
From Bedside to Diagnosis: The Role of Ocular Fundus in Systemic Infections
 ,
,  , , , , and
, , , , and
Abstract
:
1. Introduction
2. Methods
3. Ocular Fundus Examination
4. Principal Systemic Infections at Bedside
4.1. Systemic Bacterial Infections
4.2. Systemic Viral Infections
4.3. Systemic Fungal Infections
4.4. Systemic Parasitic Infections
5. When Assessing Ocular Fundus in Systemic Infections
5.1. The Evidence about Ophthalmoscopy in Systemic Fungal Infections
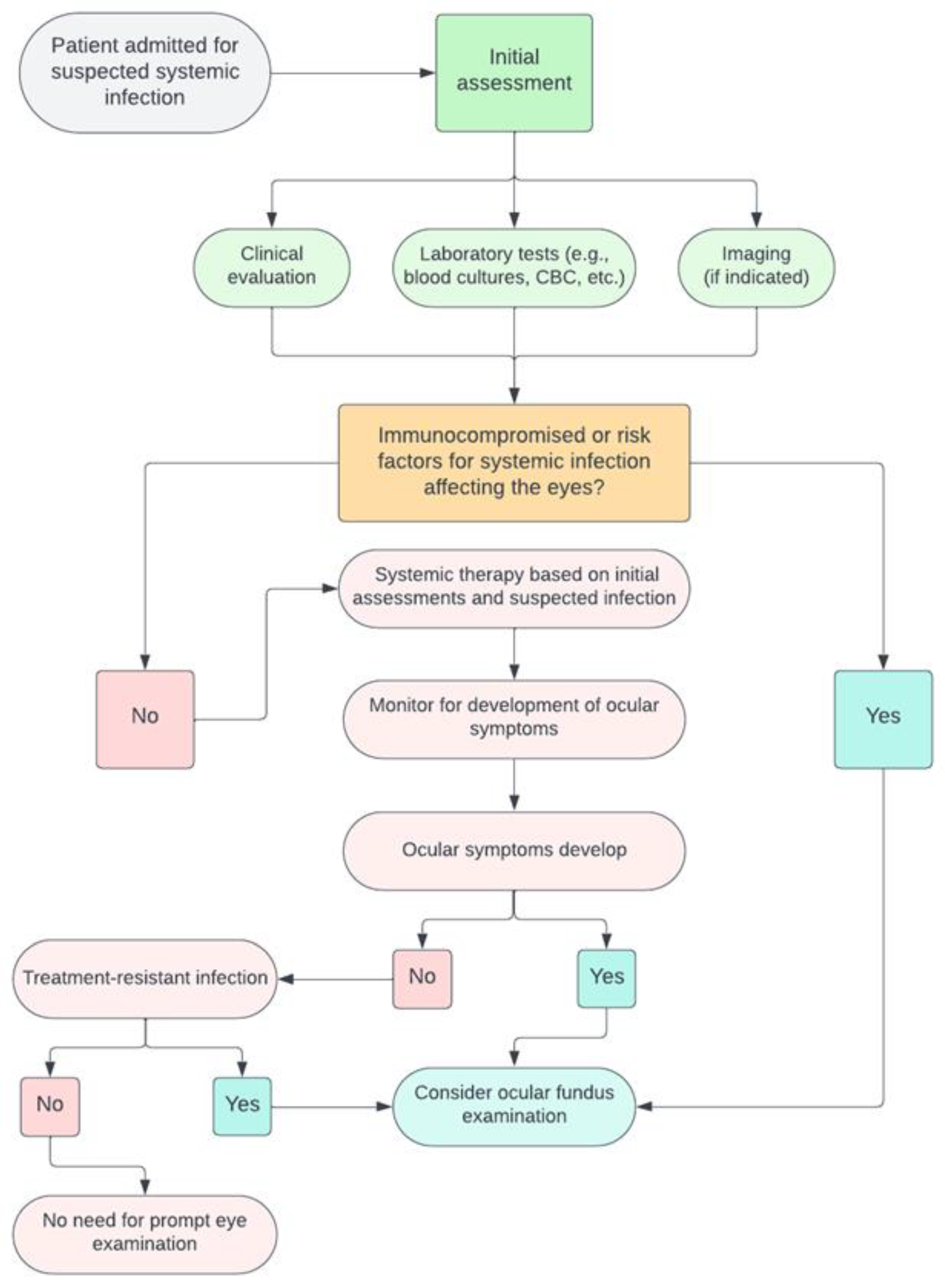
5.2. A Decision Tree for Clinicians
6. Patient Management after Ocular Fundus Examination
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pirani, V.; Pelliccioni, P.; De Turris, S.; Rosati, A.; Franceschi, A.; Cesari, C.; Nicolai, M.; Mariotti, C. The Eye as a Window to Systemic Infectious Diseases: Old Enemies, New Imaging. J. Clin. Med. 2019, 8, 1392. [Google Scholar] [CrossRef]
- Yannuzzi, L.A.; Ober, M.D.; Slakter, J.S.; Spaide, R.F.; Fisher, Y.L.; Flower, R.W.; Rosen, R. Ophthalmic Fundus Imaging: Today and Beyond. Am. J. Ophthalmol. 2004, 137, 511–524. [Google Scholar] [CrossRef]
- Salvetat, M.L.; Musa, M.; Pellegrini, F.; Salati, C.; Spadea, L.; Zeppieri, M. Considerations of COVID-19 in Ophthalmology. Microorganisms 2023, 11, 2220. [Google Scholar] [CrossRef]
- Ong, J.; Zarnegar, A.; Corradetti, G.; Singh, S.R.; Chhablani, J. Advances in Optical Coherence Tomography Imaging Technology and Techniques for Choroidal and Retinal Disorders. J. Clin. Med. 2022, 11, 5139. [Google Scholar] [CrossRef]
- Bypareddy, R.; Sujatha Rathod, B.L.; Shilpa, Y.D.; Hithashree, H.R.; Nagaraj, K.B.; Hemalatha, B.C.; Basumatary, J.; Bekal, D.; Niranjan, R.; Anusha, P.G. Fundus Evaluation in COVID-19 Positives with Non-Severe Disease. Indian. J. Ophthalmol. 2021, 69, 1271. [Google Scholar] [CrossRef]
- Narayana, S.; McGee, S. Bedside Diagnosis of the ‘Red Eye’: A Systematic Review. Am. J. Med. 2015, 128, 1220–1224.e1. [Google Scholar] [CrossRef]
- Pirraglia, M.P.; Ceccarelli, G.; Cerini, A.; Visioli, G.; d’Ettorre, G.; Mastroianni, C.M.; Pugliese, F.; Lambiase, A.; Gharbiya, M. Retinal Involvement and Ocular Findings in COVID-19 Pneumonia Patients. Sci. Rep. 2020, 10, 17419. [Google Scholar] [CrossRef]
- Mark, H.H. On the Evolution of Binocular Ophthalmoscopy. Arch. Ophthalmol. 2007, 125, 830–833. [Google Scholar] [CrossRef]
- Lynn, W.A.; Lightman, P.S. The Eye in Systemic Infection. Lancet 2004, 364, 1439–1450. [Google Scholar] [CrossRef]
- Uchio, E.; Ohno, S. Ocular Manifestations of Systemic Infections. Curr. Opin. Ophthalmol. 1999, 10, 452–457. [Google Scholar] [CrossRef]
- Madu, A.A.; Mayers, M. Ocular Manifestation of Systemic Infections. Curr. Opin. Ophthalmol. 1996, 7, 85–90. [Google Scholar] [CrossRef]
- 20 Surprising Health Problems an Eye Exam Can Catch—American Academy of Ophthalmology. Available online: https://www.aao.org/eye-health/tips-prevention/surprising-health-conditions-eye-exam-detects (accessed on 12 October 2023).
- Tsuboi, M.; Nishijima, T.; Yashiro, S.; Teruya, K.; Kikuchi, Y.; Katai, N.; Gatanaga, H.; Oka, S. Time to Development of Ocular Syphilis after Syphilis Infection. J. Infect. Chemother. 2018, 24, 75–77. [Google Scholar] [CrossRef]
- Keeler, C.R. The Ophthalmoscope in the Lifetime of Hermann von Helmholtz. Arch. Ophthalmol. 2002, 120, 194–201. [Google Scholar] [CrossRef]
- Benbassat, J.; Polak, B.C.P.; Javitt, J.C. Objectives of Teaching Direct Ophthalmoscopy to Medical Students. Acta Ophthalmol. 2012, 90, 503–507. [Google Scholar] [CrossRef]
- Rodenbeck, S.J.; MacKay, D.D. Examining the Ocular Fundus in Neurology. Curr. Opin. Neurol. 2019, 32, 105–110. [Google Scholar] [CrossRef]
- Sun, M.; Ma, A.; Li, F.; Cheng, K.; Zhang, M.; Yang, H.; Nie, W.; Zhao, B. Sensitivity and Specificity of Red Reflex Test in Newborn Eye Screening. J. Pediatr. 2016, 179, 192–196.e4. [Google Scholar] [CrossRef]
- Cordero, I. Understanding and Caring for an Indirect Ophthalmoscope. Community Eye Health 2016, 29, 57. [Google Scholar]
- Diori Adam, N.; Saa Kassoula Batomaguela, N.; Kossi, D.; Abbevi Elie, A.; Zakou, A.; Soumana, Y.; Amza, A.; Patrice Balo, K.; Adam, N.D. Contribution of the Fundus Examination in the Management of General Pathologies in Hospital in Lomé-Togo. Open J. Intern. Med. 2016, 9, 52–61. [Google Scholar] [CrossRef]
- Bouza, E.; Cobo-Soriano, R.; Rodríguez-Créixems, M.; Muñoz, P.; Suárez-Leoz, M.; Cortés, C. A Prospective Search for Ocular Lesions in Hospitalized Patients with Significant Bacteremia. Clin. Infect. Dis. 2000, 30, 306–312. [Google Scholar] [CrossRef]
- Roberts, T.; Chandna, A.; Watthanaworawit, W.; Thaiprakong, A.; Soeng, S.; Simmalavong, M.; Phoumin, P.; Saengchun, W.; Khatta, N.; Hinfonthong, P.; et al. Impact of Delayed Processing of Positive Blood Cultures on Organism Detection: A Prospective Multi-Centre Study. BMC Infect. Dis. 2022, 22, 517. [Google Scholar] [CrossRef]
- Coburn, P.S.; Wiskur, B.J.; Astley, R.A.; Callegan, M.C. Blood–Retinal Barrier Compromise and Endogenous Staphylococcus aureus Endophthalmitis. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7303–7311. [Google Scholar] [CrossRef]
- Yang, X.; Yu, X.W.; Zhang, D.D.; Fan, Z.G.; Wei, P.F. Blood-Retinal Barrier as a Converging Pivot in Understanding the Initiation and Development of Retinal Diseases. Chin. Med. J. 2020, 133, 2586. [Google Scholar] [CrossRef]
- Coburn, P.S.; Wiskur, B.J.; Miller, F.C.; Lagrow, A.L.; Astley, R.A.; Elliott, M.H.; Callegan, M.C. Bloodstream-To-Eye Infections Are Facilitated by Outer Blood-Retinal Barrier Dysfunction. PLoS ONE 2016, 11, e0154560. [Google Scholar] [CrossRef]
- Jackson, T.L.; Paraskevopoulos, T.; Georgalas, I. Systematic Review of 342 Cases of Endogenous Bacterial Endophthalmitis. Surv. Ophthalmol. 2014, 59, 627–635. [Google Scholar] [CrossRef]
- Ho, V.; Ho, L.Y.; Ranchod, T.M.; Drenser, K.A.; Williams, G.A.; Garretson, B.R. Endogenous Methicillin-Resistant Staphylococcus aureus Endophthalmitis. Retina 2011, 31, 596–601. [Google Scholar] [CrossRef]
- Levison, M.E.; Levison, J.H. Pharmacokinetics and Pharmacodynamics of Antibacterial Agents. Infect. Dis. Clin. N. Am. 2009, 23, 791–815. [Google Scholar] [CrossRef]
- Sallam, A.B.; Kirkland, K.A.; Barry, R.; Soliman, M.K.; Ali, T.K.; Lightman, S. A Review of Antimicrobial Therapy for Infectious Uveitis of the Posterior Segment. Med. Hypothesis Discov. Innov. Ophthalmol. 2018, 7, 140. [Google Scholar]
- Restivo, L.; Abbouda, A.; Nardella, C.; Bruscolini, A.; Pirraglia, M.P.; Pezzi, P.P. Uveitis Heralding Previously Unknown Luetic and HIV Infection. Syphilitic Uveitis in an Italian Referral Center. Ann. Ist. Super. Sanita 2013, 49, 133–137. [Google Scholar] [CrossRef]
- Wathek, C.; Rannen, R.; Wathek, C.; Rannen, R. Ocular Manifestations of Endocarditis. In Contemporary Challenges in Endocarditis; IntechOpen: London, UK, 2016. [Google Scholar] [CrossRef]
- Arora, N.; Dhibar, D.P.; Bashyal, B.; Agarwal, A. Roth’s Spots, a Clinical Diagnostic Clue for Infective Endocarditis. Perm. J. 2020, 24, 20.038. [Google Scholar] [CrossRef]
- Moramarco, A.; Mallone, F.; Pirraglia, M.P.; Bruscolini, A.; Giustolisi, R.; La Cava, M.; Lambiase, A. Clinical Features of Ocular Syphilis: A Retrospective Clinical Study in an Italian Referral Centre. Semin. Ophthalmol. 2020, 35, 50–55. [Google Scholar] [CrossRef]
- Mao, L.K.; Flynn, H.W.; Miller, D.; Pflugfelder, S.C. Endophthalmitis Caused by Staphylococcus aureus. Am. J. Ophthalmol. 1993, 116, 584–589. [Google Scholar] [CrossRef]
- Yoshida, M.; Yokokura, S.; Nishida, T.; Mochizuki, K.; Suzuki, T.; Maruyama, K.; Otomo, T.; Nishiguchi, K.M.; Kunikata, H.; Nakazawa, T. Endogenous Endophthalmitis Caused by Group B Streptococcus; Case Reports and Review of 35 Reported Cases. BMC Ophthalmol. 2020, 20, 126. [Google Scholar] [CrossRef]
- La Cava, M.; Bruscolini, A.; Sacchetti, M.; Pirraglia, M.P.; Moramarco, A.; Marenco, M.; Iaiani, G.; Covelli, G.; Rizzo, T.; Abicca, I.; et al. Clinical and Epidemiological Study on Tubercular Uveitis in a Tertiary Eye Care Centre in Italy. J. Ophthalmol. 2020, 2020, 4701820. [Google Scholar] [CrossRef]
- Ang, M.; Vasconcelos-Santos, D.V.; Sharma, K.; Accorinti, M.; Sharma, A.; Gupta, A.; Rao, N.A.; Chee, S.P. Diagnosis of Ocular Tuberculosis. Ocul. Immunol. Inflamm. 2018, 26, 208–216. [Google Scholar] [CrossRef]
- Sherif, N.; Khine, K.T.; Houghton, O.M. Acute Syphilitic Posterior Placoid Chorioretinitis as the Presenting Symptom of Syphilis in an Immunocompetent Patient. Am. J. Ophthalmol. Case Rep. 2022, 28, 101695. [Google Scholar] [CrossRef]
- Wang, S.; Jiang, B.; Li, Y.; Shang, Y.; Liu, Z.; Zhang, Y. A Case Report of Disseminated Nocardiosis with Ocular Involvement in a Myasthenia Gravis Patient and Literature Review. BMC Neurol. 2019, 19, 243. [Google Scholar] [CrossRef]
- Accorinti, M. Ocular Bartonellosis. Int. J. Med. Sci. 2009, 6, 131. [Google Scholar] [CrossRef]
- Tey, M.S.Y.; Govindasamy, G.; Vendargon, F.M. The Clinical Spectrum of Ocular Bartonellosis: A Retrospective Study at a Tertiary Centre in Malaysia. J. Ophthalmic Inflamm. Infect. 2020, 10, 31. [Google Scholar] [CrossRef]
- Ganatra, J.B.; Chandler, D.; Santos, C.; Kuppermann, B.; Margolis, T.P. Viral Causes of the Acute Retinal Necrosis Syndrome. Am. J. Ophthalmol. 2000, 129, 166–172. [Google Scholar] [CrossRef]
- Wu, X.N.; Lightman, S.; Tomkins-Netzer, O. Viral Retinitis: Diagnosis and Management in the Era of Biologic Immunosuppression: A Review. Clin. Exp. Ophthalmol. 2019, 47, 381–395. [Google Scholar] [CrossRef]
- Pathai, S.; Deshpande, A.; Gilbert, C.; Lawn, S.D. Prevalence of HIV-Associated Ophthalmic Disease among Patients Enrolling for Antiretroviral Treatment in India: A Cross-Sectional Study. BMC Infect. Dis. 2009, 9, 158. [Google Scholar] [CrossRef]
- Sudharshan, S.; Nair, N.; Curi, A.; Banker, A.; Kempen, J. Human Immunodeficiency Virus and Intraocular Inflammation in the Era of Highly Active Anti Retroviral Therapy—An Update. Indian. J. Ophthalmol. 2020, 68, 1787. [Google Scholar] [CrossRef]
- Carmichael, A. Cytomegalovirus and the Eye. Eye 2012, 26, 237. [Google Scholar] [CrossRef]
- Accorinti, M.; Abbouda, A.; Gilardi, M.; Zito, R.; Iannetti, L. Cytomegalovirus-Related Scleritis. Ocul. Immunol. Inflamm. 2013, 21, 413–415. [Google Scholar] [CrossRef]
- Razonable, R.R. Oral Antiviral Drugs for Treatment of Cytomegalovirus in Transplant Recipients. Clin. Microbiol. Infect. 2023, 29, 1144–1149. [Google Scholar] [CrossRef]
- Rafailidis, P.I.; Mourtzoukou, E.G.; Varbobitis, I.C.; Falagas, M.E. Severe Cytomegalovirus Infection in Apparently Immunocompetent Patients: A Systematic Review. Virol. J. 2008, 5, 47. [Google Scholar] [CrossRef]
- Becker, K.N.; Becker, N.M. Ocular Manifestations Seen in HIV. Disease-a-Month 2014, 60, 268–275. [Google Scholar] [CrossRef]
- Cheraqpour, K.; Ahmadraji, A.; Rashidinia, A.; Irannejad, M.; Shahriari, M. Acute Retinal Necrosis Caused by Co-Infection with Multiple Viruses in a Natalizumab-Treated Patient: A Case Report and Brief Review of Literature. BMC Ophthalmol. 2021, 21, 337. [Google Scholar] [CrossRef]
- Vasudevan, A.; Rojas-Moreno, C.; Tarun, T. Acute Retinal Necrosis Secondary to Varicella Zoster Virus. IDCases 2019, 18, e00585. [Google Scholar] [CrossRef]
- Radwan, A.; Metzinger, J.L.; Hinkle, D.M.; Foster, C.S. Cytomegalovirus Retinitis in Immunocompetent Patients: Case Reports and Literature Review. Ocul. Immunol. Inflamm. 2013, 21, 324–328. [Google Scholar] [CrossRef]
- Stewart, M.W. Optimal Management of Cytomegalovirus Retinitis in Patients with AIDS. Clin. Ophthalmol. 2010, 4, 285–299. [Google Scholar] [CrossRef]
- Wons, J.; Kempen, J.; Garweg, J.G. HIV-Induced Retinitis. Ocul. Immunol. Inflamm. 2020, 28, 1259–1268. [Google Scholar] [CrossRef]
- Loubsens, E.; Adam, R.; Debard, A.; Barioulet, L.; Varenne, F.; Fournié, P.; Sales de Gauzy, T.; Ollé, P.; Martin-Blondel, G.; Soler, V. First-Line Management of Necrotizing Herpetic Retinitis by Prioritizing the Investigation of Immune Status and Prognostic Factors for Poor Visual Outcomes. Int. Ophthalmol. 2023, 43, 2545. [Google Scholar] [CrossRef]
- Jabs, D.A.; Belfort, R.; Bodaghi, B.; Graham, E.; Holland, G.N.; Lightman, S.L.; Oden, N.; Palestine, A.G.; Smith, J.R.; Thorne, J.E.; et al. Classification Criteria for Cytomegalovirus Retinitis. Am. J. Ophthalmol. 2021, 228, 245. [Google Scholar] [CrossRef]
- Ho, M.; Invernizzi, A.; Zagora, S.; Tsui, J.; Oldani, M.; Lui, G.; McCluskey, P.; Young, A.L. Presenting Features, Treatment and Clinical Outcomes of Cytomegalovirus Retinitis: Non-HIV Patients Vs HIV Patients. Ocul. Immunol. Inflamm. 2020, 28, 651–658. [Google Scholar] [CrossRef]
- Venkatesh, A.; Patel, R.; Goyal, S.; Rajaratnam, T.; Sharma, A.; Hossain, P. Ocular Manifestations of Emerging Viral Diseases. Eye 2021, 35, 1117–1139. [Google Scholar] [CrossRef]
- Riotto, E.; Mégevand, V.; Mégevand, A.; Marti, C.; Pugin, J.; Stangos, A.N.; Marconi Archinto, L.; Sunaric Mégevand, G. Retinal Manifestations in Patients with COVID-19: A Prospective Cohort Study. J. Clin. Med. 2022, 11, 1828. [Google Scholar] [CrossRef]
- Teo, K.Y.; Invernizzi, A.; Staurenghi, G.; Cheung, C.M.G. COVID-19-Related Retinal Micro-Vasculopathy—A Review of Current Evidence. Am. J. Ophthalmol. 2022, 235, 98–110. [Google Scholar] [CrossRef]
- El-Abiary, M.; Jones, B.; Williams, G.; Lockington, D. Fundoscopy Screening for Intraocular Candida in Patients with Positive Blood Cultures—Is It Justified? Eye 2018, 32, 1697. [Google Scholar] [CrossRef]
- Vinikoor, M.J.; Zoghby, J.; Cohen, K.L.; Tucker, J.D. Do All Candidemic Patients Need an Ophthalmic Examination? Int. J. Infect. Dis. 2013, 17, e146–e148. [Google Scholar] [CrossRef]
- Breazzano, M.P.; Bond, J.B.; Bearelly, S.; Kim, D.H.; Donahue, S.P.; Lum, F.; Olsen, T.W. American Academy of Ophthalmology Recommendations on Screening for Endogenous Candida Endophthalmitis. Ophthalmology 2022, 129, 73–76. [Google Scholar] [CrossRef]
- Haseeb, A.A.; Elhusseiny, A.M.; Siddiqui, M.Z.; Ahmad, K.T.; Sallam, A.B. Fungal Endophthalmitis: A Comprehensive Review. J. Fungi 2021, 7, 996. [Google Scholar] [CrossRef]
- Reginatto, P.; Agostinetto, G.d.J.; Fuentefria, R.D.N.; Marinho, D.R.; Pizzol, M.D.; Fuentefria, A.M. Eye Fungal Infections: A Mini Review. Arch. Microbiol. 2023, 205, 236. [Google Scholar] [CrossRef]
- Klastersky, J. Empirical Antifungal Therapy. Int. J. Antimicrob. Agents 2004, 23, 105–112. [Google Scholar] [CrossRef]
- Gauthier, G.M.; Nork, T.M.; Prince, R.; Andes, D. Subtherapeutic Ocular Penetration of Caspofungin and Associated Treatment Failure in Candida Albicans Endophthalmitis. Clin. Infect. Dis. 2005, 41, e27–e28. [Google Scholar] [CrossRef]
- Zhang, M.K.; Rao, Z.G.; Ma, T.; Tang, M.; Xu, T.Q.; He, X.X.; Li, Z.P.; Liu, Y.; Xu, Q.J.; Yang, K.Y.; et al. Appropriate Empirical Antifungal Therapy Is Associated with a Reduced Mortality Rate in Intensive Care Unit Patients with Invasive Fungal Infection: A Real-World Retrospective Study Based on the MIMIC-IV Database. Front. Med. 2022, 9, 952611. [Google Scholar] [CrossRef]
- Danielescu, C.; Stanca, H.T.; Iorga, R.E.; Darabus, D.M.; Potop, V. The Diagnosis and Treatment of Fungal Endophthalmitis: An Update. Diagnostics 2022, 12, 679. [Google Scholar] [CrossRef]
- Singh, S.; Singh, S.; Kumar, A. Systemic Candida Albicans Infection in Mice Causes Endogenous Endophthalmitis via Breaching the Outer Blood-Retinal Barrier. 2022, 10, e0165822. [CrossRef]
- Das, D.; Ramachandra, V.; Islam, S.; Bhattacharjee, H.; Biswas, J.; Koul, A.; Deka, P.; Deka, A. Update on Pathology of Ocular Parasitic Disease. Indian. J. Ophthalmol. 2016, 64, 794. [Google Scholar] [CrossRef]
- El-Sayed, N.M.; Safar, E.H. Characterization of the Parasite-Induced Lesions in the Posterior Segment of the Eye. Indian. J. Ophthalmol. 2015, 63, 881. [Google Scholar] [CrossRef]
- Song, H.B.; Jun, H.O.; Kim, J.H.; Lee, Y.H.; Choi, M.H.; Kim, J.H. Disruption of Outer Blood-Retinal Barrier by Toxoplasma gondii-Infected Monocytes Is Mediated by Paracrinely Activated FAK Signaling. PLoS ONE 2017, 12, e0175159. [Google Scholar] [CrossRef]
- Pleyer, U.; Schlüter, D.; Mänz, M. Ocular Toxoplasmosis: Recent Aspects of Pathophysiology and Clinical Implications. Ophthalmic Res. 2014, 52, 116–123. [Google Scholar] [CrossRef]
- Ahn, S.J.; Woo, S.J.; Jin, Y.; Chang, Y.S.; Kim, T.W.; Ahn, J.; Heo, J.W.; Yu, H.G.; Chung, H.; Park, K.H.; et al. Clinical Features and Course of Ocular Toxocariasis in Adults. PLoS Negl. Trop. Dis. 2014, 8, e2938. [Google Scholar] [CrossRef]
- Klotz, S.A.; Penn, C.C.; Negvesky, G.J.; Butrus, S.I. Fungal and Parasitic Infections of the Eye. Clin. Microbiol. Rev. 2000, 13, 662. [Google Scholar] [CrossRef]
- Kalogeropoulos, D.; Sakkas, H.; Mohammed, B.; Vartholomatos, G.; Malamos, K.; Sreekantam, S.; Kanavaros, P.; Kalogeropoulos, C. Ocular Toxoplasmosis: A Review of the Current Diagnostic and Therapeutic Approaches. Int. Ophthalmol. 2022, 42, 295. [Google Scholar] [CrossRef]
- Brodeur, K.R.N.; Herculano, A.; Oliveira, K. Clinical Aspects of Malarial Retinopathy: A Critical Review. Pathog. Glob. Health 2023, 117, 450–461. [Google Scholar] [CrossRef]
- Beare, N.A.V.; Taylor, T.E.; Harding, S.P.; Lewallen, S.; Molyneux, M.E. Malarial Retinopathy: A Newly Established Diagnostic Sign in Severe Malaria. Am. J. Trop. Med. Hyg. 2006, 75, 790–797. [Google Scholar] [CrossRef]
- Ahn, S.J.; Ryoo, N.-K.; Woo, S.J. Ocular Toxocariasis: Clinical Features, Diagnosis, Treatment, and Prevention. Asia Pac. Allergy 2014, 4, 134. [Google Scholar] [CrossRef]
- Au, L.; Guduru, K.; Lipscomb, G.; Kelly, S.P.; Hospitals, B.; Bolton, N.T. Candida Endophthalmitis: A Critical Diagnosis in the Critically Ill. Clin. Ophthalmol. 2007, 1, 551. [Google Scholar]
- Grewal, D.S.; Gabr, H. Inpatient Ophthalmology Consultations. Med. Clin. N. Am. 2021, 105, 563. [Google Scholar] [CrossRef]
- Vena, A.; Muñoz, P.; Padilla, B.; Valerio, M.; Sanchez, M.I.; Puig-Asensio, M.; Fortun, J.; Fernandez-Ruiz, M.; Merino, P.; Losa, J.E.; et al. Is Routine Ophthalmoscopy Really Necessary in Candidemic Patients? PLoS ONE 2017, 12, e0183485. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Cuenca-Estrella, M.; Verweij, P.E.; Arendrup, M.C.; Arikan-Akdagli, S.; Bille, J.; Donnelly, J.P.; Jensen, H.E.; Lass-Flörl, C.; Richardson, M.D.; Akova, M.; et al. ESCMID* Guideline for the Diagnosis and Management of Candida Diseases 2012: Diagnostic Procedures. Clin. Microbiol. Infect. 2012, 18 (Suppl. S7), 9–18. [Google Scholar] [CrossRef]
- The Royal College of Ophthalmologists Ophthalmic Services Guidance; Eye Care in the Intensive Care Unit (ICU): London, UK, 2017.
- Urbak, S.E.; Degn, T. Fluconazole in the Management of Fungal Ocular Infections. Ophthalmologica 1994, 208, 147–156. [Google Scholar] [CrossRef]
- Riddell IV, J.; Comer, G.M.; Kauffman, C.A. Treatment of Endogenous Fungal Endophthalmitis: Focus on New Antifungal Agents. Clin. Infect. Dis. 2011, 52, 648–653. [Google Scholar] [CrossRef]
- Breazzano, M.P.; Day, H.R.; Bloch, K.C.; Tanaka, S.; Cherney, E.F.; Sternberg, P.; Donahue, S.P.; Bond, J.B. Utility of Ophthalmologic Screening for Patients With Candida Bloodstream Infections: A Systematic Review. JAMA Ophthalmol. 2019, 137, 698–710. [Google Scholar] [CrossRef]
- Kato, H.; Yoshimura, Y.; Suido, Y.; Ide, K.; Sugiyama, Y.; Matsuno, K.; Nakajima, H. Prevalence of, and Risk Factors for, Hematogenous Fungal Endophthalmitis in Patients with Candida Bloodstream Infection. Infection 2018, 46, 635–640. [Google Scholar] [CrossRef]
- Carpani, G.; Foresti, S.; Dell’Oro, R.; Grassi, G.; Bombelli, M. Severe Systemic Cytomegalovirus Infection in an Immunocompetent Patient Outside the Intensive Care Unit: A Case Report. BMC Infect. Dis. 2019, 19, 34. [Google Scholar] [CrossRef]
- Oh, D.J.; Kanu, L.N.; Chen, J.L.; Aref, A.A.; Mieler, W.F.; Macintosh, P.W. Inpatient and Emergency Room Ophthalmology Consultations at a Tertiary Care Center. J. Ophthalmol. 2019, 2019, 7807391. [Google Scholar] [CrossRef]
- Adam, M.K.; Vahedi, S.; Nichols, M.M.; Fintelmann, R.E.; Keenan, J.D.; Garg, S.J.; Hsu, J.; Maguire, J.I.; Spirn, M.J. Inpatient Ophthalmology Consultation for Fungemia: Prevalence of Ocular Involvement and Necessity of Funduscopic Screening. Am. J. Ophthalmol. 2015, 160, 1078–1083.e2. [Google Scholar] [CrossRef]
- Li, W.; Wang, X.; Zhao, L.; Lin, D.; Yang, Y.; Liu, Z.; Wu, X.; Wang, J.; Zhu, Y.; Chen, C.; et al. The Value and Implementation of Routine Ophthalmic Examination in the Era of HAART. EClinicalMedicine 2021, 31, 100646. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Etiological Agent (Systemic Condition) | Ocular Fundus Findings | Onset of Ocular Findings |
|---|---|---|
| Streptococcus spp. and Staphylococcus spp. (sepsis or endocarditis) | Roth spots, hemorrhages, endophthalmitis, chorioretinitis | Early |
| Neisseria meningitidis (meningitis) | Papilledema, hemorrhages | Early |
| Mycobacterium tuberculosis (tuberculosis) | Chorioretinitis, choroid tubercles, retinal vasculitis, panuveitis | Late |
| Nocardia spp. (sepsis) | Chorioretinitis, subretinal abscesses | Early |
| Treponema pallidum (syphilis) | Chorioretinitis, optic neuritis placoid lesions, retinal necrosis, vasculitis, panuveitis | Late |
| Bartonella spp. (bartonellosis) | Chorioretinitis, optic neuritis, focal retinitis, serous retinal detachment, vitritis | Late |
| Etiological Agent | Ocular Fundus Findings | Onset of Ocular Findings |
|---|---|---|
| Cytomegalovirus (CMV) | CMV retinitis, hemorrhages | Early in severe immunosuppresion |
| Herpes Simplex Virus (HSV) and Varicella-Zoster Virus (VZV) | Acute retinal necrosis (ARN), progressive outer retinal necrosis (PORN), retinitis, choroiditis | Early |
| Human Immunodeficiency Virus (HIV) with no other associated infections | Cotton-wool spots, microangiopathy | Late |
| SARS-CoV-2 (COVID-19) | Still no evidence of specific findings | Reported Early or Late |
| Etiological Agent | Ocular Fundus Findings | Onset of Ocular Findings |
|---|---|---|
| Candida spp. (candidiasis) | Retinitis, vitritis, endophthalmitis | Early/Late |
| Toxoplasma gondii (toxoplasmosis) | Retinochoroiditis (acutely or through reactivation); grey-white retinal necrosis with adjacent choroiditis and vitritis | Early Late (reactivation) |
| Toxocara canis/cati (toxocariasis) | Retinal granuloma, epiretinal membrane formation, macular edema, vitritis | Early/Late |
| Plasmodium spp. (malaria) | Retinal whitening, orange or white discoloration of vessels, hemorrhages, and potentially papilledema | Early |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Visioli, G.; Zeppieri, M.; Iannucci, V.; Manni, P.; Albanese, G.M.; Salati, C.; Spadea, L.; Pirraglia, M.P. From Bedside to Diagnosis: The Role of Ocular Fundus in Systemic Infections. J. Clin. Med. 2023, 12, 7216. https://doi.org/10.3390/jcm12237216
Visioli G, Zeppieri M, Iannucci V, Manni P, Albanese GM, Salati C, Spadea L, Pirraglia MP. From Bedside to Diagnosis: The Role of Ocular Fundus in Systemic Infections. Journal of Clinical Medicine. 2023; 12(23):7216. https://doi.org/10.3390/jcm12237216
Chicago/Turabian StyleVisioli, Giacomo, Marco Zeppieri, Valeria Iannucci, Priscilla Manni, Giuseppe Maria Albanese, Carlo Salati, Leopoldo Spadea, and Maria Pia Pirraglia. 2023. "From Bedside to Diagnosis: The Role of Ocular Fundus in Systemic Infections" Journal of Clinical Medicine 12, no. 23: 7216. https://doi.org/10.3390/jcm12237216