Wang, W.; Liang, Y.; et al. Cardiac resynchronization therapy via left bundle branch pacing vs. optimized biventricular pacing with adaptive algorithm in heart failure with left bundle branch block: A prospective, multi-centre, observational study. Europace 2022, 24, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhu, H.; Hou, X.; Wang, Z.; Zou, F.; Qian, Z.; Wei, Y.; Wang, X.; Zhang, L.; Li, X.; et al. LBBP-RESYNC Investigators. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2022, 80, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraman, P.; Sharma, P.S.; Cano, Ó.; Ponnusamy, S.S.; Herweg, B.; Zanon, F.; Jastrzebski, M.; Zou, J.; Chelu, M.G.; Vernooy, K.; et al. Comparison of Left Bundle Branch Area Pacing and Biventricular Pacing in Candidates for Resynchronization Therapy. J. Am. Coll. Cardiol. 2023, 82, 228–241. [Google Scholar] [CrossRef]
- Pujol-Lopez, M.; Jiménez-Arjona, R.; Garre, P.; Guasch, E.; Borràs, R.; Doltra, A.; Ferró, E.; García-Ribas, C.; Niebla, M.; Carro, E.; et al. Conduction System Pacing vs Biventricular Pacing in Heart Failure and Wide QRS Patients: LEVEL-AT Trial. JACC Clin. Electrophysiol. 2022, 8, 1431–1445. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.C.; Sauer, W.H.; Duque, M.; Koplan, B.A.; Braunstein, E.D.; Marín, J.E.; Aristizabal, J.; Niño, C.D.; Bastidas, O.; Martinez, J.M.; et al. Left Bundle Branch Area Pacing Versus Biventricular Pacing as Initial Strategy for Cardiac Resynchronization. JACC Clin. Electrophysiol. 2023, 9 Pt 2, 1568–1581. [Google Scholar] [CrossRef]
- Kim, J.A.; Kim, S.E.; Ellenbogen, K.A.; Vijayaraman, P.; Chelu, M.G. Clinical outcomes of conduction system pacing versus biventricular pacing for cardiac resynchronization therapy: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2023, 34, 1718–1729. [Google Scholar] [CrossRef]
- Cazeau, S.; Leclercq, C.; Lavergne, T.; Walker, S.; Varma, C.; Linde, C.; Garrigue, S.; Kappenberger, L.; Haywood, G.A.; Santini, M.; et al. Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N. Engl. J. Med. 2001, 344, 873–880. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. Cardiac resynchronization in chronic heart failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef]
- Gin, J.; Chow, C.L.; Voskoboinik, A.; Nalliah, C.; Wong, C.; Van Gaal, W.; Farouque, O.; Mohamed, U.; Lim, H.S.; Kalman, J.M.; et al. Improved outcomes of conduction system pacing in heart failure with reduced ejection fraction: A systematic review and meta-analysis. Heart Rhythm 2023, 20, 1178–1187. [Google Scholar] [CrossRef]
- Ali, N.; Arnold, A.D.; Miyazawa, A.A.; Keene, D.; Chow, J.J.; Little, I.; Peters, N.S.; Kanagaratnam, P.; Qureshi, N.; Ng, F.S.; et al. Comparison of methods for delivering cardiac resynchronization therapy: An acute electrical and haemodynamic within-patient comparison of left bundle branch area, His bundle, and biventricular pacing. Europace 2023, 25, 1060–1067. [Google Scholar] [CrossRef]
- Elliott, M.K.; Strocchi, M.; Sieniewicz, B.J.; Sidhu, B.; Mehta, V.; Wijesuriya, N.; Behar, J.M.; Thorpe, A.; Martic, D.; Wong, T.; et al. Biventricular endocardial pacing and left bundle branch area pacing for cardiac resynchronization: Mechanistic insights from electrocardiographic imaging, acute hemodynamic response, and magnetic resonance imaging. Heart Rhythm 2023, 20, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Vinther, M.; Risum, N.; Svendsen, J.H.; Møgelvang, R.; Philbert, B.T. A Randomized Trial of His Pacing Versus Biventricular Pacing in Symptomatic HF Patients With Left Bundle Branch Block (His-Alternative). JACC Clin. Electrophysiol. 2021, 7, 1422–1432. [Google Scholar] [CrossRef] [PubMed]
- Zanon, F.; Abdelrahman, M.; Marcantoni, L.; Naperkowski, A.; Subzposh, F.A.; Pastore, G.; Baracca, E.; Boaretto, G.; Raffagnato, P.; Tiribello, A.; et al. Long term performance and safety of His bundle pacing: A multicenter experience. J. Cardiovasc. Electrophysiol. 2019, 30, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Teigeler, T.; Kolominsky, J.; Vo, C.; Shepard, R.K.; Kalahasty, G.; Kron, J.; Huizar, J.F.; Kaszala, K.; Tan, A.Y.; Koneru, J.N.; et al. Intermediate-term performance and safety of His-bundle pacing leads: A single-center experience. Heart Rhythm 2021, 18, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, G.A.; Cherian, T.; Shatz, D.Y.; Beaser, A.D.; Aziz, Z.; Ozcan, C.; Broman, M.T.; Nayak, H.M.; Tung, R. Intracardiac Delineation of Septal Conduction in Left Bundle-Branch Block Patterns. Circulation 2019, 139, 1876–1888. [Google Scholar] [CrossRef] [PubMed]
- Burri, H.; Jastrzebski, M.; Cano, Ó.; Čurila, K.; de Pooter, J.; Huang, W.; Israel, C.; Joza, J.; Romero, J.; Vernooy, K.; et al. EHRA clinical consensus statement on conduction system pacing implantation: Endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS). Europace 2023, 25, 1208–1236. [Google Scholar] [CrossRef]
- Su, L.; Wang, S.; Wu, S.; Xu, L.; Huang, Z.; Chen, X.; Zheng, R.; Jiang, L.; Ellenbogen, K.A.; Whinnett, Z.I.; et al. Long-Term Safety and Feasibility of Left Bundle Branch Pacing in a Large Single-Center Study. Circ. Arrhythm. Electrophysiol. 2021, 14, e009261. [Google Scholar] [CrossRef]
- Keene, D.; Arnold, A.D.; Jastrzębski, M.; Burri, H.; Zweibel, S.; Crespo, E.; Chandrasekaran, B.; Bassi, S.; Joghetaei, N.; Swift, M.; et al. His bundle pacing, learning curve, procedure characteristics, safety, and feasibility: Insights from a large international observational study. J. Cardiovasc. Electrophysiol. 2019, 30, 1984–1993. [Google Scholar] [CrossRef]
- Jastrzębski, M.; Kiełbasa, G.; Cano, O.; Curila, K.; Heckman, L.; De Pooter, J.; Chovanec, M.; Rademakers, L.; Huybrechts, W.; Grieco, D.; et al. Left bundle branch area pacing outcomes: The multicentre European MELOS study. Eur. Heart J. 2022, 43, 4161–4173. [Google Scholar] [CrossRef]
- Strocchi, M.; Gillette, K.; Neic, A.; Elliott, M.K.; Wijesuriya, N.; Mehta, V.; Vigmond, E.J.; Plank, G.; Rinaldi, C.A.; Niederer, S.A. Comparison between conduction system pacing and cardiac resynchronization therapy in right bundle branch block patients. Front. Physiol. 2022, 13, 1011566. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021, 42, 3427–3520, Erratum in Eur. Heart J. 2022, 43, 1651. [Google Scholar] [CrossRef] [PubMed]
- Zheng, R.; Wu, S.; Wang, S.; Su, L.; Ellenbogen, K.A.; Huang, W. Case Report: Interventricular Septal Hematoma Complicating Left Bundle Branch Pacing Lead Implantation. Front. Cardiovasc. Med. 2021, 8, 744079. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, R.; Rattigan, E.; Bauch, T.D.; Mascarenhas, V.; Ahmad, T.; Subzposh, F.A.; Vijayaraman, P. Giant Interventricular Septal Hematoma Complicating Left Bundle Branch Pacing: A Cautionary Tale. JACC Case Rep. 2023, 16, 101887. [Google Scholar] [CrossRef] [PubMed]
- Del Monte, A.; Chierchia, G.B.; de Asmundis, C.; Sorgente, A. When Good Goes Bad: Interventricular Septal Hematoma Complicating Left Bundle Branch Area Pacing. JACC Case Rep. 2023, 16, 101889. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Patton, K.K.; Lau, C.P.; Dal Forno, A.R.J.; Al-Khatib, S.M.; Arora, V.; Birgersdotter-Green, U.M.; Cha, Y.M.; Chung, E.H.; Cronin, E.M.; et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023, 20, e17–e91. [Google Scholar] [CrossRef]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomström-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar]
- Strocchi, M.; Gillette, K.; Neic, A.; Elliott, M.K.; Wijesuriya, N.; Mehta, V.; Vigmond, E.J.; Plank, G.; Rinaldi, C.A.; Niederer, S.A. Effect of scar and His-Purkinje and myocardium conduction on response to conduction system pacing. J. Cardiovasc. Electrophysiol. 2023, 34, 984–993. [Google Scholar] [CrossRef]
- Ponnusamy, S.S.; Arora, V.; Namboodiri, N.; Kumar, V.; Kapoor, A.; Vijayaraman, P. Left bundle branch pacing: A comprehensive review. J. Cardiovasc. Electrophysiol. 2020, 31, 2462–2473. [Google Scholar] [CrossRef]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram, part III: Intraventricular conduction disturbances: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation 2009, 119, e235–e240. [Google Scholar]
- Vijayaraman, P.; Subzposh, F.A.; Naperkowski, A. Extraction of the permanent His bundle pacing lead: Safety outcomes and feasibility of reimplantation. Heart Rhythm 2019, 16, 1196–1203. [Google Scholar] [CrossRef]
- Vijayaraman, P. Extraction of Left Bundle Branch Pacing Lead. JACC Clin. Electrophysiol. 2020, 6, 903–904. [Google Scholar] [CrossRef] [PubMed]
- Ponnusamy, S.S.; Vijayaraman, P. Late dislodgement of left bundle branch pacing lead and successful extraction. J. Cardiovasc. Electrophysiol. 2021, 32, 2346–2349. [Google Scholar] [CrossRef] [PubMed]
- Migliore, F.; Aruta, P.; Cecchetto, A.; Iliceto, S.; Gerosa, G.; Catanzariti, D. Extraction of left bundle branch pacing lead: A safe procedure? Europace 2021, 23, 1921. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; You, H.; Chen, K.; Dai, Y.; Lu, W.; Li, Y.; Cheng, C.; Zhou, Y.; Wang, J.; Chen, R.; et al. Distance between the lead-implanted site and tricuspid valve annulus in patients with left bundle branch pacing: Effects on postoperative tricuspid regurgitation deterioration. Heart Rhythm 2023, 20, 217–223. [Google Scholar] [CrossRef]
- Zhang, L.; Cheng, X.; Chen, J.; Zhou, M.; Qian, T.; Zhang, Z.; Yin, J.; Zhang, H.; Dai, G.; Qin, Y.; et al. Left Bundle Pacing for Left Bundle Branch Block and Intermittent Third-Degree Atrioventricular Block in a MYH7 Mutation-Related Hypertrophic Cardiomyopathy With Restrictive Phenotype in a Child. Front. Pediatr. 2020, 8, 312. [Google Scholar] [CrossRef] [PubMed]
- Patra, S.; Halder, A.; Chakraborty, R.; Pande, A.; Kumar, D.; Dey, S.; Mukherjee, S.S.; Roy, R.R. Left bundle branch pacing in hypertrophic cardiomyopathy-a novel approach. Am. J. Cardiovasc. Dis. 2021, 11, 710–713. [Google Scholar] [PubMed]
- Strocchi, M.; Lee, A.W.C.; Neic, A.; Bouyssier, J.; Gillette, K.; Plank, G.; Elliott, M.K.; Gould, J.; Behar, J.M.; Sidhu, B.; et al. His-bundle and left bundle pacing with optimized atrioventricular delay achieve superior electrical synchrony over endocardial and epicardial pacing in left bundle branch block patients. Heart Rhythm 2020, 17, 1922–1929. [Google Scholar] [CrossRef]
- Sun, W.; Upadhyay, G.A.; Tung, R. Influence of Capture Selectivity and Left Intrahisian Block on QRS Characteristics During Left Bundle Branch Pacing. JACC Clin. Electrophysiol. 2022, 8, 635–647. [Google Scholar] [CrossRef]
- Ponnusamy, S.S.; Ganesan, V.; Ramalingam, V.; Syed, T.; Mariappan, S.; Murugan, S.; Kumar, M.; Anand, V.; Murugan, M.; Vijayaraman, P. MAgnetic resonance imaging based DUal lead cardiac Resynchronization therapy: A prospectIve Left Bundle Branch Pacing study (MADURAI LBBP study). Heart Rhythm 2023, 20, 1119–1127. [Google Scholar] [CrossRef]
- Wijesuriya, N.; Elliott, M.K.; Mehta, V.; Sidhu, B.S.; Strocchi, M.; Behar, J.M.; Niederer, S.; Rinaldi, C.A. Leadless Left Bundle Branch Area Pacing in Cardiac Resynchronisation Therapy: Advances, Challenges and Future Directions. Front. Physiol. 2022, 13, 898866. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Authors | Year | Study Design | Total n. of pts | Study pts | Intervention | Follow-Up (Months) | Outcomes | |
|---|---|---|---|---|---|---|---|---|
| His-CRT | Upadhyay GA et al. [5] | 2019 | RCT | 41 | QRS > 120 ms, LVEF ≤ 35%, NYHA II–IV | His-CRT vs. BiV-CRT | 12.2 | Greater QRS narrowing in His-CRT pts vs. BiV-CRT pts |
| Vinther M et al. [22] | 2021 | RCT | 50 | LBBB, LVEF ≤ 35%, | His-CRT vs. BiV-CRT | 6 | Similar clinical and physical improvement in both groups | |
| HOT-CRT | Vijayaraman et al. [8] | 2019 | Prospective, observational | 27 | LBBB or IVCD, QRS ≥140 ms, LVEF ≤ 35%, NYHA III–IV | Feasibility study | 14 ± 10 | Feasibility criteria met Greater QRS narrowing in HOT-CRT vs. BiV or His pacing Significant increase in LVEF and NYHA compared to baseline |
| LBBAP-CRT | Vijayaraman et al. [6] | 2021 | Retrospective, observational | 325 | LVEF < 50%, CRT or pacing indications | Feasibility study | 6 ± 5 | Feasibility and safety criteria met Significant QRS narrowing Significant increase in LVEF and NYHA compared to baseline |
| Vijayaraman et al. [7] | 2022 | Retrospective, observational | 121 | RBBB, LVEF < 50%, CRT or pacing indications | Feasibility study | 13 ± 8 | Feasibility criteria met Significant QRS narrowing Significant increase in LVEF and NYHA compared to baseline | |
| LOT-CRT | Jastrzębski et al. [9] | 2022 | Prospective, observational | 112 | CRT indications or non-response to CRT | Feasibility study | 7.8 ± 2.3 | Feasibility and safety criteria met Greater QRS narrowing in LOT-CRT vs. BiV or LBBAP Significant increase in LVEF and NYHA and a significant reduction in LVEDV and NT-proBNP compared to baseline |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domenichini, G.; Le Bloa, M.; Teres Castillo, C.; Graf, D.; Carroz, P.; Ascione, C.; Porretta, A.P.; Pascale, P.; Pruvot, E. Conduction System Pacing versus Conventional Biventricular Pacing for Cardiac Resynchronization Therapy: Where Are We Heading? J. Clin. Med. 2023, 12, 6288. https://doi.org/10.3390/jcm12196288
Domenichini G, Le Bloa M, Teres Castillo C, Graf D, Carroz P, Ascione C, Porretta AP, Pascale P, Pruvot E. Conduction System Pacing versus Conventional Biventricular Pacing for Cardiac Resynchronization Therapy: Where Are We Heading? Journal of Clinical Medicine. 2023; 12(19):6288. https://doi.org/10.3390/jcm12196288
Chicago/Turabian StyleDomenichini, Giulia, Mathieu Le Bloa, Cheryl Teres Castillo, Denis Graf, Patrice Carroz, Ciro Ascione, Alessandra Pia Porretta, Patrizio Pascale, and Etienne Pruvot. 2023. "Conduction System Pacing versus Conventional Biventricular Pacing for Cardiac Resynchronization Therapy: Where Are We Heading?" Journal of Clinical Medicine 12, no. 19: 6288. https://doi.org/10.3390/jcm12196288
APA StyleDomenichini, G., Le Bloa, M., Teres Castillo, C., Graf, D., Carroz, P., Ascione, C., Porretta, A. P., Pascale, P., & Pruvot, E. (2023). Conduction System Pacing versus Conventional Biventricular Pacing for Cardiac Resynchronization Therapy: Where Are We Heading? Journal of Clinical Medicine, 12(19), 6288. https://doi.org/10.3390/jcm12196288