
A Data-Driven Method to Discriminate Limb Salvage from Other Combat-Related Extremity Trauma

 , and
, and
Abstract
:1. Introduction
2. Methods
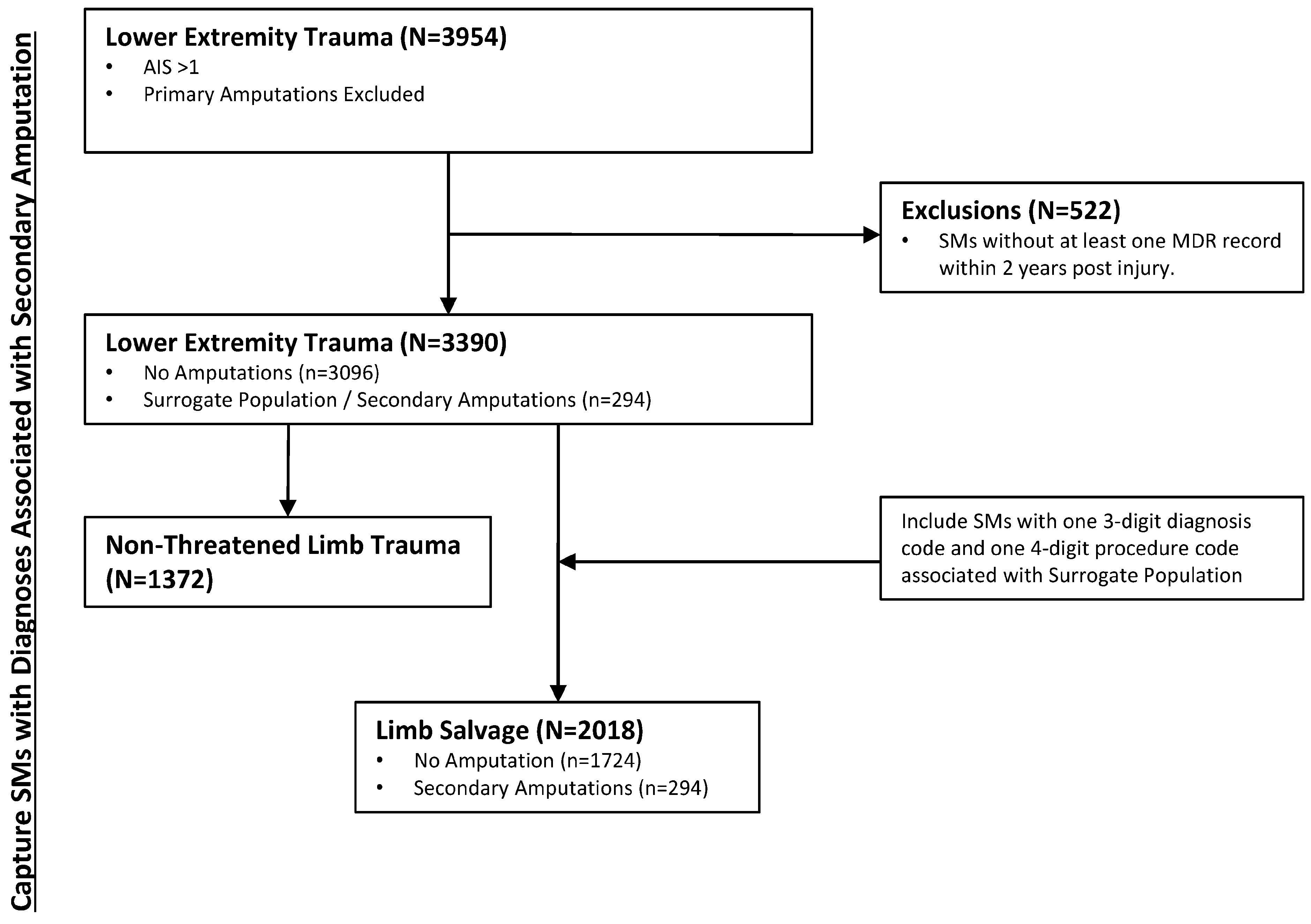
2.1. Definition of Study Populations
2.2. Systematic Grouping of Medical Codes for Discriminant Analysis
2.3. Determination of Medical Codes Associated with Limb Salvage
2.4. Validation of Data-Driven Limb Salvage Definition Approach
3. Results
3.1. Diagnoses Significantly Associated with Limb Salvage
3.2. Procedures Significantly Associated with Limb Salvage
3.3. Prevalence of Limb Salvage Cases in Combat-Related Extremity Trauma
3.4. Validation of Data-Driven Approach for Defining Limb Salvage
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
6. Disclaimer
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cross, J.D.; Ficke, J.R.; Hsu, J.R.; Masini, B.D.; Wenke, J.C. Battlefield orthopaedic injuries cause the majority of long-term disabilities. J. Am. Acad. Orthop. Surg. 2011, 19 (Suppl. S1), S1–S7. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, A.L.; Mohrle, C.R.; Galarneau, M.R.; Woodruff, S.I.; Dye, J.L.; Quinn, K.H. Battlefield extremity injuries in Operation Iraqi Freedom. Injury 2009, 40, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, M.S. Casualty Rates of US Military Personnel During the Wars in Iraq and Afghanistan. Def. Peace Econ. 2018, 29, 44–61. [Google Scholar] [CrossRef]
- Goldberg, M.S. Death and Injury Rates of U.S. Military Personnel in Iraq. Mil. Med. 2010, 175, 220–226. [Google Scholar] [CrossRef]
- Major Extremity Trauma Research Consortium. Outcomes Following Severe Distal Tibial, Ankle, and/or Mid/Hindfoot Trauma: Comparison of Limb Salvage and Transtibial Amputation (OUTLET). J. Bone Jt. Surg. Am. 2021, 103, 1588–1597. [Google Scholar] [CrossRef]
- Brown, K.V.; Henman, P.; Stapley, S.; Clasper, J.C. Limb salvage of severely injured extremities after military wounds. J. R. Army Med. Corps 2011, 157 (Suppl. S1), S315–S323. [Google Scholar] [CrossRef]
- Connelly, J.; Airey, M.; Chell, S. Variation in clinical decision making is a partial explanation for geographical variation in lower extremity amputation rates. Br. J. Surg. 2001, 88, 529–535. [Google Scholar] [CrossRef]
- Dagum, A.B.; Best, A.K.; Schemitsch, E.H.; Mahoney, J.L.; Mahomed, M.N.; Blight, K.R. Salvage after severe lower-extremity trauma: Are the outcomes worth the means? Plast. Reconstr. Surg. 1999, 103, 1212–1220. [Google Scholar] [CrossRef]
- O’Sullivan, S.T.; O’Sullivan, M.; Pasha, N.; O’Shaughnessy, M.; O’Connor, T. Is it possible to predict limb viability in complex Gustilo IIIB and IIIC tibial fractures? A comparison of two predictive indices. Injury 1997, 28, 639–642. [Google Scholar] [CrossRef]
- Song, W.; Zhou, D.; Dong, J. Predictors of secondary amputation in patients with grade IIIC lower limb injuries: A retrospective analysis of 35 patients. Medicine 2017, 96, e7068. [Google Scholar] [CrossRef]
- Ege, T.; Unlu, A.; Tas, H.; Bek, D.; Turkan, S.; Cetinkaya, A. Reliability of the mangled extremity severity score in combat-related upper and lower extremity injuries. Indian J. Orthop. 2015, 49, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Mullenix, P.S.; Steele, S.R.; Andersen, C.A.; Starnes, B.W.; Salim, A.; Martin, M.J. Limb salvage and outcomes among patients with traumatic popliteal vascular injury: An analysis of the National Trauma Data Bank. J. Vasc. Surg. 2006, 44, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, M.; Maman, P.; Curvale, G.; Rochwerger, A.; Mattei, J.-C. Amputation versus conservative treatment in severe open lower-limb fracture: A functional and quality-of-life study. Orthop. Traumatol. Surg. Res. 2018, 104, 277–281. [Google Scholar] [CrossRef]
- Bosse, M.J.; MacKenzie, E.J.; Kellam, J.F.; Burgess, A.R.; Webb, L.X.; Swiontkowski, M.F.; Sanders, R.W.; Jones, A.L.; McAndrew, M.P.; Patterson, B.M.; et al. A prospective evaluation of the clinical utility of the lower-extremity injury-severity scores. J. Bone Jt. Surg. Am. 2001, 83, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Korompilias, A.V.; Beris, A.; Lykissas, M.G.; Vekris, M.D.; A Kontogeorgakos, V.; Soucacos, P.N. The mangled extremity and attempt for limb salvage. J. Orthop. Surg. Res. 2009, 4, 4. [Google Scholar] [CrossRef] [PubMed]
- Melcer, T.; Sechriest, V.F.; Walker, J.; Galarneau, M. A comparison of health outcomes for combat amputee and limb salvage patients injured in Iraq and Afghanistan wars. J. Trauma Acute Care Surg. 2013, 75 (Suppl. S2), S247–S254. [Google Scholar] [CrossRef] [PubMed]
- Galarneau, M.R.; Hancock, W.C.; Konoske, P.; Melcer, T.; Vickers, R.R.; Walker, G.J.; Zouris, J.M. The Navy-Marine Corps Combat Trauma Registry. Mil. Med. 2006, 171, 691–697. [Google Scholar] [CrossRef]
- Eskridge, S.L.; Hill, O.T.; Clouser, M.C.; Galarneau, M.R. Association of Specific Lower Extremity Injuries With Delayed Amputation. Mil. Med. 2019, 184, e323–e329. [Google Scholar] [CrossRef]
- Piquado, T.; Hoch, E.; Engel, C.C. Limb Salvage and Recovery After Blast-Related Injury: Proceedings and Expert Findings from a U.S. Department of Defense International State-of-the-Science Meeting; RAND Corporation: Santa Monica, CA, USA, 2020. [Google Scholar]
- O’Malley, K.J.; Cook, K.F.; Price, M.D.; Wildes, K.R.; Hurdle, J.F.; Ashton, C.M. Measuring diagnoses: ICD code accuracy. Health Serv. Res. 2005, 40 Pt 2, 1620–1639. [Google Scholar] [CrossRef]
- Farrokhi, S.; Mazzone, B.; Moore, J.L.; Shannon, K.; Eskridge, S. Physical Therapy Practice Patterns for Military Service Members with Lower Limb Loss. Mil. Med. 2019, 184, e907–e913. [Google Scholar] [CrossRef]
- Castillo, R.C.; MacKenzie, E.J.; Webb, L.X.; Bosse, M.J.; Avery, J. Use and perceived need of physical therapy following severe lower-extremity trauma. Arch. Phys. Med. Rehabil. 2005, 86, 1722–1728. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ICD-9 Code Grouping Strategy | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | |
|---|---|---|---|---|---|
| Diagnosis Codes | 1-Digit Families | 71.43% | 36.34% | 9.63% | 93.05% |
| 2-Digit Families | 95.58% | 21.64% | 10.38% | 98.10% | |
| 3-Digit Families | 91.84% | 36.79% | 12.12% | 97.94% | |
| 4-Digit Families | 84.69% | 62.08% | 17.50% | 97.71% | |
| Procedure Codes | 1-Digit Families | 99.32% | 7.01% | 9.21% | 99.09% |
| 2-Digit Families | 99.32% | 8.59% | 9.35% | 99.25% | |
| 3-Digit Families | 98.64% | 11.37% | 9.56% | 98.88% | |
| 4-Digit Families | 98.64% | 12.86% | 9.71% | 99.00% | |
| ICD-9 Code | Description | Frequency (f) | Percentage (%) | LE Trauma (AIS > 1) N = 3390 | PPV | NPV | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| No Amputation n = 3096 | Surrogate Population n = 294 | |||||||||
| f | % | f | % | |||||||
| 823 | tib/fib fx | 1285 | 37.91 | 1106 | 35.72 | 179 | 60.88 | 13.9 | 94.5 | <0.0001 |
| 825 | metatarsal/tarsal fx | 942 | 27.79 | 763 | 24.64 | 179 | 60.88 | 19.0 | 95.3 | <0.0001 |
| 904 | LE blood vessel injury | 520 | 15.34 | 435 | 14.05 | 85 | 28.91 | 16.3 | 92.7 | <0.0001 |
| 824 | fx ankle (tib/fib) | 488 | 14.40 | 404 | 13.05 | 84 | 28.57 | 17.2 | 92.8 | <0.0001 |
| 838 | foot dislocation | 192 | 5.66 | 118 | 3.82 | 74 | 25.17 | 38.5 | 93.1 | <0.0001 |
| 837 | ankle dislocation | 124 | 3.66 | 86 | 2.78 | 38 | 12.93 | 30.6 | 92.2 | <0.0001 |
| ICD-9 Code | Description | LE Trauma (AIS > 1) N = 3390 | PPV | NPV | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Frequency (f) | Percentage (%) | No Amputation n = 3096 | Surrogate Population n = 294 | |||||||
| f | % | f | % | |||||||
| 86.28 | Nonexcisional debridement of wound, infection, or burn | 1782 | 52.6 | 1573 | 50.8 | 209 | 71.1 | 11.7 | 94.7 | <0.00001 |
| 86.59 | Closure of skin and subcutaneous tissue of other sites | 1454 | 42.9 | 1286 | 41.5 | 168 | 57.1 | 11.6 | 93.5 | <0.00001 |
| 86.22 | Excisional debridement of wound, infection, or burn | 1392 | 41.1 | 1214 | 39.2 | 178 | 60.5 | 12.8 | 94.2 | <0.00001 |
| 99.04 | Transfusion of packed cells | 1058 | 31.2 | 877 | 28.3 | 181 | 61.6 | 17.1 | 95.2 | <0.00001 |
| 86.69 | Other skin graft to other sites | 738 | 21.8 | 617 | 19.9 | 121 | 41.2 | 16.4 | 93.5 | <0.00001 |
| 88.38 | Other computerized axial tomography | 713 | 21.0 | 623 | 20.1 | 90 | 30.6 | 12.6 | 92.4 | 0.000025 |
| 96.59 | Other irrigation of wound | 658 | 19.4 | 576 | 18.6 | 82 | 27.9 | 12.5 | 92.2 | 0.00012 |
| 38.93 | Venous catheterization, not elsewhere classified | 595 | 17.5 | 482 | 15.6 | 113 | 38.4 | 19.0 | 93.5 | <0.00001 |
| 79.36 | Open reduction of fracture with internal fixation(tib/fib) | 555 | 16.4 | 470 | 15.2 | 85 | 28.9 | 15.3 | 92.6 | <0.00001 |
| 79.66 | Debridement of open fracture site (tib/fib) | 535 | 15.8 | 441 | 14.2 | 94 | 32.0 | 17.6 | 93.0 | <0.00001 |
| 83.45 | Other myectomy | 474 | 14.0 | 378 | 12.2 | 96 | 32.6 | 20.3 | 93.2 | <0.00001 |
| 93.59 | Other immobilization, pressure, and attention to wound | 472 | 13.9 | 402 | 13.0 | 70 | 23.8 | 14.8 | 92.3 | <0.00001 |
| 93.57 | Application of other wound dressing | 438 | 12.9 | 375 | 12.1 | 63 | 21.4 | 14.4 | 92.2 | <0.00001 |
| 99.21 | Injection of antibiotic | 380 | 11.2 | 294 | 9.5 | 87 | 29.6 | 22.8 | 93.1 | <0.00001 |
| 78.67 | Removal of implanted devices from bone (tib/fib) | 331 | 9.8 | 249 | 8.0 | 82 | 27.9 | 24.8 | 93.1 | <0.00001 |
| 79.37 | Open reduction of fracture with internal fixation (tarsal/MT) | 297 | 8.8 | 228 | 7.4 | 69 | 23.5 | 23.2 | 92.7 | <0.00001 |
| 78.17 | Application of external fixator device (tib/fib) | 279 | 8.2 | 204 | 6.6 | 75 | 25.5 | 26.9 | 93.0 | <0.00001 |
| 93.56 | Application of pressure dressing | 256 | 7.5 | 215 | 6.9 | 41 | 13.9 | 16.0 | 91.9 | 0.000014 |
| 93.54 | Application of splint | 225 | 6.6 | 190 | 6.1 | 35 | 11.9 | 15.6 | 91.8 | 0.00015 |
| 99.99 | Other | 220 | 6.5 | 183 | 5.9 | 37 | 12.6 | 16.8 | 91.9 | <0.00001 |
| 86.04 | Other incision with drainage of skin and subcutaneous tissue | 213 | 6.3 | 170 | 5.5 | 43 | 14.6 | 20.2 | 92.1 | <0.00001 |
| 79.67 | Debridement of open fracture site (tarsal/MT) | 185 | 5.5 | 129 | 4.2 | 56 | 19.0 | 30.3 | 92.6 | <0.00001 |
| 88.48 | Arteriography of femoral and other lower extremity arteries | 180 | 5.3 | 139 | 4.5 | 41 | 13.9 | 22.8 | 92.1 | <0.00001 |
| 99.07 | Transfusion of other serum | 166 | 4.9 | 129 | 4.2 | 37 | 12.6 | 22.3 | 92.0 | <0.00001 |
| 04.81 | Injection of anesthetic into peripheral nerve for analgesia | 160 | 4.7 | 128 | 4.1 | 32 | 10.9 | 20.0 | 91.9 | <0.00001 |
| ICD-9 Code | Description | Frequency (f) | Percentage (%) | LE Trauma (AIS > 1) N = 3390 | PPV | NPV | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Limb Salvage n = 2018 | Non-Threatened Limb Trauma n = 1372 | |||||||||
| f | % | f | % | |||||||
| 823 | tib/fib fx | 1285 | 37.91 | 1203 | 59.6 | 82 | 6.0 | 93.6 | 61.3 | <0.0001 |
| 825 | metatarsal/tarsal fx | 942 | 27.79 | 851 | 42.2 | 91 | 6.6 | 90.3 | 52.3 | <0.0001 |
| 904 | blood vessel injury LE | 520 | 15.34 | 493 | 24.4 | 27 | 2.0 | 94.8 | 46.9 | <0.0001 |
| 824 | fx ankle (tib/fib) | 488 | 14.40 | 444 | 22.0 | 44 | 3.2 | 91.0 | 45.8 | <0.0001 |
| 838 | foot dislocation | 192 | 5.66 | 185 | 9.2 | 7 | 0.5 | 96.3 | 42.7 | <0.0001 |
| 837 | ankle dislocation | 124 | 3.66 | 121 | 6.0 | 3 | 0.2 | 97.6 | 41.9 | <0.0001 |
| ICD-9 Code | Description | Frequency (f) | Percentage (%) | LE Trauma (AIS > 1) N = 3390 | PPV | NPV | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Limb Salvage n = 2018 | Non-Threatened Limb Trauma n = 1372 | |||||||||
| f | % | f | % | |||||||
| 86.28 | Nonexcisional debridement of wound, infection, or burn | 1782 | 52.6 | 1181 | 58.5 | 601 | 43.8 | 66.3 | 47.9 | <0.00001 |
| 86.59 | Closure of skin and subcutaneous tissue of other sites | 1454 | 42.9 | 985 | 48.8 | 469 | 34.2 | 67.7 | 46.6 | <0.00001 |
| 86.22 | Excisional debridement of wound, infection, or burn | 1392 | 41.1 | 961 | 47.2 | 431 | 31.4 | 69.0 | 47.1 | <0.00001 |
| 99.04 | Transfusion of packed cells | 1058 | 31.2 | 758 | 37.6 | 300 | 21.9 | 71.6 | 46.0 | <0.00001 |
| 86.69 | Other skin graft to other sites | 738 | 21.8 | 538 | 26.7 | 200 | 14.6 | 72.9 | 44.2 | <0.00001 |
| 88.38 | Other computerized axial tomography | 713 | 21.0 | 501 | 24.8 | 212 | 15.4 | 70.3 | 43.3 | <0.00001 |
| 96.59 | Other irrigation of wound | 658 | 19.4 | 444 | 22.0 | 214 | 15.6 | 67.5 | 42.4 | <0.00001 |
| 38.93 | Venous catheterization, not elsewhere classified | 595 | 17.5 | 410 | 20.3 | 185 | 13.5 | 68.9 | 42.5 | <0.00001 |
| 79.36 | Open reduction of fracture with internal fixation (tib/fib) | 555 | 16.4 | 541 | 26.8 | 14 | 1.0 | 97.5 | 47.9 | <0.00001 |
| 79.66 | Debridement of open fracture site (tib/fib) | 535 | 15.8 | 515 | 25.5 | 20 | 1.5 | 96.3 | 47.4 | <0.00001 |
| 83.45 | Other myectomy | 474 | 14.0 | 340 | 16.8 | 134 | 9.8 | 71.7 | 42.5 | <0.00001 |
| 93.59 | Other immobilization, pressure, and attention to wound | 472 | 13.9 | 335 | 16.6 | 137 | 10.0 | 71.0 | 42.3 | <0.00001 |
| 93.57 | Application of other wound dressing | 438 | 12.9 | 298 | 14.8 | 140 | 10.2 | 68.0 | 41.7 | 0.0001 |
| 99.21 | Injection of antibiotic | 380 | 11.2 | 291 | 14.4 | 89 | 6.5 | 76.6 | 42.6 | <0.00001 |
| 78.67 | Removal of implanted devices from bone (tib/fib) | 331 | 9.8 | 325 | 16.1 | 6 | 0.4 | 98.2 | 44.7 | <0.00001 |
| 79.37 | Open reduction of fracture with internal fixation (tarsal/MT) | 297 | 8.8 | 296 | 14.7 | 1 | <0.1 | 99.7 | 44.3 | <0.00001 |
| 78.17 | Application of external fixator device (tib/fib) | 279 | 8.2 | 278 | 13.8 | 1 | <0.1 | 99.6 | 44.1 | <0.00001 |
| 93.56 | Application of pressure dressing | 256 | 7.5 | 172 | 8.5 | 84 | 6.1 | 67.2 | 41.1 | 0.009 |
| 93.54 | Application of splint | 225 | 6.6 | 193 | 9.6 | 32 | 2.3 | 85.8 | 42.3 | <0.00001 |
| 99.99 | Other | 220 | 6.5 | 141 | 7.0 | 79 | 4.8 | 64.1 | 40.8 | NS |
| 86.04 | Other incision with drainage of skin and subcutaneous tissue | 213 | 6.3 | 158 | 7.8 | 55 | 4.0 | 74.2 | 41.4 | <0.00001 |
| 79.67 | Debridement of open fracture site (tarsal/MT) | 185 | 5.5 | 184 | 9.1 | 1 | <0.1 | 99.5 | 42.8 | <0.00001 |
| 88.48 | Arteriography of femoral and other lower extremity arteries | 180 | 5.3 | 152 | 7.5 | 28 | 2.0 | 84.4 | 41.9 | <0.00001 |
| 99.07 | Transfusion of other serum | 166 | 4.9 | 107 | 5.3 | 59 | 4.3 | 64.5 | 40.7 | NS |
| 04.81 | Injection of anesthetic into peripheral nerve for analgesia | 160 | 4.7 | 117 | 5.8 | 43 | 3.1 | 73.1 | 41.1 | 0.0003 |
| Limb Salvage? | SME Classification | ||
|---|---|---|---|
| Yes | No | ||
| Data-Driven Classification | Yes | n = 15 | n = 12 |
| No | n = 3 | n = 20 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goldman, S.M.; Eskridge, S.L.; Franco, S.R.; Souza, J.M.; Tintle, S.M.; Dowd, T.C.; Alderete, J.; Potter, B.K.; Dearth, C.L. A Data-Driven Method to Discriminate Limb Salvage from Other Combat-Related Extremity Trauma. J. Clin. Med. 2023, 12, 6357. https://doi.org/10.3390/jcm12196357
Goldman SM, Eskridge SL, Franco SR, Souza JM, Tintle SM, Dowd TC, Alderete J, Potter BK, Dearth CL. A Data-Driven Method to Discriminate Limb Salvage from Other Combat-Related Extremity Trauma. Journal of Clinical Medicine. 2023; 12(19):6357. https://doi.org/10.3390/jcm12196357
Chicago/Turabian StyleGoldman, Stephen M., Susan L. Eskridge, Sarah R. Franco, Jason M. Souza, Scott M. Tintle, Thomas C. Dowd, Joseph Alderete, Benjamin K. Potter, and Christopher L. Dearth. 2023. "A Data-Driven Method to Discriminate Limb Salvage from Other Combat-Related Extremity Trauma" Journal of Clinical Medicine 12, no. 19: 6357. https://doi.org/10.3390/jcm12196357
APA StyleGoldman, S. M., Eskridge, S. L., Franco, S. R., Souza, J. M., Tintle, S. M., Dowd, T. C., Alderete, J., Potter, B. K., & Dearth, C. L. (2023). A Data-Driven Method to Discriminate Limb Salvage from Other Combat-Related Extremity Trauma. Journal of Clinical Medicine, 12(19), 6357. https://doi.org/10.3390/jcm12196357