Abstract
Background: Percutaneous treatment for primary aneurysmal bone cysts (ABCs) has been widely accepted. The study aimed to evaluate the efficacy of various sclerotherapy agents on patients with primary ABCs. Methods: A meta-analysis of relevant studies. A systematic search was conducted on five databases, resulting in the inclusion of 25 studies with different percutaneous agents. Results: A total of 729 patients with primary ABCs were included. Patients were administered with Ethibloc, doxycycline, embolization, alcohol, polidocanol, and calcitonin with methylprednisolone, respectively. Overall, 542 (74.3%) patients with ABCs had complete healing, 120 (16.4%) had partial healing, 44 (6%) had no-ossification or failure, and 26 (3.5%) had a recurrence. However, there was a total of 45 (6.1%) patients who had surgical curettage after sclerotherapy. Among the sclerotherapy agents, doxycycline showed highly effective results with minimal complications and recurrence, but it required multiple injections per patient. Ethibloc and embolization also proved to be highly effective with fewer injections required but had a higher rate of complications. Absolute alcohol, polidocanol, and calcitonin with methylprednisolone had similar efficacity and favorable success with fewer complications and fewer injections. Conclusion: Percutaneous treatment showed promising results in treating primary ABCs. However, more robust research is needed to establish the best approach for sclerotherapy in clinical practice and to address the limitations of the current literature.
Keywords:
aneurysmal bone cysts; injection; doxycycline; Ethibloc; sclerotherapy; embolization; polidocanol; calcitonin 1. Introduction
Aneurysmal bone cysts (ABCs) were first defined in 1942 by Jaffe and Lichtenstein as self-destructive, benign, and locally aggressive bone growing tumor, which accounts for 1% of all bone tumors [1,2]. ABCs commonly occurs in children or adolescents, and most of the lesions appear before the age of 30 years [2]. The prevalence of ABCs is 1.4 per 100,000. The symptoms observed with this lesion are pain, swelling, deformity, and pathological fracture in severe cases [3]. The diagnosis is initially made using radiographic imaging, but the final and definitive diagnosis is confirmed through histopathology [4,5].
ABC treatment modalities can be subdivided broadly into three categories such as surgical, percutaneous, and others. Surgical treatment includes intralesional curettage with or without adjuvants (high-speed burr, argon beam, phenol, en bloc resection) [6,7]. Percutaneous treatment includes embolization or sclerotherapy. Other treatment modalities include radiation therapy, radionuclide ablation, or the systemic application of bisphosphonates or denosumab [8].
While surgical treatment is generally considered the standard approach for ABCs, it can present challenges in specific locations like the axial spine. Among children, the operative complications following curettage or surgical intervention are notably high [3,9,10]. Moreover, the recurrence rate after surgical treatment ranges from 18% to 59% [6,11].
Currently, percutaneous sclerotherapy and embolization for ABCs are widely accepted alternative treatments for primary ABCs or recurrent ABCs after previous surgical treatment, as they are associated with decreased morbidity and recurrence rates. Studies have reported a recurrence of 5–6% within a period of 18–24 months [3,9]. Studies have suggested that percutaneous treatment can be used as a first line of treatment or as an accepted alternative to surgery as it has been demonstrated to have many advantages over conventional surgery, including lower complications and morbidity and better functional outcomes, with a comparable healing rate [3,9,11].
Embolization is a minimally invasive procedure that blocks the arterial supply to a tumor using variable agents. It can be used as an adjuvant to decrease hemorrhage, or as an alternative treatment. It is usually performed under local anesthesia, but general anesthesia may be used. There have been few postoperative complications reported, and the most important ones are bleeding, infection, and nerve damage [2,12].
In the current literature, there are many agents have been described as sclerotherapy agents including polidocanol, doxycycline, calcitonin with methylprednisolone, absolute alcohol, and Ethibloc [13,14,15,16].
Despite the wide range of agents utilized in treatments, there is a shortage of literature comparing percutaneous treatment options to determine the most effective approach. Therefore, this systematic review and meta-analysis systematically provides evidence to determine the effectiveness of different sclerotherapy agents and embolization in treating primary ABCs. This study also presents evidence on recurrence rates, complication rates, types of complications, and the number of injections required for the treatment of ABCs with each sclerotherapy intervention.
2. Materials and Methods
2.1. Searching
A comprehensive systematic search was conducted in 5 databases, PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), Clinicaltrials.eu, Clinicaltrials.gov, and ICTRP, using the search terms ‘aneurysmal bone cyst’, ‘sclerotherapy’, ‘embolization’, ‘Ethibloc’, ‘polidocanol’, ‘doxycycline’, ‘alcohol’, ‘calcitonin’, and ‘calcitonin with methylprednisolone’. The search terms were combined using Boolean operators. Back reference searching was also conducted from previous systematic review papers. The search was restricted to the English language and citations published after the year 2000.
2.2. Selection and Screening
A two-stage screening was conducted. First, the title and abstract were screened, followed by full-text screening using predesigned inclusion and exclusion criteria. The inclusion criteria for the study were based on the PICO format.
Inclusion criteria:
- Population: Studies that had primary percutaneous ABC treatments in which interventions were evaluated with a mean follow-up period of at least 18 months.
- Intervention: Studies that used embolization, doxycycline/albumin, calcitonin with methylprednisolone, alcohol, Ethibloc, or polidocanol for treating primary ABCs.
- Comparator: Studies comparing any sclerotherapy agents, either using surgical or no intervention.
- Outcome: Complete healing, partial healing, failure, recurrence, number of injections administered for healing, and complications.
- Studies: Retrospective or prospective studies, RCTs, clinical trials. In studies with multiple intervention groups, only patients administered any sclerotherapy agents or embolization would be selected.
- Language: English.
- Time: Published from 2000 to 2021.
Exclusion criteria:
- Population: Studies that had primary percutaneous ABC treatments and evaluations of interventions with a mean follow-up period less than 18 months. Studies assessing secondary ABCs.
- Intervention: Studies that used any sclerotherapy as secondary treatment for primary ABCs, surgical therapy, non-injection therapy, or only mixed treatments.
- Comparator: Studies comparing other modalities apart from our interventions of interest.
- Outcome: Other outcomes apart from our interventions of interest.
- Studies: Case reports, letters, narrative reviews, or systematic reviews.
- Language: Non-English.
- Time: Studies published before 2000.
2.3. Data Extraction and Quality Assessment
Complete data extraction and quality assessment based on the study types were conducted. Data were extracted regarding the country published in, study setting, population type, sample size, treatment, ABC site, follow-up time, age, number of injections, complete ossification or healing, partial ossification, recurrence, failure, post-therapy surgery, and complications. In case studies with multiple interventions, data have been reported and extracted separately. For the quality assessment, the NIH study quality assessment tool was used for case series studies, before–after studies with no control group, and controlled trials studies. Each type of tool used with the studies has its domain of tool in which overall studies are marked as low-, fair-, or good-quality studies [17]. A quality score was provided for the selected studies on a scale of 0 to 14, with 0 representing a study that failed to meet any criteria and 14 signifying a study that did meet all the criteria. The total number of points revealed a study’s overall quality. The quality of the studies was rated as being low (scoring < 4), fair (5–8), or good (>8).
2.4. Narrative Synthesis and Meta-Analysis
Following data extraction and quality assessment, narrative synthesis was conducted. An overall narrative synthesis was performed based on the studies. The synthesis was performed based on the various types of sclerotherapies and embolization used compared with complications, overall complete healing, and number of injections used for complete or partial healing. A meta-analysis was also performed using the random-effect model, and the proportion of the effect (event rate) and the 95% confidence interval (95% CI) were calculated. Heterogeneity among the studies was checked using the degree of heterogeneity (I2 statistics) and a forest plot. An I2 more than 75% is considered high heterogeneity, and less than 25% is considered low heterogeneity. A subgroup analysis of different sclerotherapy and embolization therapies was conducted. All the meta-analyses were performed using the Openmetaanalyst software (OpenMeta[Analyst], version 3.X).
3. Results
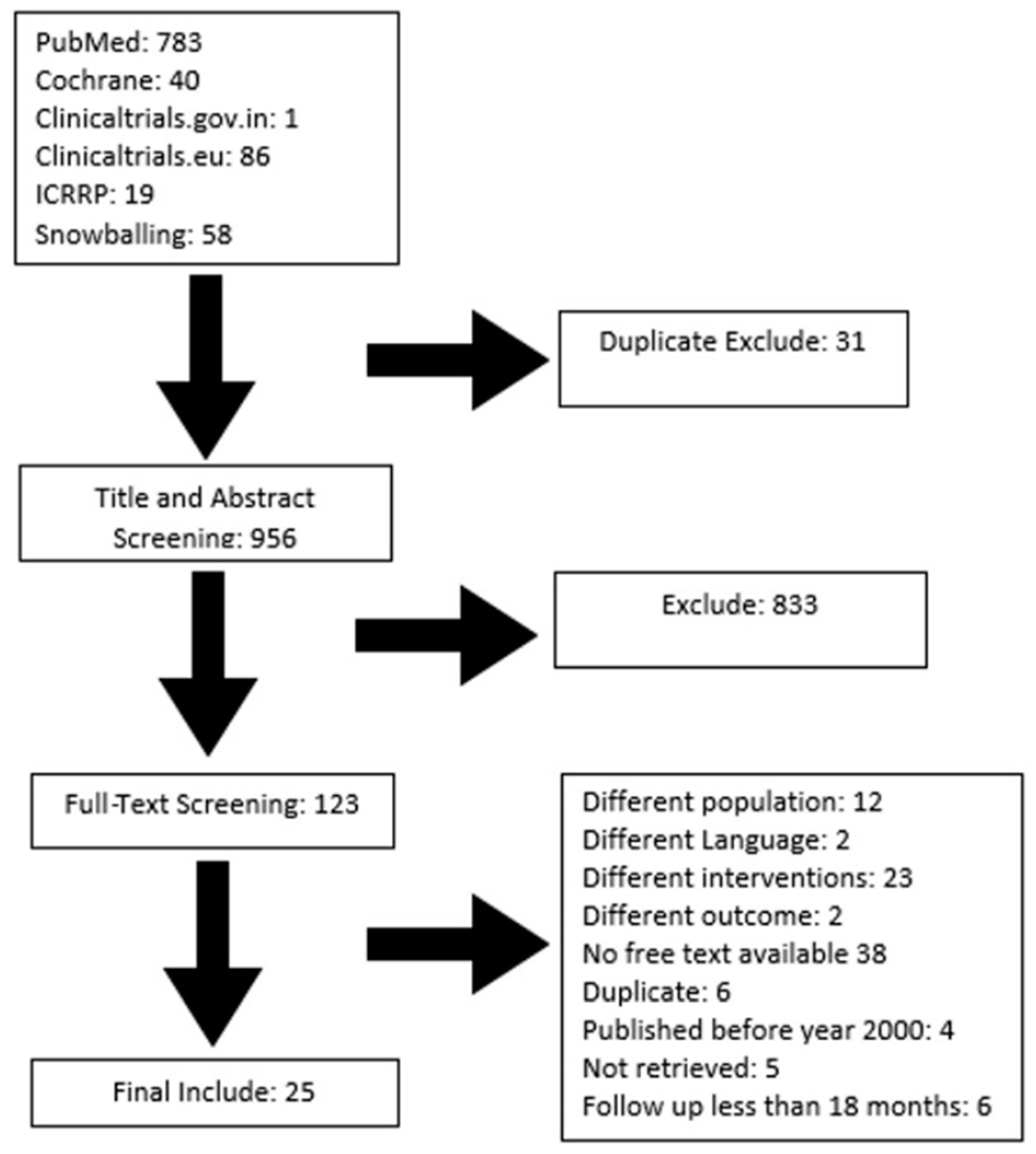
The study was conducted according to the PRISMA guidelines. Following the search of PUBMED, Cochrane, and clinical trial sites, 987 citations were retrieved, out of which 25 studies were included using our pre-designed inclusion and exclusion criteria, as shown in Figure 1. Overall, 729 patients with primary ABCs were included for analysis. A total of 118 patients were administered injection (Inj.) Ethibloc, 57 patients were administered Inj. doxycycline, 110 patients were treated with embolization, 83 patients were administered Inj. alcohol, 314 patients were administered Inj. polidocanol, and 47 patients were administered a combination of calcitonin with methylprednisolone as shown in Table 1.
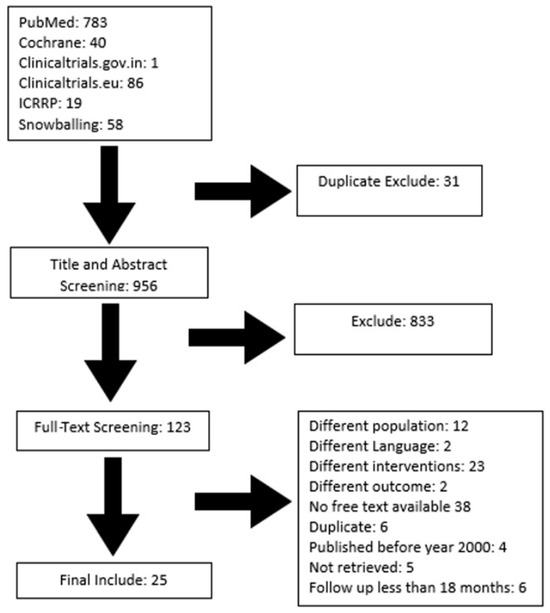
Figure 1.
PRISMA diagram for selection of studies.

Table 1.
Study characteristics.
3.1. Study Characteristics
The majority of the studies were retrospective, with only one randomized control trial and one prospective study included. The characteristics of the studies are detailed in Table 1. In terms of age, the majority of the studies included patients aged below 18 years old, with a mean age of 12.9 years (±3.7). The location of the lesion varied among the patients and included the humerus, pelvis, femur, spine, and other locations. The mean least follow-up observed was 25.5 months, and the longest follow-up observed was 84 months, with details of patient characteristics outlined in Table 2. The study quality was assessed using the NIH quality assessment tool for case studies as shown in Table 1. The quality of all included studies was assessed independently by two authors, and it was observed that 7 studies were of poor quality, 11 studies were of fair quality, and 7 studies were of good quality.
Table 2.
Patient characteristics.
3.2. Study Outcomes
Study outcome data were extracted based on complete ossification or more than 75% healing, partial ossification, no-ossification or failure, recurrence, post-therapy surgical treatment, complications, and number of injections required to be administered.
Overall, 74.3% patients (n = 542) with ABCs had complete healing or more than 75% reduction in cyst volume, 16.4% patients (n = 120) with ABCs had partial healing (25 to 75% reduction in cyst volume), 6% patients (n = 44) with ABCs had no-ossification or failure, and 3.56% patients (n = 26) with ABCs had a recurrence. However, there was a total of 6.1% patients (n = 45) who had surgical curettage after sclerotherapy (Table 3).
Table 3.
Study outcomes.
3.3. Narrative Synthesis
The highest complete healing rate was observed in the doxycycline/albumin group, at 95% (n = 54), while the lowest was in the polidocanol group, at 70.4% (n = 221). Among the embolization group, the healing rate was 79% (n = 87). We found that the highest complication rate was among those who received an Ethibloc injection, at 52.5% (n = 62). However, in the calcitonin with methylprednisolone group, no patients presented with any complications.
Overall, the main complications observed in all the intervention groups were fever, indurations, skin rash, skin necrosis, edema, cutaneous fistula, and pain, as shown in Table 4. The recurrence rate varied among the various intervention groups, with 14.5% (n = 16) in the embolization group and no recurrence observed in the alcohol and calcitonin with methylprednisolone groups. Outcomes are detailed in Table 4.
Table 4.
Outcomes across the intervention groups.
There was a lot of heterogeneity among the number of injections administered among various interventions or sclerotherapy groups as shown in Table 5. The mean number of injections required across all the sclerotherapy groups for complete or partial healing was 1.35 [1 to 4] in the Ethibloc group, 3.95 [1 to 14] in the doxycycline/albumin group, 1.6 [1 to 7] in the embolization group, 1.7 [1 to 4] in the alcohol group, 2.8 [1 to 12] in the polidocanol group, and 2.8 [1 to 7] in the calcitonin with methylprednisolone group.
Table 5.
Number of injections across the intervention groups.
3.4. Meta-Analysis
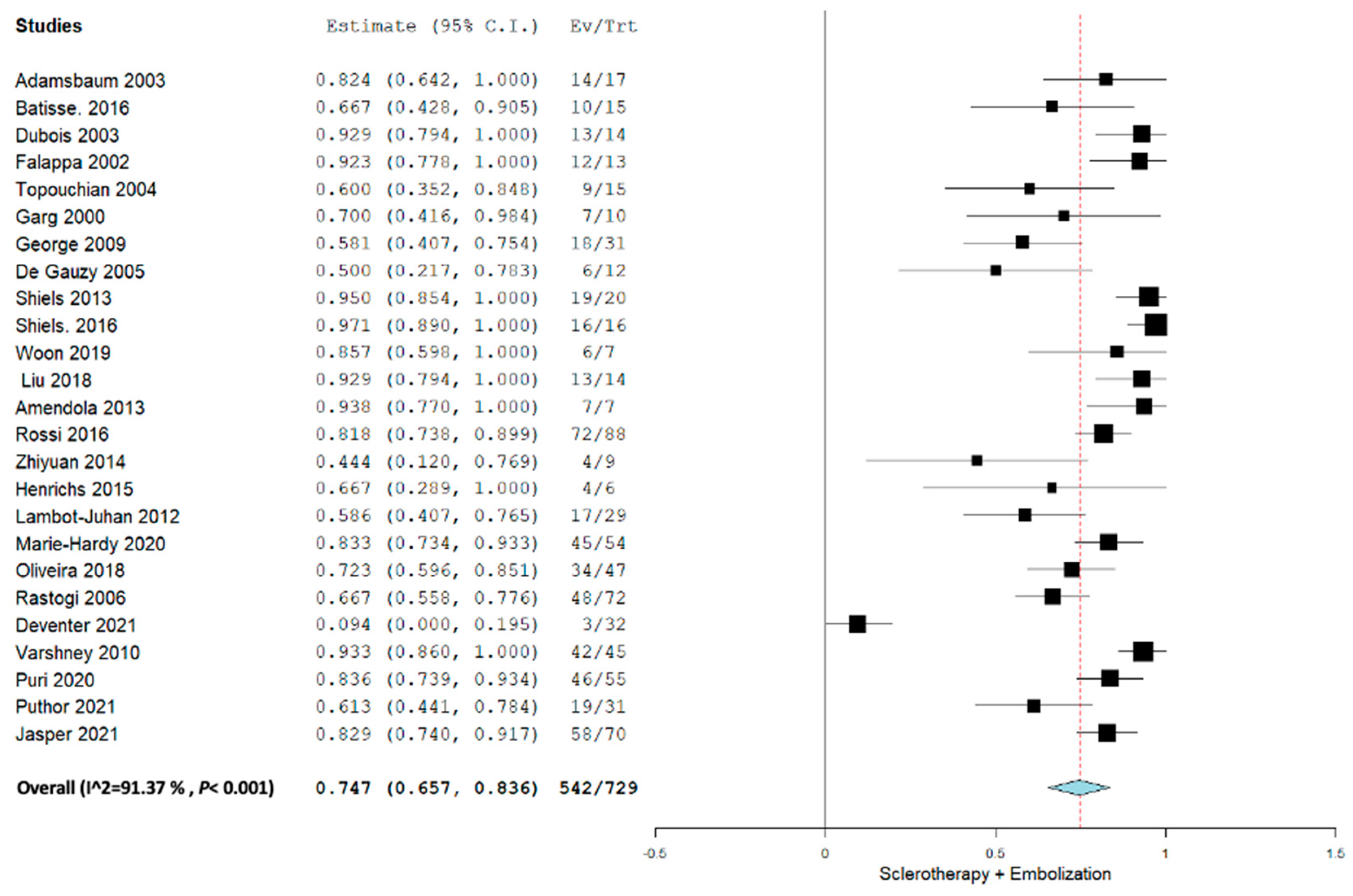
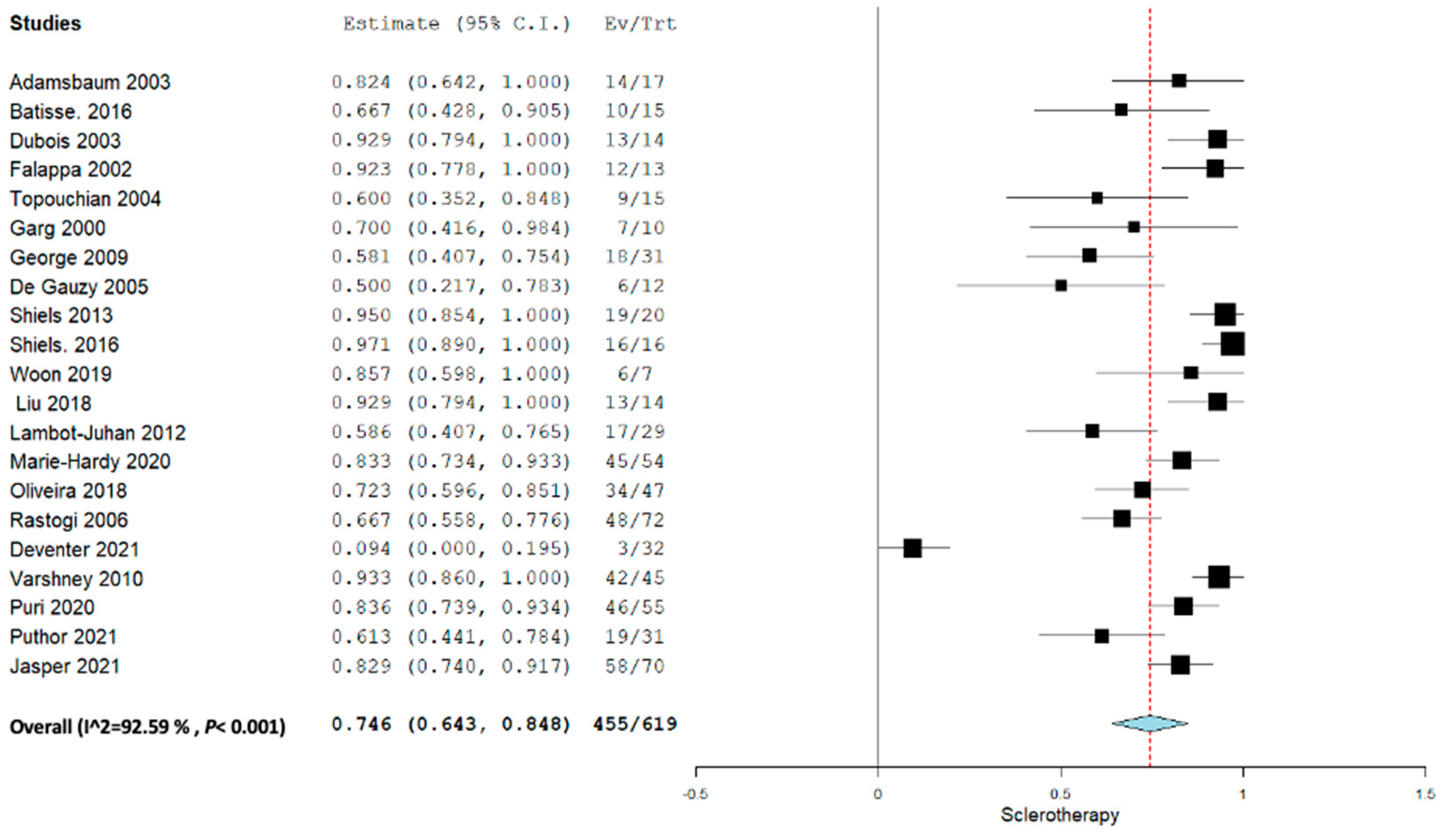
Applying the random effect model, the overall pooled proportion size for complete healing for all the sclerotherapy and embolization agents was 0.747 (95% CI, 0.657–0.836) with a heterogeneity of 91.37% as shown in Figure 2. The overall pooled proportion for only sclerotherapy agents was 0.746 (95% CI, 0.643–0.848) with a heterogeneity of 92.59%.
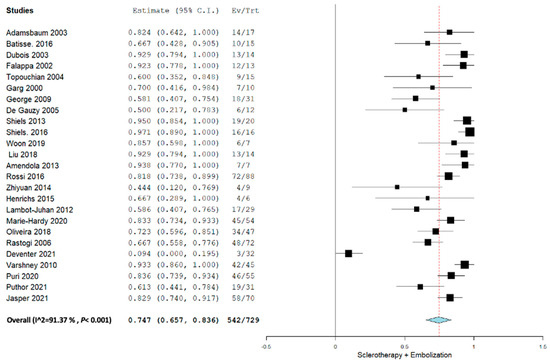
Figure 2.
Overall pooled efficacy of all sclerotherapies + embolization.
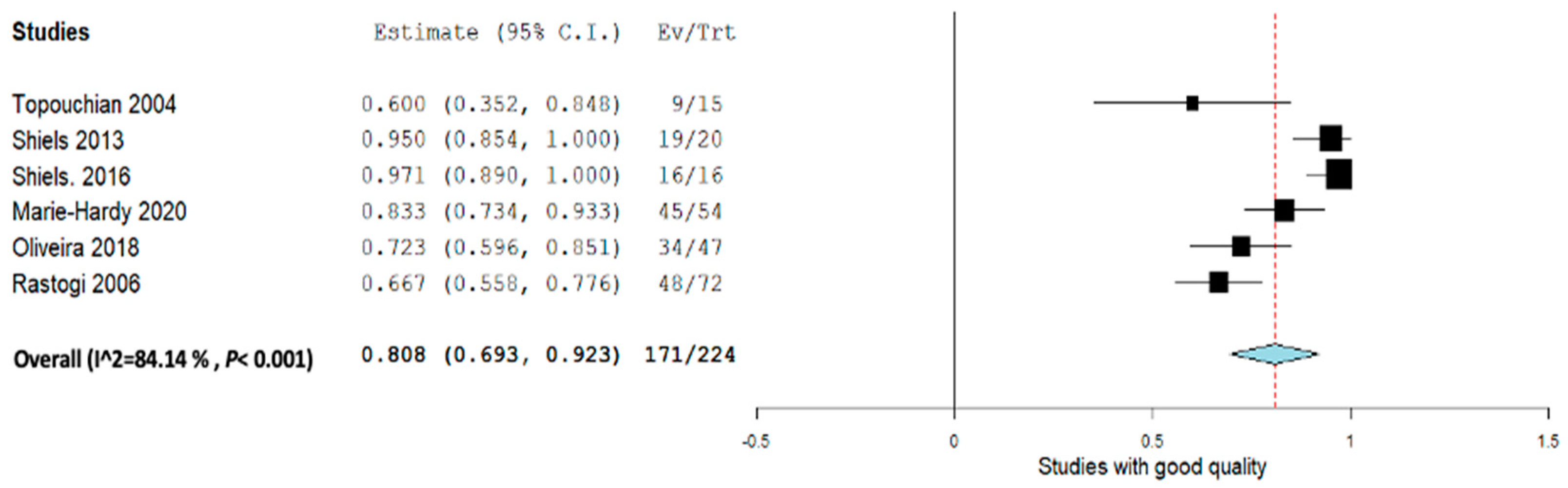
Excluding the poor- and fair-quality studies while taking into consideration the good-quality studies, the overall pooled proportion size for complete healing for all the sclerotherapies was 0.808 (95% CI,0.693–0.923) with a heterogeneity of 84.14% as shown in Figure 3. Overall, all sclerotherapy showed significant effectiveness but with a high amount of heterogeneity even after sensitivity analysis, and thus the results should be used with caution (Figure 4).
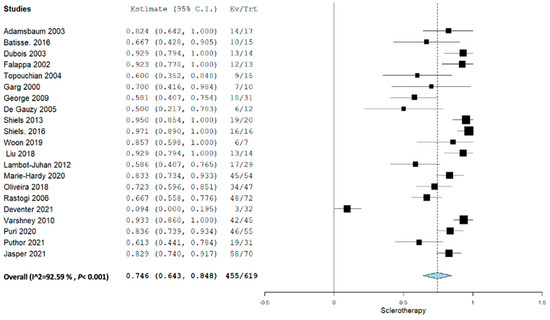
Figure 3.
Overall pooled efficacy of all sclerotherapies.
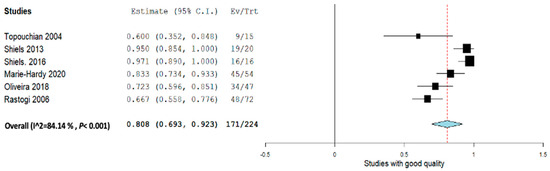
Figure 4.
Overall pooled efficacy among good-quality studies.
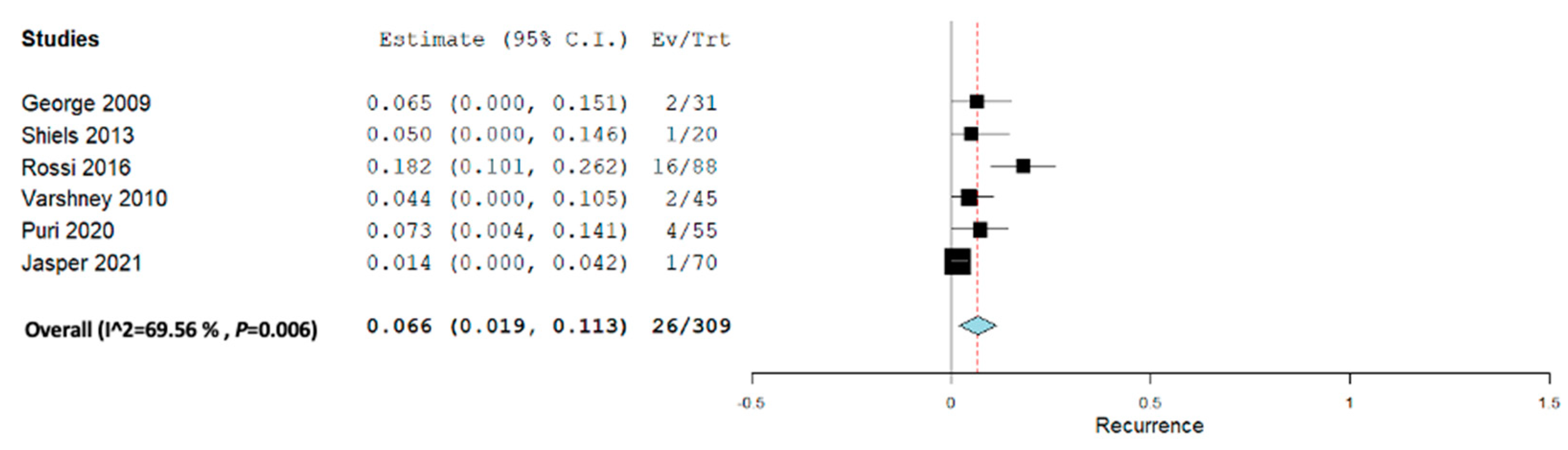
The recurrence rate as shown in Figure 5 showed significantly low recurrence with a medium amount of heterogeneity among the studies. The pooled recurrence rate was 0.66 (95% CI, 0.019–0.113) with a heterogeneity of 69.56%.
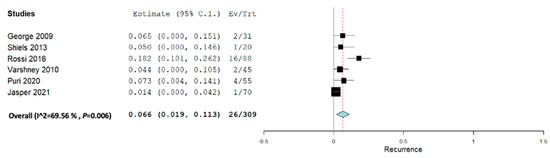
Figure 5.
Overall pooled recurrence all sclerotherapies + embolization.
3.5. Subgroup Analysis
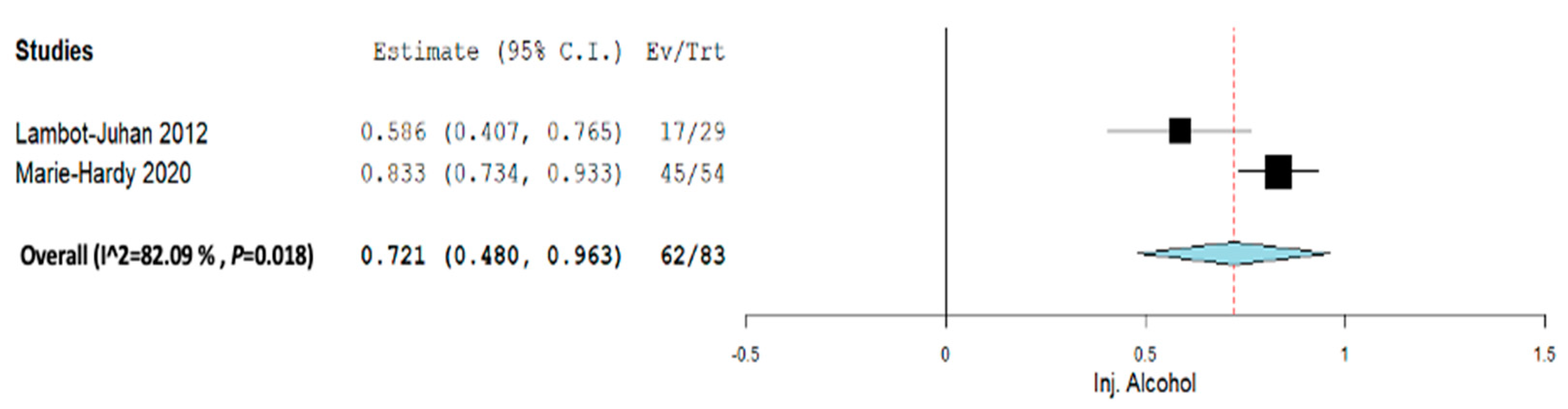
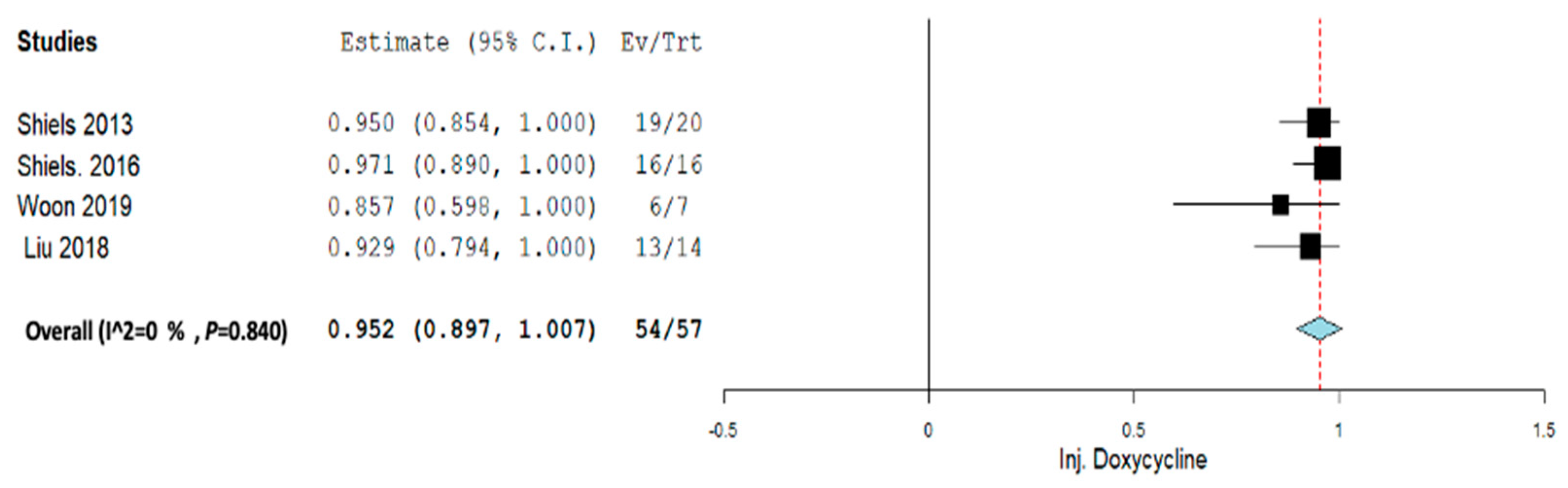
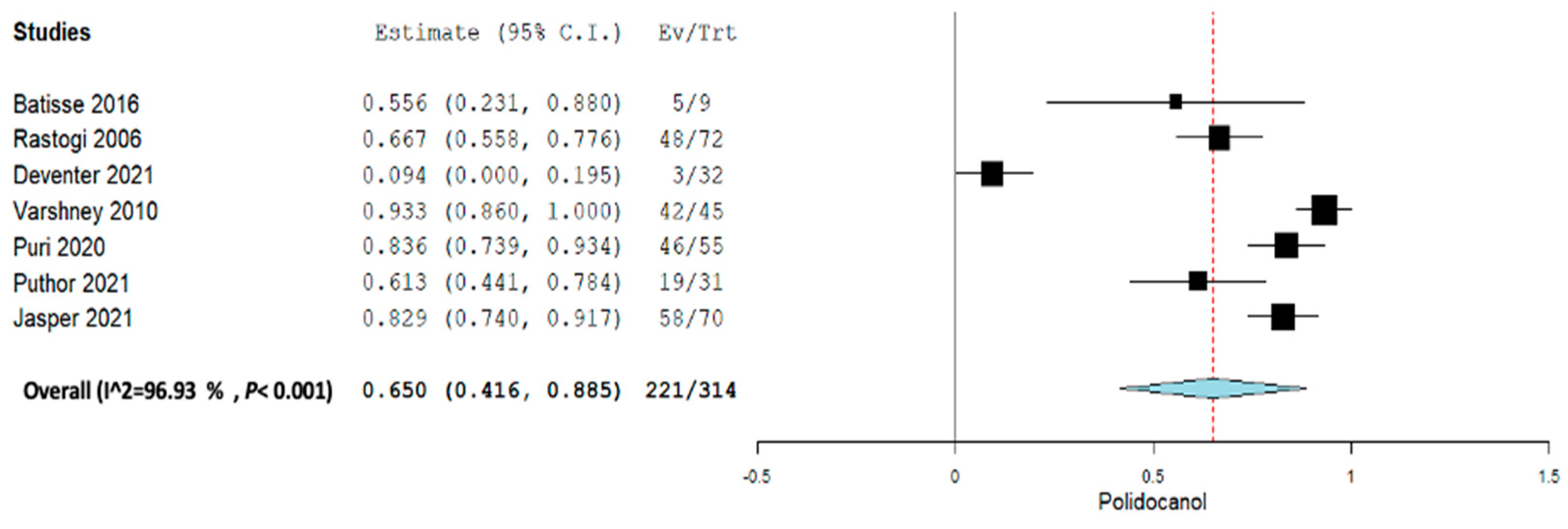
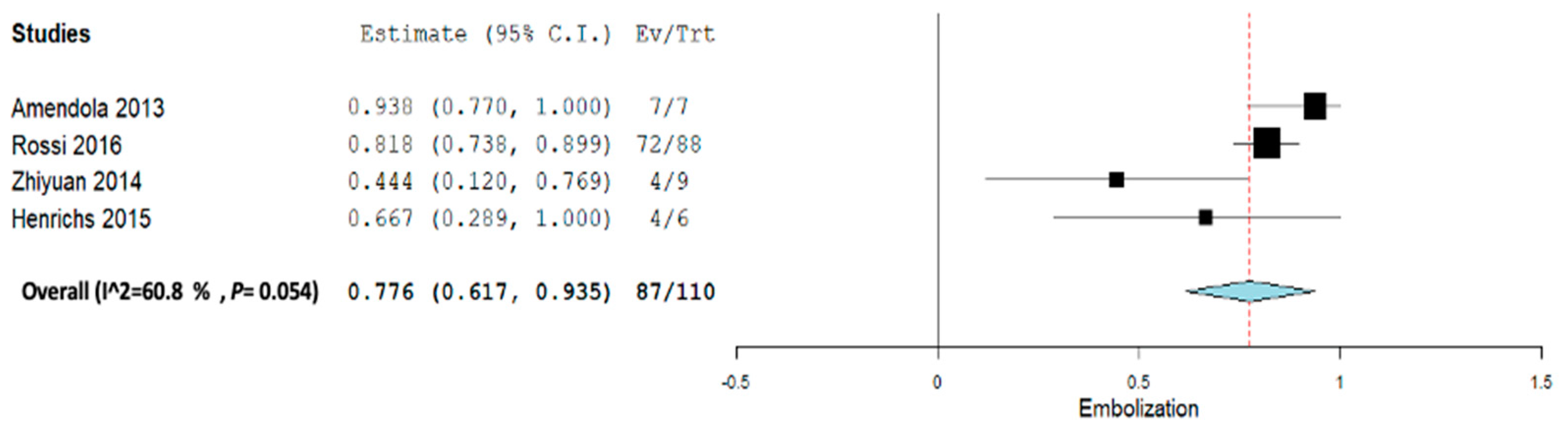
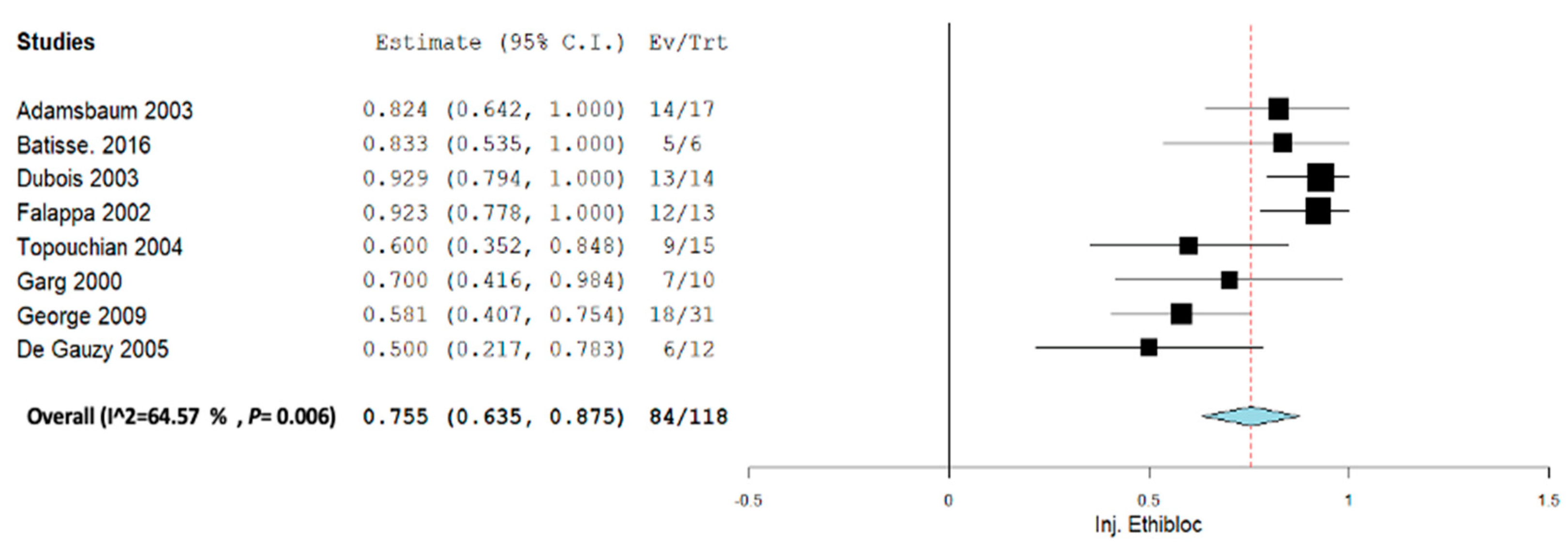
Subgroup analysis was performed across each intervention for Inj. alcohol, Inj. doxycycline, Inj. Polidocanol, and embolization. Across all the subgroup analyses, a random-effect model was used. In the Inj. alcohol group, the pooled proportion size for complete healing was 0.721 (95% CI, 0.480–0.963) with a heterogeneity of 82.09% as shown in Figure 6. In the Inj. doxycycline group, the pooled proportion size for complete healing was 0.952 (95% CI, 0.897–1.007) with a heterogeneity of 0% as shown in Figure 7. In the Inj. polidocanol group, the pooled proportion size for complete healing was 0.650 (95% CI, 0.416–0.885) with a heterogeneity of 96.93% as shown in Figure 8. In the embolization group, the pooled proportion size for complete healing was 0.776 (95% CI, 0.617–0.935) with a heterogeneity of 60.8% as shown in Figure 9. In the Inj. Ethibloc group, the pooled proportion size for complete healing was 0.755 (95% CI, 0.635–0.875) with a heterogeneity of 64.57% as shown in Figure 10.
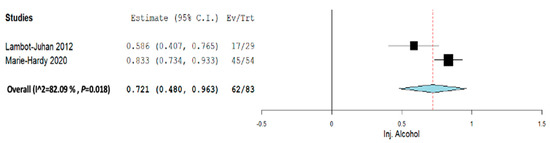
Figure 6.
Overall pooled efficacy for Inj. alcohol.
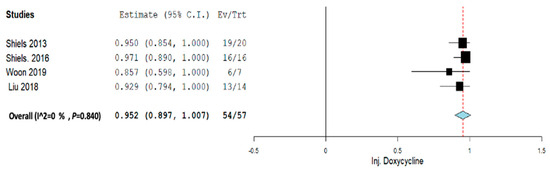
Figure 7.
Overall pooled efficacy for Inj. doxycycline.
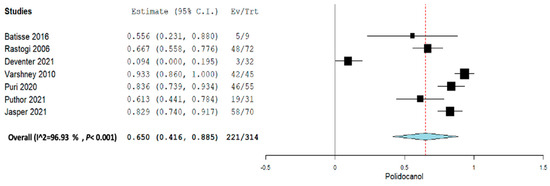
Figure 8.
Overall pooled efficacy for Inj. polidocanol.
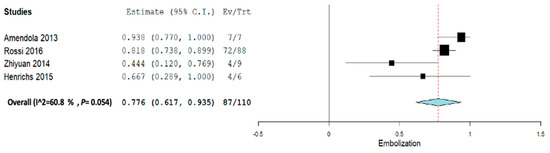
Figure 9.
Overall pooled efficacy for embolization therapy.
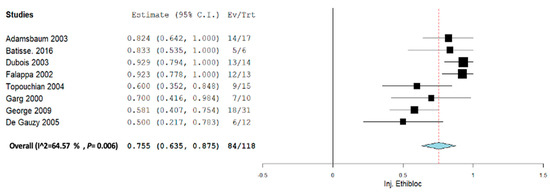
Figure 10.
Overall pooled efficacy for Inj. Ethibloc.
Overall, all five sclerotherapy interventions showed significant effectiveness in terms of complete healing. However, due to the high amount of heterogeneity in the polidocanol and alcohol groups and the moderate amount of heterogeneity in the embolization group and Ethibloc group, the effectiveness must be taken into consideration with caution. The Inj. doxycycline group showed highly effective results with the least amount of heterogeneity.
During the analysis of subgroups, the group involving calcitonin with methylprednisolone injection was not considered as a subgroup. This decision was made because there was only one study included in this meta-analysis, and it had a limited number of patients. However, after conducting a search, we found two more studies. Unfortunately, these additional studies did not meet our inclusion criteria.
4. Discussion
Percutaneous treatment of aneurysmal bone cysts (ABCs) is considered a favorable alternative to conventional therapy, yielding comparable outcomes but with a less challenging operative technique and, consequently, fewer complications. Nevertheless, numerous agents are employed as sclerosing agents, each exhibiting varying degrees of efficacy [38].
This meta-analysis aims to assess the clinical effectiveness of sclerotherapy for primary ABC patients. While previous systematic reviews and meta-analyses have been conducted [11,38,39,40], this updated meta-analysis was necessitated by concerns regarding publication bias. Additionally, this review specifically examines complications associated with different types of sclerotherapies and the number of injections required for ABC healing.
Overall, sclerotherapy has proven to be effective in reducing the size of cysts as well as healing tumors. The previous systematic review showed efficacious results in healing tumors [3,11]. The meta-analysis showed significant results overall regarding the healing rates of ABCs. Upon conducting the sensitivity analysis, sclerotherapy still possessed significant results. The overall pooled proportion of complete healing for all sclerotherapy and embolization treatments was 0.747 (95% CI, 0.657–0.836), which means that about 75% of patients healed completely. However, we found that there was high heterogeneity between the studies, meaning that there was a lot of variation in the results of the studies. This heterogeneity could be due to differences in the patient populations, treatments, or methods used in the studies.
In our study, the overall recurrence rate after an 18-month follow-up period was 3.4%. It is worth noting that the surgical technique, which is considered the gold standard treatment for ABCs, has a recurrence rate ranging from 18% to 59%, primarily attributed to incomplete cyst removal [10]. In contrast, across all the sclerotherapy methods, the overall complication rate was 20%. Sclerotherapy offers several advantages, including lower morbidity, accessibility in challenging surgical access areas, reduced technique sensitivity, and greater compatibility with patients [3,10,11]
In the doxycycline/albumin injection group, impressive efficacy rates were observed, with a 94.7% rate of complete healing and a mere 1.7% recurrence rate. However, it is noteworthy that the complication rate stood at 3.5%, with the primary complication being focal skin necrosis. Despite its effectiveness and low recurrence rate, there is one drawback regarding its utilization; it necessitates a mean of 3.5 injections, with a maximum of 14 injections required, which is considered a significant limitation.
Both polidocanol and alcohol agents have shown promising results, with efficacies of 70.6% and 74.6%, respectively, and low recurrence rates. These agents are considered safe due to their mild complication profiles compared to others. Furthermore, when compared to doxycycline, both require a lower number of injections, with a mean of 2.8 injections for polidocanol and 1.7 for alcohol. However, it is worth noting that the efficacy of polidocanol could potentially be improved by excluding the article by Deventer et al., as it appears to be an outlier in this meta-analysis. In most other articles, the efficacy rates are notably higher, such as those by Jasper et al. (83%), Rastogi et al. (97%), Varshney et al. (98%), Puri et al. (82%), and Puthoor et al. (100%). Embolization has shown good results with 79% efficacity, but there was a 14.5% recurrence rate, and the complication rate was 4.5% with observation of major complications such as paralysis. It essential to consider that the bulk of the patients in these studies had axial spine ABCs.
This study also found out that the highest rate of complications was about 52% for the Ethibloc group while the rest of the sclerotherapy agents and the embolization group had complication rates less than 20%. Most of the complications across the various therapies included fever, pain, induration, swelling, and serious local complications such as skin necrosis and cutaneous fistula. Most of the local adverse events seen were due to uneven distribution of the sclerotherapy agents, which leads to incomplete cure and can be minimized using proper biopsy and radiographic techniques [10]. Ethibloc has been withdrawn from the market and is no longer approved by the FDA due to its severe side effects, such as pulmonary embolism [22,38]. The least or negligible recurrences were observed for the alcohol, doxycycline/albumin, and calcitonin with methylprednisolone Inj. groups and were very low compared to recurrences for surgical techniques. The mean number of injections required for healing or complete ossification is 2.15 among the sclerotherapy agents and 1.6 for embolization therapy. The highest number of injections were required among the doxycycline/albumin group, ranging from 1 to 14 injections with an average of 3.95 injections. Due to the high numbers of injections, this sclerotherapy agent is not accepted as the only mode of treatment. However, it has been suggested to use sclerotherapy in most inaccessible surgical areas [10].
This study also had strengths and weaknesses in terms of study methodology. First, a robust search was conducted in all five databases followed by strict screening using the inclusion and exclusion criteria. Moreover, the study mean follow-up timing was set to at least 18 months, as most recurrences of ABCs occur between 18 and 24 months [10,18]. This criterion would lead us to find evidence regarding the recurrence of ABCs following sclerotherapy. Another key strength of the study was that quality checking of all the studies was conducted and taken into consideration while assessing their efficacy. On the other hand, all steps of this review process were conducted by a single reviewer, and no authors were contacted during the review process. However, to minimize bias, each and every step was double-checked. Secondly, most of the studies included in this review were case studies and retrospective studies. According to the hierarchy of evidence, RCTs and clinical trials provide very good clinical evidence. Lastly, the presence of substantial heterogeneity among the included studies is a significant limitation in our analysis. We recognize the importance of exercising caution when interpreting our results due to this observed heterogeneity. Heterogeneity can introduce variability into the findings, potentially influencing the overall reliability of our conclusions. To address this issue, we conducted a subgroup analysis aimed at exploring potential sources of heterogeneity. However, it is important to note that despite these efforts, some level of heterogeneity may persist. This is largely due to the inherent diversity among the included studies in terms of study design, population, and other factors that influence outcomes.
5. Conclusions
Overall, excluding the heterogeneity among studies and the study types, sclerotherapy was highly effective in controlling or healing ABCs with minimal complications and a low recurrence rate. In particular, doxycycline/albumin provided very good evidence for controlling ABCs, and it can be used in clinical practices with minimal or negligible complications, failures, and recurrence rates, but it required at least two injections for complete healing. Embolization, on the other hand, showed high healing rates with minimal complications and recurrence and no failure rates, but it was less effective compared to sclerotherapy. However, other sclerotherapy interventions should be used with caution in clinical practices, as strong evidence is lacking to support the efficacy of these interventions. Thus, good quality RCTs or clinical trials are required to determine the clinical effectiveness of sclerotherapy and its application in the clinical setting as a definitive treatment for ABCs.
Author Contributions
R.S.: study design and conceptualization, original draft preparation, review, and editing. M.A.: manuscript editing and review and data acquisition and curation. K.A.: manuscript editing and review and data acquisition and curation. M.B.: manuscript editing and review and data acquisition and curation. O.I.: methodology, formal analysis, and manuscript editing. Q.N.: methodology, formal analysis, and manuscript editing. B.H.: manuscript editing and review. J.B.: study design and conceptualization, manuscript review, editing, and supervision. L.-R.L.N.: study design and conceptualization, manuscript review, editing, and supervision. All authors reviewed and approved the final submitted version. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors have no conflict of interest regarding the present study.
References
- Deventer, N.; Schulze, M.; Gosheger, G.; de Vaal, M.; Deventer, N. Primary Aneurysmal Bone Cyst and Its Recent Treatment Options: A Comparative Review of 74 Cases. Cancers 2021, 13, 2362. [Google Scholar] [CrossRef]
- Amendola, L.; Simonetti, L.; Simoes, C.E.; Bandiera, S.; De Iure, F.; Boriani, S. Aneurysmal Bone Cyst of the Mobile Spine: The Therapeutic Role of Embolization. Eur. Spine J. 2013, 22, 533–541. [Google Scholar] [CrossRef]
- Bavan, L.; Wijendra, A.; Kothari, A. Efficacy of Treatment Interventions for Primary Aneurysmal Bone Cysts: A Systematic Review. Bone Jt Open 2021, 2, 125–133. [Google Scholar] [CrossRef]
- Cottalorda, J.; Bourelle, S. Modern Concepts of Primary Aneurysmal Bone Cyst. Arch. Orthop. Trauma Surg. 2007, 127, 105–114. [Google Scholar] [CrossRef]
- Gutierrez, L.B.; Link, T.M.; Horvai, A.E.; Joseph, G.B.; O’Donnell, R.J.; Motamedi, D. Secondary Aneurysmal Bone Cysts and Associated Primary Lesions: Imaging Features of 49 Cases. Clin. Imaging 2020, 62, 23–32. [Google Scholar] [CrossRef]
- Park, H.Y.; Yang, S.K.; Sheppard, W.L.; Hegde, V.; Zoller, S.D.; Nelson, S.D.; Federman, N.; Bernthal, N.M. Current Management of Aneurysmal Bone Cysts. Curr. Rev. Musculoskelet. Med. 2016, 9, 435–444. [Google Scholar] [CrossRef]
- Muratori, F.; Mondanelli, N.; Rizzo, A.R.; Beltrami, G.; Giannotti, S.; Capanna, R.; Campanacci, D.A. Aneurysmal Bone Cyst: A Review of Management. Surg. Technol. Int. 2019, 35, 325–335. [Google Scholar]
- Restrepo, R.; Zahrah, D.; Pelaez, L.; Temple, H.T.; Murakami, J.W. Update on Aneurysmal Bone Cyst: Pathophysiology, Histology, Imaging and Treatment. Pediatr. Radiol. 2022, 52, 1601–1614. [Google Scholar] [CrossRef]
- Varshney, M.K.; Rastogi, S.; Khan, S.A.; Trikha, V. Is Sclerotherapy Better than Intralesional Excision for Treating Aneurysmal Bone Cysts? Clin. Orthop. Relat. Res. 2010, 468, 1649–1659. [Google Scholar] [CrossRef]
- Puthoor, D.; Francis, L.; Ismail, R. Is Sclerotherapy with Polidocanol a Better Treatment Option for Aneurysmal Bone Cyst Compared to Conventional Curettage and Bone Grafting? J. Orthop. 2021, 25, 265–270. [Google Scholar] [CrossRef]
- Cruz, G.S.; Cuevas-Suárez, C.E.; Saavedra, J.P.A.; Giorgis, R.; Teixeira, M.R.K.; Muniz, F.W.M.G. Percutaneous Treatments of Primary Aneurysmal Bone Cysts: Systematic Review and Meta-Analysis. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 1287–1295. [Google Scholar] [CrossRef]
- Rossi, G.; Mavrogenis, A.F.; Papagelopoulos, P.J.; Rimondi, E.; Ruggieri, P. Successful Treatment of Aggressive Aneurysmal Bone Cyst of the Pelvis With Serial Embolization. Orthopedics 2012, 35, e963–e968. [Google Scholar] [CrossRef]
- Protas, M.; Jones, L.W.; Sardi, J.P.; Fisahn, C.; Iwanaga, J.; Oskouian, R.J.; Tubbs, R.S. Cervical Spine Aneurysmal Bone Cysts in the Pediatric Population: A Systematic Review of the Literature. Pediatr. Neurosurg. 2017, 52, 219–224. [Google Scholar] [CrossRef]
- Ohashi, M.; Ito, T.; Hirano, T.; Endo, N. Percutaneous Intralesional Injection of Calcitonin and Methylprednisolone for Treatment of an Aneurysmal Bone Cyst at C-2: Case Report. J. Neurosurg. Pediatr. 2008, 2, 365–369. [Google Scholar] [CrossRef]
- Shiels, W.E.; Mayerson, J.L. Percutaneous Doxycycline Treatment of Aneurysmal Bone Cysts With Low Recurrence Rate: A Preliminary Report. Clin. Orthop. Relat. Res. 2013, 471, 2675–2683. [Google Scholar] [CrossRef]
- Wong, M.N.; Braswell, L.E.; Murakami, J.W. Doxycycline Sclerotherapy of Cervical Spine Aneurysmal Bone Cysts: Single-Institution 13-Year Experience. Pediatr. Radiol. 2022, 52, 1528–1538. [Google Scholar] [CrossRef]
- Study Quality Assessment Tools | NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 8 September 2023).
- Adamsbaum, C.; Mascard, E.; Guinebretière, J.M.; Kalifa, G.; Dubousset, J. Intralesional Ethibloc Injections in Primary Aneurysmal Bone Cysts: An Efficient and Safe Treatment. Skelet. Radiol. 2003, 32, 559–566. [Google Scholar] [CrossRef]
- Batisse, F.; Schmitt, A.; Vendeuvre, T.; Herbreteau, D.; Bonnard, C. Aneurysmal Bone Cyst: A 19-Case Series Managed by Percutaneous Sclerotherapy. Orthop. Traumatol. Surg. Res. 2016, 102, 213–216. [Google Scholar] [CrossRef]
- Dubois, J.; Chigot, V.; Grimard, G.; Isler, M.; Garel, L. Sclerotherapy in Aneurysmal Bone Cysts in Children: A Review of 17 Cases. Pediatr. Radiol. 2003, 33, 365–372. [Google Scholar] [CrossRef]
- Falappa, P.; Fassari, F.M.; Fanelli, A.; Genovese, E.; Ascani, E.; Crostelli, M.; Salsano, V.; Montanaro, A.; Di Lazzaro, A.; Serra, F. Aneurysmal Bone Cysts: Treatment with Direct Percutaneous Ethibloc Injection: Long-Term Results. Cardiovasc. Interv. Radiol. 2002, 25, 282–290. [Google Scholar] [CrossRef]
- Topouchian, V.; Mazda, K.; Hamze, B.; Laredo, J.-D.; Penneçot, G.-F. Aneurysmal Bone Cysts in Children: Complications of Fibrosing Agent Injection. Radiology 2004, 232, 522–526. [Google Scholar] [CrossRef]
- Garg, N.K.; Carty, H.; Walsh, H.P.; Dorgan, J.C.; Bruce, C.E. Percutaneous Ethibloc Injection in Aneurysmal Bone Cysts. Skelet. Radiol. 2000, 29, 211–216. [Google Scholar] [CrossRef]
- George, H.L.; Unnikrishnan, P.N.; Garg, N.K.; Sampath, J.S.; Bass, A.; Bruce, C.E. Long-Term Follow-up of Ethibloc Injection in Aneurysmal Bone Cysts. J. Pediatr. Orthop. B 2009, 18, 375–380. [Google Scholar] [CrossRef]
- de Gauzy, J.S.; Abid, A.; Accadbled, F.; Knorr, G.; Darodes, P.; Cahuzac, J.P. Percutaneous Ethibloc Injection in the Treatment of Primary Aneurysmal Bone Cysts. J. Pediatr. Orthop. B 2005, 14, 367–370. [Google Scholar] [CrossRef]
- Shiels, W.E.; Beebe, A.C.; Mayerson, J.L. Percutaneous Doxycycline Treatment of Juxtaphyseal Aneurysmal Bone Cysts. J. Pediatr. Orthop. 2016, 36, 205–212. [Google Scholar] [CrossRef]
- Woon, J.T.K.; Hoon, D.; Graydon, A.; Flint, M.; Doyle, A.J. Aneurysmal Bone Cyst Treated with Percutaneous Doxycycline: Is a Single Treatment Sufficient? Skelet. Radiol. 2019, 48, 765–771. [Google Scholar] [CrossRef]
- Liu, X.; Han, S.B.; Si, G.; Yang, S.M.; Wang, C.M.; Jiang, L.; Wei, F.; Wu, F.L.; Liu, X.G.; Liu, Z.J. Percutaneous Albumin/Doxycycline Injection versus Open Surgery for Aneurysmal Bone Cysts in the Mobile Spine. Eur. Spine J. 2019, 28, 1529–1536. [Google Scholar] [CrossRef]
- Rossi, G.; Mavrogenis, A.F.; Facchini, G.; Bartalena, T.; Rimondi, E.; Renzulli, M.; Andreone, A.; Durante, S.; Angelini, A.; Errani, C. How Effective Is Embolization with N-2-Butyl-Cyanoacrylate for Aneurysmal Bone Cysts? Int. Orthop. (SICOT) 2017, 41, 1685–1692. [Google Scholar] [CrossRef]
- Cheng, Z.; Peng, X.; He, W. Arterial Embolization of Primary Sacral Aneurysmal Bone Cyst. Chin. Med. J. 2014, 127, 1785–1787. [Google Scholar]
- Henrichs, M.P.; Beck, L.; Gosheger, G.; Streitbuerger, A.; Koehler, M.; Heindel, W.; Hardes, J.; Vieth, V. Selective Arterial Embolisation of Aneurysmal Bone Cysts of the Sacrum: A Promising Alternative to Surgery. Rofo 2016, 188, 53–59. [Google Scholar] [CrossRef]
- Lambot-Juhan, K.; Pannier, S.; Grévent, D.; Péjin, Z.; Breton, S.; Berteloot, L.; Emond-Gonsard, S.; Boddaert, N.; Glorion, C.; Brunelle, F. Primary Aneurysmal Bone Cysts in Children: Percutaneous Sclerotherapy with Absolute Alcohol and Proposal of a Vascular Classification. Pediatr. Radiol. 2012, 42, 599–605. [Google Scholar] [CrossRef]
- Marie-Hardy, L.; El Sayed, L.; Alves, A.; Brunelle, F.; Ouchrif, Y.; Naggara, O.; Breton, S.; Mascard, E.; Glorion, C.; Pannier, S. Percutaneous Alcohol-Based Sclerotherapy in Aneurysmal Bone Cyst in Children and Adolescents. Orthop. Traumatol. Surg. Res. 2020, 106, 1313–1318. [Google Scholar] [CrossRef]
- Oliveira, M.B.D.R.; Meohas, W.; Silva, R.R.; de Carvalho, G.S.; Mello, F.C.D.Q.; Paschoal, M.E.M. Percutaneous Treatment of Aneurysmal Bone Cyst with Calcitonin and Methylprednisolone. Acta Ortop. Bras. 2018, 26, 314–319. [Google Scholar] [CrossRef]
- Rastogi, S.; Varshney, M.K.; Trikha, V.; Khan, S.A.; Choudhury, B.; Safaya, R. Treatment of Aneurysmal Bone Cysts with Percutaneous Sclerotherapy Using Polidocanol. A Review of 72 Cases with Long-Term Follow-Up. J. Bone Jt. Surg. Br. 2006, 88, 1212–1216. [Google Scholar] [CrossRef]
- Puri, A.; Hegde, P.; Gulia, A.; Parikh, M. Primary Aneurysmal Bone Cysts. Bone Jt. J. 2020, 102-B, 186–190. [Google Scholar] [CrossRef]
- Jasper, J.; van der Heijden, L.; van Rijswijk, C.S.P.; van de Sande, M.A.J. Efficacy of Sclerotherapy With Polidocanol (Ethoxysclerol) in Primary Aneurysmal Bone Cysts in Children and Adolescents. J. Pediatr. Orthop. 2021, 41, e555–e562. [Google Scholar] [CrossRef]
- Cottalorda, J.; Louahem Sabah, D.; Joly Monrigal, P.; Jeandel, C.; Delpont, M. Minimally Invasive Treatment of Aneurysmal Bone Cysts: Systematic Literature Review. Orthop. Traumatol. Surg. Res. 2022, 108, 103272. [Google Scholar] [CrossRef]
- van Geloven, T.P.G.; van de Sande, M.A.J.; van der Heijden, L. The Treatment of Aneurysmal Bone Cysts. Curr. Opin. Pediatr. 2023, 35, 131–137. [Google Scholar] [CrossRef]
- Strohm, J.A.; Strohm, P.C.; Kühle, J.; Schmal, H.; Zwingmann, J. Management of Juvenile and Aneurysmal Bone Cysts: A Systematic Literature Review with Meta-Analysis. Eur. J. Trauma Emerg. Surg. 2023, 49, 361–372. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).